3rd-4th Compartment Interval | Lister Tubercle Landmark | EPL Transposition | Dorsal Buttress Plating
- Indications: dorsal Barton (absolute), dorsally comminuted Colles (AO/OTA 23-A3 / 23-C3), scaphoid proximal-pole ORIF, chronic scapholunate ligament reconstruction, and the wrist arthroscopy 3-4 portal.
- Interval used: the 3rd compartment (EPL) and 4th compartment (EDC/EIP) — both innervated by the posterior interosseous nerve (PIN), so NOT a true internervous plane but a safe tendon interval with minimal morbidity.
- Key landmark — Lister tubercle: the palpable dorsal prominence between the 2nd and 3rd compartments; the EPL uses it as a pulley. The dorsal watershed line lies 15-20mm proximal to it, and a dorsal plate MUST sit proximal to that line.
- EPL transposition — CRITICAL: lift the EPL out of the 3rd compartment during exposure and do NOT replace it; this prevents scarring, friction over Lister tubercle, and re-entrapment that predispose to attrition rupture.
- Superficial radial nerve (SRN) — at risk: its dorsoradial sensory branches cross the field over the 1st/2nd compartments; injury causes dorsal thumb and first web-space numbness or a painful neuroma.
- Fixation strategy: a low-profile dorsal locking plate placed proximal to the watershed line, supplemental K-wires for metaphyseal comminution, and meticulous fluoroscopic screw-length checking.
When & Why
What it exposes. The dorsal approach gives direct access to the dorsal distal radius — the dorsal cortex, the dorsal articular rim, and the dorsal capsule — and is the exposure of choice whenever the pathology is dorsal. It is built around Lister's tubercle, the palpable dorsal prominence between the 2nd and 3rd extensor compartments, which is the single landmark that makes the whole approach navigable. Why dorsal (and not volar). Volar locking-plate fixation has become the workhorse for most distal radius fractures because it controls volar tilt with a fixed-angle construct and sits under a thick soft-tissue envelope. But a volar plate cannot buttress a dorsal cortex, and several patterns genuinely demand a dorsal exposure: a dorsal Barton shear fracture (the carpus follows the dorsal rim and redislocates without a dorsal buttress), severe dorsal comminution (AO/OTA 23-A3 or 23-C3) where the dorsal wall will collapse, and dorsal die-punch impaction. The dorsal route is also the natural corridor for scaphoid proximal-pole ORIF, chronic scapholunate ligament reconstruction, and the 3-4 wrist arthroscopy portal. Indications - Dorsal Barton fracture — shear fracture of the dorsal rim with radiocarpal subluxation (the carpus follows the dorsal fragment dorsally). This is an absolute indication for ORIF: closed reduction cannot hold it, and a dorsal buttress plate is required. It represents 5-10% of distal radius fractures and follows a high-energy fall on a flexed wrist.
- Dorsally displaced, comminuted Colles fractures — when there is significant dorsal comminution, metaphyseal impaction, or articular step-off requiring direct dorsal visualisation. AO/OTA 23-A3 (complete metaphyseal comminution) and 23-C3 (complete articular with metaphyseal comminution) patterns often need a dorsal plate because a volar plate cannot buttress the dorsal cortex.
- Scaphoid nonunion ORIF (dorsal approach) — proximal-pole and waist nonunions with DISI deformity are approached dorsally for screw fixation and grafting; the dorsal approach gives direct access to the proximal pole and a dorsal-to-volar screw trajectory that respects the dorsal vascular supply (the dorsal carpal branch of the radial artery enters at the waist).
- Chronic scapholunate ligament reconstruction — static SL dissociation (gap greater than 3mm on AP, DISI on lateral) needs access to the dorsal SL ligament (the strongest component) for tenodesis or bone-ligament-bone reconstruction.
