Displaced intra-articular calcaneal fractures | L-shaped full-thickness flap | Sural nerve at risk
- Full-thickness flap is non-negotiable. The L-shaped incision (Benirschke-Sangeorzan) elevates skin, subcutaneous tissue and periosteum as a SINGLE UNIT straight off bone in a sharp subperiosteal plane. The lateral calcaneal artery (terminal branch of the peroneal artery) supplies the flap apex — a thin or undermined flap devascularises the skin and necroses.
- Time the surgery to the soft tissues, not the calendar. Wait until swelling settles and the wrinkle sign is positive (skin wrinkles when the ankle is moved). Operating very early is associated with more wound complications (De Boer 2017). EXCEPTION — a tongue-type fragment tenting the posterior skin is a surgical emergency: the skin will necrose under tension and needs urgent reduction.
- The sural nerve runs in the posterior limb. It travels with the lesser saphenous vein in the subcutaneous fat — either identify and protect it within the flap, or divide it sharply and bury the proximal stump in muscle. Permanent lateral-foot/heel numbness occurs in roughly 10–20% regardless of strategy.
- Posterior-facet reduction is the goal. Subtalar (posterior facet) articular congruity drives outcome. The Sanders CT classification grades posterior-facet comminution: I non-displaced, II two-part, III three-part, IV four-or-more-part. Sanders 1993 achieved anatomic reduction in 86% of type II, 60% of type III and 0% of type IV.
- The indication is selective. Displaced intra-articular Sanders II–III in a HEALTHY patient. The Buckley 2002 RCT found NO overall difference between ORIF and nonoperative care, but operatively-treated patients NOT on workers' compensation — and women, younger patients, and those with a step-off of 2mm or less — did significantly better.
- Contraindications / high wound-risk hosts. Active smoking, poorly-controlled diabetes, peripheral arterial disease, severe soft-tissue injury, and Sanders IV (anatomic reduction essentially unachievable, 9% good/excellent). In these, favour nonoperative care or a less-invasive (sinus tarsi) approach.
When & Why
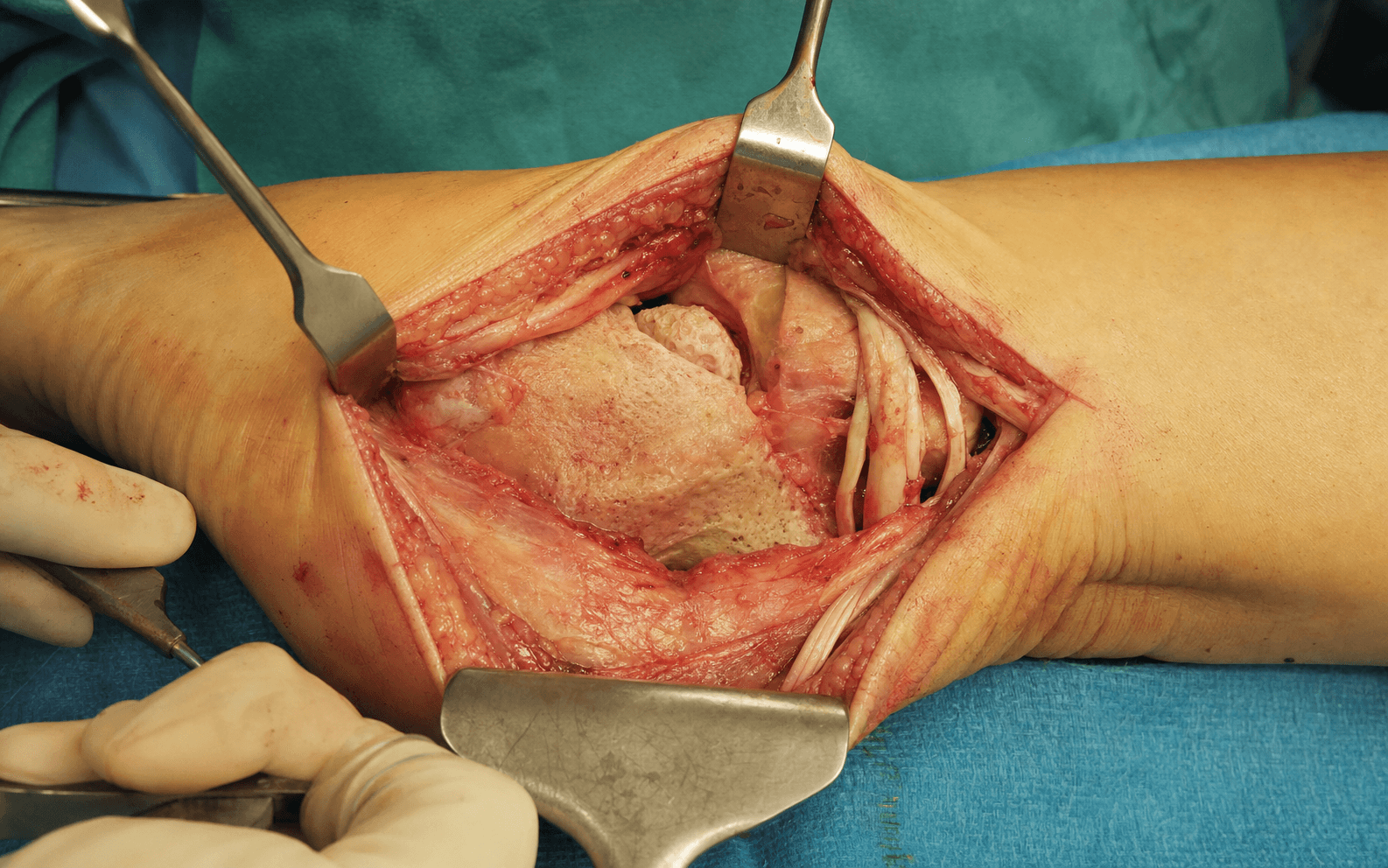
