Stage-directed surgical treatment of lunate avascular necrosis — joint levelling, revascularisation, intercarpal fusion and salvage
- Kienbock disease is avascular necrosis of the lunate, classically in the dominant wrist of men aged 20-40 who perform manual labour. The aetiology is multifactorial: negative ulnar variance concentrates load on the lunate, repetitive microtrauma disrupts the tenuous dual blood supply (primarily dorsal vessels through the dorsal radiocarpal and intercarpal ligaments, supplemented by volar vessels), and a single-vessel lunate anatomy predisposes to ischaemia.
- The Lichtman classification (revised 2002) drives surgical decision-making: Stage I = normal radiographs with MRI signal change only; Stage IIA = linear or compression fracture without carpal collapse; Stage IIIA = sclerosis and fragmentation without carpal height loss; Stage IIIB = lunate collapse with fixed scaphoid rotation (scapholunate angle greater than 60 degrees) and a carpal height ratio less than 0.54; Stage IV = pancarpal arthritis.
- Ulnar variance is the second governing variable and must be measured on a standardised PA wrist film in neutral rotation. Ulnar-negative wrists are treated with radial shortening osteotomy in stages I-IIIA; ulnar-neutral or positive wrists require capitate shortening or revascularisation instead, because shortening the radius would overload the distal radioulnar joint.
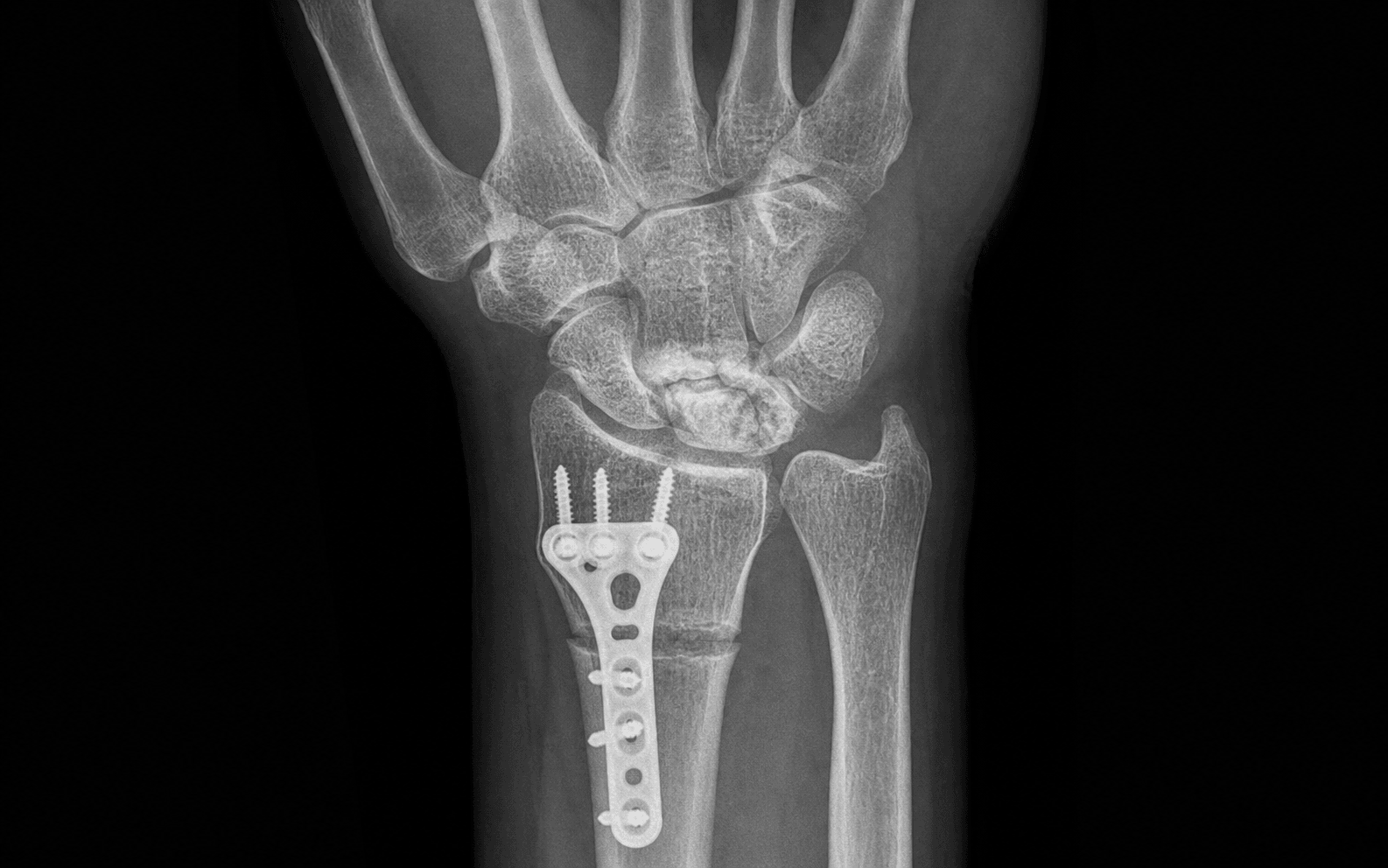
- Radial shortening osteotomy removes 2-4 mm of distal radius (to a target postoperative ulnar variance of 0 to plus 1 mm), fixed with a dorsal plate, transferring load off the lunate. Never shorten by more than the ulnar variance plus 2 mm, or the DRUJ is overloaded — a classic, specifically tested exam trap.