- Wrist arthroscopy portal placement — the 3-4 portal (between the 3rd and 4th compartments, 1cm distal to Lister's tubercle in line with the radial border of the 3rd metacarpal) is the primary arthroscopy portal. Relative indications include reduction of a volar lunate dislocation when closed reduction fails (acute carpal tunnel syndrome complicates 30-40% of lunate dislocations, so a concomitant volar release is common), revision of failed volar plating with dorsal collapse, and high-energy radiocarpal fracture-dislocation. ORIF thresholds (any approach). Operative fixation is generally supported for dorsal angulation greater than 10 degrees, radial shortening greater than 3mm, intra-articular step-off greater than 2mm, or loss of reduction after an acceptable closed reduction. Contraindications - Absolute: active infection (cellulitis, abscess, osteomyelitis) over the dorsal wrist, and inadequate soft-tissue coverage (severe open injuries are spanned by an external fixator and plated staged once the soft tissues heal).
- Relative: low-demand elderly patients with minimally displaced extra-articular fractures — multiple trials in patients over 65 (including the widely cited Arora volar-plate-versus-cast study) show that despite better radiographic alignment with fixation, patient-reported outcomes (DASH/PRWE) are similar to non-operative care by one year, supporting shared decision-making. Severe comorbidity also tempers the decision: uncontrolled diabetes (HbA1c greater than 8%) and active smoking (greater than 10 cigarettes/day, which roughly triples nonunion risk) raise wound and infection rates; a prior CRPS history carries a 10-15% recurrence risk; and a very thin dorsal envelope (BMI less than 18) or rheumatoid arthritis raises extensor-tendon irritation from dorsal hardware (15-20% versus 2-5%), favouring a volar plate. Position & landmarks. Supine, arm on a radiolucent hand table, upper-arm tourniquet at about 250mmHg. The shoulder is abducted 90 degrees and the elbow flexed 90 degrees with the forearm in neutral rotation. Palpate and mark Lister's tubercle (between 2nd and 3rd compartments), the radial styloid, the course of the superficial radial nerve branches on the dorsoradial side, and the planned longitudinal incision directly over the tubercle. Bilateral wrist radiographs of the uninjured side are a useful template for radial height and inclination.
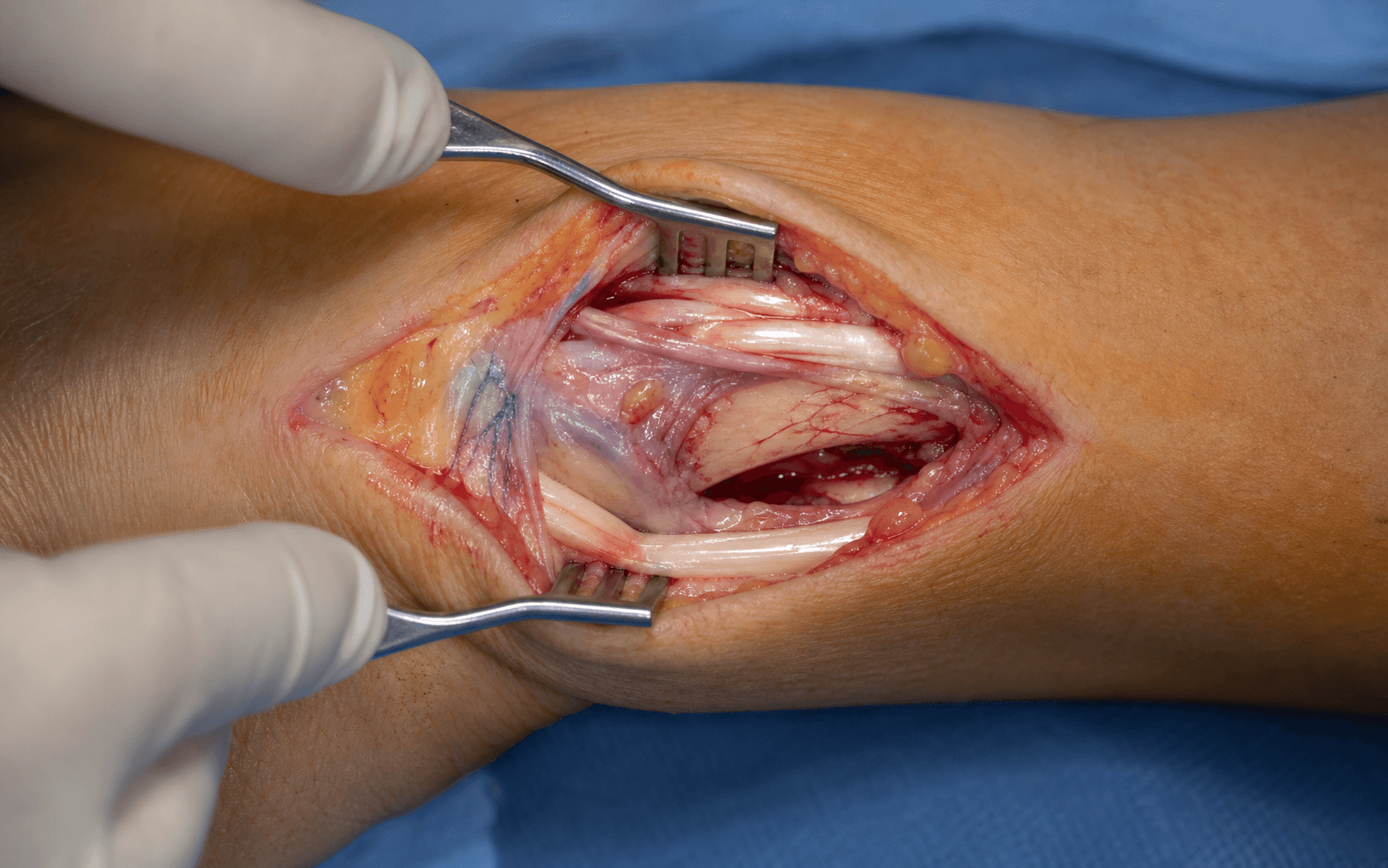
The Exposure
