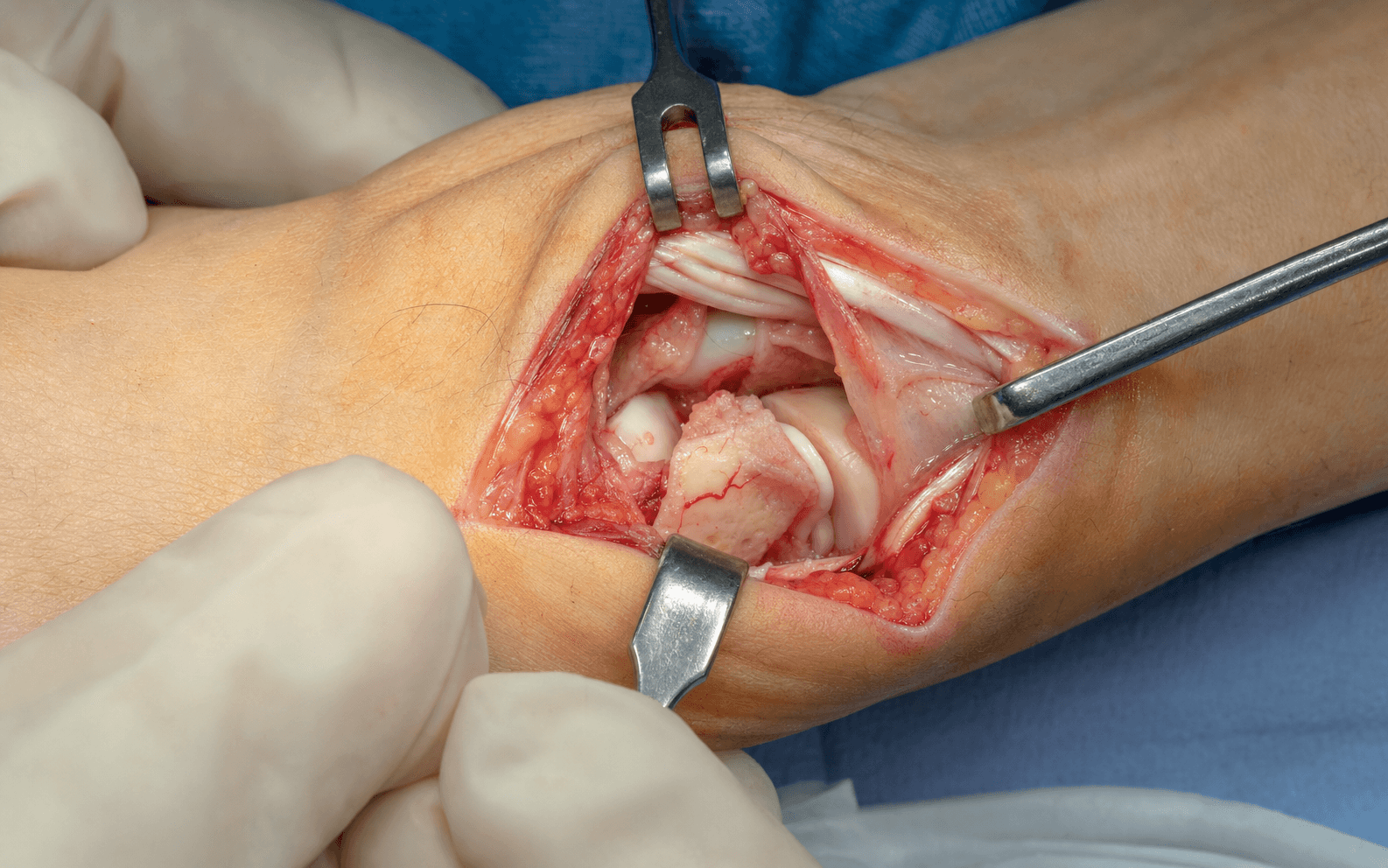
Dorsal approach through the 3rd/4th extensor compartment interval (EPL-EDC), over Lister's tubercle · advanced
- Proximal pole fractures (Herbert B3) carry a 30-50% AVN risk because the proximal pole has NO direct blood supply — it depends entirely on retrograde intraosseous flow from dorsal ridge vessels that the fracture interrupts.
