IWGDF/IDSA severity classification guides treatment | Probe-to-bone test diagnoses osteomyelitis | Multidisciplinary care reduces amputation rates
- Acute limb-threatening infection requires emergency surgical debridement within 24 hours
- Empiric antibiotics must cover MRSA in moderate-severe infections (vancomycin or linezolid)
- Duration: 1-2 weeks for soft tissue only, 4-6 weeks for osteomyelitis with debridement, 12 weeks if conservative
- Systemic signs may be absent despite severe infection due to neuropathy and vasculopathy
- Multidisciplinary diabetic foot team reduces amputation rates by 50% compared to standard care
- “Probe-to-bone positive in deep ulcer (>2cm²) has 89% PPV for osteomyelitis
- “Severe (PEDIS 4) infection with SIRS requires emergency debridement within 24 hours
- “MRI triad for osteomyelitis: low T1, high T2/STIR, cortical destruction
- “Deep tissue cultures (curettage) essential; superficial swabs misleading
Prognosis Overview
Diabetic foot infections carry significant morbidity and mortality, with outcomes depending on infection severity, vascular status, and timeliness of appropriate treatment.
Diabetic Foot Ulcer Recurrence and Long-Term Risk
Anatomy & Pathophysiology
Diabetic Foot Triad
- Loss of protective sensation
- Inability to detect ulcer formation
- Delayed recognition of infection
- Continued weight-bearing on infected area
- Intrinsic muscle atrophy
- Claw toe deformities
- Abnormal pressure points
- Altered biomechanics
- Anhidrosis causing dry cracked skin
- Loss of thermoregulation
- Impaired inflammatory response
- Atherosclerosis of tibial vessels
- Calcified vessels (Monckeberg's sclerosis)
- Reduced perfusion to foot
- Impaired wound healing
- Basement membrane thickening
- Endothelial dysfunction
- Reduced oxygen delivery
- Impaired neutrophil function
- Delayed healing
- Increased infection risk
- Higher amputation rates
- Impaired neutrophil chemotaxis
- Reduced phagocytic function
- Decreased bactericidal activity
- Delayed inflammatory response
- Glycosylation of immunoglobulins
- Impaired antibody function
- Reduced complement activity
- Hyperglycemia impairs immunity
- Advanced glycation end products
- Increased susceptibility to infection
Classification
IWGDF/IDSA Classification System
International Working Group on Diabetic Foot (IWGDF) Classification
This is the most widely used classification system for diabetic foot infections, endorsed by the Infectious Diseases Society of America (IDSA). It guides antibiotic selection and surgical decision-making.
IWGDF/IDSA Infection Severity Classification
The PEDIS (Perfusion, Extent, Depth, Infection, Sensation) grading system integrates infection severity with other wound characteristics to provide comprehensive assessment.
SIRSSIRS - Systemic Inflammatory Response Syndrome
Hook:SIRS criteria help identify severe infection requiring emergency intervention
Additional Classification Considerations
Differential Diagnosis
Differential Diagnosis of the Hot, Swollen Diabetic Foot
Clinical Presentation

History and Risk Factors
- Diabetes duration greater than 10 years
- HbA1c greater than 8% (poor glycemic control)
- Peripheral arterial disease (absent pedal pulses, ABI less than 0.7)
- Previous foot ulcer or amputation
- Severe neuropathy (inability to feel 10g monofilament)
- Renal insufficiency (eGFR less than 60)
- Immunosuppression (steroids, chemotherapy)
- Poor footwear or barefoot walking
- Rapid progression over 24-48 hours
- Crepitus suggesting gas in tissues (necrotizing infection)
- Foul-smelling discharge (anaerobic infection)
- Systemic signs: fever, tachycardia, hypotension
- Mental status changes in elderly
- Wet gangrene with tissue necrosis
- Bullae formation (necrotizing fasciitis)
Physical Examination
- Size: measure length, width, depth in centimeters
- Location: pressure points (metatarsal heads, heel) high risk
- Depth: superficial vs deep (probe-to-bone test)
- Base: granulation tissue (healthy) vs necrotic tissue
- Drainage: serous (uninfected) vs purulent (infected)
- Odor: foul smell suggests anaerobic infection
- Use sterile metal probe or cotton swab
- Gently insert into ulcer and probe to base
- Positive: hard, gritty bone felt at base
- Sensitivity 87%, Specificity 83%, PPV 89% for osteomyelitis
- Most accurate in ulcers greater than 2cm² and depth greater than 3mm
- Measure erythema extent from wound edge
- Palpate for induration, fluctuance (abscess)
- Check for lymphangitic streaking
- Assess for crepitus (gas in soft tissues)
- Document any exposed bone, tendon, or joint
The probe-to-bone test should be performed in all diabetic foot ulcers greater than 2cm² or depth greater than 3mm. A positive test in the appropriate clinical context is highly predictive of osteomyelitis and may be sufficient to initiate treatment without confirmatory imaging.
