Open or arthroscopic removal of diseased synovium · localised vs diffuse disease dictates approach
- Indications span inflammatory synovitis refractory to medical therapy, pigmented villonodular synovitis (PVNS / diffuse-type tenosynovial giant cell tumour), synovial chondromatosis, haemophilic arthropathy, and septic arthritis as a debridement adjunct
- Completeness of synovectomy — especially the posterior compartment — is the single biggest determinant of recurrence; diffuse PVNS often requires a combined anterior arthroscopic plus open posterior approach
- Arthroscopic synovectomy gives faster recovery and lower stiffness but is technically demanding; open synovectomy offers more complete clearance for diffuse or posterior disease but higher arthrofibrosis risk
- Adjuvant radiosynovectomy or external-beam radiotherapy lowers recurrence in diffuse PVNS; pexidartinib (CSF1R inhibitor) is a systemic option for unresectable or recurrent diffuse-type disease
When & Why
What the operation is. Synovectomy is the surgical removal of diseased synovium from the knee. It is used for a heterogeneous group of conditions in which proliferative or haemosiderin-laden synovium is the driver of symptoms and joint destruction. The single most important distinction before you operate is localised versus diffuse disease — it dictates the approach, the completeness you can achieve, and the recurrence risk. Primary indications - Inflammatory / rheumatoid synovitis — persistent boggy synovitis despite optimised medical therapy (DMARDs, biologics) for at least 6 months, with recurrent effusions and pain and preserved articular cartilage. Best results are in early, pre-erosive disease. The aim is symptom control and slowing of joint destruction, not cure; benefit tends to diminish over years. It is performed less often in the biologic era but remains relevant when synovitis is monoarticular and drug-refractory.
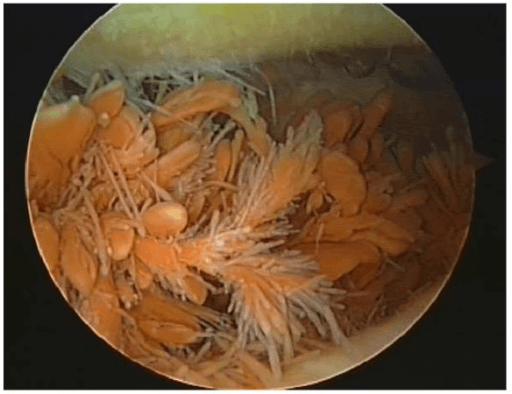
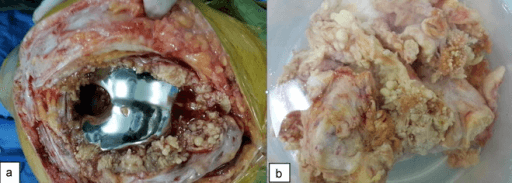
- PVNS / diffuse-type tenosynovial giant cell tumour (TGCT) — localised (nodular) disease is a focal intra-articular nodule, often pedunculated, cured by local excision (frequently arthroscopic) with low recurrence. Diffuse disease carpets the synovium and frequently involves the posterior compartment, requiring total synovectomy and carrying a much higher recurrence rate (reported 8-46%). The knee is the most commonly affected joint (around 80% of PVNS cases).
- Synovial chondromatosis — metaplastic cartilaginous or osteocartilaginous loose-body formation within the synovium (Milgram phases). Operate for mechanical symptoms (locking, catching), pain and effusion from loose bodies. Treatment is synovectomy plus removal of all loose bodies; recurrence relates to active synovial metaplasia.
- Haemophilic arthropathy — recurrent haemarthrosis driving chronic haemophilic synovitis and a vicious bleed-synovitis-bleed cycle. Indicated when bleeds persist despite optimised factor prophylaxis (and often after failure of radiosynovectomy). The goal is to reduce bleed frequency and slow cartilage destruction; it sits earlier in the cascade than arthroplasty.
