Dorsal approach over the scapholunate interval · chronic reducible SL instability without SLAC arthritis
- Indication: a chronic scapholunate (SL) ligament tear — six months to two years from injury — with reducible DISI malalignment and NO scapholunate advanced collapse (SLAC) arthritis. The absence of arthritis is the absolute gatekeeper.
- DISI pattern: the lunate extends dorsally and the scaphoid flexes palmarly, giving a scapholunate angle greater than 70 degrees on the lateral view (normal 30–60 degrees).
- The dorsal component of the SL ligament is the strongest region and provides about 80% of scapholunate stability — dorsal capsulodesis recreates this primary restraint.
- A distally-based dorsal capsular flap (about 10–15mm wide and 20–25mm long) is raised with its distal attachment preserved as the vascular pedicle, then tethered across the scapholunate interval to both the scaphoid and the lunate.
- Reduction precedes reconstruction: a K-wire joystick extends the scaphoid, the lunate is flexed, the gap is closed, and the position is held with two divergent scapholunate K-wires and one scaphocapitate K-wire.
- Long arm immobilisation for the first four weeks is essential — it prevents forearm rotation, which otherwise places torsional stress on the reconstruction and causes early failure.
- Diagnostic triad on imaging: Terry Thomas sign (SL gap greater than 3mm), cortical ring sign (flexed scaphoid) and SL angle greater than 70 degrees (DISI).
- Counsel the patient honestly: a 10–30% recurrence or failure rate, about 30–40% loss of wrist motion, a six to twelve month recovery, and a lifelong need to avoid high-impact loading.
When & Why
Primary indication. A chronic scapholunate (SL) ligament tear — six months to two years from injury — with symptomatic carpal instability (pain, weakness, clicking) and a reducible DISI malalignment, in a wrist with no SLAC arthritis, that has failed conservative management (splinting, activity modification, therapy). Before offering reconstruction, confirm each of the following: - SL injury confirmed on MRI or arthroscopy.
- Reducible scapholunate malalignment and DISI deformity — test with stress views or fluoroscopic pressure; an irreducible (fixed) deformity will not hold.
- No radiographic SLAC arthritis — the radioscaphoid, radiolunate and capitolunate joints must all be intact. This is the single most important exclusion.
- Adequate capsular tissue quality for a flap, and a patient who will comply with prolonged immobilisation and rehabilitation. Radiographic criteria that justify surgery: - Scapholunate interval greater than 3mm on the PA view (the Terry Thomas sign; normal less than 2–3mm).
- Scapholunate angle greater than 70 degrees on the lateral view (the DISI pattern; normal 30–60 degrees).
- Cortical ring sign on the PA view (the flexed scaphoid viewed end-on).
- Intact radioscaphoid, radiolunate and capitolunate joints — no arthritis. Absolute contraindications. SLAC wrist Stage II or higher (radioscaphoid arthritis present); an irreducible scapholunate deformity; active wrist or hand infection; severe osteoporosis in which K-wire fixation would fail; and medical comorbidities that preclude prolonged immobilisation. Relative contraindications. SLAC Stage I (radial styloid arthritis only — consider with a styloidectomy); very chronic injuries (greater than two to three years) with poor tissue quality; scaphoid malunion or lunate pathology; high-demand manual labourers (higher failure risk); poor compliance; revision after a failed reconstruction; and inflammatory arthropathy such as rheumatoid arthritis. Alternative procedures when reconstruction is contraindicated: - SLAC Stage II–III — four-corner fusion (scaphoid excision with capitate-lunate-hamate-triquetrum fusion).
- SLAC Stage III–IV — proximal row carpectomy (if the capitolunate joint is preserved) or total wrist fusion.
- Acute SL tears (less than six weeks) — primary ligament repair.