Systematic Approach to Diagnosis
- Classify infection severity using IWGDF/IDSA criteria
- Perform probe-to-bone test if ulcer greater than 2cm² or depth greater than 3mm
- Assess perfusion with pulse examination and ABI
- Check for systemic signs (SIRS criteria)
- CBC, CRP, ESR, metabolic panel, HbA1c
- Blood cultures if systemic signs present
- Deep tissue culture (curettage or intraoperative biopsy)
- Plain radiographs (AP, lateral, oblique) for all patients
- If probe-to-bone positive or radiographs show changes: obtain MRI
- If MRI contraindicated: consider CT or nuclear medicine study
- If moderate-severe infection with ischemia: vascular imaging (CTA, MRA, or angiography)
- Mild infection + probe-to-bone negative + normal radiographs: treat as soft tissue only
- Moderate infection + probe-to-bone positive: obtain MRI to confirm osteomyelitis
- Severe infection: emergency surgery, imaging should not delay debridement
- Any infection + ischemia (ABI less than 0.7): urgent vascular consultation
Investigations

Laboratory Studies
- White blood cell count (WBC greater than 12 or less than 4 suggests SIRS)
- C-reactive protein (CRP) - elevated in infection, useful for monitoring response
- Erythrocyte sedimentation rate (ESR) - elevated greater than 70 suggestive of osteomyelitis
- Procalcitonin - if available, suggests bacterial infection if elevated
- Glucose and HbA1c (assess control)
- Creatinine and eGFR (renal function for antibiotic dosing)
- Electrolytes (K if DKA concern)
- Lactate (elevated in sepsis)
- Debride superficial tissue and wound edges
- Curettage or biopsy of ulcer base after cleaning
- Intraoperative bone biopsy if osteomyelitis suspected
- Send for aerobic, anaerobic, fungal, and mycobacterial culture
- Superficial wound swabs (inaccurate, grow colonizers)
- Cultures before wound cleaning
- Incomplete anaerobic specimen handling
Culture results guide definitive antibiotic therapy but should not delay empiric antibiotics in moderate-severe infection.
CULTURECULTURE - Deep Tissue Sampling Principles
Hook:Remember to CULTURE properly for accurate microbiological diagnosis — Exam Tip: In diabetic foot, differentiate osteomyelitis from Charcot arthropathy: osteomyelitis shows focal involvement at ulcer site with soft tissue changes, while Charcot shows more diffuse bone marrow edema, fragmentation, and joint destruction without overlying ulcer.
Imaging
Imaging Modalities for Diabetic Foot Infection
Probe-to-Bone Test - Original Description (Grayson)
Probe-to-Bone Test - Outpatient Validation (Lavery)
Diagnostic Algorithm
Management
Antibiotic Therapy
Mild Infection (Outpatient Oral):
First-Line Options:
- Cephalexin 500mg QID, OR
- Amoxicillin-clavulanate 875/125mg BID, OR
- Clindamycin 300mg TID (if penicillin allergic)
Duration: 1-2 weeks for soft tissue infection only
Coverage: S. aureus and Streptococcus spp (primary pathogens in acute mild infection)
- Vancomycin 15-20mg/kg IV q8-12h (target trough 15-20 for serious infection), PLUS
- Piperacillin-tazobactam 4.5g IV q6h or 3.375g q4h
- Vancomycin PLUS ciprofloxacin 400mg IV q12h PLUS metronidazole 500mg IV q8h
Duration: 2-3 weeks for soft tissue, 4-6 weeks if osteomyelitis with surgical debridement
Coverage: MRSA, Gram-negatives including Pseudomonas, anaerobes
Severe Infection (ICU, Broad-Spectrum):
Recommended Regimen:
- Vancomycin 15-20mg/kg IV q8-12h (or linezolid 600mg IV q12h), PLUS
- Meropenem 1g IV q8h or imipenem-cilastatin 500mg IV q6h, PLUS
- Consider adding metronidazole 500mg IV q8h if extensive necrosis
Duration: Minimum 4-6 weeks, often longer depending on clinical response
Empiric therapy must be started immediately after obtaining cultures in moderate-severe infection. Do NOT wait for culture results to initiate antibiotics.