- Septic arthritis (adjunct) — synovectomy or debridement as part of arthroscopic or open washout, removing infected proliferative and biofilm-laden tissue combined with copious lavage and antibiotics. Contraindications - Active skin infection over portal or incision sites (unless the procedure is for sepsis)
- End-stage arthritis where arthroplasty is more appropriate than synovectomy
- Uncontrolled coagulopathy or inadequate factor cover in haemophilia
- Medical comorbidity precluding anaesthesia Open versus arthroscopic synovectomy — the decision
Faster recovery, less pain, lower wound morbidity, earlier return of motion and lower stiffness. Technically demanding — complete clearance of the posterior compartment needs posteromedial and posterolateral portals and considerable skill. Best for localised disease and diffuse disease confined to accessible compartments.
Allows more thorough clearance, especially for diffuse disease, a large loose-body burden, or posterior-compartment disease. Higher rates of arthrofibrosis and wound problems, and longer rehabilitation.
The evidence-based strategy for diffuse PVNS to ensure the posterior compartment is fully cleared. This combination most strongly reduces recurrence in diffuse disease.
Adjuvant therapy for diffuse PVNS. Radiosynovectomy (intra-articular radioisotope, e.g. yttrium-90) and external-beam radiotherapy lower recurrence after subtotal or total synovectomy of diffuse disease. Pexidartinib, a CSF1R inhibitor, is approved for symptomatic diffuse-type TGCT not amenable to surgery (ENLIVEN trial) — hepatotoxicity requires monitoring. Radiosynovectomy is also a mainstay in haemophilic synovitis as a less-invasive alternative or adjunct. Consent specifically for disease recurrence (diffuse PVNS recurs in 8-46%), arthrofibrosis and stiffness (the commonest functional complication), haemarthrosis, popliteal neurovascular injury, common peroneal nerve injury and foot drop, saphenous nerve numbness or a painful neuroma, and infection or wound problems. In haemophilia, consent is as much haematological as surgical. Setup. Supine with a thigh tourniquet and a side post or leg holder that allows valgus and varus stress and flexion to 90 degrees and beyond — the knee must flex to 90 degrees for safe posterior work. Examination under anaesthesia confirms range of motion and stability. For haemophilia, confirm the factor level is corrected to 80-100% before incision. For diffuse PVNS, plan posterior portals and a possible open posterior conversion in advance. General or regional anaesthesia; the tourniquet gives the bloodless field essential for identifying diseased synovium and avoiding incomplete clearance.
The Operation
The goal is a complete, compartment-by-compartment synovectomy — every recess cleared — while protecting the cruciate ligaments, the articular cartilage and the popliteal neurovascular bundle. The exposure is the operation: arthroscopically it is portal placement (standard anterior portals for the front, posteromedial and posterolateral portals for the back); for diffuse or bulky disease it is a medial parapatellar arthrotomy anteriorly plus an open posterior approach. The posterior compartment is the classic site of residual disease and recurrence, so the exposure must reach it deliberately. The knee's synovium is the most extensive in the body and forms numerous recesses where disease hides: the supra-patellar pouch, the medial and lateral gutters (paratrochlear recesses), the intercondylar notch around the cruciates, the infrapatellar fat pad (Hoffa) and ligamentum mucosum anteriorly, and the posteromedial and posterolateral recesses behind the femoral condyles posteriorly (separated by the posterior cruciate ligament and its synovial sheath). A mental checklist of these recesses prevents the commonest technical error — under-resection.
Operative sequence
- Supine, thigh tourniquet, leg holder or side post; ensure the knee flexes to 90 degrees. Loupe-grade lighting through the camera; tourniquet inflated for a bloodless field.
- Establish the anterolateral (viewing) and anteromedial (working) portals (often interchanged).
- Systematically inspect every compartment and document the distribution of disease — focal nodule versus diffuse carpet, and the loose-body burden.
- Take synovial biopsies for histology before resection to confirm the diagnosis (haemosiderin-laden giant cells in PVNS; cartilaginous loose bodies in chondromatosis).
- Add a superolateral (and/or superomedial) portal for access and outflow — this is the exposure of the pouch, often the bulkiest disease burden.
- Use a motorised shaver or resector to remove synovium from the pouch, working systematically across the whole recess.
- Maintain a clear view; control bleeding with the tourniquet and intermittent radiofrequency haemostasis if needed.
- Clear synovium from both gutters (paratrochlear recesses) out to the periphery, where disease tracks and is easily missed.
- Interchange viewing and working portals to reach every corner.
- This peripheral synovium is easily under-resected — be deliberate.