What it exposes. The lateral extensile (extended lateral) approach, popularised by Benirschke and Sangeorzan in the early 1990s (building on Palmer 1948), gives the most complete exposure for open reduction and internal fixation of displaced intra-articular calcaneal fractures. It displays the posterior facet (subtalar joint articular surface), the angle of Gissane, the lateral calcaneal wall, the calcaneal body and the calcaneocuboid joint — everything needed for direct anatomic reduction of a comminuted joint. Why this approach (and not a smaller one). Its singular advantage is complete exposure of the posterior facet for direct, visualised reduction. The trade-off is a high wound-complication rate (around 25% — Backes 2013). That morbidity has driven minimally-invasive alternatives: meta-analysis shows the sinus tarsi approach restores Böhler/Gissane angles and calcaneal dimensions equally but with roughly one-third the wound-complication risk (Attenasio 2024, RR 2.82; Lv 2020). The extensile approach is therefore reserved for fractures that genuinely need its wider exposure — highly comminuted Sanders III–IV and patterns with anterior-process or calcaneocuboid involvement. Why operative management is selective, not routine. The landmark Canadian multicentre RCT (Buckley 2002, 424 patients) found no overall difference between ORIF and nonoperative care (SF-36 64.7 nonoperative vs 68.7 operative, p = 0.13). Benefit was confined to subgroups — patients NOT on workers' compensation, women, younger patients, and those whose reduction achieved a step-off of 2mm or less. A companion analysis (Csizy/Buckley 2003) showed nonoperative treatment carried a roughly six-fold higher likelihood of needing late subtalar fusion, and that Sanders IV pattern and a Böhler angle below 0 degrees were the strongest predictors of fusion. Current consensus: selective ORIF for displaced Sanders II–III in healthy patients with surgeon expertise; nonoperative care for non-displaced (Sanders I), Sanders IV (anatomic reduction unachievable), high-risk hosts, and elderly/low-demand patients. Position & landmarks. Lateral decubitus, injured side up. Support with a bean-bag and lateral positioners; place an axillary roll under the dependent axilla and a pillow between the knees; pad all bony prominences. Flex the knee 20–30° to relax gastrocnemius; hold the ankle neutral so the lateral hindfoot faces the ceiling. A thigh tourniquet (300–350 mmHg) is used selectively — some surgeons keep it down to preserve flap perfusion. Gravity assists by letting the flap fall away from the field, and the C-arm comes in easily from posterior.
The Exposure
Work down through the layers along the L-shaped line, raising skin, subcutaneous tissue and periosteum as a single full-thickness flap straight off bone, then read and reduce the fracture against the intact sustentaculum tali.
