Sanders CT Classification | Extensile Lateral Approach | Wound Complication Management
- Sanders classification based on coronal CT through widest posterior facet
- Bohler angle under 20 degrees predicts poor outcome with conservative treatment
- Extensile lateral approach provides best exposure but 20-30% wound complications
- ORIF timing: Wait 10-21 days for swelling to resolve (wrinkle test positive)
- Primary subtalar fusion for Sanders IV in heavy laborers over 50 years
- “Always assess for lumbar spine injury (10% concurrent with bilateral calcaneal fractures)
- “Compartment syndrome in 10% - clinical diagnosis, fasciotomy if suspected
- “ORIF benefit is selective, not universal - pragmatic UK Heel Fracture Trial (Griffin 2014) showed no overall advantage; Canadian RCT (Buckley 2002) showed benefit in younger, non-compensation patients
- “Sinus tarsi approach alternative for Sanders II - lower wound complication rate

Sanders classification is CT-based. Type determined by number of fracture lines through posterior facet on coronal view. Type II (single line, 2 fragments) has best ORIF outcomes. Type IV (comminuted) consider primary fusion in older laborers.
Wait for swelling to resolve. ORIF performed at 10-21 days when wrinkle test positive (skin wrinkles with gentle pinch). Early surgery increases wound complications from 20% to over 40%. Document neurovascular status and soft tissue condition.
20-30% wound dehiscence with extensile lateral approach. Risk factors: smoking, diabetes, obesity, swelling. Sinus tarsi approach reduces risk to under 10% but limited to Sanders II. Meticulous soft tissue handling and delayed closure critical.
10% have lumbar spine fracture (bilateral calcaneal fractures increase to 25%). Always examine spine and order imaging if bilateral. Check for compartment syndrome (10%) - clinical diagnosis based on pain out of proportion and pain with passive toe dorsiflexion.
- Fracture Pattern
- Sanders I (all subtypes)
- Treatment
- NWB boot 6 weeks, progressive WB
- Key Pearl
- Excellent outcomes with conservative care
- Fracture Pattern
- Sanders II (single fracture line)
- Treatment
- ORIF extensile lateral at 10-21 days
- Key Pearl
- Best outcomes - restoration of height and width
- Fracture Pattern
- Sanders III (2 fracture lines)
- Treatment
- ORIF extensile lateral at 10-21 days
- Key Pearl
- Good outcomes but more challenging reduction
- Fracture Pattern
- Sanders IV (comminuted)
- Treatment
- Consider primary subtalar fusion
- Key Pearl
- Better than delayed fusion after failed ORIF
- Fracture Pattern
- Sanders II-IV displaced
- Treatment
- Conservative - NWB 6-8 weeks
- Key Pearl
- Functional outcomes acceptable despite deformity
Overview and Epidemiology
Calcaneal fractures are devastating injuries occurring primarily in working-age males (mean age 35-45 years) from high-energy axial loading (falls from height, motor vehicle accidents). The injury mechanism - axial load driving talus into calcaneus - produces a predictable fracture pattern with the sustentaculum tali remaining attached to talus while lateral and posterior fragments displace. Outcomes depend on articular involvement, age, occupation, and achieving anatomical reduction of posterior facet.
- Peak age: 30-50 years (working population)
- Male predominance: 75-80% of cases
- Fall from height: 60-70% (over 2 meters)
- Motor vehicle accident: 20-25%
- Other trauma: 10-15% (industrial, crush)
Most fractures occur in manual laborers and construction workers.
- Work disability: 30-40% never return to previous employment
- Subtalar arthritis: 50-70% by 2 years (Sanders III-IV)
- Persistent pain: 40-60% at 2 years despite treatment