- Resect synovium around the cruciate ligaments without injuring the ACL or PCL.
- Address the infrapatellar fat pad (Hoffa) and ligamentum mucosum where involved.
- In synovial chondromatosis, remove all visible loose bodies — count and account for them.
- Flex the knee to 90 degrees so the popliteal neurovascular bundle falls posteriorly, away from the posterior capsule.
- View the posteromedial recess via a trans-notch (modified Gillquist) approach, transilluminate the skin, and establish a posteromedial portal under direct vision about 1 cm above the joint line behind the medial femoral condyle.
- Resect posteromedial synovium with the shaver opening directed away from the posterior capsule — keep the cutting window facing the joint, never the capsule.
- Establish a posterolateral portal behind the lateral collateral ligament and biceps tendon, protecting the common peroneal nerve which runs postero-laterally behind biceps toward the fibular neck.
- Clear the posterolateral recess, again keeping instruments on the capsule with the cutting window facing the joint.
- A posterior cannula helps protect the capsule and improve outflow.
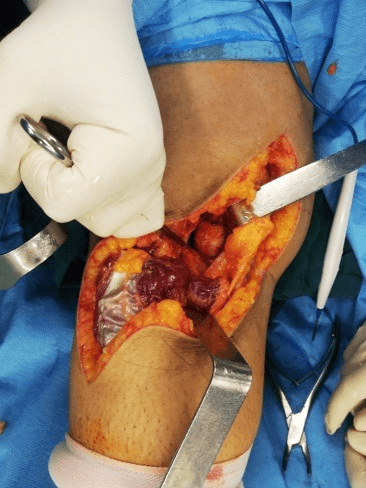
- A medial parapatellar arthrotomy gives open access to the supra-patellar pouch, gutters, notch and fat pad.
- Excise diseased synovium sharply and with rongeurs, protecting articular cartilage and the cruciates.
- Reserve this for very bulky diffuse disease, a large loose-body burden, or when arthroscopic clearance is inadequate.
- For diffuse PVNS with extensive posterior disease, convert to a combined anterior arthroscopic plus open posterior strategy — the approach that most reduces recurrence.
- A posteromedial or posterolateral open approach (or a formal posterior approach) exposes the posterior recesses.
- Identify and protect the popliteal neurovascular bundle and the common peroneal nerve, and work directly on the capsule.
- Excise posterior synovium completely — this step is what reduces recurrence in diffuse disease.
- Re-inspect every compartment for residual disease, particularly the posterior recesses and the periphery.
- Achieve haemostasis — release the tourniquet and identify bleeders if needed.
- Lavage thoroughly; consider a drain after extensive resection.
- Meticulous haemostasis to prevent haemarthrosis, which precipitates stiffness and, in haemophilia, a fresh bleed-synovitis cycle.
- Drain after extensive open synovectomy per surgeon preference; layered closure, avoiding a tight capsular closure that limits early motion.
- Soft compressive dressing — the goal is comfort while permitting early movement. Plan continuous passive motion and early active range of motion from day 1 to prevent arthrofibrosis.
- For diffuse disease, plan adjuvant radiosynovectomy or external-beam radiotherapy post-operatively to lower recurrence.
- For unresectable or recurrent diffuse-type TGCT, refer for consideration of systemic pexidartinib.
The popliteal artery, vein and tibial nerve lie immediately posterior to the posterior capsule, closest to the joint with the knee extended. During any posterior synovectomy: flex the knee to 90 degrees so the bundle drops posteriorly, stay on the capsule, keep the shaver cutting window facing the joint (never the capsule), use a posterior cannula or retractor, and never push an instrument blindly through the posterior capsule. Vascular injury is a surgical emergency — direct pressure, urgent vascular surgery referral and repair. Document neurovascular status before and after the operation.
With the knee extended the popliteal vessels lie hard against the posterior capsule; flexing to 90 degrees (70-90 degrees acceptable) lets them fall posteriorly and widens the safety margin. Combined with keeping the shaver window facing the joint, this single habit prevents the catastrophe of popliteal injury.
The common peroneal nerve runs behind the biceps femoris tendon and around the fibular neck. Place the posterolateral portal behind the lateral collateral ligament and biceps, identify and protect the nerve, and avoid aggressive lateral retraction. Injury causes foot drop and dorsal foot numbness.