- Chronic irreducible deformity — scaphoid-trapezium-trapezoid fusion with ligament reconstruction. Consent specifically for a 10–30% recurrence or failure rate, about 30–40% loss of wrist motion, superficial radial sensory nerve numbness or a painful neuroma (around 5%), pin-tract infection (5–10%), stiffness, and a six to twelve month recovery with possible lifelong activity modification. Setup. Supine with the arm on a radiolucent hand table and an upper-arm pneumatic tourniquet; general anaesthesia or a brachial plexus (supraclavicular, infraclavicular or axillary) block, with optional local infiltration along the incision for post-operative pain. A mini C-arm is draped sterile for PA, true lateral and oblique views. Position the hand flat with a towel roll under the distal forearm for wrist extension, or use finger-trap traction of 5–10 lb. Loupe magnification is mandatory — identification of the small sensory nerve branches is the whole game.
The Operation
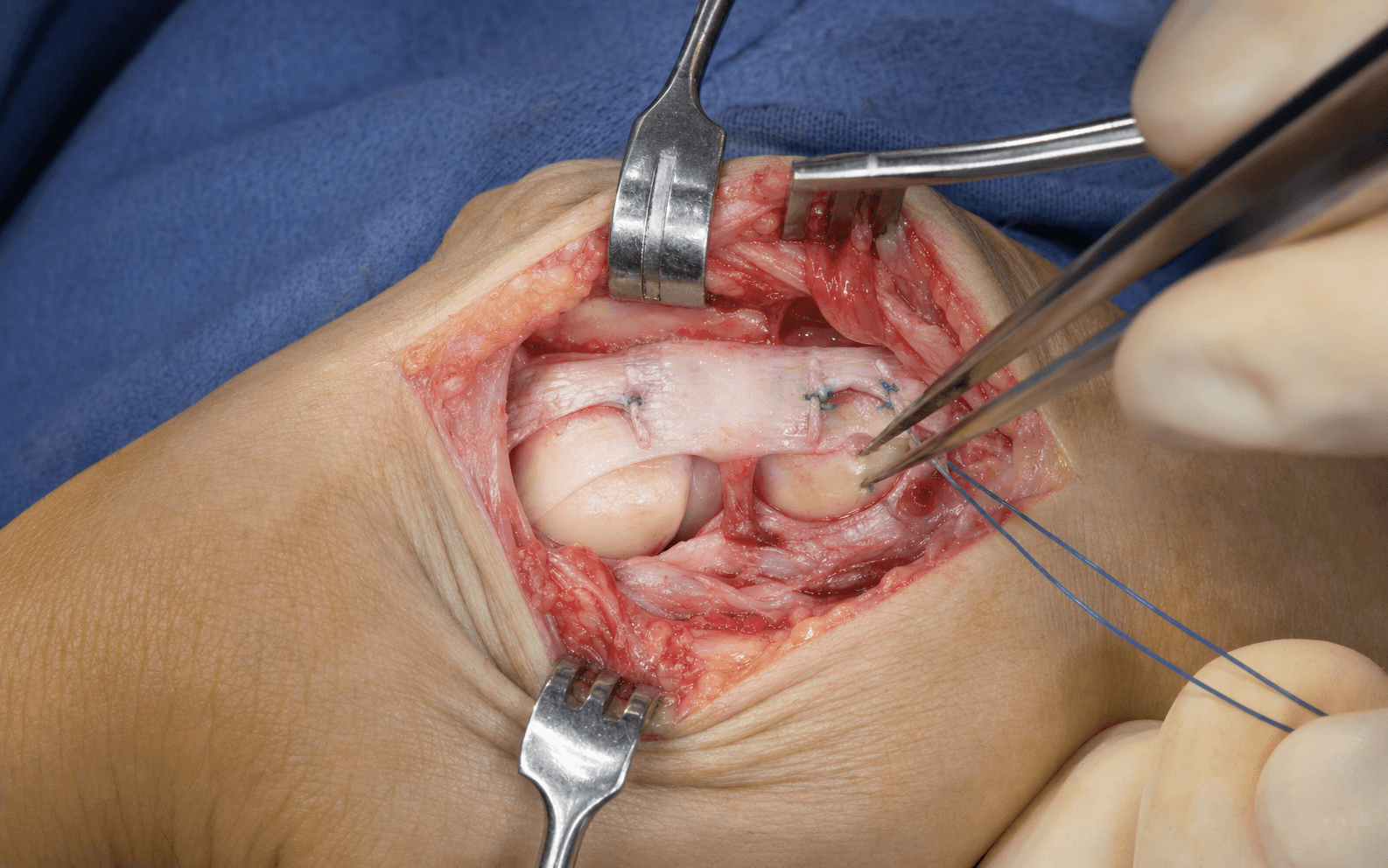
The goal is to expose the scapholunate interval through a longitudinal dorsal approach, reduce the DISI deformity, raise a distally-based dorsal capsular flap with its distal vascular pedicle preserved, and tether that flap across the scapholunate interval to both the scaphoid and the lunate — recreating the function of the torn dorsal SL ligament. The exposure and the step-by-step sequence follow.