Work straight down over Lister's tubercle, protect the superficial radial nerve on the radial side, open the 3rd compartment and transpose the EPL, then capsulotomise to the dorsal radius. The 3rd-4th compartment interval is the heart of the approach.
Exposure sequence
- Supine on a radiolucent hand table; general or regional anaesthesia (an axillary or supraclavicular block gives 12-18 hours of analgesia and reduces opioid use).
- Shoulder abducted 90 degrees, elbow flexed 90 degrees, forearm in neutral rotation; upper-arm tourniquet inflated to 250mmHg (or 100mmHg above systolic) after Esmarch exsanguination. Keep ischaemia time under 90 minutes.
- C-arm opposite the surgeon; the surgeon stands on the radial side. Display AP, lateral and oblique films (and a CT if intra-articular) on the OR monitor.
- A longitudinal incision over the dorsum of the wrist directly over Lister's tubercle, beginning 4-5cm proximal to the tubercle and extending 2-3cm distally (total 6-8cm).
- The incision lies over the 3rd compartment (EPL), between the 2nd compartment (ECRL/ECRB) radially and the 4th compartment (EDC/EIP) ulnarly. Staying centred — not too radial — keeps the incision off the superficial radial nerve branches.
- Incise skin and subcutaneous tissue sharply; ligate or coagulate crossing dorsal veins.
- Use blunt spreading in the subcutaneous fat to identify the superficial radial nerve branches — white cords 1-2mm in diameter running obliquely from radial to ulnar across the field. Gently retract them with vessel loops; do not stretch or transect them.
- Identify the 3rd compartment (the solitary EPL tendon running around the ulnar side of Lister's tubercle) and the 4th compartment (EDC/EIP) ulnar to it.
- Incise the retinaculum longitudinally over the 3rd compartment along the full length of the wound and elevate the radial leaf off the EPL. The 3rd-4th compartment interval is the window to the bone.
- Free the EPL proximally and distally with a right-angle clamp or tenotomy scissors, lift it out of the 3rd compartment, and transpose it radially (superficial to the 2nd compartment).
- The EPL is left transposed and NOT replaced at closure — this prevents adhesions to the periosteum, reduces friction over Lister's tubercle, and removes the re-entrapment that predisposes to attrition rupture. The floor of the 3rd compartment (distal radius periosteum) now forms a clean window to the fracture.
- Incise the dorsal wrist capsule longitudinally over the fracture (4-5cm); elevate capsular flaps radially and ulnarly with a periosteal elevator.