Exposure and reduction sequence
- Confirm a positive wrinkle sign before incising — passively dorsiflex/plantarflex the ankle; if the lateral hindfoot skin wrinkles, oedema has resolved and it is safe to proceed. If the skin stays tight and shiny, delay further.
- Mark the L-shape: the posterior (vertical) limb runs along the lateral border of the tendo-Achilles from 8–10 cm proximal to the tuberosity; the horizontal limb follows the junction of lateral and plantar skin to the calcaneocuboid joint. The two limbs meet in a gentle curve (not a sharp angle) at the posterolateral corner — this protects the flap apex.
- Palpate and mark the lateral malleolus (superior landmark), the peroneal tendons posterior to it, and the calcaneocuboid joint anteriorly (the anterior limit of the incision).
- With a #10 or #15 blade, cut the L-shaped line and immediately deepen through subcutaneous fat directly onto calcaneal bone in a single cut.
- Skin, subcutaneous tissue and periosteum are raised as ONE UNIT — do NOT dissect between layers. The flap's blood supply (subcutaneous plexus and periosteal vessels) reaches the skin from deep; separating periosteum from the skin devascularises it (necrosis risk 15–25%).
- Teaching check: if you can see white calcaneal cortex easily before clearing the haematoma, your flap is too thin — the periosteum should come up WITH the flap, not stay on bone.
- The sural nerve runs with the lesser saphenous vein in the subcutaneous fat of the posterior limb — it is unavoidable and must be deliberately managed.
- Option A — identify and protect: dissect it out, gently retract it anteriorly within the flap. Keeps the chance of normal sensation but the small (2–3 mm), variable nerve can still be injured by traction or cautery, and an unrecognised partial injury is the type most prone to a painful neuroma.
- Option B — deliberate sharp division with proximal-stump burial in muscle: predictable area of permanent numbness, places the cut end deep and away from shoe pressure, tends to lower symptomatic-neuroma risk. Many experienced surgeons prefer this.
- Either way, expect roughly 10–20% permanent lateral-foot numbness. There is no high-quality randomised comparison and no consensus — this is shared decision-making at consent.
- Insert a wide periosteal elevator (Cobb or Key) at the plantar (inferior) edge and strip the periosteum OFF the calcaneus, keeping the periosteum WITH the flap — the true subperiosteal plane.
- Work inferior to superior, so the flap hinges along its superior border near the peroneal tendons (like turning the page of a book).
- The lateral calcaneal artery (terminal branch of the peroneal artery) feeds the flap apex — keep the elevator on bone, never undermine or thin the flap, and ligate only the small crossing vessels you meet.
- Retract the flap with K-wires bent into adjacent bone (talus, cuboid, fibula), or with Army-Navy retractors / stay sutures through the flap margin to distribute tension.
- Never use Weitlaner or self-retaining retractors on the skin edges — they crush and ischaemia the flap. Keep the flap moist with saline-soaked sponges and release retraction periodically.
- The entire lateral calcaneal wall, posterior facet, angle of Gissane and calcaneocuboid joint are now exposed.
- Evacuate the fracture haematoma and irrigate.
- Read the fragments against the pre-operative CT: the lateral wall (usually blown out laterally — widened heel), the posterior facet (depressed and comminuted, the intra-articular step-off), the sustentaculum tali (medial, usually intact — the reduction template) and the tuberosity (varus/valgus position).
- Identify the angle of Gissane (the strut where the posterior facet meets the anterior process) and clear debris off the posterior-facet cartilage so reduction can be judged under direct vision.
- Restore height and length: the Essex-Lopresti maneuver — insert a Steinmann pin or Schanz screw through the tuberosity and apply traction (pull posteriorly and inferiorly) to disimpact the posterior facet; use a bone tamp/lever to lift depressed fragments. Check lateral fluoroscopy — Böhler angle should climb back toward 25–40°.
- Reduce the posterior facet (the outcome-determining step): reduce the fragments to the intact sustentaculum tali (the medial reference), hold with pointed reduction clamps, and confirm under direct vision (goal: step-off of 2mm or less). Provisional K-wires or 2.0–2.7 mm lag screws.
- Correct varus/valgus on the axial view (varus is common — the tuberosity tilts medially); re-impact the lateral wall medially to restore heel width.