- Healthcare cost: Substantial per-patient cost in high-income settings
- Bilateral fractures: 10% overall, 25% with lumbar spine injury
Economic impact includes lost productivity and long-term disability.
Pathophysiology and Mechanisms
The sustentaculum tali is the key to understanding calcaneal fracture patterns. This medial process remains attached to the talus via strong interosseous talocalcaneal ligament and deltoid ligament complex. During injury, the sustentaculum acts as a hinge - the primary fracture line runs lateral to it (primary fracture line of Sanders), and all other fragments displace relative to this stable medial fragment. This anatomical constant guides reduction - reduce all fragments to the sustentaculum fragment.
- Anatomical Detail
- Largest articular surface, bears 80% weight
- Fracture Relevance
- Fracture disruption causes subtalar arthritis
- Surgical Pearl
- Must restore to within 2mm step-off for good outcome
- Anatomical Detail
- Medial shelf, supports talar head
- Fracture Relevance
- Remains attached to talus - stable reference
- Surgical Pearl
- Reduce all fragments to sustentaculum position
- Anatomical Detail
- Forms lateral border, thin cortex
- Fracture Relevance
- Blowout fragment causes widening
- Surgical Pearl
- Restore height and width to prevent impingement
- Anatomical Detail
- Articulates with cuboid
- Fracture Relevance
- Separate injury (avulsion), not Sanders classification
- Surgical Pearl
- If isolated, treat conservatively
- Anatomical Detail
- Neurovascular bundle passage
- Fracture Relevance
- Risk of tarsal tunnel syndrome (5-10%)
- Surgical Pearl
- Decompress if acute compartment syndrome
Classification Systems
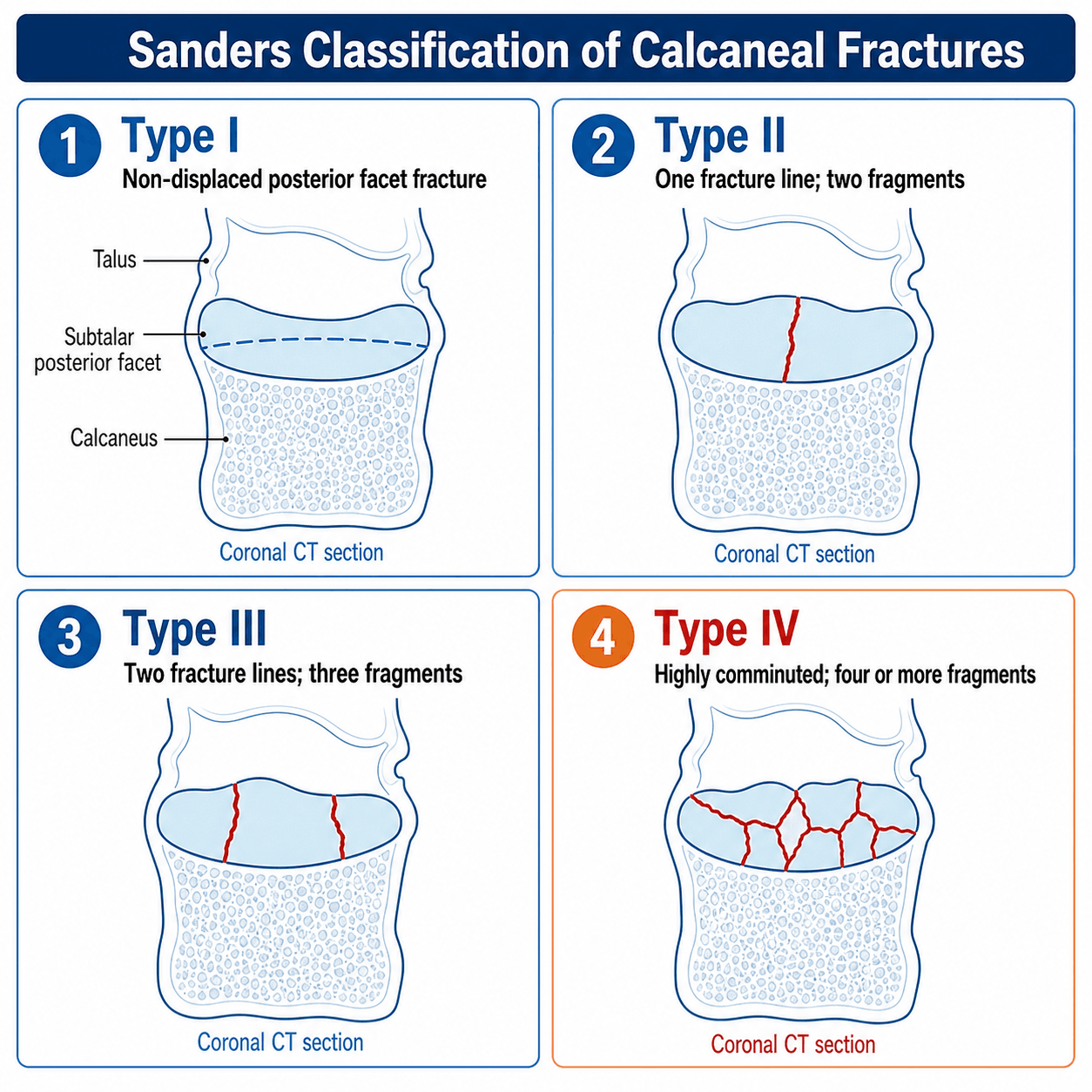

Sanders Classification (1993)
The gold standard classification for intra-articular calcaneal fractures, based on coronal CT through the widest portion of the posterior facet. Classification determines treatment and predicts outcomes.
Sanders classification is performed on coronal CT slice through widest posterior facet. Identify sustentaculum tali (medial, constant fragment). Count fracture lines from lateral to medial: A (lateral third), B (central third), C (medial third between central and sustentaculum). Subtypes based on which lines present: IIA (A only), IIB (B only), IIC (C only), IIIABC (all three lines present).
Clinical Assessment and Radiographic Evaluation
Mechanism:
- Fall from height (most common)
- Motor vehicle accident (dashboard injury)
- Industrial crush injury
Key questions:
- Height of fall (energy assessment)
- Bilateral injury? (always examine both feet)
- Back pain? (10% lumbar fracture with bilateral)
- Timing of injury (swelling progression)
- Medical comorbidities (diabetes, smoking, PVD)
- Occupation (manual labor affects treatment choice)
Inspection:
- Swelling and ecchymosis (lateral and plantar)
- Heel widening (compare to contralateral)
- Loss of normal heel contour
- Skin integrity (open fractures 5-10%)
- Fracture blisters (delay surgery)
Palpation:
- Tenderness over calcaneus
- Palpable step-off lateral wall
- Compartment assessment (firm, tense)
Neurovascular:
- Dorsalis pedis and posterior tibial pulses
- Sensation (tibial, sural, superficial peroneal)
- Pain with passive toe dorsiflexion (compartment syndrome)
10% of calcaneal fractures develop compartment syndrome. This is a clinical diagnosis - do not wait for pressure measurements. Key signs: pain out of proportion to injury, pain with passive toe dorsiflexion (stretches deep flexors), tense swollen foot. Presence of pulses does NOT exclude compartment syndrome. If suspected: urgent fasciotomy of all 9 foot compartments. Delayed diagnosis leads to clawing, contractures, and chronic pain.