- The dorsal approach is chosen SPECIFICALLY for the proximal pole: it gives direct visualization of the fragment and access to the dorsal radius vessels used for a 1-2 ICSRA vascularized graft.
- The internervous plane runs between EPL (3rd compartment) and EDC (4th compartment) — both posterior interosseous nerve, but different terminal branches.
- Wrist FLEXION of 10-20 degrees (not extension) opens the dorsal scaphoid space — the opposite of volar approach positioning.
- A retrograde screw (proximal-to-distal) is preferred when the fragment is greater than 25% of scaphoid length; an antegrade screw (distal-to-proximal) salvages a fragment too small for retrograde entry.
- Preserve the dorsal ridge blood supply with minimal periosteal stripping, and plan a 1-2 ICSRA vascularized graft when pre-op MRI shows AVN (T1 dark signal) — 88% union versus 47% with non-vascularized fixation (Merrell).
When & Why
Indication. Operative fixation of a proximal pole scaphoid fracture through a dorsal approach, chosen when the fragment must be visualized directly and/or a vascularized graft from the dorsal radius is planned. The absolute indications are: - Displaced proximal pole fracture (Herbert B3) — displacement greater than 1mm.
- Proximal pole non-union — failed conservative management or delayed presentation.
- Avascular necrosis (AVN) of the proximal pole — requires a 1-2 ICSRA vascularized bone graft plus fixation. Relative indications are a non-displaced proximal pole fracture in a high-demand patient (athlete, manual labourer), a failed volar approach to the proximal pole (inadequate visualization or fixation), and a proximal pole fracture with a scapholunate ligament injury that allows direct SL repair at the same sitting. Contraindications. Absolute: severe comminution where the fragment is too small for any fixation (salvage may be needed) and active infection (debride first). Relative: severe osteoporosis (consider K-wire augmentation), and a waist or distal pole fracture — for these the volar approach is preferred for better access and to avoid the stiffness the dorsal approach can cause. Pre-operative imaging is the whole plan. - Plain radiographs — PA, lateral, scaphoid view (PA with ulnar deviation) and oblique.
- CT — assess fragment size (can it accept a screw?), displacement, comminution and any arthritic change.
- MRI — essential to assess AVN; a dark T1 signal predicts the need for a vascularized graft. Decision algorithm. (1) Fragment size — greater than 25% of scaphoid length is required for a retrograde screw. (2) AVN — if present on MRI, plan a 1-2 ICSRA vascularized graft. (3) Screw trajectory — retrograde (proximal-to-distal) preferred; antegrade (distal-to-proximal) if the fragment is too small. (4) Graft — non-vascularized cancellous for non-union without AVN; vascularized ICSRA for AVN. Equipment checklist. Mini C-arm positioned for perfect scaphoid views BEFORE draping; a headless compression screw set (lengths 16-30mm); a 0.045-inch guidewire and cannulated drill bits; K-wires for provisional fixation and joystick control; microsurgical instruments if an ICSRA graft is planned; and a wrist bump for 10-20 degrees of flexion. Consent specifically for the 30-50% AVN risk despite optimal surgery, prolonged healing (12-20 weeks), superficial radial nerve numbness or neuroma, possible EPL irritation/rupture, non-union (15-20%), and the possible need for a bone graft (and, with AVN, a vascularized graft or later salvage). Setup. Supine, arm on a hand table, forearm pronated with the wrist flexed 10-20 degrees over a bump (flexion opens the dorsal scaphoid space and brings the proximal pole into the field — the opposite of the volar approach). Test the C-arm for perfect PA, lateral and oblique scaphoid views BEFORE draping. Loupe magnification is recommended for nerve and vessel identification.
The Operation
The goal: expose the proximal pole through the dorsal EPL-EDC interval over Lister's tubercle, preserve the dorsal ridge blood supply, reduce the fracture anatomically, and stabilize it with a headless compression screw — adding a vascularized 1-2 ICSRA graft when the fragment is avascular. The exposure (Steps 1-5 below) is the heart of the operation and is laid out in full.