- The pronator quadratus may be partially lifted off the volar cortex if volar visualisation is needed (radial-to-ulnar), but extensive stripping devascularises fragments and is avoided. Dorsal comminution and metaphyseal impaction are now directly visible.
- Restore length with longitudinal traction, restore volar tilt with a volar-translation force, and reduce any articular step-off by direct pressure.
- For reluctant fragments, use 0.062-inch K-wires as joysticks in the metaphyseal pieces. Confirm articular congruity (step-off less than 2mm, ideally under 1mm) on AP, lateral and oblique fluoroscopy. A volar die-punch fragment may need a volar capsulotomy from within this exposure or conversion to a volar approach (see Viva scenarios).
- Apply a low-profile dorsal locking plate contoured to the dorsal radius, its distal end 2-3mm proximal to the dorsal articular rim and the whole plate 15-20mm proximal to Lister's tubercle (proximal to the watershed line) to avoid extensor irritation.
- Fix the shaft first (3.5mm cortical screws in oblong holes), then place 4-6 divergent 2.4/2.7mm locking screws into the subchondral bone, stopping 2-3mm short of the articular surface. Countersink any prominent plate edge into a small bony depression. Fill a large metaphyseal void with calcium phosphate cement or allograft chips.
- Final fluoroscopy confirms radial height (10-12mm), volar tilt (11 degrees or neutral), inclination (20-23 degrees), step-off under 2mm, and no intra-articular or volar screw penetration.
- Repair the capsule with 2-0 Vicryl; leave the EPL transposed radially; repair the retinaculum loosely over the 4th compartment (leaving room for the EPL); close subcutaneous tissue (3-0 Vicryl) and skin (4-0 nylon mattress or 4-0 Monocryl subcuticular). Apply a volar resting splint with the wrist in 20 degrees of extension.
The EPL runs around Lister's tubercle in the 3rd compartment with a tenuous watershed blood supply. Closed EPL rupture complicates roughly 0.2-5% of distal radius fractures (up to 12.5% in some series; Kunes 2022) and, paradoxically, is classically described after NON- or minimally displaced fractures: the intact 3rd compartment seals the haematoma, raising pressure and causing ischaemia, while sharp dorsal fragments add friction. Transpose the EPL out of the 3rd compartment and never replace it, ensure no dorsal screw prominence, and counsel patients to report loss of thumb IP extension.
The dorsoradial sensory branches cross the field over the 1st/2nd compartments. Transection causes dorsal thumb and first-web numbness or a painful neuroma — a source of dissatisfaction despite a well-fixed fracture. Centre the incision on Lister's tubercle (not too radial), dissect bluntly in the subcutaneous plane, identify and loop the branches with vessel loops, and keep them out of the skin sutures at closure.
Volar cortex penetration of even 1-2mm risks flexor pollicis longus rupture (5-10% in some series). Obtain a true lateral (volar and dorsal cortices superimposed), measure each screw before insertion, start distal holes short, and check EVERY screw individually — one prominent screw usually means a systematic length error.
A volar splint is worn for 10-14 days until suture removal, then a removable brace. Finger and thumb motion starts on day 1; wrist motion at 2-3 weeks. Radiographs at 2, 6 and 12 weeks monitor union (expected at 6-8 weeks for extra-articular, 8-12 weeks for intra-articular fractures). Grip strengthening begins at 6 weeks and full activity at 12 weeks; heavy manual work or contact sport at 3-4 months. Remove the plate only for symptomatic tenosynovitis once united — not routinely.
Dangers & Extensions
Structures at risk, by layer
- Why it is at risk
- Dorsoradial sensory branches cross the field over the 1st/2nd compartments; transection causes a painful neuroma and dorsal thumb/web numbness
- How to protect it
- Centre the incision on Lister (not too radial); blunt subcutaneous dissection; identify and loop branches with vessel loops
- Why it is at risk
- Runs around Lister in the 3rd compartment with a tenuous watershed supply; prone to ischaemic/attrition rupture
- How to protect it
- Transpose out of the 3rd compartment radially and do NOT replace; avoid dorsal screw prominence and sharp dorsal fragments
- Why it is at risk
- Lie directly under the plate through a thin (2-3mm) dorsal envelope
- How to protect it
- Low-profile plate proximal to the watershed line; countersink edges; meticulous screw-length checking
- Why it is at risk
- Screws penetrating the volar cortex rub on FPL and the median nerve
- How to protect it
- Perfect lateral fluoroscopy; stop screws 2-3mm short of the volar cortex; check EVERY screw
Dorsal versus volar plating. Most distal radius fractures are better served by a volar plate, but the choice is driven by the fracture pattern. The dorsal route earns its place when the dorsal cortex needs a buttress or when the target is dorsal/carpal.