- At stage IIIB the algorithm branches to salvage: scaphotrapeziotrapezoid or scaphocapitate fusion stabilises the collapsed row, or proximal row carpectomy (PRC) lets the capitate articulate with the radius. PRC preserves about 60-70 percent of grip and 50-60 degrees of flexion-extension but is contraindicated if the capitate head cartilage is worn — check the preoperative MRI.
When & Why
Kienbock disease (avascular necrosis of the lunate) is managed surgically once conservative treatment has failed and symptoms are intrusive. Two independent variables govern every decision: the Lichtman radiographic stage (the degree of lunate collapse and carpal instability) and the ulnar variance (which determines which joint-levelling procedure is biomechanically appropriate).
- Ulnar negative
- Observe; immobilise; consider radial shortening if progressive pain
- Ulnar neutral / positive
- Observe; immobilise; consider capitate shortening or core decompression if progressive
- Ulnar negative
- Radial shortening osteotomy (2-4 mm)
- Ulnar neutral / positive
- Capitate shortening osteotomy or revascularisation
- Ulnar negative
- Radial shortening osteotomy (2-4 mm)
- Ulnar neutral / positive
- Capitate shortening, revascularisation, or core decompression
- Ulnar negative
- STT fusion, scaphocapitate fusion, or PRC
- Ulnar neutral / positive
- STT fusion, scaphocapitate fusion, or PRC
- Ulnar negative
- Total wrist fusion or arthroplasty
- Ulnar neutral / positive
- Total wrist fusion or arthroplasty
Absolute indications for surgery - Lichtman stage IIA or greater with persistent pain despite 3-6 months of conservative treatment (immobilisation, NSAIDs, activity modification)
- Progressive lunate collapse on serial radiographs
- Loss of carpal height or fixed scaphoid flexion (stage IIIB)
- Pancarpal arthritis (stage IV) Relative indications - Stage I with persistent symptoms greater than 6 months despite immobilisation (some surgeons offer earlier joint levelling in manual labourers)
- Bilateral Kienbock disease (operate the more symptomatic side first)
- Patient preference for definitive surgical management over prolonged immobilisation
Ulnar-neutral or positive variance (shortening the radius would worsen the imbalance), pre-existing DRUJ arthritis or instability, active infection, or uncorrected smoking (significantly increases nonunion risk).
Capitate head chondrosis on MRI (PRC relies on a capitate-radius articulation), radiocarpal arthritis (stage IV), or active infection. MRI before PRC is mandatory.
Midcarpal arthritis extends beyond the targeted fusion site, advanced pancarpal arthritis (stage IV), or poor bone quality precluding reliable fixation.
Conservative management first. Stage I and early stage IIA disease may be managed with a short-arm thumb spica cast or splint for 4-12 weeks to reduce mechanical load on the lunate, with activity modification and NSAIDs. Approximately 20-30 percent of stage I patients improve with immobilisation alone, though many progress to surgery. Core decompression (percutaneous drilling of the lunate to stimulate vascular channels) is a low-morbidity option for early stages (I-IIA) regardless of ulnar variance, with small case series reporting symptom improvement in 60-80 percent of patients. Consent specifically for: nonunion (1-5 percent after radial shortening, 5-10 percent after capitate shortening), progressive lunate collapse (10-20 percent despite an adequate joint-levelling procedure), DRUJ overload from excessive radial shortening, wrist stiffness, complex regional pain syndrome, and the possibility that the chosen procedure may not fully relieve symptoms (about 10-20 percent of patients ultimately require a salvage operation). Setup. Supine, arm abducted 90 degrees on a hand table with the forearm in neutral rotation (essential for confirming ulnar variance on fluoroscopy), upper-arm tourniquet inflated to 250 mmHg. General or regional (brachial plexus) anaesthesia depending on duration — regional suffices for an isolated osteotomy; combined procedures favour general anaesthesia. Prophylactic antibiotics (e.g. cefazolin 2 g IV at induction), as the procedure involves bone work and implants. Position the C-arm from the ulnar side to allow AP and lateral imaging without moving the arm.
The Operation
The goal is to offload or replace the avascular lunate through the dorsal approach — the workhorse exposure for every procedure in Kienbock disease. The exposure is laid out in full as the first steps below (it is the heart of the operation); the procedure then diverges by stage and ulnar variance into joint levelling, salvage, or revascularisation.
Dorsal approach to the wrist — the shared exposure
- Supine, arm table, forearm in neutral rotation, upper-arm tourniquet to 250 mmHg.
- Confirm the ulnar variance on a true PA wrist fluoroscopy view in neutral rotation (shoulder abducted 90, elbow flexed 90) before prepping — pronation or supination shifts the measurement by up to 2 mm.
- C-arm from the ulnar side; verify PA and lateral views of the wrist.
- A longitudinal or slightly curved incision centred over the Lister tubercle (the dorsal radial prominence), extending about 4 cm proximal and 3 cm distal to the radiocarpal joint, along the axis of the third metacarpal to optimise the scar.
- Danger: the superficial branch of the radial nerve (SBRN) lies in the subcutaneous fat over the anatomical snuffbox — stay radial to the Lister tubercle and do not dissect into the snuffbox. The dorsal cutaneous branch of the ulnar nerve lies on the ulnar side — protect it with careful skin-flap elevation.