- Distinguishing features
- Heel widening, plantar/lateral bruising, reduced Bohler angle, posterior facet involvement
- Key investigation
- Lateral/axial X-ray then fine-cut CT (Sanders classification)
- Why it matters
- Index diagnosis - drives operative vs non-operative decision
- Distinguishing features
- Localised tenderness, posterior facet spared, often lower-energy or avulsion
- Key investigation
- X-ray and CT; oblique views for anterior process
- Why it matters
- Usually managed non-operatively; not Sanders-classified
- Distinguishing features
- Pain anterior to calcaneus, deformity, talar dome tenderness
- Key investigation
- CT - high rate of associated injury and AVN risk
- Why it matters
- Different fixation and AVN counselling; commonly coexists
- Distinguishing features
- Insidious onset, low energy or repetitive load, positive squeeze test
- Key investigation
- MRI (marrow oedema) when X-ray normal
- Why it matters
- Non-operative; missing it delays diagnosis in athletes/elderly
- Distinguishing features
- Tenderness over ATFL, no bony point tenderness, intact Bohler angle
- Key investigation
- X-ray to exclude fracture (Ottawa rules)
- Why it matters
- Avoid mislabelling an occult fracture as a sprain
- Distinguishing features
- Palpable gap or bony fragment, weak plantarflexion, skin at risk posteriorly
- Key investigation
- Lateral X-ray; assess overlying skin urgently
- Why it matters
- Tuberosity avulsion threatens skin - may need urgent fixation
Investigations
Essential views:
- Lateral foot: Assess Bohler angle (normal 20-40 degrees) and Gissane angle (normal 120-145 degrees)
- Axial (Harris view): Assess varus/valgus angulation and calcaneal width
- AP and oblique foot: Evaluate anterior process and calcaneocuboid joint involvement
Measurements:
- Bohler angle under 20 degrees predicts poor outcome
- Compare calcaneal height and width to contralateral side
Protocol:
- Fine-cut (1-2mm) slices with coronal, sagittal, and axial reconstructions
- Coronal view through widest posterior facet is critical for Sanders classification
- 3D reconstruction helpful for surgical planning (not for classification)
Assessment:
- Sanders type and subtype determination
- Fracture line location and number of fragments
- Posterior facet step-off and displacement
- Lateral wall comminution and widening
- Calcaneocuboid joint involvement
- Timing
- Emergency Department (initial)
- Purpose
- Confirm fracture, assess displacement, measure angles
- Key Information
- Bohler angle, Gissane angle, calcaneal height/width, open fracture
- Timing
- Within 24-48 hours of presentation
- Purpose
- Sanders classification, surgical planning, assess comminution
- Key Information
- Sanders type, posterior facet fragments, lateral wall integrity, calcaneocuboid joint
- Timing
- If bilateral calcaneal fractures or back pain
- Purpose
- Rule out associated lumbar fracture (10-25% incidence)
- Key Information
- L1-L2 compression fracture most common (axial loading mechanism)
- Timing
- Rarely indicated
- Purpose
- Occult fracture, stress fracture, ligament injury assessment
- Key Information
- Useful if high clinical suspicion with negative X-ray, or for suspected bifurcate ligament injury
Management Algorithm
Non-Operative Treatment
Indications:
- Sanders Type I (non-displaced)
- Extra-articular fractures (anterior process, sustentaculum, body)
- Sanders IV elderly or low-demand patients
- Severe medical comorbidities precluding surgery
- Patient preference after informed consent
Conservative Protocol
- Non-weight bearing in CAM boot or short leg cast
- Elevate leg above heart level 23 hours/day first 2 weeks
- Ice therapy and compression
- Early ankle ROM exercises (plantarflexion/dorsiflexion)
- DVT prophylaxis (LMWH if immobilized, high-risk)
- Monitor for compartment syndrome first 48 hours
- Start protected weight bearing at 6 weeks
- Progress from partial (20kg) to full WB over 4 weeks
- Continue boot until 12 weeks
- Subtalar ROM exercises
- Gait re-education (avoid antalgic patterns)
- Full weight bearing in supportive footwear
- Heel cup or orthotic for persistent heel pain
- Gradual return to activities
- Consider subtalar fusion if persistent pain over 1 year
Understanding these conservative options helps guide treatment selection.
Sanders Type I: 85-90% good outcomes with conservative care. Sanders II-III displaced: 50-60% good outcomes (inferior to ORIF). Sanders IV: 40-50% good outcomes, similar to ORIF - conservative reasonable choice for low-demand elderly. Key prognostic factor: Bohler angle under 0 degrees predicts poor outcome regardless of treatment.
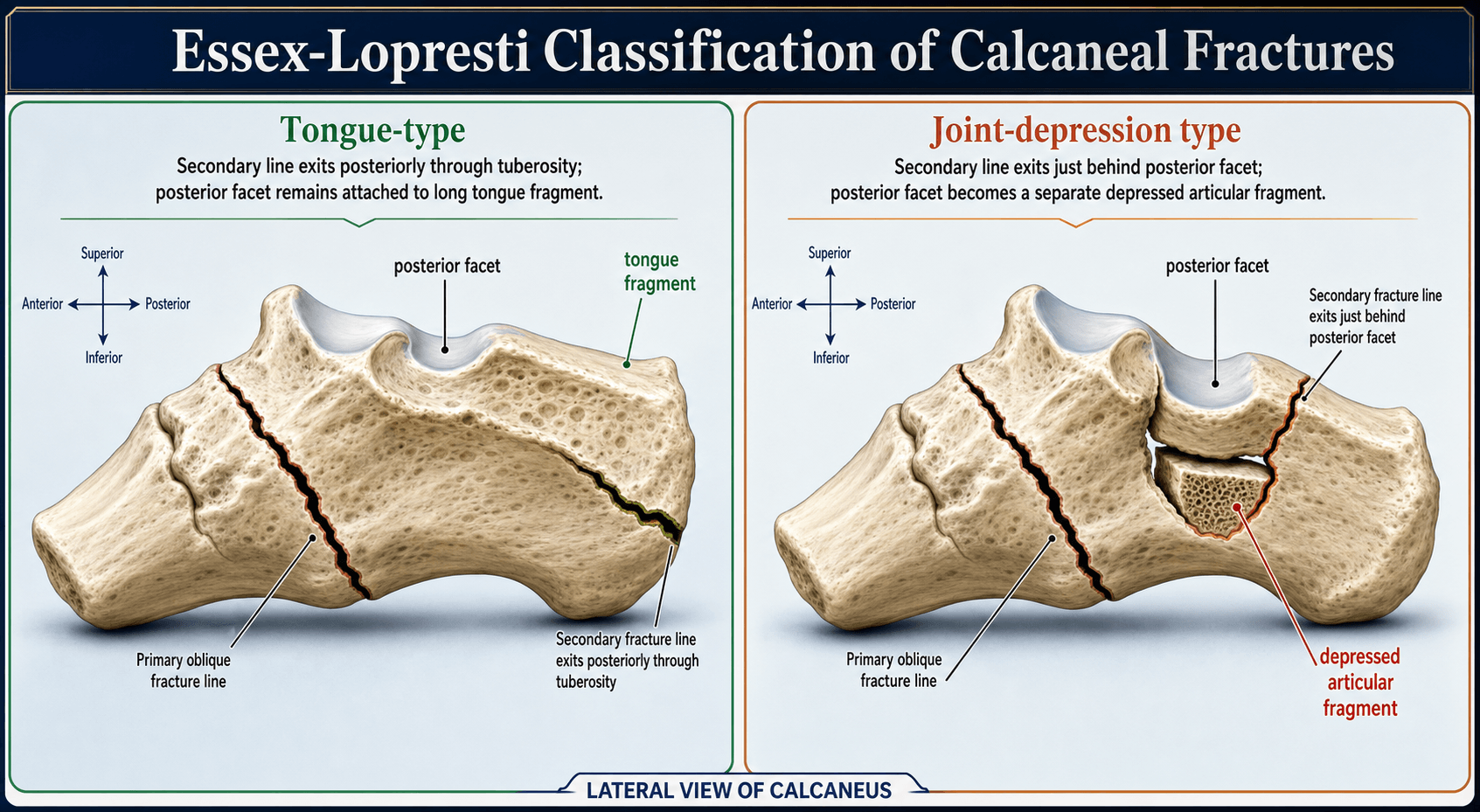
Tongue-Type Fractures: A Soft-Tissue Emergency
Most displaced intra-articular calcaneal fractures are operated in a delayed fashion (10-21 days, once the wrinkle test is positive). The important exception is the displaced tongue-type fracture (Essex-Lopresti), which can be a true soft-tissue emergency.