- Dorsal approach
- Dorsal Barton shear, severe dorsal comminution (AO 23-A3/C3), dorsal die-punch
- Volar approach
- Volarly displaced (Smith), volar Barton, most extra-articular fractures (~90% of DRF)
- Dorsal approach
- 3rd-4th compartment (EPL vs EDC/EIP), both PIN — not a true internervous plane
- Volar approach
- FCR (median) vs radial artery — a true internervous plane
- Dorsal approach
- EPL tendon (transpose), SRN branches
- Volar approach
- FPL tendon, median nerve, radial artery
- Dorsal approach
- Proximal to the watershed line (15-20mm from Lister); countersink
- Volar approach
- On or above the watershed line (Soong Zone 0-1)
- Dorsal approach
- Extensor tenosynovitis ~7.5%, rupture ~1.7% (Azzi 2017)
- Volar approach
- Flexor tenosynovitis ~4.5%, rupture ~1.5%; FPL rupture rises with Soong Zone 2
- Dorsal approach
- Thin (2-3mm); wound complications 5-8%; hardware prominence common
- Volar approach
- Thick (10-15mm); wound complications 1-2%; better hardware cover
Extensile options. The dorsal approach is extensile along the radius: extend proximally along the shaft for diaphyseal control, and distally toward the carpus for scapholunate and scaphoid work. The 3-4 arthroscopy portal is the same interval, made 1cm distal to Lister's tubercle in line with the radial border of the 3rd metacarpal. Closure. Dorsal capsule with 2-0 Vicryl; the EPL remains transposed radially and is not replaced; the retinaculum is repaired loosely over the 4th compartment leaving room for the transposed EPL; subcutaneous 3-0 Vicryl and skin with 4-0 nylon or 4-0 Monocryl; a volar resting splint holds the wrist in 20 degrees of extension. Complications. The dominant problems are tendon-related. EPL rupture (0.2-5%, ischaemia/friction) is reconstructed with an EIP-to-EPL transfer rather than primary repair. Extensor tenosynovitis (~7.5% versus ~4.5% volar; Azzi 2017) is limited by a low-profile plate above the watershed line and countersinking, and symptomatic cases settle with plate removal after union. FPL rupture from volar screw penetration may need an FDS transfer. SRN injury causes dorsal thumb/web numbness or a neuroma. Wound issues are commoner in diabetics and smokers because the dorsal envelope is thin. CRPS is mitigated with early motion and vitamin C 500mg daily for 50 days. Residual shortening or dorsal tilt causing a symptomatic malunion may need a corrective osteotomy, and an articular step-off greater than 2mm predicts post-traumatic arthritis (Knirk & Jupiter 1986).
Procedures Through This Approach
- Dorsal ORIF of scaphoid proximal-pole nonunion — direct access to the proximal pole with a dorsal-to-volar screw trajectory that respects the dorsal vascular supply.
- Scapholunate ligament reconstruction / dorsal capsulodesis — access to the dorsal SL ligament (the strongest component) for tenodesis or capsulodesis.
- Wrist arthrodesis — dorsal exposure of the radiocarpal and intercarpal joints for fusion.
- Dorsal buttress plating of dorsal Barton and severely comminuted Colles fractures.
- The 3-4 wrist arthroscopy portal and arthroscopy-assisted articular reduction.
Viva & Exam Focus
LISTERLISTER — the dorsal distal-radius exposure
COMPARTMENTSSIX COMPARTMENTS — dorsal extensor anatomy
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old woman sustains a displaced distal radius fracture (Colles pattern) treated with closed reduction and casting. At 6-week follow-up she cannot extend her thumb tip and cannot lift the thumb off a flat table, though the thumb MCP extends normally. What is the diagnosis and management?”