- Apply a low-profile lateral calcaneal locking plate (proximal screws into the posterior facet/sustentaculum for interfragmentary compression, middle screws into the body, distal screws into the anterior process if the plate runs forward). Add lag screws across the posterior facet and bicortical tuberosity screws engaging the medial cortex; locking screws help in osteoporotic bone.
- Graft large post-reduction voids with cancellous autograft (iliac crest), allograft chips, or a calcium phosphate/sulphate substitute.
- Confirm on lateral, axial and Broden (10/20/30/40°) fluoroscopy — Böhler/Gissane restored, no intra-articular screw penetration.
- Close tension-free over a closed suction drain (protective against wound infection — Backes 2013); use vertical-mattress nylon (3-0/4-0) to evert the edges, remove sutures at 3–4 weeks (delayed vs the usual 10–14 days for this high-risk wound). Bulky compressive dressing, posterior splint, and strict elevation above heart level.
Wound complications are the dominant threat to a good result regardless of how perfect the reduction is — around 25% wound infection with this approach (Backes 2013), and roughly three times the risk of a sinus tarsi approach (Attenasio 2024, RR 2.82). Four principles: (1) time surgery to the soft tissues — wait for the wrinkle sign, except a tongue-type fragment tenting the posterior skin which is an emergency; (2) full-thickness, no-touch, no-undermining flap on bone, perfused at its apex by the lateral calcaneal artery; (3) optimise the host — smoking cessation and glycaemic control; (4) early wound surveillance at 48 hours — dusky, cool or blistered skin means impending necrosis: act with offloading, negative-pressure wound therapy or debridement.
Meta-analysis (Attenasio 2024) shows the extensile lateral and sinus tarsi approaches restore Böhler/Gissane angles and calcaneal dimensions equally — so the choice of approach changes the wound risk, not the radiographic result. Reserve the extensile lateral for fractures (highly comminuted Sanders III–IV, anterior-process/calcaneocuboid involvement) that genuinely need full posterior-facet exposure.
It is the terminal branch of the peroneal artery, running roughly midway between the lateral malleolus and the Achilles, and it perfuses the flap apex. Keep the full-thickness flap on bone, do not undermine, and avoid retractor pressure on the apex — a thin or apically crushed flap necroses.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Sural nerve with the lesser saphenous vein — 10–20% permanent lateral-foot numbness
- How to protect it
- Identify and protect within the flap, or divide sharply and bury the stump in muscle; avoid traction and cautery near it
- Structure at risk
- Lateral calcaneal artery (terminal branch of the peroneal artery) — the flap's lifeline
- How to protect it
- Full-thickness subperiosteal flap kept on bone; never undermine or thin; avoid retractor pressure at the apex
- Structure at risk
- Peroneal tendons (brevis and longus) behind the lateral malleolus
- How to protect it
- Stay inferior to the tendons during elevation; they remain on the fibula, not in the flap (injury risk less than 1% if respected)
- Structure at risk
- Flap ischaemia and necrosis — the dominant complication
- How to protect it
- No self-retaining retractors on skin; K-wire / Army-Navy / stay-suture retraction; tension-free closure; closed suction drain
- Structure at risk
- Cartilage — residual step-off drives post-traumatic subtalar arthritis
- How to protect it
- Reduce to the intact sustentaculum tali; goal step-off of 2mm or less; confirm under direct vision and on Broden views
Sural nerve — the unavoidable structure. The sural nerve (pure sensory, lateral foot and heel) descends between the gastrocnemius heads, pierces the deep fascia 10–15 cm proximal to the lateral malleolus, and runs subcutaneously with the lesser saphenous vein — directly in the path of the posterior limb. Symptomatic problems (numbness, dysaesthesia, painful neuroma) occur in roughly 10–20% whether the nerve is preserved or deliberately divided. Preservation keeps the chance of normal sensation but risks an unrecognised partial injury (the type most prone to a painful neuroma). Deliberate division with deep stump burial gives a predictable area of permanent numbness and tends to lower symptomatic-neuroma risk. There is no consensus and no high-quality randomised comparison — counsel the patient and document the shared decision. Extensile options. The approach already runs from the tuberosity posteriorly to the calcaneocuboid joint anteriorly, and from the