- Why it is urgent: in a tongue-type pattern the secondary fracture line exits posteriorly through the tuberosity, so the superior "tongue" fragment is pulled proximally by the Achilles. The sharp superior edge of this rotating fragment presses against and tents the posterior heel skin from the inside. Unrelieved, this causes pressure ischaemia and full-thickness posterior skin necrosis within hours to a couple of days, converting a closed injury into an open one over the worst possible soft-tissue envelope.
- Recognise it: a displaced tongue-type fracture on the lateral radiograph plus blanching, tenting, or a dusky/indented patch of skin over the posterosuperior heel. This patient is reduced urgently, not at 10-21 days.
- Essex-Lopresti / Westhues percutaneous reduction: with the knee flexed to relax the gastrocsoleus, a large Steinmann pin or Schanz screw is driven into the displaced tongue fragment along its long axis and used as a lever (joystick) to reduce the fragment - and the posterior facet attached to it - back down into position. The reduction is then secured percutaneously (the pin advanced across the fracture and/or supplementary lag screws). This immediately decompresses the threatened skin and can definitively fix simple tongue-type patterns without the extensile dissection.
- If the skin is already compromised, manage as an open injury (debridement, soft-tissue-led plan) rather than proceeding to formal ORIF through devitalised tissue.
Examiner question: "Which calcaneal fracture is a surgical emergency rather than a delayed operation?"
Answer: "A displaced tongue-type fracture threatening the posterior heel skin. The proximally pulled superior tuberosity fragment tents the skin and will cause full-thickness necrosis within hours to days. It needs urgent reduction - classically the Essex-Lopresti (Westhues) maneuver, levering the tongue fragment down with an axial Steinmann pin or Schanz screw and fixing percutaneously - to decompress the skin, rather than the usual 10-21 day soft-tissue wait."
Surgical Technique - ORIF via Extensile Lateral Approach
Alternative Fixation Techniques

Pre-operative Assessment and Planning
Optimal timing: 10-21 days post-injury
Reasons for delay:
- Allow soft tissue swelling to resolve
- Wrinkle test positive (skin wrinkles with gentle pinch)
- Fracture blisters to epithelialize
- Patient optimization (smoking cessation, glucose control)
Early surgery (under 7 days): 40-50% wound complication rate
Delayed surgery (over 3 weeks): Fracture fragment malunion, difficult reduction
Key risks to discuss:
- Wound complications: 20-30% (dehiscence, necrosis)
- Infection: 5-10% superficial, 2-5% deep
- Sural nerve injury: 5-10% (numbness lateral foot)
- Hardware prominence: 10-15% (may require removal)
- Subtalar arthritis: 30-50% by 5 years (disease, not surgery)
- Need for subtalar fusion: 15-25% within 5 years
- DVT/PE: 2-5% (prophylaxis given)
- Chronic pain: 30-40% despite anatomical reduction
Pre-operative Checklist
- Smoking cessation (minimum 4 weeks ideal, 2 weeks acceptable)
- Diabetic control (HbA1c under 8%)
- Nutrition optimization (albumin over 3.5)
- Weight loss if obese (BMI over 35 high risk)
- Review CT to template plate size and screw lengths
- Standard: Lateral calcaneal locking plate (7-9 holes)
- Screws: 3.5mm cortical and locking, 35-50mm lengths
- K-wires: 1.6mm and 2.0mm for provisional fixation
- Consider calcium phosphate bone void filler for voids
- C-arm fluoroscopy (confirm positioning before draping)
- Lamina spreaders or Schantz pins for distraction
- Dental picks or curettes for fracture debris removal
- Self-retaining retractors (avoid excessive tension)
- Headlight or surgical loupe magnification
Ensuring proper equipment facilitates successful reduction.
The wrinkle test determines surgical timing. Gently pinch lateral skin over fracture site - if skin wrinkles, swelling has resolved sufficiently for surgery. If skin remains tense and shiny (negative wrinkle test), delay surgery. Operating on swollen tissue increases wound complication rate from 20% to over 40%. No specific number of days - assess clinical swelling.




Complications
- Incidence
- 20-30% (ORIF), 0% (conservative)
- Risk Factors
- Smoking, diabetes, obesity, early surgery (under 10 days), extensile approach
- Management
- Local wound care, negative pressure therapy, delayed closure, skin graft if needed, flap rarely
- Incidence
- 5-10%
- Risk Factors
- Wound dehiscence, diabetes, immunosuppression, obesity
- Management
- Oral antibiotics, wound care, remove superficial sutures, allow drainage
- Incidence
- 2-5%
- Risk Factors
- Open fracture, wound dehiscence, diabetes, smoking
- Management
- IV antibiotics, surgical debridement, retain hardware if stable, remove if loose, bone culture
- Incidence
- 5-10%
- Risk Factors
- Extensile lateral approach, excessive retraction, direct laceration
- Management
- Numbness lateral foot - usually well-tolerated, no treatment, neuropathic pain rare
- Incidence
- 10% (acute injury)
- Risk Factors
- High-energy injury, crush mechanism, swelling, vascular injury
- Management
- Urgent fasciotomy all 9 compartments (medial, lateral, superficial/deep central, interosseous ×4)
- Incidence
- 30-50% by 5 years (all treatments)
- Risk Factors
- Sanders III-IV, step-off over 2mm, high-energy injury, age over 50
- Management
- Conservative initially (NSAIDs, injections), subtalar fusion if persistent pain limiting function
- Incidence
- 10-15%
- Risk Factors
- Lateral wall widening, hardware prominence, fibular impingement
- Management
- Conservative (NSAIDs, physio), hardware removal if prominent, lateral wall decompression osteotomy
- Incidence
- 10-15%
- Risk Factors
- Thin soft tissue, prominent plate, weight gain post-op
- Management
- Observation if asymptomatic, hardware removal after 12 months if symptomatic (fracture healed)
- Incidence
- 15-25% (conservative), 5-10% (ORIF)
- Risk Factors
- Inadequate reduction, loss of fixation, non-compliance NWB
- Management
- Salvage options: corrective osteotomy, subtalar fusion, triple arthrodesis
- Incidence
- 30-40% (all treatments)
- Risk Factors
- High-energy injury, Sanders IV, depression/anxiety, litigation
- Management
- Multidisciplinary pain management, psychological support, avoid repeat surgery unless clear indication
Calcaneal Malunion: Classification and Salvage
Malunion is the characteristic late consequence of a displaced fracture healed in a deformed position (more common after non-operative care, and after failed/lost ORIF). The deformity is multiplanar and its components drive distinct symptoms:
- Loss of calcaneal height → the talus settles into a more horizontal ("flat-top"/declined) position, causing anterior ankle impingement and loss of ankle dorsiflexion.