The posterior compartment cannot be reached adequately from standard anterior portals alone, and it is the classic site of residual disease. Mollon's individual-patient meta-analysis showed recurrence is reduced most strongly by a combined open-and-arthroscopic synovectomy (OR 0.19 versus arthroscopy alone) — so for diffuse posterior disease, plan the combined anterior-arthroscopic plus open-posterior strategy from the outset.
Aftercare & Complications
Rehabilitation | Phase | Timing | Goals | |-------|--------|-------| | Immediate | 0-2 weeks | Soft compressive dressing; remove drain (if used) at 24-48 hours; weight-bearing as tolerated unless an extensive open or posterior procedure dictates protection. Begin active and passive range of motion on day 1, with continuous passive motion after extensive resection; quadriceps activation and patellar mobilisation; aim to regain 90 degrees of flexion within 1-2 weeks. Multimodal analgesia, ice and elevation; aspirate a tense effusion or haemarthrosis. In haemophilia, maintain factor cover per haematology protocol. | | Intermediate | 2-6 weeks | Advance to full range of motion and address any extension lag promptly; begin progressive quadriceps and hamstring strengthening; wound check, suture or portal-site care and scar management. Coordinate post-operative radiosynovectomy or external-beam radiotherapy for diffuse PVNS once wounds are healed. | | Recovery | 6 weeks-6 months | Arthroscopic synovectomy: most return to daily activities by 4-6 weeks and sport by 3 months. Open or combined posterior synovectomy: slower, with greater emphasis on regaining motion; return to demanding activity at 3-6 months. Stiffness, not recurrence, is the commonest early problem. Continue strengthening and proprioceptive rehabilitation; for inflammatory disease, ensure ongoing DMARD or biologic therapy is optimised by rheumatology. | | Long-term | 6 months plus | Diffuse PVNS: structured MRI surveillance to detect clinically silent recurrence (baseline post-op MRI then periodic imaging). Synovial chondromatosis: monitor for recurrent loose bodies and active metaplasia. Haemophilia: track bleed frequency and joint scores. Seek urgent evaluation for distal ischaemia or progressive neurological deficit, a tense hot painful joint with systemic upset, or rapidly recurrent effusion. | Complications
- Recognition
- Recurrent effusion, swelling, mechanical symptoms; MRI shows low-signal haemosiderin synovium (PVNS) or recurrent loose bodies; return of pre-operative symptoms
- Prevention
- Complete compartment-by-compartment synovectomy including posterior recesses; combined anterior + open posterior for diffuse disease; adjuvant radiotherapy or radiosynovectomy for diffuse PVNS; remove all loose bodies in chondromatosis
- Management
- Confirm with MRI and histology; revision synovectomy addressing missed compartments; adjuvant radiotherapy if not already given; pexidartinib for unresectable or recurrent diffuse-type TGCT
- Recognition
- Progressive loss of range of motion early post-op; pain at terminal motion; failure to regain expected flexion by 6 weeks
- Prevention
- Meticulous haemostasis to avoid haemarthrosis; early continuous passive motion and active range of motion; adequate analgesia; avoid prolonged immobilisation; favour arthroscopy where feasible
- Management
- Intensive physiotherapy and CPM; manipulation under anaesthesia if refractory by 8-12 weeks; arthroscopic arthrolysis or adhesiolysis for established arthrofibrosis
- Recognition
- Tense painful effusion early post-op; falling haemoglobin, expanding swelling; in haemophilia suspect inadequate factor cover
- Prevention
- Meticulous haemostasis with tourniquet release and bleeder control before closure; drain after extensive resection; haemophilia factor to 80-100% peri-operatively under haematology
- Management
- Aspiration or evacuation if large or tense; correct coagulopathy or boost factor levels; compression, elevation, analgesia; return to theatre for washout if recurrent or infected
- Recognition
- Brisk bleeding, expanding popliteal swelling, absent distal pulses; tibial nerve motor or sensory deficit; distal ischaemia