subtalar joint superiorly to the plantar surface inferiorly. Extend proximally along the Achilles for better control of a posterior tuberosity/tongue fragment. When the posterior facet can be reduced indirectly, the limited sinus tarsi approach is the lower-morbidity alternative — same radiographic restoration, roughly one-third the wound risk. Closure pearls. Deflate the tourniquet and achieve haemostasis; lower the flap without tension and confirm the edges are pink with brisk capillary refill (do NOT close a non-viable flap — use NPWT and delayed closure/skin graft). Reapproximate periosteum where possible with 2-0 absorbable suture, close subcutaneously with 3-0 absorbable, and close skin with vertical-mattress nylon (evert the edges; avoid staples). Leave a closed suction drain (protective — Backes 2013). Remove sutures at 3–4 weeks. Bulky dressing, posterior splint, and strict elevation above heart level is the single most important early wound-protective measure. Complications
- Rate / timing
- ~25% (Backes 2013: 11% superficial, 14% deep); early post-op
- Management
- Inspect the wound at 48 h. Superficial: local care, oral antibiotics (cephalexin/clindamycin). Deep: return to OR for washout, IV antibiotics (vancomycin if MRSA), NPWT, hardware salvage or removal
- Rate / timing
- 2–5%; early
- Management
- Early debridement of non-viable tissue, NPWT; small defects (less than 2–3 cm) heal by secondary intention, medium (3–5 cm) skin graft, large (greater than 5 cm) local/free flap
- Rate / timing
- 10–20% permanent numbness; any time
- Management
- Neuropraxia recovers over 6–12 months; neuropathic analgesia (gabapentin/pregabalin); painful neuroma — excision and proximal-stump burial
- Rate / timing
- ~40–50% long-term; tracks with initial injury severity more than reduction (Csizy 2003)
- Management
- Conservative first — footwear/orthosis, NSAIDs, image-guided steroid injection; subtalar arthrodesis if refractory (in-situ when height maintained, distraction bone-block when height lost)
- Rate / timing
- Early — inadequate fixation or poor bone
- Management
- Revision ORIF if less than 4 weeks; observe and plan late subtalar fusion if beyond
- Rate / timing
- Late
- Management
- Shoe modification or lateral-wall ostectomy for widening; corrective osteotomy or fusion in corrected position for varus/valgus
- Rate / timing
- 10–15%; late
- Management
- Remove plate and screws after union — wait greater than 12 months (calcanei heal slowly)
Procedures Through This Approach
- Calcaneal fractures (clinical topic) — the condition this approach treats; selection of operative vs nonoperative care.
- ORIF of displaced intra-articular calcaneal fractures (Sanders II–III in a healthy host) — the principal operation: posterior-facet reduction to the sustentaculum, lateral-wall and height/length restoration, low-profile lateral plating.
- Bone grafting of large post-reduction metaphyseal voids (autograft, allograft, or calcium phosphate/sulphate substitute).
- Primary subtalar arthrodesis for highly comminuted Sanders IV fractures (anatomic reduction essentially unachievable) — controversial, done through the same exposure in one stage.
- Lateral-wall ostectomy for symptomatic heel widening after malunion (cosmetic/shoe-fit improvement).
Viva & Exam Focus
WRINKLEWRINKLE — soft-tissue readiness before calcaneal ORIF
FLAPFLAP — full-thickness flap elevation technique
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old manual labourer (smoker, 1 pack per day for 15 years) presents 3 days after a fall from a ladder with a displaced intra-articular calcaneal fracture. CT shows a Sanders type III pattern. He is keen to be operated on tomorrow 'to get back to work'. Soft-tissue exam: swollen hindfoot, tight shiny skin, no wrinkle sign, clear fracture blisters on the lateral heel. What is your management plan, and how do you counsel him about smoking and surgical timing?”
“You performed calcaneal ORIF via the lateral extensile approach for a Sanders type III fracture. Intra-operative fluoroscopy showed anatomic posterior-facet reduction and the Böhler angle was restored to 32 degrees (pre-op 12 degrees). The wound healed and he returned to full weight-bearing at 12 weeks. Now at 18 months he has persistent lateral hindfoot pain (VAS 7/10), worse on uneven ground. Ankle ROM is normal, but subtalar motion is reduced to about 5 degrees of inversion/eversion. Radiographs show maintained alignment and intact hardware but subtalar joint-space narrowing and subchondral sclerosis. What has developed, why did it occur despite anatomic reduction, and what is your plan?”