Antibiotic Duration in Nonsurgically Treated Diabetic Foot Osteomyelitis
Surgical Management
- Remove all necrotic and infected tissue
- Obtain deep tissue and bone cultures
- Reduce bacterial burden
- Convert chronic wound to acute healing wound
- Assess extent of infection
- Patient supine, thigh tourniquet available (use controversial, may limit bleeding assessment)
- Ensure adequate IV access for resuscitation
- Broad-spectrum antibiotics already on board
- Prepare for possible amputation if extensive involvement
- Excise all necrotic skin and subcutaneous tissue
- Remove callus around ulcer edges (keratinocytes impair healing)
- Open all deep spaces and compartments
- Probe for tracking sinuses and abscess pockets
- Resect obviously infected bone (visual inspection: dark, mushy, non-bleeding)
- Send multiple deep tissue specimens for culture (3-5 samples)
- Copious irrigation with normal saline (3-6 liters)
- Debride to bleeding viable tissue (the 4 C's: Color pink/red, Consistency firm, Contraction with stimulus, Circulation bleeding)
- Be aggressive but preserve functional structures if possible
- Leave wound open for delayed closure or healing by secondary intention
- Plan for serial debridements every 48-72 hours if needed
The concept of damage control debridement applies in severe infections: remove obviously infected tissue at first operation, reassess at 48-72 hours, and perform definitive reconstruction only after infection controlled.
Adjunctive Therapies
- Total contact cast (TCC) - gold standard for plantar ulcers
- Removable cast walker (CAM boot) if patient reliable
- Felted foam off-loading for specific pressure points
- Heel off-loading boot for posterior ulcers
- Crutches or wheelchair for non-weight bearing
- TCC reduces plantar pressure by 85-90%
- Healing rates with TCC: 80-90% at 12 weeks
- Patient compliance critical for removable devices
- Off-loading must continue until complete healing
- Inpatient goal: 140-180 mg/dL (less stringent during acute illness)
- Outpatient goal: HbA1c less than 7% (individualize)
- Avoid hypoglycemia (impairs wound healing)
- Most patients require insulin during acute infection
- Basal-bolus regimen or insulin infusion if ICU
- Transition back to oral agents when stable
- HbA1c greater than 8% associated with delayed healing
- Each 1% increase in HbA1c increases infection risk by 20%
- Hyperglycemia impairs neutrophil function and collagen synthesis
- Chronic non-healing ulcer despite optimal treatment
- Compromised host (advanced age, comorbidities)
- Ischemic wounds with PAD (after revascularization)
- 100% oxygen at 2.0-2.5 atmospheres
- Sessions 90-120 minutes
- Typically 30-40 treatments over 6-8 weeks
- Modest reduction in amputation rates (NNT 10-15)
- Most benefit in ischemic wounds
- Limited high-quality evidence
- Not covered by all insurance plans
- Recombinant PDGF-BB
- Apply daily to clean ulcer bed
- May improve healing rates by 10-15%
- Black box warning: cancer risk with prolonged use
- Dermagraft, Apligraf, EpiFix
- Bioengineered skin products
- May accelerate healing in chronic ulcers
- Expensive, limited evidence for superiority
- Autologous platelet concentrate
- Multiple growth factors
- Conflicting evidence for efficacy
- Not standard of care
Angiosome-Directed Revascularization
The evidence section refers to angiosome-directed revascularization, but the angiosome concept itself is worth setting out because it determines which vessel to target when restoring perfusion to a diabetic foot wound. The foot is supplied by three source arteries dividing into six angiosomes - three-dimensional vascular territories each fed by a single source artery, with adjacent territories linked by choke (collateral) vessels.
The Six Angiosomes of the Foot
Revascularization in the Ischaemic Infected Foot: Timing and Modality
A recurring theme of this topic is that infection will not resolve and wounds will not heal without adequate perfusion. Where chronic limb-threatening ischaemia coexists with infection, revascularization is therefore part of management, and two questions arise: how it is sequenced with infection control, and whether to revascularize by open bypass or endovascular means.