- Heel widening with a lateral wall exostosis → subfibular and peroneal impingement (lateral hindfoot pain, peroneal tendon irritation or subluxation).
- Hindfoot malalignment (usually varus, occasionally valgus).
- Post-traumatic subtalar arthritis.
Stephens-Sanders CT classification of calcaneal malunion matches the salvage to the deformity:
- Type I - lateral wall exostosis with subfibular/peroneal impingement, without significant subtalar arthritis → lateral wall exostectomy (± peroneal tenolysis).
- Type II - lateral exostosis plus subtalar arthritis, with acceptable overall alignment → exostectomy plus in-situ subtalar arthrodesis.
- Type III - the above plus hindfoot malalignment and loss of height → exostectomy plus corrective subtalar arthrodesis, using a distraction bone-block (interposition) subtalar arthrodesis to restore lost height, with a calcaneal osteotomy (e.g. Dwyer for fixed varus) to correct alignment.
The distraction bone-block subtalar arthrodesis interposes a tricortical graft in the distracted subtalar joint to restore talar declination - this is what relieves the anterior ankle impingement and recovers dorsiflexion that a simple in-situ fusion leaves behind. The high-risk group for needing this late fusion (presenting Bohler angle under 0 degrees, Sanders IV, heavy-labour Workers'-Compensation males, initial non-operative treatment) is exactly that defined in the Csizy/Buckley data cited above. (See the dedicated subtalar arthrodesis and malunion topics for fusion technique and general malunion principles.)
Key principle: calcaneal malunion is multiplanar (height, width, alignment, arthritis), so salvage is matched to the Stephens type - lateral wall exostectomy alone for impingement without arthritis (Type I), add in-situ subtalar fusion when arthritis supervenes (Type II), and add a distraction bone-block subtalar arthrodesis (± Dwyer osteotomy) to restore height/alignment in Type III. The trap is performing an in-situ fusion when height is lost: it fixes the arthritis but leaves the anterior ankle impingement and horizontal talus uncorrected.
Postoperative Care and Rehabilitation
Post-ORIF Rehabilitation Timeline
- Elevation: Leg above heart level continuously (pillows, CPM device)
- Ice: 20 minutes on, 40 minutes off around dressing
- NWB: Strict non-weight bearing, crutches or knee walker
- Pain control: Multimodal (paracetamol, NSAID, opioid prn)
- DVT prophylaxis: LMWH (enoxaparin 40mg daily) or DOAC
- Wound check: 48 hours (remove drain if present, mark ecchymosis)
- Discharge: When pain controlled, mobile NWB, safe at home
- NWB continues: 6 weeks minimum (fracture healing)
- Splint: Backslab first 2 weeks, then CAM boot (allows removal for hygiene)
- Wound check: Week 2 (assess healing, watch dehiscence), Week 3-4 (suture removal - delayed healing expected)
- Elevation: Continue elevating leg when seated (above heart level 6-8 hours/day)
- Ankle ROM: Gentle active plantarflexion/dorsiflexion in boot (avoid inversion/eversion)
- X-rays: 6 weeks (check hardware, no loss of reduction)
- DVT prophylaxis: Continue until mobile or 6 weeks
- Start PWB: 20-30kg (toe-touch) in boot at 6 weeks if X-ray shows healing
- Progress WB: Increase 10-20kg every 1-2 weeks based on pain tolerance
- FWB target: 10-12 weeks
- Boot weaning: Transition to supportive shoe with heel cup (12 weeks)
- Physical therapy: Gait re-education, subtalar/ankle ROM, strengthening (intrinsics, gastrocnemius)
- Swelling: Expect significant swelling with WB (compression sock, continue elevation when seated)
- Footwear: Supportive shoes with cushioned heel (avoid flat shoes, high heels)
- Orthotic: Custom orthotic or heel cup for persistent heel pain
- Activity progression: Walking → incline → stairs → jogging (if desired and pain-free)
- Work: Light duty 3-4 months, heavy labor 6-9 months
- Sport: Low-impact (cycling, swimming) 4-6 months, high-impact (running) 9-12 months
- Hardware removal: Consider if prominent and symptomatic after 12 months (fracture healed)
- Follow-up: 6 months, 1 year, then annually or prn
- X-rays: Annual for first 2 years (assess subtalar arthritis)
- Subtalar fusion: If progressive arthritis with pain limiting function (15-25% by 5 years)
- Chronic pain: Multidisciplinary if persists (pain clinic, psychology, physio)
- Realistic expectations: 30-40% have some persistent pain despite anatomical reduction
Long-term surveillance identifies late complications requiring intervention.
NWB for minimum 6 weeks is mandatory - calcaneal bone is cancellous and slow to heal. Early weight bearing (before 6 weeks) risks loss of reduction and fixation failure. PWB starts at 6 weeks only if X-ray shows early healing (fracture lines blurring). Progress slowly - aggressive WB causes swelling, pain, and potential secondary displacement. Many patients take 12-16 weeks to achieve comfortable FWB. Set expectations early.