Operative sequence
- Forearm pronated, wrist flexed 10-20 degrees over a bump — flexion opens the dorsal scaphoid space and brings the proximal pole into the field (extension closes the space and hides it).
- Test the C-arm for perfect PA, lateral and oblique scaphoid views BEFORE draping; the proximal pole can be hard to visualize on fluoroscopy.
- Mark Lister's tubercle — the palpable dorsal prominence on the distal radius separating the 3rd and 4th extensor compartments — and plan the incision centered on it.
- Review the imaging: proximal pole fracture location, displacement, and proximal fragment size.
- A 4cm longitudinal incision over Lister's tubercle, extending from the distal radius onto the carpus.
- Incise skin and subcutaneous tissue; identify and protect the superficial radial nerve (SRN) branches with vessel loops — they cross the dorsal wrist radially and are the structure most often injured (numbness or a painful neuroma / Wartenberg syndrome).
- Keep the incision centered on Lister's tubercle (ulnar to the main SRN branches) to minimize nerve risk.
- Identify the extensor retinaculum and incise it longitudinally between the 3rd compartment (EPL) and the 4th compartment (EDC) — this is an internervous plane (both posterior interosseous nerve, different terminal branches).
- Elevate retinacular flaps for later repair (repair prevents EPL bowstringing and delayed rupture).
- Identify the tendons: EPL is a single tendon in the 3rd compartment coursing around Lister's tubercle; EDC has four tendons (plus EIP) in the 4th compartment.
- Retract the EPL radially and the EDC tendons ulnarly to open the interval and expose the radiocarpal joint capsule over the proximal scaphoid.
- The capsule overlies the proximal scaphoid and the scapholunate interval; the dorsal radiocarpal (DRC) and dorsal intercarpal (DIC) ligaments are visible on the capsule and must be preserved.
- Use gentle retraction only on the EPL — no prolonged tension, to avoid ischemia and delayed rupture.
- Make a careful longitudinal capsulotomy over the proximal scaphoid, creating a radially-based capsular flap that preserves the DRC and DIC ligaments.
- CRITICAL: minimize periosteal stripping — the dorsal blood supply (70-80% of scaphoid vascularity) enters at the dorsal ridge (the junction of the waist and proximal pole). Use the elevator gently and remove only the soft tissue essential for visualization.
- Identify the fracture site; for a non-union, clear the fibrous tissue. Aggressive dorsal stripping devascularizes the fragment and causes AVN.
- Preserve the dorsal scapholunate ligament — keep the capsulotomy over the scaphoid and do not extend it ulnarly into the SL interval.
- Assess proximal pole fragment size: a fragment greater than 25% of scaphoid length can accept a retrograde screw; a smaller fragment may need an antegrade screw or K-wire fixation.
- Assess displacement, rotation and angulation; gently clean the fracture site of haematoma or fibrous tissue.
- If pre-op MRI shows AVN (T1 dark signal), plan a 1-2 ICSRA vascularized graft at this stage.
- Reduce the fracture anatomically using: a 0.9mm K-wire joystick in the proximal fragment for rotation/angulation control, wrist positioning, and direct manipulation with an elevator or dental pick.
- Confirm cortical alignment on all four sides with no articular step-off; provisionally stabilize with a K-wire if needed.
- Confirm reduction on fluoroscopy — PA (no displacement), lateral (scapholunate angle 30-60 degrees, no DISI) and oblique (cortical alignment).
- With the fracture reduced, place the guidewire at the CENTER of the proximal pole articular surface, aiming parallel to the scaphoid long axis toward the distal pole.
- Confirm the wire is central on ALL views — PA, lateral and oblique — before drilling. An eccentric wire causes malreduction or screw cutout.
- Measure length (typically 20-28mm), drill with the cannulated drill, and insert a headless compression screw.
- The screw head buries below the proximal pole articular cartilage and heals over — a proud head causes radiocarpal impingement. Advance until the trailing threads engage the distal fragment and compression is achieved.
- If the proximal fragment is too small for retrograde entry (less than 25% of scaphoid), place the guidewire from the waist directed proximally into the proximal pole.