Revascularization Strategy in the Ischaemic Infected Diabetic Foot
Management Algorithm
IDSA Clinical Practice Guideline for Diabetic Foot Infections
Complications
Treatment-Related Complications
- C. difficile colitis (10-15% with broad-spectrum antibiotics)
- Antibiotic-associated diarrhea
- Vancomycin: nephrotoxicity, red man syndrome
- Linezolid: bone marrow suppression, peripheral neuropathy (with prolonged use greater than 6 weeks)
- Fluoroquinolones: tendon rupture, QT prolongation, peripheral neuropathy
- Allergic reactions and drug rashes
- Persistent infection after debridement (10-15%)
- Need for higher-level amputation (15-20%)
- Wound dehiscence (20-30% in ischemic limbs)
- Phantom limb pain after major amputation
- Falls and fractures from altered biomechanics after partial foot amputation
- Pressure ulcers at new weight-bearing sites
- Recurrent ulceration (30-40% at 1 year, 60% at 3 years)
- Charcot arthropathy in denervated foot
- Contralateral limb ulceration (50% within 3 years)
- Progression of PAD requiring revascularization
- Worsening renal function from diabetes and sepsis
- Reduced quality of life and mobility
Multidisciplinary Care and Amputation in Diabetic Foot Ulcers
Postoperative Care
Postoperative Management Principles
- Daily wound inspection for first 48-72 hours
- Wet-to-dry dressings or negative pressure therapy
- Keep wound bed moist but not macerated
- Serial debridements every 48-72 hours if needed
- Transition to appropriate wound dressing based on exudate
- Weekly wound measurements to track progress
- Monitor for signs of recurrent infection
- Total contact cast (gold standard for plantar ulcers)
- Removable cast walker (CAM boot)
- Non-weight bearing if mid/hindfoot involvement
- Continue until complete wound closure
- Typically 6-12 weeks minimum
- May require permanent footwear modification
Antibiotic Completion
- Complete planned antibiotic course based on infection type
- Soft tissue: 1-2 weeks
- Osteomyelitis with resection: 4-6 weeks
- Monitor CRP weekly (should decrease by 50% in 2 weeks if responding)
Prognosis
Outcomes and Predictive Factors
Overall Outcomes:
- Soft tissue infection with adequate treatment: 85-90% resolution without amputation
- Osteomyelitis with surgical resection: 70-80% healing without major amputation
- Severe infection with sepsis: 60-70% limb salvage, 15-20% mortality
- Forefoot amputation (TMA or ray): 70-80% healing, 50% ambulatory at 1 year
- Major amputation: BKA 60-70% healing primary, AKA 85-90% healing primary
Predictive Factors for Poor Outcome:
- Advanced age (greater than 75 years)
- End-stage renal disease on dialysis
- Severe PAD (ABI less than 0.5, TcPO2 less than 30)
- Poor glycemic control (HbA1c greater than 9%)
- Severe immunosuppression
- Malnutrition (albumin less than 3.0 g/dL)
- Active smoking
- Wound size greater than 4cm²
- Wound depth to bone or joint
- Wound duration greater than 6 months
- Heel or midfoot location (worse than forefoot)
- Presence of wet gangrene
- Polymicrobial with resistant organisms (MRSA, Pseudomonas)
- Failed previous amputation or debridement
- PEDIS Grade 4 (severe) infection
- Necrotizing soft tissue infection
- Systemic sepsis requiring ICU
- Osteomyelitis with extensive bone involvement
- Presence of SIRS or septic shock
- Delayed presentation (greater than 1 week symptoms)
- Gas in soft tissues on imaging
Five-Year Outcomes After Diabetic Foot Infection:
- Recurrent ulceration: 60-65%
- Minor amputation (toe, ray, TMA): 30-35%
- Major amputation (BKA, AKA): 15-20%
- Contralateral limb ulceration or amputation: 40-50%
- Cardiovascular event (MI, stroke): 25-30%
- Mortality: 40-50% (primarily from cardiovascular disease and sepsis)
These sobering statistics underscore the importance of prevention, early intervention, multidisciplinary care, and long-term surveillance.
Predictors of Amputation in Infected Diabetic Foot Ulcers (Eurodiale cohort)
Guidelines, Registries & Global Practice
Global Epidemiology
According to PubMed-indexed evidence, the global pooled prevalence of diabetic foot ulceration is 6.3% (Zhang 2017, Ann Med; PMID 27585063), and approximately 18.6 million people worldwide develop a diabetic foot ulcer each year (Armstrong 2023, JAMA; PMID 37395769). Around 50-60% of ulcers become infected, and roughly 20% of moderate-to-severe infections lead to lower-extremity amputation.