Operative sequence
- Supine, arm on a radiolucent hand table, upper-arm tourniquet (not yet inflated), mini C-arm positioned for PA and lateral views.
- On preoperative fluoroscopy: PA — measure the SL interval (normal less than 3mm; pathologic greater than 3–5mm), confirm the Terry Thomas and cortical ring signs; lateral — measure the SL angle (normal 30–60 degrees; DISI greater than 70 degrees) and confirm lunate extension.
- Critically confirm there is no radioscaphoid or capitolunate arthritis, and document that the deformity is reducible with manual pressure and stress views.
- Exsanguinate with an Esmarch bandage and inflate the tourniquet to 250mmHg.
- Longitudinal dorsal incision centred over the scapholunate interval, from just proximal to Lister's tubercle to the midcarpal level (about 6–8cm).
- In the subcutaneous plane, identify and protect the superficial radial sensory nerve branches on the radial side — two to three small branches cross the field only 2–5mm from the skin; retract them radially with vessel loops.
- Identify and protect the dorsal sensory branch of the ulnar nerve on the ulnar side near the sixth extensor compartment; retract it ulnarly.
- Expose the extensor retinaculum — its longitudinal fibres overlie the extensor tendons.
- Incise the extensor retinaculum longitudinally between the third (EPL) and fourth (EDC/EIP) compartments — this internervous interval gives direct access to the dorsal capsule.
- Identify the EPL in the third compartment as it courses around Lister's tubercle and retract it radially — it can be attenuated or frayed here in chronic cases, so handle it gently.
- Retract the fourth-compartment EDC and EIP tendons ulnarly, or split the compartment and pass between the tendons for better exposure.
- The dorsal wrist capsule now lies visible beneath the extensor tendons.
- Map the dorsal capsule: the dorsal radiocarpal ligament and dorsal intercarpal ligament form a characteristic V or inverted-Y converging on the dorsal lunate — incorporate this into the flap.
- Raise a distally-based rectangular capsular flap: begin proximally at the distal radius dorsal rim, make two parallel longitudinal cuts about 10–15mm apart, and extend distally 20–25mm to the capitate-lunate level.
- Leave the distal attachment intact — this is the vascular pedicle that maintains flap blood supply. Elevate from proximal to distal.
- The scapholunate interval is now fully exposed; the dorsal SL ligament is typically frayed, attenuated or absent.
- Joystick: insert a 0.062-inch K-wire into the scaphoid waist and extend the scaphoid to correct its flexion; manipulate the lunate into flexion; close the SL gap with a pointed reduction forceps or manual pressure.
- Confirm reduction on fluoroscopy: PA shows SL interval less than 3mm with no cortical ring sign; lateral shows SL angle 30–60 degrees.
- Hold the reduction with temporary K-wires: two 0.062-inch scapholunate K-wires in a divergent pattern (prevents rotation) and one scaphocapitate K-wire for additional stability, left proud of the skin about 1cm.
- With reduction held by the K-wires, gently roughen the dorsal cortex of the proximal scaphoid and the lunate with a small rongeur or a 2–3mm burr — superficial only (1–2mm), to create a bleeding bed that promotes fibrous ingrowth, without breaching the joint or weakening the bone.