- Ensure adequate proximal pole engagement (a minimum of 10-15mm of screw purchase).
- The screw head sits at the waist and must be countersunk below the dorsal cortex to avoid extensor tendon irritation; this trajectory is similar to the volar approach.
- Non-union WITHOUT AVN: non-vascularized cancellous graft from the distal radius, harvested through a window about 2cm proximal to the joint via the same incision, packed around the non-union after debridement to bleeding bone (pooled union around 88%, Pinder).
- Non-union WITH AVN (T1 dark on MRI): a vascularized graft is essential — non-vascularized graft fails. Use the 1-2 ICSRA pedicled graft: identify the artery between the 1st and 2nd (or 2nd and 3rd) compartments, harvest a rectangular bone block (about 8-10mm by 15-20mm) with the arterial pedicle attached, rotate it 90 degrees into the non-union defect, and fix it with a screw into the distal scaphoid. It provides both structural support and revascularization (88% union versus 47% with screw and non-vascularized inlay/wedge fixation in AVN — Merrell).
- Obtain final PA, lateral and oblique views and confirm: the screw is central on all views; the screw head is buried below cartilage (retrograde) or cortex (antegrade); the fracture is anatomically reduced with no gap; there is no joint penetration; and screw length and engagement are adequate.
- Test fracture stability under direct vision; revise now rather than accept suboptimal fixation. Document the intraoperative findings and images.
- Irrigate thoroughly. Repair the dorsal capsule with 3-0 absorbable suture (interrupted or figure-of-eight) to restore ligamentous stability and proprioception; confirm the SL ligament is intact.
- Repair the extensor retinaculum between the 3rd and 4th compartments — this is critical to prevent EPL bowstringing (loss of thumb extension power and risk of delayed rupture).
- Confirm the EPL glides smoothly through the 3rd compartment over Lister's tubercle without catching.
- Close subcutaneous tissue with 4-0 absorbable suture and skin with interrupted 4-0/5-0 nylon or a running subcuticular suture.
- Apply a well-padded thumb spica splint with the wrist neutral and the thumb in the column position, with the IP joint free for motion to prevent stiffness.
- Immobilization is longer than for waist fractures because of the proximal pole's tenuous blood supply.
The dorsal carpal branch of the radial artery enters the scaphoid at the dorsal ridge (junction of the waist and proximal pole) and supplies 70-80% of the bone and the entire proximal pole by retrograde intraosseous flow. Create a radially-based capsular flap, use the elevator only where necessary, and preserve every attachment at the dorsal ridge. Aggressive stripping is how a fixable fragment becomes avascular.
- Retrograde (proximal-to-distal)
- Fragment greater than 25% of scaphoid length
- Antegrade (distal-to-proximal)
- Fragment less than 25% — too small for retrograde entry
- Retrograde (proximal-to-distal)
- Center of the proximal pole articular surface, parallel to the scaphoid axis
- Antegrade (distal-to-proximal)
- From the waist, directed proximally into the proximal pole
- Retrograde (proximal-to-distal)
- Buries below the proximal pole cartilage (heals over)
- Antegrade (distal-to-proximal)
- At the waist — must be countersunk below the dorsal cortex
- Retrograde (proximal-to-distal)
- Best compression and purchase; direct visualization of the proximal pole
- Antegrade (distal-to-proximal)
- Larger entry point at the waist; salvages a small fragment
- Retrograde (proximal-to-distal)
- Proud head causes radiocarpal impingement
- Antegrade (distal-to-proximal)
- Inadequate proximal engagement (need 10-15mm) — pull-out and non-union
Before drilling, confirm the guidewire is central on PA, lateral AND oblique fluoroscopy. An eccentric wire is the commonest cause of malreduction and screw cutout. For a retrograde screw the wire starts at the centre of the proximal pole articular surface — counter-intuitive, but the headless screw buries completely below cartilage and heals over.