Diabetic Foot Ulcer Prevalence by Region (Zhang 2017 meta-analysis)
Ulcers are more prevalent in men than women and in type 2 than type 1 diabetes; affected patients tend to be older with longer diabetes duration, hypertension, retinopathy and a smoking history. Indigenous and socially disadvantaged populations (including Indigenous Australians, and Black, Hispanic and Native American populations in the USA) carry substantially higher rates of ulceration and amputation.
Major Guidelines Side by Side
Guideline Comparison - Diabetic Foot Infection
There is broad international agreement on the core principles: grade severity, reserve antibiotics for infected wounds, culture deep tissue rather than superficial swabs, image with plain films first then MRI, and refer urgently to a multidisciplinary foot service. Genuine variation lies mainly in empiric antibiotic choice (driven by local resistance patterns and drug availability) and in resource-dependent access to MRI, revascularisation and specialist teams.
Practice Variation and Registry Context
- High-resource centres: rapid-access foot clinics, MRI, vascular intervention, prompt deep-tissue culture
- Limited-resource settings: later presentation, less imaging and revascularisation, higher amputation rates
- Telehealth and structured screening programmes help bridge access gaps in remote regions
- Multidisciplinary care associated with lower major amputation (3.2% vs 4.4%; OR 0.40, 95% CI 0.32-0.51; Armstrong 2023, PMID 37395769)
- Core team: podiatry, infectious diseases, vascular surgery, endocrinology, orthopaedics, wound-care nursing
- National diabetic foot programmes and audits track amputation rates as a quality metric across health systems
Exam Viva Point - Global Framing: Frame management around the world standard of care rather than one country's system: (1) grade severity with the IWGDF/IDSA classification, (2) culture deep tissue not superficial swabs, (3) plain radiographs then MRI for suspected osteomyelitis, (4) severity-stratified empiric antibiotics adjusted for local resistance and drug availability, and (5) urgent referral to a multidisciplinary foot service, which reduces major amputation. Be ready to discuss regional differences in epidemiology, antibiotic choice and access to imaging and revascularisation.
MCQ Practice Points
Q: What clinical finding differentiates osteomyelitis from soft tissue infection in a diabetic foot ulcer?
A: Probe-to-bone test (positive predictive value 89%). Using a sterile blunt probe, ability to touch bone through the ulcer indicates osteomyelitis. Other indicators: ulcer size greater than 2cm², duration greater than 2 weeks, ESR greater than 70mm/hr. MRI has highest sensitivity/specificity (90%/80%) for diagnosis. X-ray changes lag 2-3 weeks behind infection.
Q: What organisms should empiric antibiotic therapy cover in a limb-threatening diabetic foot infection?
A: Broad-spectrum coverage: Gram-positives (including MRSA), Gram-negatives (including Pseudomonas), AND anaerobes. Typical regimen: piperacillin-tazobactam + vancomycin OR meropenem + vancomycin. Tailor therapy based on deep wound cultures (NOT superficial swabs). Duration: 2-4 weeks for soft tissue, 4-6 weeks for osteomyelitis (or until amputation margin healed).
Q: What is the IDSA/IWGDF classification system for diabetic foot infections and its implications?
A: Grade 1: Uninfected. Grade 2: Mild (superficial, less than 2cm cellulitis). Grade 3: Moderate (cellulitis greater than 2cm, lymphangitis, deep abscess). Grade 4: Severe (systemic toxicity, SIRS, metabolic instability). Grades 3-4 require hospitalization, IV antibiotics, and urgent surgical evaluation. Grade 4 infections have 50% amputation rate.
Q: What is the role of vascular assessment in diabetic foot infections?
A: Essential for all diabetic foot infections. Measure: Ankle-brachial index (ABI) - but may be falsely elevated due to arterial calcification. Toe-brachial index (TBI) greater than 0.7 or toe pressure greater than 30mmHg suggests adequate perfusion for healing. Absent pedal pulses require vascular surgery referral. Revascularization before major amputation may allow limb salvage.
Q: What is the recommended surgical approach for diabetic foot osteomyelitis of the first metatarsal head?