- For secure fixation in chronic or severe cases, prefer suture anchors: place two 2.0mm or 2.4mm anchors in the dorsal proximal scaphoid and two in the dorsal lunate, loaded with 2-0 or 3-0 braided non-absorbable suture (FiberWire or Ethibond).
- Pass the scaphoid anchor sutures through the flap and tie it to the dorsal scaphoid under firm tension; then pass the lunate anchor sutures through the flap and tie it to the dorsal lunate. The flap now bridges the scapholunate interval as a tether.
- Reinforce with interrupted sutures along the flap edges.
- Alternative — transosseous bone tunnels (1.5–2.0mm, dorsal to palmar) through the scaphoid and lunate: pass 2-0 or 3-0 braided suture through the flap and tunnels and tie on the palmar cortex (more demanding, avoids anchor cost).
- Tension is the critical technical point: too loose and it will not prevent recurrent gapping (failure); too tight and it tears the flap or pulls through bone (failure). The flap should be visibly taut, approximate the bones, and show only minimal gapping when the interval is gently stressed.
- For severe chronic instability, high-demand patients or revision cases, augment the capsulodesis.
- Modified Brunelli (bone-retinaculum-bone): a separate dorsal capsular strip passed through a 3–4mm dorsal-to-palmar tunnel in the scaphoid waist, looped back and secured to the dorsal capsule or proximal scaphoid — a dynamic tether resisting scaphoid flexion.
- SLAM (scapholunate axis method): a harvested palmaris longus (or toe extensor) graft passed in a figure-8 through dorsal-palmar tunnels in both the scaphoid and the lunate and tensioned — a strong internal brace.
- Decision: simple capsulodesis is adequate for most subacute to early chronic cases; reserve augmentation for revision surgery, severe chronic instability (greater than two years), poor tissue quality, or high-demand patients and athletes.
- PA: SL interval less than 3mm, cortical ring sign absent, Gilula's three carpal arcs restored and parallel, K-wires crossing the joint with good purchase.
- Lateral: SL angle 30–60 degrees, radiolunate angle 0 degrees (plus or minus 10 degrees), capitate and lunate colinear (no DISI or VISI).
- Bend and cut the K-wires outside the skin leaving about 1cm proud, and protect the ends with plastic guards (alternatively bury them, which then needs a mini-open removal).
- Irrigate thoroughly with normal saline (3–6 litres) to clear bone debris.
- Close the dorsal capsule over the reconstruction with 3-0 absorbable (Vicryl) if enough tissue remains — if the capsule is thin after flap harvest, leave it open (acceptable; do not force a tight closure).
- Close the extensor retinaculum over the tendons with 3-0 absorbable, Z-lengthening it if tight to keep the extensor tendons gliding smoothly.
- Subcutaneous layer with 4-0 absorbable; skin with 4-0 nylon vertical mattress or running subcuticular 4-0 absorbable; protect pin sites with a sterile dressing and plastic guards.
- Apply a well-moulded long arm cast or splint with the wrist neutral, the forearm in neutral rotation, the elbow at 90 degrees, and the fingers free for ROM.
- Rationale: a long arm cast blocks forearm rotation (pronation-supination), which otherwise places torsional stress on the healing reconstruction; a short arm cast permits that rotation and risks early failure.
- Plan four weeks in the long arm cast, then transition to a short arm cast for a further four to eight weeks (total immobilisation 8–12 weeks minimum).
- Superficial radial sensory nerve — two to three branches cross the dorsal-radial wrist 2–5mm from the skin, superficial to the retinaculum; identify and retract radially with vessel loops (the most commonly injured nerve; a painful neuroma results).
- Dorsal sensory branch of the ulnar nerve — emerges about 5cm proximal to the ulnar styloid and courses near the sixth compartment; protect on the ulnar side.
- Extensor pollicis longus — third compartment, around Lister's tubercle, where it may be attenuated or frayed in chronic cases; retract gently and radially.
- Radial artery dorsal carpal branch — supplies the dorsal capsule and runs within its layers over the scapholunate interval; preserve the distal pedicle when raising the flap.