Outcomes and Prognosis

- Good Prognosis
- Type I or II
- Poor Prognosis
- Type IV
- Impact
- Type predicts outcome regardless of treatment
- Good Prognosis
- Under 40 years
- Poor Prognosis
- Over 60 years
- Impact
- Younger patients tolerate residual stiffness better
- Good Prognosis
- Sedentary, light manual
- Poor Prognosis
- Heavy laborer, prolonged standing
- Impact
- Heavy labor 60% cannot return to same job
- Good Prognosis
- Step-off under 2mm
- Poor Prognosis
- Step-off over 2mm
- Impact
- Over 2mm step-off: 2x increased arthritis rate
- Good Prognosis
- Restored to over 20 degrees
- Poor Prognosis
- Remains under 15 degrees
- Impact
- Under 15 degrees: 3x worse functional score
- Good Prognosis
- Unilateral
- Poor Prognosis
- Bilateral
- Impact
- Bilateral: 50% worse function, disability higher
- Good Prognosis
- No claim
- Poor Prognosis
- Active claim
- Impact
- Compensation claim: 2x worse outcome scores
Counsel patients realistically: Even with perfect ORIF of Sanders II, 20-25% will have suboptimal outcomes. Sanders IV has poor outcomes regardless of treatment (40-50% good results with ORIF or conservative). Subtalar arthritis develops in 30-50% by 5 years (reflects injury severity, not treatment failure). Heavy laborers: Only 40-60% return to same occupation. Set expectations early to avoid dissatisfaction and chronic pain syndrome.
Guidelines, Registries & Global Practice
Global Epidemiology
- Figure
- Calcaneus is the most commonly fractured tarsal bone; ~60-75% are intra-articular
- Source
- Sanders R 1993 (PMID 8472475) and standard texts
- Figure
- Predominantly working-age men injured by axial loading (fall from height / road trauma)
- Source
- Tennent TD 2001 two-centre series (PMID 11476816): 76% male, 88% falls from height
- Figure
- Significantly lower health-related quality of life than population norms; chronic disability common, though ~85% return to some work
- Source
- Alexandridis G, Injury 2016 (PMID 27156040)
- Figure
- Male Workers' Compensation heavy labourers with Bohler angle under 0 degrees and Sanders IV are at greatly increased risk of secondary fusion
- Source
- Csizy M / Buckley R, J Orthop Trauma 2003 (PMID 12571499)
Guideline & Practice Comparison Across Systems
- Stance on routine ORIF
- Routine ORIF not recommended for typical displaced fractures; selective surgery for specific patterns
- Evidence basis
- Griffin BMJ 2014 pragmatic RCT (PMID 25059747)
- Level
- Level 1
- Stance on routine ORIF
- Selective ORIF favoured - benefit concentrated in younger, non-compensation, anatomically reducible fractures
- Evidence basis
- Buckley JBJS Am 2002 RCT (PMID 12377902)
- Level
- Level 1
- Stance on routine ORIF
- Anatomic restoration of posterior facet, Bohler/Gissane angles, height and width when operating; increasing use of minimally invasive sinus tarsi exposure
- Evidence basis
- Bai OTSR 2018 meta-analysis (PMID 29410159)
- Level
- Level 2
- Stance on routine ORIF
- Active operative tradition (Zwipp/Rammelt); CT-based planning, with primary subtalar fusion considered for non-reconstructable Sanders IV
- Evidence basis
- Buckley/COTS RCT, J Orthop Trauma 2014 (PMID 24983433)
- Level
- Level 2
There is no dedicated international calcaneal-fracture implant registry comparable to arthroplasty registries (AOANJRR/NJR/AJRR), because fixation uses generic trauma plates and screws rather than tracked implants. Evidence therefore rests on RCTs and meta-analyses rather than registry data. Practice varies widely: the pragmatic UK trial pushed many UK units toward non-operative management, whereas North American and continental European centres maintain a more operative, anatomic-reduction philosophy with growing adoption of minimally invasive approaches. In the exam, defend your plan from the trial evidence and the individual patient (age, occupation, compensation status, soft tissues, fracture pattern) rather than from a single national guideline.
Perioperative Standards
-
VTE prophylaxis for immobilised lower-limb fracture: pharmacological prophylaxis (LMWH such as enoxaparin 40 mg daily, or a DOAC) is standard, continued until the patient is mobile, with extended duration for higher-risk patients
-
Antibiotic prophylaxis for ORIF: cefazolin 2 g IV at induction; for severe penicillin allergy, substitute a glycopeptide (e.g. vancomycin) per local protocol; re-dose for prolonged surgery or major blood loss
-
Smoking cessation is a modifiable wound-risk factor and should be actively supported before elective ORIF
(These are widely accepted perioperative standards; verify against the local formulary and protocol at the time of use.)
Critical documentation for calcaneal fracture management:
Consent discussion (must document):
- Wound complication risk 20-30% (higher with smoking, diabetes)
- Infection risk 5-10%
- Nerve injury (sural nerve) 5-10%
- Subtalar arthritis 30-50% by 5 years (disease progression, not surgical failure)
- Need for future subtalar fusion 15-25%
- Alternative treatments discussed (conservative, primary fusion)
- Realistic return to work expectations (40-60% return to heavy labor)
Operative documentation (critical details):
- Pre-operative soft tissue assessment (wrinkle test positive, no fracture blisters)
- Fluoroscopy-confirmed reduction (Bohler angle, step-off measurement)
- Hardware used (plate type, screw sizes and positions)
- Intra-operative complications and management
- Estimated blood loss, tourniquet time
- Post-operative instructions (NWB duration, elevation, wound check timing)
Common litigation issues:
- Wound complications not consented - patients surprised by dehiscence
- Compartment syndrome missed - delayed fasciotomy with permanent damage
- Operating too early - swelling present, wound breakdown blamed on timing
- Poor functional outcome - patient expected return to normal (unrealistic expectations)
Protection: Document detailed consent, realistic outcome discussion, appropriate timing (wrinkle test), and compartment syndrome surveillance in first 48 hours.
Mnemonics and Memory Aids
SANDERSSanders Classification
Hook:SANDERS classification uses the Single view that matters - the coronal CT through the widest posterior facet - to count the Number of articular fragments!
ANGLESBohler and Gissane Angles
Hook:ANGLES guide your assessment - Normal Bohler over 20 degrees predicts Good outcomes, Loss of height (under 20) needs Elevation with surgery!
SMOKEWound Complication Risk Factors
Hook:SMOKE signals danger - these factors turn a 20% wound complication rate into over 50%!