A: Options: (1) Conservative debridement with 4-6 weeks antibiotics, (2) Partial first ray amputation (metatarsal head resection), (3) Full first ray amputation. Decision based on: extent of infection, bone viability, soft tissue coverage, vascular status, patient function. First ray amputation causes significant gait disturbance. Spare as much length as possible while achieving clear margins.
At a Glance
Diabetic foot infections are polymicrobial soft tissue and/or bone infections complicating neuropathic ulcers, with Staphylococcus aureus the most common pathogen and MRSA coverage required for moderate-severe cases. The diabetic foot triad of neuropathy, peripheral arterial disease, and immunologic dysfunction impairs recognition, healing, and infection control. Classification uses IWGDF/IDSA severity criteria (uninfected/mild/moderate/severe) guiding antibiotic selection and surgical urgency. Probe-to-bone test has 89% positive predictive value for osteomyelitis; MRI is gold standard (90% sensitivity). Acute limb-threatening infections (wet gangrene, necrotizing fasciitis, deep abscess) require emergency debridement within 24 hours. Multidisciplinary diabetic foot teams reduce amputation rates by 50%.
TRIADTRIAD - Diabetic Foot Pathophysiology
Hook:The TRIAD of problems that predispose diabetic patients to foot infections — Exam Tip: Absence of pain does not exclude severe infection in diabetic neuropathy. Systemic signs may be blunted. Always assess infection severity by local findings and SIRS criteria, not patient symptoms alone.
Microbiology
Microbiology by Infection Duration
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old man with poorly controlled type 2 diabetes presents to emergency with 2-day history of rapidly progressive right foot swelling, erythema extending to ankle, and purulent drainage from plantar ulcer. He is febrile to 38.7°C, HR 110, BP 95/60. Examination shows extensive cellulitis, crepitus in forefoot, and probe-to-bone positive at ulcer. WBC 18,000, lactate 3.2. How would you manage this patient?”
“You are seeing a 58-year-old woman in clinic with 4-month history of painless plantar ulcer under 2nd metatarsal head. She has type 2 diabetes for 15 years, HbA1c 8.5%. Examination shows 3cm diameter ulcer, probe-to-bone positive, mild surrounding erythema 1cm from wound edge, no systemic signs. How would you classify and manage this infection?”
Pathophysiology Triad
- Neuropathy (sensory, motor, autonomic)
- PAD (macro and microvascular)
- Immunologic dysfunction (impaired neutrophils, hyperglycemia)