- Incise the dorsal retinaculum along the line of the third extensor compartment (EPL), creating a radial-based flap.
- Elevate the second compartment (ECRB, ECRL) radially and the fourth compartment (EDM) ulnarly.
- Release the EPL from its groove at the Lister tubercle and retract it radially — this exposes the dorsal wrist capsule.
- In the floor of the fourth extensor compartment, identify the PIN running with the posterior interosseous artery on the dorsal wrist capsule.
- The PIN is small (1-2 mm) and easily transected or crushed during retinacular elevation — identify it deliberately before any deeper dissection.
- Either protect it with a vessel loop, or perform a short-segment neurectomy about 1-2 cm proximal to the radiocarpal joint, which provides reliable pain relief without detectable motor deficit (the PIN is purely motor to EDM and EPL distally, and loss is clinically silent).
- Create a longitudinal capsular incision or a radially-based capsular flap depending on the planned procedure.
- For an osteotomy, a limited capsulotomy over the radiocarpal joint suffices; for PRC or fusion, raise a wider flap to expose the whole carpus.
- Orient on the scaphoid (radial and proximal), the lunate (central, between scaphoid and triquetrum — the target of revascularisation), the triquetrum (ulnar and proximal) and the capitate (central, distal to the lunate; its head forms the midcarpal joint and is the key landmark for PRC and capitate shortening).
The posterior interosseous nerve lies on the floor of the fourth extensor compartment, directly on the dorsal wrist capsule, deep to the EDM tendons. If it is divided unrecognised, a painful neuroma can develop; if it is caught under a plate or screw, it causes chronic dorsal wrist pain. Identify it as the retinaculum is elevated and either protect it with a vessel loop or perform a prophylactic neurectomy at the distal-radius level. Never leave it as an unidentified structure crossing the operative field.
I identify the PIN on the floor of the fourth compartment in every dorsal wrist approach. I either protect it with a vessel loop for the duration of the procedure, or I perform a short segment neurectomy about 1.5 cm proximal to the radiocarpal joint, which provides reliable pain relief. I do not leave it as an unidentified structure where it could be caught in plates or screws.
After exposure, the procedure diverges. Joint-levelling osteotomies (radial or capitate shortening) are used in stages I-IIIA; at stage IIIB the algorithm shifts to motion-sparing salvage (STT/scaphocapitate fusion or PRC); stage IV requires total wrist fusion or arthroplasty; revascularisation is added for a viable lunate.
Radial shortening osteotomy (ulnar-negative, stages I–IIIA)
- Confirm ulnar variance on intraoperative fluoroscopy (PA wrist, neutral rotation; compare with the contralateral side if available).
- Calculate the target: aim for a postoperative ulnar variance of 0 to plus 1 mm. The amount of shortening equals the current negative variance plus the desired offset.
- Mark the osteotomy on the dorsal cortex 2-3 cm proximal to the radiocarpal joint, at the metaphyseal flare, perpendicular to the long axis of the radius.
- Danger: measuring variance on pronated or supinated views is inaccurate (variance shifts up to 2 mm); over-shortening beyond variance plus 2 mm causes irreversible DRUJ overload; placing the cut too proximally enters the diaphysis and slows healing.
- With an oscillating saw under saline irrigation, create a transverse osteotomy through the dorsal cortex at the marked site.
- Complete the cut carefully through the volar cortex with osteotomes or the saw, protecting the volar soft tissues — especially the superficial branch of the radial nerve on the volar radial aspect.
- Remove a measured sliver of cortex to achieve the planned 2-4 mm shortening, confirmed with a calibrated osteotomy template or ruler.
- Apply a 3.5 mm LC-DCP or locking compression plate to the dorsal surface, contoured to the dorsal radius and centred over the osteotomy.
- Overbend the plate slightly and use eccentric screw placement in the proximal fragment to compress across the osteotomy.
- Confirm compression and the achieved ulnar variance on fluoroscopy before final tightening.
- Irrigate thoroughly.
- Close the dorsal retinaculum over the plate where possible (reduces tendon irritation), then subcutaneous tissue and skin.
- Apply a below-elbow plaster backslab in neutral rotation.
Never shorten the radius by more than the measured ulnar variance plus 2 mm (and never more than 4 mm total). Excessive shortening reverses the load imbalance, overloading the ulnar side of the DRUJ and causing ulnar-sided wrist pain, radioulnar impingement and progressive DRUJ arthritis. If the DRUJ is already symptomatic or arthritic, radial shortening is contraindicated — use capitate shortening instead.
I use a pre-contoured distal radius locking plate placed dorsally, overbend it slightly, and use eccentric screw placement in the proximal fragment to compress across the osteotomy. I confirm the achieved shortening and ulnar variance on intraoperative fluoroscopy before final tightening. The non-negotiable rule is: never shorten more than the measured ulnar variance plus 2 mm.