- Radiocarpal and midcarpal articular cartilage — lies immediately deep to the capsule; avoid direct instrument contact and keep K-wires extra-articular on both views.
The dorsal component of the SL ligament is the thickest and strongest region and provides about 80% of scapholunate stability. A distally-based dorsal capsular flap, secured across the interval in the anatomically correct dorsal position, substitutes for exactly this lost primary restraint — which is why dorsally-based repairs succeed where palmar repairs tend to fail.
If radioscaphoid or capitolunate arthritis is present, the reconstruction will predictably fail and the patient needs a salvage procedure (four-corner fusion or proximal row carpectomy), not reconstruction. Confirm the absence of arthritis on the preoperative fluoroscopy before committing to a capsulodesis.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy and goals | |-------|--------|----------------|-------------------| | 1 | 0–4 weeks | Long arm cast — wrist neutral, forearm neutral, elbow 90 degrees | Fingers free for active ROM; K-wires in situ | | 2 | 4–8/10 weeks | Short arm cast, neutral wrist | Continue full wrist immobilisation; K-wires remain in situ | | 3 | 8–12 weeks | Remove K-wires if alignment held; removable wrist splint | Gentle AROM/AAROM only (flexion-extension, deviation, rotation); no strengthening | | 4 | 12–16 weeks | Splint for heavy tasks | Progressive ROM; light strengthening (therapy putty); light ADLs | | 5 | 4–6 months | Night or heavy-task splint | Progressive resistance; work and sport simulation | | 6 | 6 months and beyond | Activity-based | Unrestricted activity if pain-free, ROM at least 70%, grip at least 80%, and alignment maintained; avoid high-impact loading lifelong | K-wire removal (typically 8–12 weeks). Confirm on radiographs that the SL interval remains less than 3mm and the SL angle 30–60 degrees with no loss of reduction. Remove in clinic under local anaesthetic: clean the pin sites, grasp each wire with a needle driver, and back it out with gentle rotation — scapholunate wires first, then the scaphocapitate wire. Pin sites heal by secondary intention. Begin hand therapy immediately for gentle ROM only; no strengthening until after 12 weeks. Follow-up. Two weeks (wound and cast check, pin-site care), six weeks (radiographs in cast), 8–12 weeks (radiographs and wire removal, start therapy), four months and six months (clinical and radiographic review), one year (final assessment for maintained reduction and any SLAC development), then consider annual radiographs long-term to monitor for arthritis progression. Complications
- Recognition
- Recurrent pain, clicking, weakness; widened SL interval greater than 3mm, SL angle greater than 70 degrees, return of DISI on serial imaging
- Prevention
- Correct patient selection (no SLAC), adequate flap tissue, secure tensioned fixation, K-wire protection 8–12 weeks, a compliant long arm phase
- Management
- Asymptomatic or mild: observe, modify activity, splint, NSAIDs. Symptomatic: revision with tendon-graft augmentation (SLAM). Salvage (four-corner fusion or PRC) if SLAC develops
- Recognition
- Widening SL interval greater than 3mm or SL angle greater than 60–70 degrees; may be asymptomatic; K-wire migration on radiograph
- Prevention
- Adequate K-wire configuration (2 SL divergent plus 1 scaphocapitate), long arm cast for the first 4 weeks, confirm reduction before wire removal
- Management
- During immobilisation and if acute: closed reduction and re-pinning. After wire removal: observe if asymptomatic; revise if symptomatic; salvage if SLAC
- Recognition
- Wire backs out or advances on serial films; sudden change in position; erythema, drainage, pain or fever at pin sites
- Prevention
- Bend wires outside skin, protective guards and dressing, daily pin care, remove by 8–12 weeks
- Management
- Migration: remove early. Breakage: remove accessible portion, use fluoroscopy to find the fragment, rarely operative. Infection: pin care and oral antibiotics (cephalexin or clindamycin); earlier removal or IV antibiotics if spreading