The dorsal approach uses wrist flexion of 10-20 degrees, the opposite of the volar approach. Flexion opens the dorsal scaphoid space and delivers the proximal pole into the field; extension closes the space and hides the fragment.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy & monitoring | |-------|--------|----------------|----------------------| | 1 | 0-2 weeks | Thumb spica splint, wrist neutral, thumb column, IP joint FREE | Elevation, ice, finger active range of motion; suture removal at 10-14 days | | 2 | 2-8 weeks | Thumb spica CAST (longer than for a waist fracture) | Light ADLs with the splint; X-rays at 2 and 6 weeks — expect minimal callus (intra-articular bone) | | 3 | 8-12 weeks | Removable thumb spica IF early union signs | Hand therapy AROM and gentle strengthening; CT often needed to confirm union | | 4 | 3-6 months | Splint for heavy tasks only | Progressive strengthening and proprioception; MRI at 3-6 months if AVN is suspected (T1 signal) | Proximal pole fractures take longer to unite than waist fractures — typically 12-20 weeks (versus 8-12 for the waist) — so immobilization is extended. Plain films are often inadequate to confirm proximal pole union, so a CT is frequently required. Expected outcomes with ORIF: union in 80-85% of acute fractures, 80-90% of contralateral wrist motion, 85-95% of contralateral grip at one year, and unrestricted activity at 4-6 months after solid union. Contact sports are deferred to 6 months (later than for waist fractures). Counsel the patient that AVN can still develop in 30-50% despite optimal surgery. Complications
- Recognition
- Dark T1 signal on MRI at 3-6 months, sclerosis on X-ray, persistent pain, delayed or non-union
- Prevention
- Minimal periosteal stripping, preserve the dorsal ridge supply, gentle handling, early diagnosis with pre-op MRI
- Management
- Asymptomatic: observe; with collapse: revision with a 1-2 ICSRA vascularized graft, or salvage (PRC, 4-corner fusion)
- Recognition
- Persistent fracture line at 12-16 weeks, no bridging callus on CT, snuffbox tenderness
- Prevention
- Anatomic reduction, adequate screw compression, bone grafting for established non-union, smoking cessation, 8-10 weeks immobilization
- Management
- Revision ORIF with graft — non-vascularized if no AVN, 1-2 ICSRA vascularized if AVN present; salvage if revision fails
- Recognition
- SL interval greater than 3mm on PA, DISI pattern on lateral (SL angle greater than 60 degrees), positive scaphoid shift test
- Prevention
- Capsulotomy OVER the scaphoid only, gentle manipulation, preserve the dorsal SL ligament, no instruments in the SL interval
- Management
- Acute: SL repair with suture anchor and temporary K-wire SL fixation; chronic: reconstruction versus salvage
- Recognition
- Painful/palpable screw head, loss of fixation with fragment migration, rare breakage
- Prevention
- Adequate countersinking, central wire placement, correct screw size, measure length twice
- Management
- Removal after union confirmed (4-6 months); revision fixation if cutout before union; observe asymptomatic breakage after union
- Recognition
- Numbness over the dorsal thumb/first web, painful Tinel sign, hypersensitivity, neuroma
- Prevention
- Identify SRN branches during the skin incision, protect with vessel loops, avoid cautery near the nerve, incision centered on Lister's tubercle
- Management
- Neuropraxia: observe 6-12 weeks with desensitization; persistent painful neuroma: excision and burial in pronator quadratus or bone
- Recognition
- Loss of thumb IP extension, palpable tendon gap, dropped thumb posture
- Prevention
- Gentle EPL retraction (no prolonged tension), preserve its blood supply, meticulous retinaculum repair, test EPL gliding
- Management
- EIP to EPL tendon transfer (most common); palmaris graft if EIP absent
- Recognition
- Progressive activity-related wrist pain, reduced grip and motion, arthritic X-ray (Stage 1 radial styloid, Stage 2 radioscaphoid, Stage 3 capitolunate)
- Prevention
- Anatomic reduction, achieve union, prevent malunion, early intervention for non-union
- Management
- Stage 1: radial styloidectomy; Stage 2: PRC versus 4-corner fusion; Stage 3: 4-corner fusion versus total wrist fusion; activity modification and NSAIDs
Viva & Exam Focus
DORSALDORSAL ACCESS
PROXIMALPROXIMAL POLE PRIORITIES
Each structure below can be injured during this approach — know its location and how to protect it.