“You are consenting a 28-year-old woman (non-smoker, active runner) for ORIF of a Sanders type II fracture with a 5 mm step-off, 12 days after injury with a positive wrinkle sign. She has read that some surgeons deliberately cut the sural nerve while others try to preserve it, and asks for your approach and the reasoning. How do you counsel her on sural nerve management?”
Critical anatomy
- Sural nerve runs IN the posterior limb of the incision (with the lesser saphenous vein); purely sensory (lateral foot/heel); 10–20% injury regardless of preservation vs division
- Full-thickness flap = skin + subcutaneous + periosteum as a single unit; the lateral calcaneal artery (terminal peroneal branch) perfuses the apex — a thin/undermined flap necroses
- Posterior facet = subtalar articular surface; anatomic reduction (step-off 2mm or less) determines outcome
- Sustentaculum tali = medial fragment, usually intact — the reduction template for the posterior facet
- Böhler angle normal 25–40° (fracture often less than 20° or negative); Gissane angle normal 120–145°
Selection (selective, not routine)
- Operate on Sanders II–III displaced intra-articular fractures in a healthy host (non-smoker, well-controlled/no diabetes, good soft-tissue envelope)
- Buckley 2002 RCT (n=424): no overall difference vs nonoperative; benefit confined to non-workers'-compensation patients, women, younger patients, step-off 2mm or less
- Nonoperative for Sanders I, Sanders IV (0% anatomic reduction — Sanders 1993), high-risk hosts, elderly/low-demand (more late subtalar fusions — Csizy 2003)
- Delay elective surgery for the wrinkle sign; very early surgery brings more wound complications (De Boer 2017) — but a tongue-type fragment tenting the skin is an emergency
- Sinus tarsi approach gives equivalent radiographic reduction with about one-third the wound risk (Attenasio 2024, RR 2.82)
The exposure
- Position: lateral decubitus, injured side up, ankle neutral, thigh tourniquet selective (many keep it down to protect flap perfusion)
- Incision: L-shaped — posterior limb along the Achilles border 8–10 cm proximal; horizontal limb along the lateral/plantar skin junction to the calcaneocuboid joint; gentle curve at the corner
- Flap: elevate FULL-THICKNESS (skin + subcut + periosteum) subperiosteally, inferior to superior, hinging along the peroneal tendons; no crushing, keep moist
- Reduction sequence: (1) restore height/length (Essex-Lopresti, bone tamp), (2) reduce posterior facet to the sustentaculum (step-off 2mm or less), (3) correct varus/valgus, (4) re-impact the lateral wall
- Fixation: low-profile lateral locking plate, lag screws across the posterior facet, bone graft for large voids
- Closure: tension-free, vertical-mattress nylon, closed suction drain, sutures out at 3–4 weeks, strict elevation
Complications
- Wound complications ~25% (Backes 2013) — infection, dehiscence, necrosis — the dominant threat regardless of reduction quality
- Risk factors: smoking, poorly-controlled diabetes, higher ASA grade, very early surgery (De Boer 2017), thin/undermined flap, tension closure, no suction drain (Backes 2013)
- Sural nerve injury ~10–20% — permanent numbness (not functionally limiting); painful neuroma is the feared outcome
- Subtalar arthritis ~40–50% long-term — tracks with initial injury severity more than reduction quality (Csizy 2003); subtalar arthrodesis if conservative care fails
- Early wound surveillance at 48 h — dusky/cool/blistered skin is impending necrosis: act with offloading, NPWT or debridement
Evidence
- Buckley 2002 RCT (n=424): no overall difference ORIF vs nonoperative (SF-36 68.7 vs 64.7, p = 0.13); benefit in subgroups [PMID 12377902]
- Sanders 1993 (n=120): anatomic reduction 86/60/0% and good/excellent 73/70/9% for types II/III/IV — classification is descriptive AND prognostic [PMID 8472475]
- Backes 2013 (n=191): extensile-approach wound infection 24.6% (11% superficial, 14% deep); suction drain protective, higher ASA a risk factor [PMID 24281853]
- Attenasio 2024 meta-analysis (n=2086): wound complications RR 2.82 extensile vs sinus tarsi, equivalent radiographic reduction; Lv 2020 concurs [PMID 38729077 / 32728979]
- De Boer 2017 (n=560): tongue-type fractures threaten posterior skin; surgery within 2 days associated with more complications [PMID 29248185]
Power phrases