SAFEExtensile Lateral Approach Layers
Hook:Keep it SAFE - elevate the lateral wall as a single full-thickness flap to protect blood supply!
MCQ Practice Points
Q: On which imaging view is the Sanders classification of calcaneal fractures determined?
A: Coronal CT through the widest portion of the posterior facet of the calcaneus. The classification is based on the number of articular fragments created by fracture lines on this single critical coronal slice. Type I = non-displaced (any number of lines), Type II = 1 fracture line (2 fragments), Type III = 2 fracture lines (3 fragments), Type IV = comminuted (over 3 fragments). Subtypes (IIA, IIB, IIC, etc.) based on which fracture lines (A=lateral, B=central, C=medial) are present.
Q: What is the normal range for Bohler angle, and what value predicts poor outcome with conservative management?
A: Normal Bohler angle is 20-40 degrees (typically 30-35 degrees). Measured on lateral foot radiograph as the angle formed by: (1) line from posterior superior calcaneus to highest point of posterior facet, intersecting (2) line from highest point of posterior facet to anterior process. Bohler angle under 20 degrees (especially under 10 degrees) predicts poor functional outcome with conservative management, indicating significant loss of calcaneal height. ORIF goal is restoration to over 20 degrees minimum.
Q: What is the optimal timing for ORIF of calcaneal fractures and why?
A: Optimal timing is 10-21 days post-injury. Rationale: Allow soft tissue swelling to resolve to minimize wound complications (20-30% rate, increases to 40-50% if surgery under 7 days). The wrinkle test determines readiness - gently pinch lateral skin; if wrinkles form, swelling resolved and safe to operate. Early surgery (under 7 days) has double the wound complication rate. Delayed surgery (over 3 weeks) makes reduction more difficult due to early fracture healing and fibrous tissue formation. The window of 10-21 days balances wound healing risk against ease of reduction.
Q: What is the incidence of compartment syndrome with calcaneal fractures and how is it diagnosed?
A: 10% of calcaneal fractures develop acute compartment syndrome - highest rate of any foot injury. This is a clinical diagnosis based on: (1) Pain out of proportion to injury, (2) Pain with passive toe dorsiflexion (stretches deep flexor muscles in deep compartments), (3) Tense, swollen foot. Key point: pulses are usually present (compartment syndrome is increased pressure in fascial compartments, not arterial occlusion). Do not delay for pressure measurements if clinically suspected. Treatment: urgent fasciotomy of all 9 foot compartments (medial, lateral, superficial central, deep central, 4 interosseous, calcaneal). Delay over 6 hours causes irreversible muscle necrosis leading to clawing, contractures, chronic pain.
Q: What did the two major RCTs (Griffin/UK Heel Fracture Trial and Buckley/Canadian trial) show for ORIF vs non-operative treatment of displaced calcaneal fractures?
A: The UK Heel Fracture Trial (Griffin et al, BMJ 2014, PMID 25059747) was a pragmatic multicentre RCT of 151 patients. The primary outcome was the Kerr-Atkins score at 2 years (69.8 operative vs 65.7 non-operative, 95% CI of difference -7.1 to 7.0) - no significant difference, with higher complications/reoperations after surgery (OR 7.5), leading the authors to conclude ORIF is not recommended for typical displaced fractures. The earlier Canadian RCT (Buckley et al, JBJS Am 2002, PMID 12377902) of 424 patients found overall equivalence (SF-36 64.7 vs 68.7, p=0.13) but, after excluding Workers' Compensation patients, identified subgroups that benefited from surgery - younger patients, women, light-workload patients, moderately reduced Bohler angle (0-14 degrees), and anatomically reducible fractures (step-off 2 mm or less). Clinical implication: surgery should be selective, targeting younger, non-compensation patients with reducible fractures, rather than offered routinely. (Note: "ORCA" is an informal label sometimes applied to these trials; cite the named trials and authors in the exam.)
Q: In which patients should primary subtalar fusion be considered instead of ORIF for calcaneal fractures?
A: Primary subtalar fusion indications: (1) Sanders Type IV fractures in heavy laborers over 50 years, (2) Severe comminution precluding stable fixation, (3) Pre-existing subtalar arthritis. Rationale: Sanders IV fractures have poor outcomes with any treatment and a high rate of progression to subtalar arthritis requiring late fusion. Primary fusion (ORIF + primary subtalar arthrodesis) aims to achieve the definitive endpoint in one operation and pre-empt a secondary procedure. Evidence: the only RCT in this area (Buckley/Canadian Orthopaedic Trauma Society, J Orthop Trauma 2014, PMID 24983433) randomised 31 Sanders IV fractures and found no statistically significant difference between ORIF alone and ORIF + primary subtalar arthrodesis (SF-36 PCS 30.2 vs 37.8, p=0.10), but noted primary fusion may speed recovery and avoid late secondary fusion. Consider especially in heavy labourers in whom subtalar arthritis is near-inevitable.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old builder presents after falling 3 meters from scaffolding, landing on both feet. He has bilateral heel pain and swelling. X-rays show bilateral calcaneal fractures with loss of Bohler angles. You order CT scans. The right calcaneus shows a single fracture line through the posterior facet on the coronal view (Sanders IIB), and the left shows two fracture lines with three articular fragments (Sanders IIIAB). How do you manage this patient?”
“You are performing ORIF for a Sanders Type IIA calcaneal fracture in a 38-year-old patient. Walk me through your surgical approach and reduction technique. The examiner hands you a model calcaneus and asks you to describe the key steps.”
“You performed ORIF via extensile lateral approach for a Sanders IIB calcaneal fracture 2 weeks ago. The patient returns with 3cm wound dehiscence over the lateral incision, exposing the plate but no purulence. The patient is a smoker and diabetic (HbA1c 8.5%). How do you manage this complication?”