Enters at the dorsal ridge (junction of the waist and proximal pole) via the dorsal carpal branch of the radial artery — 70-80% of supply. Protect with minimal periosteal stripping, a radially-based capsular flap, and preservation of all dorsal ridge attachments.
Terminal branches cross the dorsal wrist radially in the subcutaneous tissue. Identify them during the skin incision, protect with vessel loops, avoid cautery nearby, and keep the incision centered on Lister's tubercle.
The dorsal SL ligament is the strongest portion and the primary stabilizer. Keep the capsulotomy over the scaphoid — do not extend ulnarly into the SL interval — and avoid instruments there.
The EPL courses around Lister's tubercle with a sharp turn and is vulnerable to ischemia and rupture. Retract gently with no prolonged tension, preserve its blood supply, repair the retinaculum, and confirm smooth gliding.
The proximal scaphoid articulates with the radial fossa and is vulnerable to wire, screw and instrument penetration. Confirm wire position on fluoroscopy before drilling, measure length twice, and countersink the screw head below the articular surface.
Warn pre-operatively about the 30-50% AVN risk, the 12-20 week healing time, and the possible need for a vascularized graft or later salvage — even with optimal technique.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Why does the proximal pole have such high AVN risk and how does this influence your surgical approach?”
“What is the 1-2 ICSRA vascularized bone graft and when do you use it for proximal pole non-union?”
“Explain the differences between retrograde and antegrade screw fixation for proximal pole fractures — when would you use each technique?”
Indications
- Displaced proximal pole fracture (Herbert B3) — displacement greater than 1mm
- Proximal pole non-union; AVN of the proximal pole (needs a 1-2 ICSRA vascularized graft plus fixation)
- Non-displaced proximal pole in a high-demand patient; failed volar approach
- Contraindications: severe comminution (fragment too small), active infection, waist/distal pole (volar preferred)
Key anatomy
- Blood supply: dorsal vessels (70-80%) enter at the dorsal ridge; volar vessels (20-30%) at the tubercle/waist
- Proximal pole: NO direct supply — 100% retrograde intraosseous flow (30-50% AVN risk with fracture)
- Internervous plane: EPL (3rd compartment) versus EDC (4th compartment) — both PIN
- Lister's tubercle separates the 3rd and 4th compartments; dorsal SL ligament is the primary stabilizer
- 1-2 ICSRA: intercompartmental supraretinacular artery — source of the vascularized graft
Critical steps
- Position: forearm PRONATED, wrist FLEXION 10-20 degrees, C-arm BEFORE draping
- Approach: 4cm incision over Lister's tubercle, protect SRN, retinaculum between EPL (3rd) and EDC (4th)
- Exposure: retract EPL radial/EDC ulnar; capsulotomy over the scaphoid with MINIMAL periosteal stripping
- Fixation: retrograde if fragment greater than 25%, antegrade if less than 25%
- Guidewire central on PA, lateral and oblique; screw head buried below cartilage (retrograde) or cortex (antegrade)
- Graft: non-vascularized for non-union without AVN; 1-2 ICSRA vascularized if AVN (T1 dark MRI)
- Closure: repair capsule and retinaculum to prevent EPL bowstringing; confirm EPL glides
Danger zones
- Dorsal scaphoid blood supply at the dorsal ridge (70-80%) — minimal stripping
- Superficial radial nerve branches — protect with vessel loops
- Dorsal scapholunate ligament — capsulotomy over the scaphoid only
- EPL in the 3rd compartment — gentle retraction, repair the retinaculum
- Radiocarpal articular cartilage — fluoroscopy confirms no joint penetration
Technique pearls
- Wrist flexion (NOT extension) opens the dorsal space — opposite of the volar approach
- The retrograde screw head buries in proximal pole cartilage and heals over
- Central wire on ALL views before drilling prevents malreduction and cutout
- Greater than 25% scaphoid length needed for retrograde; less than 25% needs antegrade
- 1-2 ICSRA vascularized graft for confirmed AVN — 88% union versus 47% non-vascularized (Merrell)
- Proximal pole union takes 12-20 weeks (versus 8-12 for the waist); CT often needed to confirm union
Complications
- AVN (30-50%) — preserve the dorsal ridge supply; manage with ICSRA graft or salvage