- Prevention
- Flex the knee to 90 degrees during posterior work; stay on the capsule with the cutting window facing the joint; use a posterior cannula or retractor; never push instruments blindly through the capsule
- Management
- Vascular injury is a surgical emergency — urgent vascular surgery referral and repair; nerve injury, explore or repair as indicated; document neurovascular status pre- and post-op
- Recognition
- Weak ankle dorsiflexion and eversion; numbness over the dorsum of the foot and first web space; foot drop gait
- Prevention
- Identify and protect the nerve behind biceps femoris during posterolateral access; avoid aggressive lateral retraction; know the safe corridor for the posterolateral portal
- Management
- Neuropraxia: observe with an ankle-foot orthosis, recovery over weeks to months; transection recognised intra-op: microsurgical repair; persistent foot drop: tendon transfer or AFO
- Recognition
- Erythema, warmth, discharge, increasing pain and effusion; raised inflammatory markers and fever; positive aspirate culture
- Prevention
- Prophylactic antibiotics and aseptic technique; meticulous wound closure avoiding haematoma; optimise comorbidities (diabetes, immunosuppression)
- Management
- Superficial: antibiotics and wound care; septic arthritis: arthroscopic or open washout, debridement and culture-directed antibiotics; remove non-viable tissue
Managing recurrent diffuse PVNS. Recurrence is most often residual posterior or peripheral synovium — re-image with MRI to map the missed disease. Revision synovectomy should specifically address the compartments missed first time, frequently via a combined anterior plus open posterior approach. Add adjuvant radiotherapy or radiosynovectomy if it was not used initially. Multiply recurrent or unresectable diffuse-type TGCT is an indication for systemic pexidartinib (CSF1R inhibitor) — counsel on hepatotoxicity and the need for monitoring. Haemophilia-specific considerations. The procedure must be planned jointly with haematology; uncorrected factor levels are an absolute contraindication. Factor replacement to 80-100% pre-operatively, maintained through the inflammatory and rehabilitation phase, prevents catastrophic bleeding and stiffness. Screen for inhibitors pre-operatively — an inhibitor changes the entire peri-operative plan. Radiosynovectomy is an established less-invasive alternative to surgical synovectomy for haemophilic synovitis.
Viva & Exam Focus
PAIRPAIR — indications for knee synovectomy
CLEARCLEAR — principles of a complete synovectomy
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 34-year-old presents with a 2-year history of recurrent atraumatic knee effusions, intermittent locking and a brown-stained aspirate. MRI shows diffuse low-signal synovial thickening on T1 and T2 with blooming on gradient-echo sequences, extending into the posterior compartment. How do you interpret this and how would you manage it?”
“A 28-year-old man with severe haemophilia A has recurrent right knee bleeds and a chronically boggy, swollen joint despite factor prophylaxis. He is being considered for knee synovectomy. What are the key considerations and how does this differ from synovectomy in other conditions?”
“Talk me through how you perform an arthroscopic knee synovectomy and ensure it is complete. Where is disease most commonly left behind, and how do you address it safely?”
Key indications
- Inflammatory or rheumatoid synovitis refractory to optimised medical therapy for at least 6 months with preserved cartilage
- PVNS / diffuse-type TGCT — localised (focal excision) versus diffuse (total synovectomy)
- Synovial chondromatosis with mechanical symptoms — synovectomy plus removal of all loose bodies
- Haemophilic synovitis with recurrent bleeds despite prophylaxis; septic arthritis debridement as an adjunct
Localised vs diffuse PVNS
- Localised (nodular): focal intra-articular nodule, often pedunculated — simple or arthroscopic excision, low recurrence
- Diffuse: carpets synovium, frequent posterior involvement — requires total synovectomy, recurrence 8-46%
- Knee is the most commonly affected joint (around 80% of PVNS)