Key Anatomy
- Posterior facet = 80% weight bearing surface, articular with talus
- Sustentaculum tali = medial shelf, attached to talus (stable reference for reduction)
- Bohler angle = 20-40 degrees normal, under 20 degrees poor outcome
- Gissane angle (critical angle) = 120-145 degrees normal
- Sural nerve = 1-2cm posterior to fibula, at risk in extensile lateral approach
- Lateral calcaneal artery = from peroneal, supplies lateral wall and skin
Sanders Classification (CT Coronal View)
- Type I = Non-displaced (any lines), conservative, 85-90% good outcomes
- Type II = 1 fracture line, 2 fragments (IIA lateral, IIB central, IIC medial), ORIF, 75-85% good outcomes
- Type III = 2 fracture lines, 3 fragments (AB, AC, BC, ABC), ORIF, 60-70% good outcomes
- Type IV = Comminuted over 3 fragments, conservative or primary fusion, 40-50% good outcomes
- Coronal slice through WIDEST posterior facet used for classification
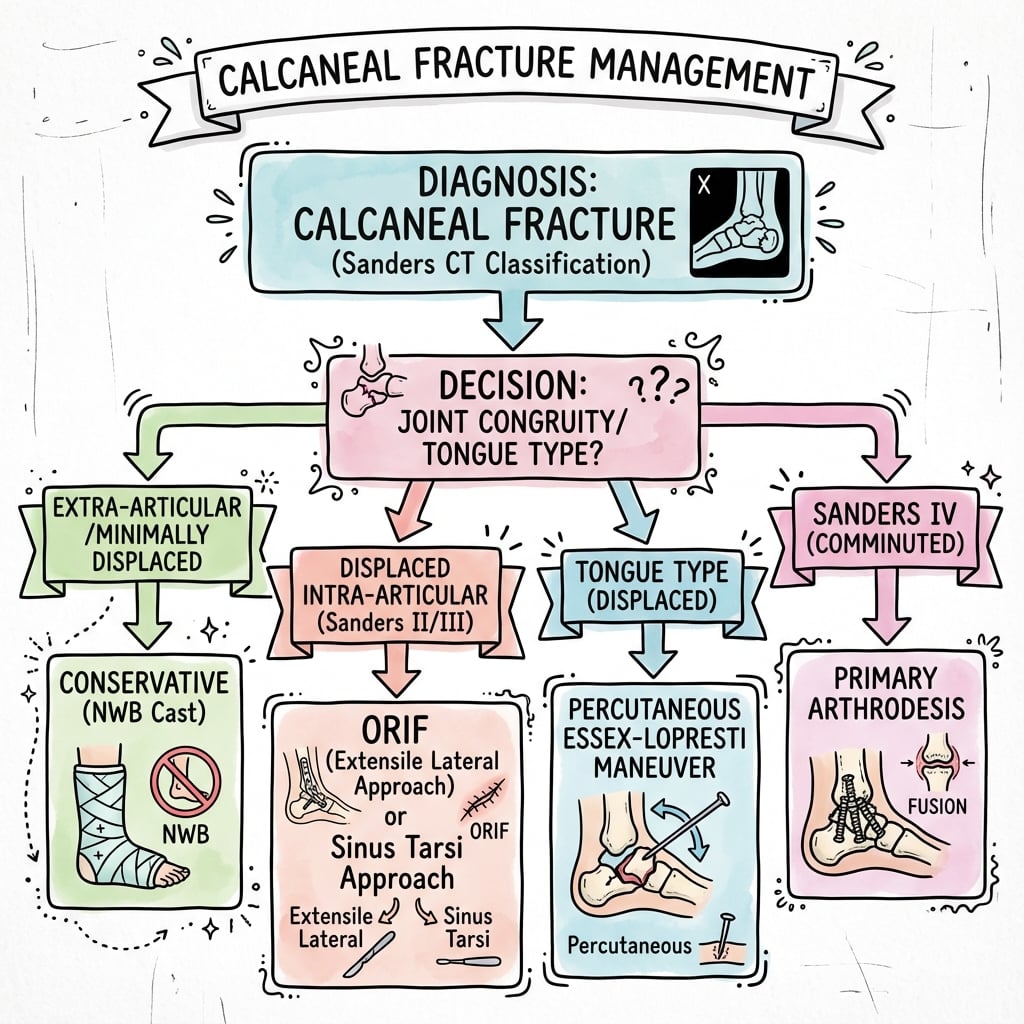
Treatment Algorithm
- Sanders I → Conservative (NWB 6 weeks, boot)
- Sanders II-III active under 60 years → ORIF extensile lateral at 10-21 days
- Sanders II simple pattern → Consider sinus tarsi approach (lower wound complications)
- Sanders IV heavy laborer over 50 years → Primary subtalar fusion
- Sanders IV elderly low-demand → Conservative
- ORIF timing = 10-21 days (wrinkle test positive), early surgery doubles wound complications
ORIF Surgical Pearls
- Extensile lateral approach: L-shaped incision, full-thickness flap (no undermining)
- Protect sural nerve (1cm below fibula tip with horizontal limb)
- Reduction sequence: (1) Height (distraction), (2) Posterior facet to sustentaculum, (3) Width
- Goal: Bohler angle over 20 degrees, step-off under 2mm
- Key fixation: Screws from lateral plate to sustentaculum medially (40-50mm locking)
- Closure: Meticulous, no tension, drain 24-48h, strict elevation post-op
Complications
- Wound dehiscence = 20-30% (ORIF), higher with smoking/diabetes/obesity/early surgery
- Compartment syndrome = 10%, clinical diagnosis, pain with passive toe dorsiflexion, urgent fasciotomy 9 compartments
- Sural nerve injury = 5-10%, lateral foot numbness
- Subtalar arthritis = 30-50% by 5 years (disease, not treatment failure), 15-25% need fusion
- Infection = 5-10% superficial, 2-5% deep
- Chronic pain = 30-40% despite anatomical reduction
Evidence Base and Key Trials
UK Heel Fracture Trial - Operative vs Non-Operative for Displaced Intra-Articular Calcaneal Fractures
- Pragmatic, assessor-blinded multicentre RCT (22 UK hospitals): 151 patients with closed displaced intra-articular fractures randomised to ORIF (n=73) or non-operative care (n=78)
- Primary outcome was the Kerr-Atkins pain/function score at 2 years (not SF-36): 69.8 (operative) vs 65.7 (non-operative), adjusted 95% CI of difference -7.1 to 7.0 - no significant difference
- No significant difference in any secondary outcome (AOFAS hindfoot, SF-36, EQ-5D, walking speed, gait symmetry)
- Complications and reoperations were markedly MORE common after surgery (odds ratio 7.5, 95% CI 2.0 to 41.8)
- Authors concluded ORIF is NOT recommended for typical displaced intra-articular calcaneal fractures