“During dorsal plating of a distal radius fracture, the lateral fluoroscopy view shows a screw tip protruding 3mm beyond the volar cortex. What are the risks and the intra-operative management?”
“Through a dorsal approach you cannot reduce a volar lunate-facet (die-punch) fragment — it remains volarly displaced despite traction. How do you address it?”
Indications — when to go dorsal
- Absolute: dorsal Barton fracture (dorsal rim shear with radiocarpal subluxation; 5-10 percent of DRF) — needs a dorsal buttress plate
- Relative: dorsally displaced Colles with severe dorsal comminution (AO/OTA 23-A3 or 23-C3) that a volar plate cannot buttress
- Alternative uses: scaphoid proximal-pole ORIF, chronic SL ligament reconstruction, wrist arthroscopy 3-4 portal, volar lunate dislocation reduction
- ORIF thresholds (any approach): dorsal angulation over 10 degrees, radial shortening over 3mm, articular step-off over 2mm, or loss of reduction after casting
Critical anatomy at risk
- EPL tendon — 3rd compartment around Lister; the most commonly ruptured extensor tendon (0.2-5 percent); transpose radially and do not replace
- Superficial radial nerve — dorsoradial branches over the 1st/2nd compartments; protect with blunt dissection and a non-radial incision
- Lister tubercle — dorsal prominence between 2nd/3rd compartments; the palpable landmark for incision and EPL identification
- Six extensor compartments — 1st APL/EPB, 2nd ECRL/ECRB, 3rd EPL, 4th EDC/EIP, 5th EDM, 6th ECU
- The PIN terminates 4-5cm proximal to the wrist in the floor of the 4th compartment — not at risk
Technique — key steps
- Position: supine, hand table, tourniquet 250mmHg, forearm neutral, ischaemia under 90 minutes
- Incision: longitudinal 6-8cm centred on Lister (4-5cm proximal, 2-3cm distal)
- Superficial: protect SRN branches with blunt dissection and vessel loops
- EPL transposition (critical): lift EPL out of the 3rd compartment, transpose radially, do not replace
- Capsulotomy: longitudinal over the fracture; expose the dorsal comminution
- Fixation: dorsal locking plate 15-20mm proximal to Lister (above the watershed); countersink; check every screw for volar penetration
- Closure: capsule 2-0 Vicryl; EPL left transposed; retinaculum loosely over the 4th compartment
Reduction goals — radiographic parameters
- Radial height 10-12mm; shortening over 2-3mm overloads the ulnocarpal joint (a 20-40 percent DRUJ pressure rise per mm)
- Volar tilt 11 degrees (neutral acceptable); dorsal tilt over 10 degrees raises radiocarpal pressure 40-50 percent
- Radial inclination 20-23 degrees ulnar slope
- Articular step-off under 2mm mandatory (Knirk & Jupiter: over 2mm = 91 percent arthritis); ideally under 1mm
- No volar screw penetration — even 1mm risks FPL rupture (5-10 percent)
Complications
- EPL rupture (0.2-5 percent, ischaemia/friction) — reconstruct with an EIP-to-EPL transfer
- Extensor tenosynovitis (~7.5 percent dorsal vs 4.5 percent volar; Azzi 2017) — low-profile plate above the watershed, countersink; remove after union if symptomatic
- FPL rupture from volar screw penetration — may need an FDS transfer
- SRN injury — dorsal thumb/web numbness or neuroma; prevent with blunt dissection
- Wound issues, CRPS (vitamin C 500mg for 50 days, early motion), malunion, post-traumatic arthritis
Evidence to quote
- Rozental 2009 (JBJS, RCT): volar locking-plate ORIF vs percutaneous fixation — faster early recovery, equivalent by 1 year
- Kunes 2022 (Hand, systematic review): EPL is the most commonly ruptured extensor tendon (0-12.5 percent); dorsal screw prominence and dorsal fragments drive it
- Azzi 2017 (PRS, systematic review, 6278 patients): rupture ~1.7 percent dorsal vs ~1.5 percent volar; tenosynovitis ~7.5 percent dorsal vs ~4.5 percent volar
- Knirk & Jupiter 1986 (JBJS): residual radiocarpal incongruity 91 percent arthritis vs 11 percent if congruous — basis for the 2mm threshold
- Pogue 1990 (JHS, cadaver): radial shortening (significant at 2mm) and angulation over 20 degrees alter radiocarpal contact pressure