- Non-union (15-20%) — revision with graft (vascularized if AVN)
- SL dissociation — capsulotomy over scaphoid only; repair if injured
- Hardware prominence/cutout; SRN injury (Wartenberg); EPL rupture (EIP-to-EPL transfer)
- SNAC arthritis — anatomic reduction prevents; salvage with PRC (early) or 4-corner/wrist fusion (late)
Post-op protocol
- Thumb spica splint 2 weeks, then cast to 8 weeks total; IP joint FREE
- LONGER than waist fractures due to tenuous proximal pole blood supply
- Radiographs at 2, 6, 12, 20 weeks; CT to confirm union; MRI at 3-6 months if AVN suspected
- Contact sports at 6 months after solid union (later than waist)
- Monitor for AVN even with optimal surgery (30-50% risk); hardware removal rarely needed (5-10%)
Background & Evidence
Epidemiology & natural history. The proximal pole is the unforgiving part of the scaphoid: proximal pole fractures carry the highest AVN rate (30-50%) and the highest non-union rate (15-20%, versus 5-10% for the waist). Acute proximal pole fractures unite in 80-85% with ORIF (versus 60-70% non-operative), over 12-20 weeks. Left untreated, a scaphoid non-union progresses to SNAC arthritis in around 95% of cases within 10 years (Kerluke) — which is why achieving union matters. Pathoanatomy — the scaphoid blood supply (the critical concept). The scaphoid's vascularity is the key to the whole topic. The dorsal vessels (70-80%) are branches of the radial artery that enter at the dorsal ridge (junction of the middle and proximal thirds) and supply the entire proximal pole by retrograde intraosseous flow. The volar vessels (20-30%) enter at the tubercle and waist and supply only the distal 20-30%. The proximal pole has no direct blood supply — it is entirely dependent on retrograde flow from the dorsal ridge, so a proximal pole fracture interrupts that flow and renders the fragment avascular. This is why a dorsal exposure must minimise stripping at the dorsal ridge, while still giving access to the very same dorsal radius vessels used for ICSRA grafting. The volar approach is the least traumatic to this supply, but it cannot reach the proximal pole directly — hence the dorsal approach for this fracture. Surgical anatomy. The 3rd extensor compartment contains the single EPL tendon, which courses around Lister's tubercle; the 4th compartment contains the four EDC tendons plus EIP. The dorsal capsule is reinforced by the dorsal radiocarpal (DRC) and dorsal intercarpal (DIC) ligaments, and the dorsal scapholunate ligament (the strongest part of the SL complex and the primary stabilizer) sits just ulnar to the proximal scaphoid. The superficial radial nerve crosses the dorsal wrist radially; the radial artery gives off the dorsal carpal branch that supplies the scaphoid; and the 1-2 and 2-3 intercompartmental supraretinacular arteries run on the dorsal radius between compartments and are the basis of the vascularized grafts. Classification — SNAC arthritis staging (the long-term consequence of a missed or failed proximal pole fracture):
- Radiographic features
- Arthritis confined to the radial styloid
- Typical management
- Radial styloidectomy; activity modification and NSAIDs
- Radiographic features
- Radioscaphoid arthritis (scaphoid fossa of the radius)
- Typical management
- Proximal row carpectomy versus 4-corner fusion
- Radiographic features
- Capitolunate arthritis (midcarpal involvement)
- Typical management
- 4-corner fusion versus total wrist fusion
Outcomes & comparative evidence. With ORIF, acute proximal pole fractures achieve 80-85% union over 12-20 weeks; functional recovery is around 80-90% of contralateral wrist motion (extension most affected by the dorsal approach) and 85-95% of contralateral grip at one year, with 80-85% good-to-excellent results at 5 years. The dorsal approach is recommended specifically for the proximal pole (better visualization and ICSRA access, at the cost of a higher stiffness rate than the volar approach). Biomechanically, retrograde and antegrade screws achieve equivalent compression with perfect central placement; the choice is driven by fragment size. For a confirmed AVN proximal fragment, a vascularized graft roughly doubles union compared with non-vascularized fixation (Merrell); across all non-unions the two graft types are broadly similar (Pinder), so the vascularized advantage is concentrated in AVN.