- Radial shortening
- Ulnar negative
- Capitate shortening
- Ulnar neutral or positive
- Radial shortening
- 2-4 mm
- Capitate shortening
- 2-3 mm
- Radial shortening
- Dorsal plate (3.5 mm LC-DCP or locking)
- Capitate shortening
- Headless compression screw or mini-plate
- Radial shortening
- Greater than 95 percent
- Capitate shortening
- 90-95 percent
- Radial shortening
- Overload if excessive shortening
- Capitate shortening
- Unaffected
- Radial shortening
- Dorsal or volar radial
- Capitate shortening
- Dorsal wrist (same as STT fusion)
- Radial shortening
- 70-90 percent
- Capitate shortening
- 70-85 percent
- Radial shortening
- 80-90 percent of preoperative
- Capitate shortening
- 80-90 percent of preoperative
- Radial shortening
- I, IIA, IIIA
- Capitate shortening
- I, IIA, IIIA
Capitate shortening osteotomy (neutral / positive variance, stages I–IIIA)
- Dorsal approach as described, with the capsular exposure extended to the midcarpal joint.
- Identify the capitate body and expose its waist through the dorsal capsulotomy.
- Create a transverse osteotomy at the capitate waist (the narrowest point of the capitate, distal to the head).
- Remove a 2-3 mm sliver of bone.
- Fix with an intramedullary headless compression screw (Acutrak or Herbert-type) directed from proximal to distal along the capitate axis; a mini-fragment plate is an alternative.
- Confirm screw position and the achieved shortening on fluoroscopy.
- Close the capsule and wound in layers; apply a short-arm thumb spica splint.
Scaphotrapeziotrapezoid (STT) fusion (stage IIIB)
Indication: stage IIIB with carpal collapse, fixed scaphoid flexion, and no pancarpal arthritis.
- Dorsal wrist approach with wide capsular exposure.
- Identify the STT joint (scaphoid-trapezium-trapezoid articulation on the radial side).
- Denude the articular cartilage from the scaphoid distal pole, the trapezium and the trapezoid using curettes and a burr; decorticate to bleeding cancellous surfaces.
- Correct the scaphoid flexion by manually dorsiflexing the distal pole of the scaphoid.
- Fix with K-wires or headless compression screws across scaphoid-to-trapezium and scaphoid-to-trapezoid surfaces.
- Pack the fusion bed with autologous cancellous bone graft from the distal radius or iliac crest.
- Confirm fixation and carpal alignment on fluoroscopy — the scapholunate angle should be less than 60 degrees after correction.
- Close the capsule and wound; apply a below-elbow plaster splint in neutral rotation.
Inadequate cartilage removal causes nonunion — denude all articular surfaces completely. Failure to correct the scaphoid flexion before fixation leaves the proximal carpal row collapsed. And dorsal hardware prominence irritates the extensor tendons — use buried screws or K-wires where possible; plate removal is often required later.
Proximal row carpectomy (stage IIIB)
Indication: stage IIIB (or stage III with midcarpal arthritis) when the capitate head cartilage is intact. PRC is simpler than intercarpal fusion and avoids nonunion risk.
- Before excising the carpal row, inspect the capitate head articular surface directly (or by arthroscopy).
- If the cartilage is intact (smooth, no fibrillation, no exposed bone), proceed. If chondrosis is present, abandon PRC and proceed to total wrist fusion or arthroplasty.
- Even when the MRI was reassuring, if the capitate looks worn at surgery, stop and change the plan.
- Remove the lunate first (central, easiest access), then the triquetrum (ulnar), then the scaphoid (radial), piecemeal through the dorsal capsulotomy using rongeurs and osteotomes.
- Remove the entire scaphoid — a retained distal pole impinges on the trapezium.
- Protect the capitate head during piecemeal excision of the lunate — it must remain pristine.
- The capitate should settle proximally into the lunate fossa of the radius; flex and extend the wrist to confirm a smooth arc without crepitus or impingement.
- Irrigate the carpal bed, close the dorsal capsule, then retinaculum, subcutaneous tissue and skin.
- Apply a below-elbow plaster backslab in neutral to slight extension; begin early mobilisation at 2-3 weeks.
Total wrist fusion (stage IV)
Indication: stage IV with pancarpal arthritis when pain is the dominant symptom and the patient accepts loss of wrist motion.
- Dorsal approach with wide exposure of the radiocarpal and midcarpal joints.
- Excise the proximal carpal row, or denude the articular surfaces depending on technique.
- Position the wrist in slight extension (about 10-15 degrees) — the most functional position for activities of daily living.
- Apply a dorsal wrist fusion plate from the distal radius to the third metacarpal.
- Pack all denuded joint surfaces with autologous cancellous bone graft.
- Fix with locking screws into the distal radius (3-4 screws) and the third metacarpal (2-3 screws).
- Confirm position, plate placement and fusion alignment on fluoroscopy.
- Close in layers; apply a long-arm plaster with the elbow at 90 degrees and the wrist in extension.
Revascularisation with a vascularised bone graft (early stage, viable lunate)
Indication: stage I-IIIA with a viable (non-collapsed) lunate, especially in younger patients (less than 35 years) where preserving lunate architecture is a priority — often combined with a joint-levelling osteotomy to offload and revascularise simultaneously.
- Dorsal approach with extended exposure of the distal radius.
- Identify the fourth and fifth extensor compartment arteries (branches of the anterior interosseous artery) running on the dorsal surface of the distal radius.
- Raise a pedicled corticocancellous bone graft from the dorsal distal radius (about 1 x 0.5 x 0.5 cm) based on these vessels.
- Create a dorsal cortical window in the lunate and curette the necrotic bone.
- Insert the vascularised graft into the lunate, maintaining the vascular pedicle; secure with a K-wire if needed.
- Optionally combine with radial or capitate shortening through the same approach.