Guidelines, registries & global practice
- Epidemiology: the distal radius is the most commonly fractured long bone in adults; bimodal — young (male, high-energy) and older (female, low-energy falls)
- AAOS (US): supports fixation for post-reduction shortening over ~3mm, dorsal tilt over ~10 degrees, or step/gap over ~2mm; similar 1-year patient-reported outcomes in older lower-demand patients
- NICE / BOA-BOAST (UK): early definitive management, prompt surgery when indicated, shared decision-making in the elderly
- AO Foundation: guides approach selection and watershed-line plate placement
- A fragility distal radius fracture is a sentinel event — refer to a fracture liaison service for bone-health assessment
- Rehabilitation: digital motion from day 1; light/sedentary work ~6-8 weeks; heavy manual work ~12-16 weeks once united
References
Volar Plate ORIF vs Percutaneous Fixation for Unstable Dorsally Displaced Distal Radius Fractures
- Prospective randomised trial of 45 patients with displaced, unstable dorsally displaced extra-articular or simple intra-articular distal radius fractures
- Volar locking plate ORIF with early mobilisation (n=23) versus closed reduction and percutaneous pin fixation/casting (n=22)
- ORIF group had significantly better DASH scores at 6, 9 and 12 weeks (e.g. DASH 27 vs 53 at 6 weeks, p less than 0.01) and earlier recovery of motion and strength
- By one year there was no significant difference in DASH between the two groups
- Fewer complications in the ORIF group (2 vs 6)
Extensor Tendon Injury After Distal Radius Plating - EPL Most Commonly Ruptured
- Systematic review of 90 studies on extensor tendon injury after volar locking plate fixation of distal radius fractures
- Reported incidence of extensor tendon rupture ranged from 0% to 12.5% across studies
- Extensor pollicis longus (EPL) was the most commonly ruptured extensor tendon
- Key intraoperative risk factors were dorsal screw prominence and protruding dorsal fracture fragments
- Management of established rupture is typically hardware removal plus tendon transfer or reconstruction rather than primary repair
Residual Radiocarpal Incongruity Predicts Post-Traumatic Arthritis
- Retrospective study of 43 intra-articular distal radius fractures in 40 young adults (mean age 27.6 years), mean follow-up 6.7 years
- Post-traumatic radiographic arthritis developed in 65% of fractures overall
- Of joints that healed with residual radiocarpal incongruity, 91% developed arthritis, versus only 11% of joints that healed congruously
- Accurate articular restoration was the single most important determinant of outcome
- A depressed die-punch fragment was anatomically reduced by closed means in only 49% and accounted for 75% of residual incongruities
Effects of Distal Radius Malunion on Wrist Joint Mechanics
- Cadaveric biomechanical study using pressure-sensitive film to measure radiocarpal contact areas and pressures with simulated distal radius malunions
- Radial shortening increased total contact area in the lunate fossa, becoming significant at 2mm of shortening
- Angulating the distal radius more than 20 degrees (dorsal or palmar) shifted the scaphoid and lunate high-pressure zones dorsally and concentrated the load
- Decreasing radial inclination shifted load distribution toward the lunate fossa and away from the scaphoid fossa
- Demonstrated that relatively modest malalignment measurably alters radiocarpal load distribution
Tendon Rupture and Tenosynovitis After Distal Radius Plating - Dorsal vs Volar
- Systematic review of 56 studies including 6278 patients reporting tendon complications after internal fixation of distal radius fractures
- Overall tendon-related adverse events occurred in 6.8% of patients
- Tendon rupture rate was 1.5% with volar plates and 1.7% with dorsal plates
- Tenosynovitis was more common with dorsal plates (7.5%) than volar plates (4.5%)
- Extensor digitorum communis rupture (1.3% vs 0.05%) and EPL tenosynovitis (1.1% vs 0.3%) were higher with dorsal than volar fixation