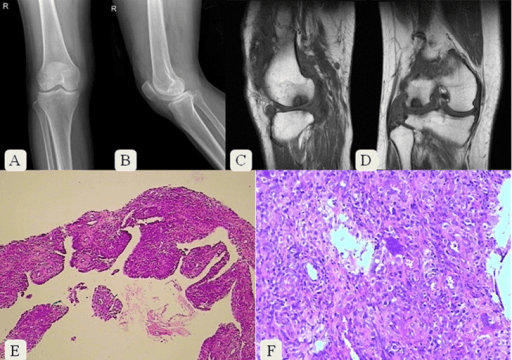
- MRI hallmark: low signal on T1 and T2 with blooming on gradient-echo from haemosiderin
Open vs arthroscopic
- Arthroscopic: faster recovery, less stiffness, lower wound morbidity; technically demanding posteriorly
- Open: more complete clearance for diffuse or posterior disease and a large loose-body burden; higher arthrofibrosis
- Combined anterior arthroscopic plus open posterior is the strategy of choice for diffuse PVNS with posterior disease
- Rheumatoid knee: arthroscopy gives equal pain relief but somewhat more recurrence and radiographic progression than open (Chalmers); favoured for lower morbidity (Matsui)
Critical operative steps
- Systematic compartment-by-compartment clearance: supra-patellar pouch, both gutters, notch, fat pad, posterior recesses
- Superolateral portal for the pouch; interchange anterior portals to reach the gutter periphery
- Posterior compartment via posteromedial (trans-notch Gillquist) and posterolateral portals with the knee flexed 90 degrees
- Shaver window always faces the joint, never the posterior capsule; use a posterior cannula or retractor
- Low threshold to convert to an open posterior approach for diffuse posterior disease
- Remove and account for all loose bodies in synovial chondromatosis
Danger zones
- Popliteal neurovascular bundle behind the posterior capsule — flex the knee 90 degrees, stay on the capsule, never push instruments blindly
- Common peroneal nerve behind biceps femoris at the posterolateral portal — identify and protect, avoid foot drop
- Saphenous nerve and infrapatellar branch at medial portals — use longitudinal incisions and careful portal placement
- Incomplete posterior or peripheral synovectomy — the principal driver of recurrence in diffuse disease
- Arthrofibrosis — the commonest functional complication, worse after extensive open synovectomy
Adjuvant and systemic therapy
- Radiosynovectomy (intra-articular isotope, e.g. yttrium-90) and external-beam radiotherapy lower recurrence in diffuse PVNS
- Surgery plus radiotherapy reduces recurrence versus surgery alone for diffuse PVNS of the knee (Mollon meta-analysis, 2015)
- Pexidartinib (CSF1R inhibitor) for symptomatic unresectable or recurrent diffuse-type TGCT (ENLIVEN trial) — monitor hepatotoxicity
- Radiosynovectomy is a mainstay or alternative in haemophilic synovitis
Haemophilia peri-operative management
- Plan jointly with haematology — this is as much a haematological as a surgical procedure
- Correct factor to 80-100% before incision and maintain through the rehabilitation period
- Screen for inhibitors pre-operatively — presence changes the entire plan
- Meticulous haemostasis and early motion; haemarthrosis precipitates both rebleed and stiffness
High-yield concepts
- Always distinguish localised from diffuse PVNS — it dictates the whole operative plan and prognosis
- The posterior compartment is the answer when asked about recurrence and surgical difficulty
- Cite Mollon (2015) for surgery plus radiotherapy reducing diffuse PVNS recurrence
- Know pexidartinib and ENLIVEN for unresectable diffuse-type TGCT
- Haemophilia equals factor cover plus inhibitor screen plus haematology before any synovectomy
Background & Evidence
Epidemiology. The knee is by far the most commonly affected joint in pigmented villonodular synovitis, involved in around 80% of cases. Diffuse disease recurs in a reported 8-46% of patients after surgery, driven principally by incomplete excision — most often in the posterior compartment. Pathoanatomy and histology (PVNS / diffuse-type TGCT). Histology shows hyperplastic synovium with haemosiderin-laden macrophages, multinucleate giant cells, foam cells and a mononuclear stromal cell population. The underlying biology is driven by CSF1 overexpression that recruits CSF1R-positive cells — the rationale for pexidartinib. MRI is the investigation of choice: low signal on T1 and T2 with characteristic blooming on gradient-echo (susceptibility) sequences from haemosiderin, and it defines disease extent and posterior involvement. The localised-versus-diffuse distinction is the single most important factor for planning and prognosis.