- Post-operatively: short-arm thumb spica cast for 4-6 weeks, with serial MRI at 3-6 months to assess revascularisation (return of normal T1 signal). If revascularisation fails (persistent low signal with progressive collapse), escalate to motion-sparing salvage.
Aftercare & Complications
Rehabilitation | Phase | Timing | Focus | |-------|--------|-------| | Immediate | Day 0-7 | Elevation for 48 hours; interim splint or cast; paracetamol and NSAIDs (short opioid course 48-72 hours); finger flexion-extension from day 1 to prevent digital stiffness; wound check at 5-7 days | | Immobilisation | Weeks 1-6 | Procedure-specific cast/splint (see table); finger and elbow range of motion throughout | | Rehabilitation | Weeks 6-12 | Progressive wrist range of motion under hand therapy; avoid heavy loading for 8-12 weeks after osteotomy and 12-16 weeks after fusion; grip strengthening once bony healing is confirmed | | Return to function | Weeks 12-16+ | Office work at 2-4 weeks (osteotomy) or 6-8 weeks (fusion); manual work at 8-12 weeks (osteotomy/PRC) or 12-16 weeks (fusion); driving at 4-6 weeks (osteotomy/PRC) or 8-12 weeks (fusion) |
- Immobilisation
- Below-elbow cast 4-6 weeks
- Mobilisation start
- Finger ROM day 1; wrist at 4-6 weeks
- Grip strengthening
- From 6-8 weeks
- Union confirmation
- XR at 6 and 12 weeks
- Immobilisation
- Short-arm thumb spica 4-6 weeks
- Mobilisation start
- Finger ROM day 1; wrist at 4-6 weeks
- Grip strengthening
- From 6-8 weeks
- Union confirmation
- XR at 6 and 12 weeks
- Immobilisation
- Below-elbow cast 6-8 weeks
- Mobilisation start
- Finger ROM day 1; wrist at 6-8 weeks
- Grip strengthening
- From 8-10 weeks
- Union confirmation
- XR at 8 weeks, CT at 12-16 weeks
- Immobilisation
- Splint 2-3 weeks only
- Mobilisation start
- Wrist ROM from 2-3 weeks
- Grip strengthening
- From 4-6 weeks
- Union confirmation
- Not applicable (no fusion to heal)
- Immobilisation
- Long-arm cast 4 weeks, then short-arm 4-8 weeks
- Mobilisation start
- Finger and forearm ROM day 1; elbow from 4 weeks
- Grip strengthening
- From 12 weeks (once fused)
- Union confirmation
- XR at 8 and 12 weeks
Complications
- Incidence
- 10-20 percent after joint levelling
- Recognition
- Worsening pain, decreasing carpal height on serial radiographs, increasing sclerosis or fragmentation, loss of grip
- Prevention and management
- Prevention: accurate staging before surgery (stage IIIA and beyond benefit less); ensure adequate shortening. Management: escalate to motion-sparing salvage (STT fusion or PRC)
- Incidence
- 1-5 percent radial; 5-10 percent capitate
- Recognition
- Persistent pain at the osteotomy site after 3-4 months, no bridging trabeculae, hardware loosening
- Prevention and management
- Prevention: rigid plate fixation, smoking cessation, nutritional optimisation. Management: revision with bone grafting and enhanced fixation
- Incidence
- 5-15 percent
- Recognition
- Persistent midcarpal pain after 4-6 months, no bridging bone on CT, lucency around hardware, loss of correction
- Prevention and management
- Prevention: thorough cartilage denudement, rigid fixation (screws over K-wires), autologous bone graft, correct scaphoid position before fixation. Management: revision fusion; if persistent, convert to PRC or total wrist fusion
- Incidence
- 5-10 percent of radial shortening
- Recognition
- Ulnar-sided wrist pain with forearm rotation, painful clicking at the DRUJ, radiographic ulnar impingement (less than 2 mm DRUJ joint space)
- Prevention and management
- Prevention: never shorten more than ulnar variance plus 2 mm; confirm on intraoperative fluoroscopy. Management: activity modification and splinting; if severe, ulnar shortening osteotomy or Sauve-Kapandji
- Incidence
- 10-20 percent
- Recognition
- Tender prominence under the skin, pain with gripping or wrist extension, extensor tendon crepitus over hardware
- Prevention and management
- Prevention: low-profile plates contoured flush; close retinaculum over plate. Management: hardware removal once union is confirmed (typically 9-12 months)
- Incidence
- 10-30 percent
- Recognition
- Reduced flexion-extension arc, grip weakness, functional limitation at 3-6 months
- Prevention and management
- Prevention: early mobilisation protocol; hand therapy from 2-4 weeks; splint in a functional position. Management: structured hand therapy, dynamic and static progressive splinting, manipulation under anaesthesia if refractory
- Incidence
- 2-5 percent
- Recognition
- Disproportionate pain, swelling, colour change, temperature asymmetry, allodynia, stiffness disproportionate to surgery
- Prevention and management
- Prevention: early mobilisation, adequate analgesia, patient education. Management: gabapentin or pregabalin, hand therapy, mirror therapy; specialist pain clinic if refractory
- Incidence
- 15-25 percent at 10 years
- Recognition
- Progressive dorsal wrist pain, reduced grip, radiographic narrowing of the capitate-radius joint, osteophytes
- Prevention and management
- Prevention: strict MRI selection (intact capitate cartilage); avoid PRC if any midcarpal arthritis. Management: conversion to total wrist fusion if symptomatic
- Incidence
- 1-3 percent
- Recognition
- Erythema, warmth, discharge at the incision within 2 weeks
- Prevention and management
- Prevention: sterile technique, perioperative antibiotics. Management: wound swab and oral antibiotics; if deep, washout and IV antibiotics
If joint levelling fails. Persistent or worsening pain more than 6 months after a united osteotomy, with progressive carpal height loss or lunate fragmentation, means the disease has progressed despite offloading (10-20 percent of cases — a property of the disease, not necessarily a technical error). Confirm osteotomy union on CT (to exclude nonunion as the cause of pain), assess the current Lichtman stage, and MRI the capitate head: if IIIA or early IIIB with intact capitate cartilage, move to STT fusion or PRC; if IIIB with capitate chondrosis or stage IV, proceed to total wrist fusion.