References
The vascularity of the scaphoid bone
- Cadaveric injection study (15 specimens): 70-80% of intraosseous vascularity and the ENTIRE proximal pole are supplied by radial artery branches entering through the dorsal ridge
- 20-30% of the bone (distal tuberosity region) is supplied by volar radial artery branches; the proximal pole receives no direct volar supply
- The authors noted the volar operative approach is least traumatic to the proximal pole blood supply
Treatment of scaphoid nonunions: quantitative meta-analysis of the literature
- Systematic quantitative meta-analysis of 36 eligible studies from 1,121 screened
- For AVN of the proximal fragment, union was 88% with a vascularized graft versus 47% with screw and inlay/wedge non-vascularized fixation
- For unstable non-unions, screw fixation with grafting (94%) was superior to K-wires and wedge grafting (77%); solid screw fixation did not require postoperative immobilization
Treatment of scaphoid nonunion: a systematic review of the existing evidence
- Systematic review with meta-analysis of proportions: 48 studies, 1,602 patients
- Vascularized and non-vascularized grafts had similar pooled union (92% versus 88%); distal radius and iliac crest grafts were comparable (89% versus 87%) but iliac crest had more donor-site complications
- Screw and K-wire fixation gave higher union (88% and 91%) than no fixation (79%); no surgical approach was statistically superior
A new vascularized bone graft for scaphoid nonunion (1-2 ICSRA)
- Original description of a consistent distally based vascularized graft from the dorsoradial distal radius (the 1-2 intercompartmental supraretinacular artery pedicle)
- Cadaveric latex-injection anatomy plus a clinical series of 11 long-standing non-unions treated with good results
- Offered shorter immobilization and higher union than conventional inlay grafting in this series
A capsular-based vascularized distal radius graft for proximal pole scaphoid pseudarthrosis
- 13 proximal pole non-unions (10 with AVN) treated with a capsular-based dorsal distal radius vascularized graft plus Herbert screw
- 10 of 13 overall and 8 of 10 AVN cases achieved solid union at a mean 19 months
- No donor-site morbidity; the technique avoids dissection of a small-caliber pedicle or microsurgical anastomosis
Treatment of scaphoid fractures and nonunions
- Comprehensive review of scaphoid fracture treatment
- Proximal pole fractures have the highest AVN rate (30-50%) and non-union rate (15-20%), requiring specialized surgical approaches
The significance of the 1-2 intercompartmental supraretinacular artery (1-2 ICSRA) as a distally pedicled dorsal wrist bone flap
- Detailed anatomic study of the 1-2 ICSRA vascularized graft technique
- Used for proximal pole non-union with AVN
Minimally invasive management of scaphoid nonunions
- Describes percutaneous and limited open techniques for scaphoid ORIF
- Includes the dorsal approach for proximal pole fractures with retrograde screw fixation
Management of the fractured scaphoid using a new bone screw
- Original description of the headless compression screw for scaphoid fixation
- Defines the Herbert classification of scaphoid fractures (B3 = proximal pole)
Non-union of the scaphoid: treatment with cannulated screws compared with treatment with Herbert screws
- Randomized trial of cannulated versus Herbert screws for scaphoid non-union
- Headless compression screws achieve 85-90% union for scaphoid non-unions with appropriate bone grafting
Vascularized bone grafts for scaphoid nonunions and Kienbock's disease
- Review of vascularized bone graft options for scaphoid AVN
- Covers pedicled ICSRA grafts and free medial femoral condyle grafts
Nonunion of the scaphoid: a critical analysis of recent natural history studies
- Natural history study of untreated scaphoid non-unions
- Untreated non-unions progress to SNAC arthritis in around 95% of cases within 10 years — emphasizing the importance of achieving union