- Localised (nodular)
- Focal intra-articular nodule, often pedunculated
- Diffuse
- Carpets the synovium; frequent posterior compartment involvement
- Localised (nodular)
- Local excision, often arthroscopic
- Diffuse
- Total synovectomy; combined anterior plus open posterior when posterior disease present
- Localised (nodular)
- Low
- Diffuse
- 8-46%
- Localised (nodular)
- Focal low-signal nodule
- Diffuse
- Diffuse low-signal T1/T2 synovium with blooming on gradient-echo
- Synovium
- Active intrasynovial metaplasia
- Loose bodies
- None
- Management
- Synovectomy alone
- Synovium
- Transitional (active)
- Loose bodies
- Present
- Management
- Synovectomy plus loose-body removal
- Synovium
- Quiescent
- Loose bodies
- Multiple free loose bodies
- Management
- Loose-body removal (plus synovectomy of any residual active disease)
References
Combined synovectomy and peri-operative radiotherapy reduce recurrence of diffuse PVNS of the knee
- Individual-patient meta-analysis: 35 studies, 630 patients; overall recurrence 137/630 (21.8%)
- Diffuse PVNS recurrence reduced by open synovectomy (OR 0.47) and most by combined open plus arthroscopic synovectomy (OR 0.19) versus arthroscopy alone
- Peri-operative radiotherapy reduced diffuse-PVNS recurrence (OR 0.31); surgical approach did not affect localised disease
Long-term follow-up of primary and recurrent PVNS — recurrence increases with time
- 107 patients (localised 27%, diffuse 70%); knee affected in 88%
- Diffuse PVNS recurrence-free survival 69% at 1 year but only 32% at 5 years
- PVNS becomes progressively harder to cure over time; SF-36 general-health scores reduced versus population norms
Subtotal synovectomy plus external-beam radiotherapy gives durable control of diffuse knee PVNS
- 8 patients with diffuse PVNS treated by subtotal arthroscopic plus open posterior synovectomy and adjuvant external-beam radiotherapy
- Single recurrence (12.5%) at mean 8.6-year follow-up; no radiographic arthritis progression and no major radiotherapy late effects
- Supports a planned combined-approach plus radiotherapy pathway for diffuse disease
ENLIVEN: pexidartinib (CSF1R inhibitor) for advanced tenosynovial giant cell tumour
- Randomised phase 3 trial, 120 patients with symptomatic TGCT not amenable to surgery
- Overall response at week 25 by RECIST: 39% (24/61) with pexidartinib versus 0% with placebo (p less than 0.0001)
- Mixed or cholestatic hepatotoxicity is an identified risk requiring liver-function monitoring (enrolment stopped early for this)
Rheumatoid synovectomy — arthroscopic versus open: does approach matter?
- Meta-analysis of 58 studies, 2589 patients, mean 6.1-year follow-up (knees and elbows)
- Arthroscopic synovectomy gave similar pain relief but more frequent recurrence of synovitis and radiographic progression than open synovectomy
- Advanced pre-operative degenerative change did not predict worse pain or greater need for later arthroplasty
Primary arthroscopic synovectomy for PVNS of the knee — recurrence and function at mean 7 years
Primary arthroscopic synovectomy series (16 nodular, 7 diffuse) reporting only 2 recurrences among 21 reviewed patients at mean seven-year follow-up, with significantly improved Tegner-Lysholm scores — confirming arthroscopy can control even diffuse disease in selected hands while preserving function.
Lowering the recurrence rate in PVNS — a series of 120 resections
Large single-centre surgical series (120 resections) built on meticulous open anterior-and-posterior synovectomy including the popliteal space, achieving an 18% recurrence rate (over 90% recurring within 3 years) and emphasising complete resection to reduce recurrence of PVNS.
Arthroscopic management of knee synovial chondromatosis — systematic review of outcomes and recurrence
Systematic review of arthroscopic synovectomy and loose-body removal for synovial chondromatosis (84 patients; 22.6% recurrence, predominantly after loose-body removal alone and lower when synovectomy was added), underlining that active synovial metaplasia drives recurrence.
Synovitis in haemophilia — preventing, detecting and treating joint bleeds
Review of the bleed-synovitis cycle and the role of radiosynovectomy, chemical synovectomy and arthroscopic synovectomy in haemophilic arthropathy.
Arthroscopic versus open synovectomy in the rheumatoid knee
Early comparative study of arthroscopic and open synovectomy in the rheumatoid knee, informing the lower-morbidity preference for the arthroscopic approach.