Viva & Exam Focus
VARIANCEVARIANCE — surgical decision framework
Stage and ulnar variance drive every choice in Kienbock disease.
LICHTMANLICHTMAN — staging and treatment algorithm
The Lichtman classification (revised 2002) guides management from conservative treatment through joint-preserving procedures to salvage.
The trap: Measuring ulnar variance on a PA wrist radiograph taken in pronation or supination — ulnar variance shifts by up to 2 mm with forearm rotation. The fix: Measure on a standardised PA wrist taken with the shoulder abducted 90 degrees, elbow flexed 90 degrees, and the forearm in neutral rotation. Compare with the contralateral side; a difference of 2 mm or greater is significant. Negative variance means the ulna is shorter than the radius at the DRUJ — the critical measurement that determines whether radial shortening is appropriate.
The trap: Operating on a stage I patient with a salvage procedure (PRC or fusion) when joint-preserving options (joint levelling or revascularisation) are still appropriate. The fix: Stages I and IIA are treated conservatively or with joint levelling or revascularisation. Stage IIIA still accepts joint levelling. Only at stage IIIB (carpal collapse with fixed scaphoid rotation) does the algorithm branch to motion-sparing salvage (STT fusion or PRC). Stage IV requires total wrist fusion or arthroplasty. Staging too aggressively sacrifices motion that could have been preserved.
The trap: Shortening the radius by more than the measured ulnar variance plus 2 mm — this overloads the DRUJ and causes ulnar-sided wrist pain, radioulnar impingement and progressive DRUJ arthritis. The fix: Calculate the exact shortening preoperatively; never shorten by more than 4 mm total. Confirm the achieved shortening on intraoperative fluoroscopy before final fixation. If the DRUJ is already symptomatic or arthritic, radial shortening is contraindicated — use capitate shortening instead.
The trap: Performing a proximal row carpectomy when the capitate head or the lunate fossa of the radius has chondrosis — the capitate-radius articulation will fail rapidly. The fix: MRI is mandatory before PRC. If the capitate head cartilage is intact, PRC gives reliable outcomes; if capitate head wear is present, perform total wrist fusion or arthroplasty instead. Direct visual inspection of the capitate at surgery is the final check — if chondrosis is seen, abandon PRC.
The trap: The posterior interosseous nerve lies on the floor of the fourth extensor compartment and can be transected, crushed, or entrapped in hardware, causing a painful neuroma. The fix: Identify the PIN as the dorsal retinaculum is elevated — it runs with the posterior interosseous artery on the dorsal capsule. Either protect it with a vessel loop, or perform a prophylactic PIN neurectomy at the distal-radius level. Never leave it as an unidentified structure crossing the operative field.
The trap: Choosing STT fusion for a patient whose primary complaint is radiocarpal pain — STT fusion stabilises the proximal row but does not address radiocarpal arthritis. The fix: STT and scaphocapitate fusion are for isolated carpal collapse without radiocarpal arthritis. PRC is preferred when there is midcarpal arthritis or when a simpler, nonunion-free procedure is wanted. PRC gives more flexion-extension (about 100 degrees versus about 60 degrees for STT fusion) but loses carpal height; STT fusion preserves height but reduces radial deviation.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old right-handed male carpenter presents with a 12-month history of insidious right wrist pain. He reports pain with heavy gripping and pushing. Examination reveals tenderness over the dorsum of the wrist, reduced grip strength, and pain on axial loading. PA radiograph in neutral rotation shows a sclerotic lunate with a linear fracture line, carpal height preserved, scapholunate angle 48 degrees, and ulnar variance minus 2 mm. MRI shows low T1 signal in the lunate with preserved lunate morphology. What is the diagnosis, stage, and surgical management?”
“A 45-year-old woman presents with long-standing right wrist pain. PA radiograph shows a collapsed and fragmented lunate, carpal height ratio 0.48, scapholunate angle 68 degrees, and mild narrowing of the radioscaphoid joint. Ulnar variance is neutral. MRI shows low T1 signal throughout the lunate with capitate head cartilage intact. What is the Lichtman stage and what are the surgical options?”
“A 28-year-old woman with Kienbock disease underwent a radial shortening osteotomy 18 months ago. The osteotomy united uneventfully. She now presents with worsening wrist pain, reduced grip, and stiffness. Radiographs show the lunate has collapsed further, the carpal height ratio is 0.50, and the scapholunate angle is 65 degrees. What is happening and what is the next step?”