- Recognition
- Limited wrist flexion-extension (expect about 40–50 degrees each way), limited deviation, reduced grip
- Prevention
- Cannot be fully prevented — a consequence of surgery and prolonged immobilisation; early ROM after wire removal and consistent therapy
- Management
- ROM and joint mobilisation, heat or paraffin, progressive strengthening after 12 weeks; most reach 70–80% of the other side by 6–12 months
- Recognition
- Numbness or paraesthesia over the dorsal-radial hand and thumb; tender Tinel over the scar; occasional painful neuroma
- Prevention
- Careful identification and protection of branches, vessel-loop retraction, loupe magnification, avoid cautery near nerves
- Management
- Neuropraxia usually resolves over 3–6 months; desensitisation and NSAIDs; a painful neuroma may need excision with burial (rare)
- Recognition
- Progressive pain despite maintained SL alignment; arthritis at radial styloid (I), radioscaphoid (II), then capitolunate (III)
- Prevention
- Operate before arthritis develops, achieve and maintain anatomic reduction, counsel on long-term activity modification
- Management
- Stage I: radial styloidectomy. Stage II–III: salvage — four-corner fusion or PRC (if capitolunate joint preserved). Stage IV: total wrist fusion or arthroplasty
- Recognition
- Ongoing pain despite anatomic radiographs; pain on loading, gripping or end-range motion
- Prevention
- Anatomic reduction, assess the DRUJ pre-operatively, gentle technique, early therapy to prevent CRPS
- Management
- Work up for occult arthritis (bone scan or MRI) and DRUJ pathology; therapy, NSAIDs, injection; address the DRUJ separately; CRPS needs aggressive therapy and pain management
Viva & Exam Focus
DORSALDORSAL — why dorsally-based repairs work
REPAIRSREPAIRS — post-operative protocol essentials
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old rock climber presents 8 months after a wrist injury with clicking, pain and weakness. The PA radiograph shows a 5mm scapholunate interval and a cortical ring sign; the lateral shows an SL angle of 75 degrees. How do you interpret these findings and what is your management?”
“Explain the biomechanics of scapholunate ligament injury, why DISI develops, and why dorsal capsulodesis restores stability.”
“Describe your step-by-step technique for creating and securing a distally-based dorsal capsular flap, including your fixation options and how you judge flap tension.”
Indication
- Chronic SL tear (6 months to 2 years) with reducible DISI and NO SLAC arthritis
- Failed conservative care; intact radioscaphoid, radiolunate and capitolunate joints
- Adequate tissue and a compliant patient
Diagnostic triad
- Terry Thomas sign — SL gap greater than 3mm on PA
- Cortical ring sign — flexed scaphoid viewed end-on
- SL angle greater than 70 degrees on lateral (DISI)
Key anatomy
- SL ligament: dorsal strongest (80% of stability), proximal membranous weakest, palmar intermediate
- Scaphoid flexes, lunate extends — the intact ligament restrains both
- Protect: superficial radial nerve, dorsal ulnar sensory nerve, EPL, radial artery dorsal branch
Critical steps
- Dorsal incision; open retinaculum between 3rd (EPL) and 4th (EDC) compartments
- Raise distally-based flap (10–15mm by 20–25mm) — preserve the distal pedicle
- Reduce: joystick extends scaphoid, flex lunate, close gap; 2 SL plus 1 scaphocapitate K-wires
- Secure flap to both bones with appropriate tension; confirm on fluoroscopy
- Long arm cast 4 weeks, then short arm — total 8–12 weeks
Post-op protocol
- 0–4 weeks: long arm cast, K-wires in situ, finger ROM
- 4–8/10 weeks: short arm cast, no active wrist motion
- 8–12 weeks: radiographs, remove K-wires, removable splint, gentle ROM only
- 12–16 weeks: progress ROM and light strengthening
- 6 months: unrestricted if pain-free, 70% ROM, 80% grip, alignment held
Complications
- Reconstruction failure 10–30%
- Loss of reduction; K-wire problems 5–10%
- Stiffness 30–40% ROM loss (expected)
- Superficial radial nerve injury about 5%
- Progression to SLAC — needs salvage
Exam pitfalls