- "Wound complications are the dominant complication — around 25% (Backes 2013) — so patient selection, host optimisation and soft-tissue timing matter as much as the reduction"
- "Time surgery to the soft tissues, not the calendar — wait for the wrinkle sign; very early surgery brings more wounds (De Boer 2017) — but a tongue-type fragment tenting the skin is an emergency"
- "Full-thickness flap is mandatory — skin, subcutaneous tissue and periosteum as one unit straight off bone, fed at its apex by the lateral calcaneal artery; never undermine or thin"
- "Posterior-facet reduction is the goal (step-off 2mm or less, to the intact sustentaculum) but its feasibility is set by the pattern — 86% anatomic in Sanders II, 60% in III, 0% in IV (Sanders 1993)"
- "Operative management is selective — the Buckley RCT showed benefit only in subgroups; the sinus tarsi approach gives equivalent reduction with about one-third the wound risk (Attenasio 2024)"
References
Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: a prospective, randomized, controlled multicenter trial
- Multicentre RCT — 424 patients with 471 displaced intra-articular calcaneal fractures, randomised to ORIF via a lateral approach vs nonoperative care (ice, elevation, rest — no attempted closed reduction)
- No overall difference at 2 years: SF-36 64.7 (nonoperative) vs 68.7 (operative), p = 0.13; visual analogue scale 64.3 vs 68.6, p = 0.12
- After excluding workers'-compensation patients, several operative subgroups did significantly better: non-WCB patients (higher satisfaction, p = 0.001), women (p = 0.015), and younger patients, those with a moderately reduced Böhler angle, a comminuted fracture, light workload, or a post-reduction step-off of 2mm or less (p = 0.04)
Soft tissue complications and timing of surgery in patients with a tongue-type displaced intra-articular calcaneal fracture: an international retrospective cohort study
- International cohort — 560 patients with 632 displaced intra-articular calcaneal fractures (295 tongue-type, 337 non-tongue-type)
- Tongue-type fractures had a 1.2–3.4-fold higher rate of local wound complications and 2–8-fold more antibiotics, debridements, soft-tissue coverage and amputations — the posterior fragment tents and ischaemises the skin
- Patients operated within 2 days of injury had a higher risk of any complication (especially superficial infection) than those operated at 3–7 days; no difference between 3–7 and 8-or-more days
Wound infections following open reduction and internal fixation of calcaneal fractures with an extended lateral approach
- Retrospective case series — 191 closed unilateral calcaneal fractures treated by ORIF via the extended lateral approach (2000–2010)
- Postoperative wound infection in 47 patients (24.6%): 11.0% superficial and 13.6% deep — quantifying the high wound morbidity of this approach
- ASA class higher than 1 increased risk; placement of a closed suction drain was protective (15% vs 35% infection, p = 0.002); notably none of the classically-cited risk factors (including smoking and diabetes) reached significance in this cohort
Postoperative wound complications in extensile lateral approach versus sinus tarsi approach for calcaneal fractures: an updated meta-analysis
- PRISMA meta-analysis — 21 studies (4 RCTs, 17 cohorts), 2086 patients (1129 extensile lateral, 957 sinus tarsi)
- Wound complications were significantly more common with the extensile lateral approach (RR 2.82, 95% CI 2.00–3.98), with longer time to surgery, longer operative times and longer hospital stay; this excess risk is trending down in more recent series
- No significant difference between approaches in final Böhler angle, angle of Gissane, or calcaneal height/length/width — the two approaches restore bony anatomy equally
Operative treatment in 120 displaced intraarticular calcaneal fractures: results using a prognostic computed tomography scan classification
- Foundational paper defining the Sanders CT classification (coronal section through the widest part of the posterior facet): type I non-displaced, II two-part, III three-part, IV four-or-more-part / highly comminuted
- Anatomic articular reduction was achieved in 86% of type II, 60% of type III, and 0% of type IV fractures
- Excellent or good clinical results occurred in 73% of type II, 70% of type III, and only 9% of type IV fractures; a clear surgeon learning curve was demonstrated (27% good/excellent in 1987 rising to 84% in 1990)