Diagnosis and staging
- Kienbock disease is avascular necrosis of the lunate; dominant wrist of young manual labourers (20-40 years); multifactorial: negative ulnar variance, repetitive loading, tenuous blood supply
- Lichtman staging (revised 2002): I = MRI signal change only; IIA = fracture, no collapse; IIIA = sclerosis/fragmentation, no height loss; IIIB = collapse, fixed scaphoid flexion (SL angle greater than 60 degrees), carpal height ratio less than 0.54; IV = pancarpal arthritis
- Ulnar variance is measured on a PA wrist in neutral rotation (shoulder abducted 90, elbow flexed 90) — variance shifts up to 2 mm with forearm rotation
- MRI: low T1 signal in the lunate confirms AVN; also assess capitate head cartilage (critical for PRC planning) and any radiocarpal or midcarpal arthritis
Surgical decision algorithm
- Stage I-IIA (negative variance): radial shortening osteotomy 2-4 mm, dorsal plate fixation
- Stage I-IIA (neutral or positive variance): capitate shortening osteotomy or revascularisation
- Stage IIIA (negative variance): radial shortening still appropriate — the last stage for joint levelling
- Stage IIIA (neutral or positive): capitate shortening or revascularisation
- Stage IIIB (any variance): STT fusion, scaphocapitate fusion, or PRC — joint levelling no longer works
- Stage IV (any variance): total wrist fusion or total wrist arthroplasty (older, low-demand patients only)
Radial shortening osteotomy
- Indication: Lichtman I-IIIA, ulnar-negative variance
- Shortening amount: equal to the ulnar variance (target neutral to plus 1 mm postoperatively)
- Maximum shortening: never more than ulnar variance plus 2 mm — excessive shortening causes DRUJ overload
- Fixation: 3.5 mm LC-DCP or locking plate dorsally, osteotomy 2-3 cm proximal to the radiocarpal joint
- Union rate greater than 95 percent; cast 4-6 weeks; mobilise at 4-6 weeks
Capitate shortening osteotomy
- Indication: Lichtman I-IIIA, ulnar-neutral or positive variance
- Shortening amount: 2-3 mm at the capitate waist
- Fixation: headless compression screw (Acutrak or Herbert) intramedullary
- Key advantage: does not disturb the DRUJ — preferred when radial shortening is contraindicated
- Nonunion rate 5-10 percent (higher than radial shortening)
Motion-sparing salvage (stage IIIB)
- PRC: remove scaphoid, lunate, triquetrum; capitate articulates with radius; no nonunion risk; preserves 60-70 percent grip and 50-60 degrees flexion-extension; REQUIRES intact capitate cartilage on MRI
- STT fusion: stabilises the carpal row, preserves carpal height; nonunion 5-15 percent; reduces radial deviation
- PRC vs STT fusion: PRC gives more motion, no nonunion risk; STT fusion preserves height but less motion; choice depends on surgeon preference and specific pathology
Total wrist salvage (stage IV)
- Total wrist fusion: gold standard salvage; pain relief greater than 90 percent; grip 80-90 percent of contralateral; zero wrist motion; plate from radius to third metacarpal
- Total wrist arthroplasty: motion-preserving; reserved for low-demand patients older than 50 years; limited implant longevity; revision to fusion is complex but possible
Dorsal approach — key steps
- Longitudinal incision centred on the Lister tubercle
- Release the EPL from the third compartment, retract radially to expose the capsule
- Identify the PIN on the floor of the fourth compartment — protect or deliberately neurectomise
- Capsulotomy exposes the radiocarpal and midcarpal joints
Danger zones and exam traps
- DRUJ overload: shorten the radius no more than ulnar variance plus 2 mm — irreversible ulnar-sided impingement
- PRC without MRI: capitate head chondrosis causes rapid postoperative failure — MRI is non-negotiable
- Wrong ulnar variance measurement: must use a PA wrist in neutral rotation; pronation or supination changes the value by up to 2 mm
- Stage progression after a successful osteotomy: 10-20 percent progress despite union — counsel the patient preoperatively
- Total wrist fusion in a young patient: preferred over arthroplasty due to implant longevity; arthroplasty is for older, low-demand patients
Background & Evidence
Epidemiology. Kienbock disease most often affects the dominant wrist of men aged 20-40 who perform manual labour. Bilateral involvement occurs in approximately 2-5 percent of patients, and is more common with systemic risk factors such as steroid use, sickle cell disease and systemic lupus erythematosus. Pathoanatomy — the lunate blood supply. The lunate receives blood through dorsal and volar vascular pedicles entering via its ligamentous attachments. This anatomy explains why the disease occurs and underpins revascularisation procedures. - Dorsal vessels (the primary supply in 70-80 percent of lunates): enter through the dorsal radiocarpal and intercarpal ligaments, arising from the radial artery via dorsal branches and the anterior interosseous artery, and supply about two-thirds to three-quarters of the bone. They are the most vulnerable to disruption in dorsal fracture patterns and surgical dissection.
- Volar vessels (supplemental): enter through the radiolunotriquetral and volar radiocarpal ligaments and supply the volar pole; in a minority of lunates they are the sole supply.