- SLAC arthritis is a contraindication — needs salvage, not reconstruction
- Reducibility is essential — test with stress views
- DISI: lunate extended, scaphoid flexed (opposite in VISI)
- Long arm cast first — prevents rotation stress
- Counsel on failure rate, ROM loss and prolonged recovery
Background & Evidence
Mechanism and natural history. The SL ligament typically tears in hyperextension, ulnar deviation and intercarpal supination — most often a fall on the outstretched hand. The injury then evolves in phases: an acute phase (0–6 weeks) in which the ligament fails (usually dorsally) and the scaphoid begins to flex and the lunate to extend; a subacute phase (6 weeks to 6 months) with progressive deformity, a widening gap and an established DISI pattern; a chronic phase (beyond 6 months) in which the deformity may become fixed and the secondary restraints fail, raising the risk of arthritis; and, over years, SLAC — progressive arthritis at the radial styloid, then the radioscaphoid joint, then the capitolunate joint. Pathoanatomy — the three regions of the SL ligament. The dorsal region is the thickest, composed of short transversely oriented collagen fibres, and is the principal load-bearing restraint to scaphoid flexion and abnormal SL rotation (about 80% of stability). The proximal (membranous) region is principally fibrocartilage with few longitudinal fibres and is the weakest — it tears first in acute injuries. The palmar region is thin with obliquely oriented fascicles and is an intermediate, weaker secondary restraint. This anatomy is the rationale for dorsally-based reconstructions: recreating the strongest (dorsal) component is what restores stability.
- Site of arthritis
- Radial styloid only
- Typical management
- Radial styloidectomy; observe or reconstruct if still reducible
- Site of arthritis
- Radioscaphoid joint
- Typical management
- Salvage — four-corner fusion (or PRC if capitolunate joint preserved)
- Site of arthritis
- Capitolunate joint (radiolunate spared)
- Typical management
- Salvage — four-corner fusion or proximal row carpectomy
- Site of arthritis
- Pan-carpal arthritis
- Typical management
- Total wrist fusion or wrist arthroplasty
Reconstruction options side by side. When the deformity is reducible and there is no arthritis, several soft-tissue reconstructions are available; all share the principle of recreating the dorsal restraint, and the choice turns on tissue quality, chronicity and patient demand.
- Concept
- Distally-based dorsal capsular flap tethered to both scaphoid and lunate
- Best for
- Subacute to early chronic instability with adequate tissue
- Drawback
- 10–30% failure in severe cases; 30–40% ROM loss
- Concept
- Capsular strip through a scaphoid-waist tunnel as a dynamic tether
- Best for
- Higher-demand or more severe instability
- Drawback
- Risk of scaphoid fracture through the tunnel; flap pull-through
- Concept
- Palmaris (or toe extensor) graft in a figure-8 through both bones
- Best for
- Severe or revision cases; robust fixation
- Drawback
- Tendon-harvest morbidity; tunnel fracture risk; demanding
- Concept
- Distally-based dorsal strip fixed to the distal scaphoid; 3LT adds FCR through the scaphoid
- Best for
- Primary deforming force is scaphoid flexion
- Drawback
- Addresses scaphoid flexion more than lunate extension
Key evidence. Berger's anatomic study established the three-region structure of the SL ligament and the dominance of the dorsal region — the basis for all dorsally-based repairs. Szabo's prospective series showed dorsal intercarpal ligament capsulodesis reliably corrected the SL angle and gap at short to medium term with only minor motion and grip loss. The tendon-graft alternatives (3LT, modified Brunelli) give durable pain relief and function, but the largest pooled systematic review (Goeminne, 2024) shows radiographic correction is not always maintained long-term, secondary degeneration develops in about 15%, and radiographic decay does not correlate with clinical outcome — so clinical, not purely radiographic, endpoints should drive counselling and follow-up.