- Together create perfect storm for infection
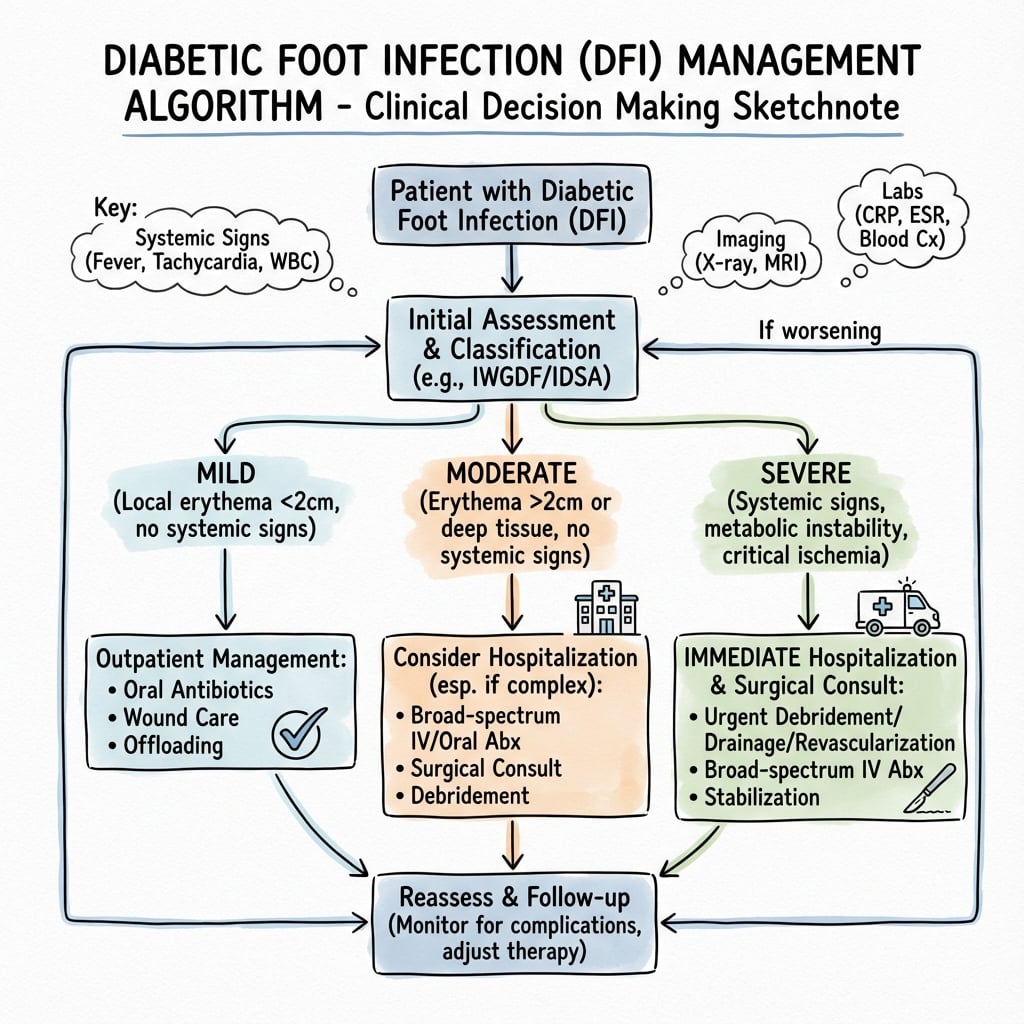
IWGDF/IDSA Classification
- Uninfected (no signs)
- Mild (PEDIS 2): cellulitis less than 2cm, outpatient oral antibiotics
- Moderate (PEDIS 3): erythema greater than 2cm or deep tissue, IV antibiotics, admission
- Severe (PEDIS 4): SIRS, systemic toxicity, emergency surgery
Microbiology
- Acute/Mild: S. aureus, Streptococcus (monomicrobial 70%)
- Chronic/Moderate-Severe: polymicrobial with MRSA 20-30%, gram-negatives, anaerobes
- Always get deep tissue culture not superficial swab
Probe-to-Bone Test
- Sensitivity 87%, Specificity 83%, PPV 89% for osteomyelitis
- Use in ulcers greater than 2cm² or depth greater than 3mm
- Positive test = hard gritty bone felt at ulcer base with sterile metal probe
Imaging
- Plain radiographs first (3 views)
- MRI gold standard for osteomyelitis (sens 90%, spec 79%)
- Classic MRI triad: low T1, high T2/STIR, cortical destruction
- Obtain ABI for all patients
Antibiotics
- Mild: oral cephalexin or amoxicillin-clavulanate 1-2 weeks
- Moderate: IV vancomycin PLUS piperacillin-tazobactam 2-3 weeks
- Severe: vancomycin PLUS carbapenem
- Osteomyelitis: 4-6 weeks if resected, 12 weeks if conservative
Surgery
- Severe infection (PEDIS 4): emergency debridement less than 24 hours
- Necrotizing infection: immediate surgery
- Abscess: I&D required
- Osteomyelitis: resection (ray amputation, TMA, partial calcanectomy) shortens antibiotic duration and improves cure
Outcomes
- Soft tissue only: 85-90% heal
- Osteomyelitis with surgery: 70-80% heal
- Severe with sepsis: 60-70% salvage, 15-20% mortality
- 5-year: 60% recurrent ulcer, 30% minor amputation, 15% major amputation, 50% mortality
- MDT reduces amputation 50%
Evidence Base
Key Evidence Summary
- Level I evidence supports surgical resection for forefoot osteomyelitis with 80-90% remission rates vs 60-70% with antibiotics alone
- Antibiotics-only acceptable in patients with high surgical risk or minimal bone involvement
- IWGDF 2019 guidelines recommend 6 weeks antibiotics if surgery leaves residual infection, 3-5 days if complete bone resection achieved
- Grayson 1995 landmark study: PPV 89% in high-prevalence population
- Lavery 2007 validation: Sensitivity 87%, Specificity 83%
- Test most useful in ulcers greater than 2cm² with visible bone or depth greater than 3mm
- Cochrane review 2020: MDT care reduces amputation rates by 40-50%
- Teams should include: vascular surgery, infectious diseases, podiatry, endocrinology, wound care, orthotist
- Weekly case conferences improve outcomes