- Viegas (1999) vascular types: Type I — a single vessel (about 20 percent of lunates, the highest AVN risk); Type II — two vessels with dorsal dominance (about 60 percent); Type III — multiple dorsal and volar vessels (about 20 percent, the lowest risk). A Type I lunate is the most vulnerable to AVN after injury, and repetitive loading in an ulnar-negative wrist concentrates force on the radial side of the lunate, microfracturing trabeculae and disrupting the dorsal vessels. Why the operation works — DRUJ biomechanics. Ulnar variance (the relative length of the ulna and radius at the DRUJ) determines load distribution across the wrist. In an ulnar-negative wrist the ulna is shorter and a greater proportion of axial load falls on the lunate through the radius. Radial shortening corrects this by shortening the radius and equalising load between radius and ulna; excessive shortening reverses the imbalance, overloading the ulnar side of the DRUJ. The Lichtman classification (revised 2002, MRI-enhanced) remains the framework that drives management:
- Radiographic features
- Normal radiographs; MRI signal change only (low T1)
- Typical management
- Conservative — immobilise, activity modification, NSAIDs; consider joint levelling if progressive
- Radiographic features
- Linear or compression fracture of the lunate; no carpal collapse
- Typical management
- Joint levelling (radial shortening if ulnar-negative; capitate shortening or revascularisation if neutral or positive)
- Radiographic features
- Lunate sclerosis and fragmentation; no carpal height loss
- Typical management
- Joint levelling still appropriate — the last stage for joint-preserving osteotomies
- Radiographic features
- Lunate collapse with fixed scaphoid flexion (SL angle greater than 60 degrees); carpal height ratio less than 0.54
- Typical management
- Motion-sparing salvage — STT or scaphocapitate fusion, or PRC
- Radiographic features
- Pancarpal degenerative arthritis
- Typical management
- Total wrist fusion or arthroplasty
Key evidence. Radial shortening is the most studied procedure: Weiss et al. (1991) reported 94 percent good-to-excellent results in 36 wrists at an average 5-year follow-up, and a systematic review (Shin et al., 2018) found radial osteotomy superior to non-operative management for symptomatic disease. For neutral or positive variance, Bain et al. (2020) described a simplified single-cut single-screw capitate-shortening technique that offloads the lunate without disturbing the DRUJ. Vascularised bone grafting shows better radiographic revascularisation than non-operative care in early disease (Park et al., 2023), especially when combined with joint levelling. For salvage, PRC gives reliable long-term relief when the capitate cartilage is intact (Croog and Stern, 2008, average 10-year follow-up), and STT fusion preserves carpal height in stage IIIB (Minami et al., 2003). The modern reference (Lichtman and Pientka, 2025) integrates the osseous Lichtman stage with perfusion (Schmitt) and articular cartilage (Bain) classification systems.
References
Kienbock Disease: Recent Advances in Understanding and Management
- Comprehensive review by the originator of the Lichtman classification, integrating advances in perfusion-based classification and arthroscopic cartilage assessment
- Updated treatment algorithm combining osseous (Lichtman), perfusion (Schmitt), and articular cartilage (Bain) classification systems
- Summarised evidence for joint levelling, revascularisation, intercarpal fusion, proximal row carpectomy, and salvage procedures across all stages
Radial shortening for Kienbock disease
- Landmark series reporting outcomes of radial shortening osteotomy for Kienbock disease with long-term follow-up
- Demonstrated reliable pain relief and wrist motion preservation in early and intermediate Lichtman stages with negative ulnar variance
- Established radial shortening as the primary joint-levelling procedure for ulnar-negative wrists
Comparison of Long-Term Outcomes of Radial Osteotomy and Nonoperative Treatment for Kienbock Disease: A Systematic Review
- Systematic review comparing radial osteotomy with nonoperative treatment for Kienbock disease, evaluating long-term pain relief and functional outcomes
- Found that radial osteotomy provided superior outcomes compared with nonoperative management in patients with symptomatic disease
- Highlighted that outcomes correlate with Lichtman stage and adequacy of ulnar variance correction
Single-Cut Single-Screw Capitate-Shortening Osteotomy for Kienbock Disease
- Described a simplified single-cut single-screw technique for capitate shortening osteotomy in Kienbock disease
- Achieved lunate offloading without disturbing the distal radioulnar joint, suitable for neutral or positive ulnar variance
- Reported reliable pain relief and maintained wrist motion with low complication rates
Comparison of Long-term Outcomes between Nonoperative Treatment and Vascularized Bone Graft for Kienbock Disease: A Systematic Review and Single-Arm Meta-Analysis
- Systematic review and meta-analysis comparing vascularized bone grafting with nonoperative treatment for Kienbock disease
- Vascularized bone grafting demonstrated better radiographic revascularisation and clinical outcomes than nonoperative management in early-stage disease
- Outcomes were best when revascularisation was combined with joint-levelling procedures (radial or capitate shortening)
Proximal row carpectomy for advanced Kienbock disease: average 10-year follow-up
- Series of proximal row carpectomies performed for Kienbock disease at Lichtman stage III and IV with average 10-year follow-up
- Demonstrated reliable pain relief and functional improvement, with most patients maintaining useful grip strength and wrist motion
- Emphasised that intact capitate head cartilage on MRI is a prerequisite for successful PRC outcomes
Scaphotrapeziotrapezoid fusion: long-term follow-up study
- Long-term follow-up of scaphotrapeziotrapezoid (STT) fusion for Kienbock disease with carpal collapse
- Demonstrated that STT fusion stabilises the proximal carpal row, reduces pain, and preserves carpal height in Lichtman stage IIIB
- Reported satisfactory outcomes in the majority of patients, though radial deviation is predictably reduced