References
The gross and histologic anatomy of the scapholunate interosseous ligament
- Cadaveric study (21 fresh, 16 fixed adult wrists) established that the scapholunate interosseous ligament is consistently divisible into three regions: dorsal, proximal (membranous) and palmar
- Dorsal region is the thickest and is composed of short, transversely oriented collagen fibres - the strongest, load-bearing portion
- Proximal region is principally fibrocartilage (few longitudinal collagen fibres) and is the weakest portion; palmar region is thin with obliquely oriented fascicles
- The radioscapholunate ligament (vessel-carrying, not a true mechanical restraint) separates the proximal and palmar regions
Dorsal intercarpal ligament capsulodesis for chronic, static scapholunate dissociation: clinical results
- Prospective series of 21 patients (22 wrists), age 16-62, followed 1 to 4 years with independent examiners and standardised radiographs
- Dorsal intercarpal ligament capsulodesis significantly improved both scapholunate angle and scapholunate gap at final follow-up
- Only minor loss of range of motion and grip strength; patients satisfied with mean DASH 17 and SF-12 of 83
- Conceptual advantage: avoids a radioscaphoid tether and keeps the proximal row linked as a functional unit
Three-ligament tenodesis for the treatment of scapholunate dissociation: indications and surgical technique
- Defined a widely adopted treatment algorithm for SL instability based on reducibility, repairability and presence of secondary osteoarthritis
- Described the three-ligament tenodesis (3LT) using a distally based FCR strip routed through the scaphoid for non-repairable complete SL rupture with reducible malalignment and no arthritis
- Reconstructs dorsal SL, dorsal intercarpal and scaphotrapezial restraints in a single tendon-based construct
- Reported promising early results for restoring carpal alignment in reducible deformity without secondary osteoarthritis
Results of the modified Brunelli tenodesis for treatment of scapholunate instability: a retrospective study of 19 patients
- 19 modified Brunelli (FCR) tenodeses for reducible dynamic or static SL instability without arthritis; mean follow-up 37 months
- 15 of 19 patients had no to mild pain (mean VAS 3/10); grip strength recovered to 78% and flexion-extension to roughly 73-75% of the uninvolved wrist
- Static SL distance was maintained (mean 2.4mm), but the SL angle relapsed: 61 degrees pre-op, 53 degrees immediately post-op, rising back to 62 degrees at review
- One patient progressed to SLAC stage II
Treatment of chronic scapholunate dissociation with FCR tenodesis: a systematic review of the results of MBT and 3LT technique
- PRISMA systematic review of 15 studies (289 modified Brunelli tenodeses and 311 three-ligament tenodeses; 600 patients)
- Both techniques gave satisfactory clinical outcomes with a mean pain reduction of about 3 points on the visual analogue scale and a functional flexion-extension arc
- Radiographic improvement was seen at medium term, but loss of reduction occurred in the long term and radiographic decay did not correlate with clinical outcome
- Secondary degeneration developed in about 15% and the overall complication rate was about 9%
The natural progression of scaphoid instability
Described the natural history and progressive stages of scaphoid instability that culminate in the SLAC pattern — the basis for staging and for intervening before arthritis develops.
Capsulodesis in reconstructive hand surgery: dorsal capsulodesis for the unstable scaphoid
The original description of dorsal capsulodesis for the unstable scaphoid — the foundation of the procedure performed today.
A new surgical technique for carpal instability with scapho-lunar diastasis
Original description of the FCR tenodesis for carpal instability with scapholunate diastasis — the eponymous Brunelli procedure and its modifications.
Autograft replacements for the scapholunate ligament: a biomechanical comparison of hand-based autografts
Biomechanical comparison of hand-based autograft options for scapholunate ligament replacement, informing graft choice for augmented reconstructions.
Scapholunate ligament reconstruction using a bone-retinaculum-bone autograft
Description of the bone-retinaculum-bone autograft technique for scapholunate ligament reconstruction.
The role of three-ligament tenodesis in the treatment of chronic scapholunate instability
Reported the role and clinical results of three-ligament tenodesis in chronic scapholunate instability.
The RASL procedure: reduction and association of the scaphoid and lunate using the Herbert screw
Description of the RASL procedure — reduction and association of the scaphoid and lunate held with a Herbert screw, an alternative for selected reducible SL injuries.