Neuropathy + Vasculopathy + Immunopathy | Wagner and Texas Classifications | Offloading is Key
- Pathophysiology triad: sensory neuropathy (loss of protective sensation), peripheral vascular disease, and impaired immunity lead to ulcer formation
- Wagner classification: depth-based (0-5); Texas classification: adds ischemia and infection to depth grading (4x4 grid)
- Offloading is THE critical treatment - total contact casting reduces plantar pressure by 80-90% and is gold standard
- Probe-to-bone test: in infected high-risk wounds sensitivity 66%, specificity 85%, PPV 89% (Grayson) - a positive probe in a moderate/severe ulcer means treat for osteomyelitis until proven otherwise
- IDSA guidelines: treat infection (purulence OR 2+ inflammatory signs), NOT colonization - tissue cultures after debridement only
- “Monofilament testing: 10g (5.07 Semmes-Weinstein) = loss of protective sensation threshold
- “ABI less than 0.9 indicates PAD; less than 0.5 critical ischemia; greater than 1.3 falsely elevated (calcified vessels)
- “TCC (total contact cast) is gold standard offloading but instant total contact walker is alternative
- “5-year mortality after major amputation exceeds 70% (JAMA 2023) - worse than most cancers
Three pathological processes drive ulcer formation: (1) Sensory neuropathy leads to loss of protective sensation and unrecognized trauma, (2) Motor neuropathy causes intrinsic muscle atrophy, clawing, and abnormal pressure points, (3) Peripheral arterial disease impairs healing. Add immunopathy (WBC dysfunction) and you have the perfect storm.
Wagner (0-5) is most commonly used and grades by depth only. University of Texas adds ischemia and infection to create a 4x4 grid (depth A-D, grade 0-3). PEDIS system (Perfusion, Extent, Depth, Infection, Sensation) is IWGDF standard. Know all three and when each is used.
No offloading = no healing. Total contact casting (TCC) is gold standard - reduces plantar pressure by 80-90%, healing rate 85-95% at 12 weeks. Alternative: instant total contact walker (iTCC). Removable devices fail due to non-compliance. Offloading is treatment, NOT adjunct.
IDSA criteria for infection: purulence OR 2 or more inflammatory signs (warmth, erythema greater than 2cm, lymphangitis, edema, pain/tenderness). Swab cultures are meaningless - colonization only. Deep tissue cultures AFTER debridement. MRI for osteomyelitis if probe-to-bone negative but high suspicion.
OFFLOADOFFLOAD - Principles of Pressure Relief
Hook:OFFLOAD summarizes the critical principles of mechanical pressure reduction in diabetic foot ulcer treatment
Overview and Epidemiology
Diabetic foot ulcers (DFUs) are chronic wounds occurring in individuals with diabetes mellitus, resulting from the interaction of neuropathy, peripheral arterial disease, and repetitive trauma. They represent the most common and costly complication of diabetes, with devastating consequences for patients and healthcare systems.
Epidemiology and Burden
Global Impact (Zhang, Ann Med 2016, PMID 27585063; Armstrong, JAMA 2023, PMID 37395769):
- Pooled global prevalence among people with diabetes: 6.3% (95% CI 5.4-7.3%), with wide regional variation (North America ~13%, Oceania ~3%)
- Approximately 18.6 million people develop a diabetic foot ulcer worldwide each year
- Approximately 80% of diabetes-related lower-limb amputations are preceded by a foot ulcer
- Lifetime risk of foot ulceration in diabetes is commonly cited at roughly 15-25%
Outcomes and Prognosis (Armstrong, JAMA 2023, PMID 37395769; NEJM 2017, PMID 28614678):
- Only ~30-40% of ulcers heal at 12 weeks under usual care
- Recurrence: ~42% at 1 year, ~60% at 3 years, ~65% at 5 years despite initial healing
- About 20% of moderate-to-severe infections lead to lower-extremity amputation
- ~30% 5-year mortality after a diabetic foot ulcer; greater than 70% after a major amputation (worse than most cancers)
Risk Factors
- Previous foot ulceration: strongest predictor (relative risk 12-36)
- Peripheral neuropathy: loss of protective sensation (10g monofilament)
- Peripheral arterial disease: ABI less than 0.9
- Foot deformity: claw toes, Charcot foot, hallux valgus
- High plantar pressure: greater than 600 kPa at forefoot
- Poor glycemic control: HbA1c greater than 8%
- Duration of diabetes: greater than 10 years
- Vision impairment: inability to self-inspect
- Chronic kidney disease (dialysis patients 2-3x higher risk)
- Smoking (impairs wound healing)
- Limited joint mobility (especially ankle)
- Inappropriate footwear
- Male gender (1.6x higher risk)
- Low socioeconomic status
IWGDF Risk Stratification System (0-3):
- Category 0: No neuropathy - annual screening
- Category 1: Neuropathy alone - screen every 6-12 months
- Category 2: Neuropathy + PAD or deformity - screen every 3-6 months
- Category 3: Previous ulcer or amputation - screen every 1-3 months
This guides surveillance frequency and prevention intensity.
Pathophysiology
The Pathophysiological Triad
Diabetic foot ulcers result from the interaction of three primary pathological processes: neuropathy, vascular disease, and trauma. When combined with immunopathy, these create the conditions for chronic non-healing wounds.
1. Neuropathy (85% of DFUs)
- Loss of protective sensation to 10g monofilament (5.07 Semmes-Weinstein)
- Unable to perceive minor trauma (foreign body, friction, thermal injury)
- Reduced pain perception delays recognition of injury
- Distal, symmetric, "stocking-glove" distribution
- Mechanism: sorbitol accumulation, advanced glycation end-products (AGEs), oxidative stress
- Intrinsic muscle atrophy (lumbricals, interossei)
- Claw toe deformity develops from imbalance
- Met heads become more prominent
- Abnormal pressure distribution: peak pressures at met 2-3 heads
- Loss of dynamic shock absorption
- Decreased sweating (anhidrosis) leads to dry, cracked skin
- Arteriovenous shunting in foot (bounding pulses despite poor perfusion)
- Warm, dry foot with dilated veins
- Impaired thermoregulation
2. Peripheral Arterial Disease (PAD)
- Tibial and peroneal artery disease (below-knee)
- Spares foot vessels (pedal arch often patent)
- Medial arterial calcification (Mönckeberg sclerosis) - falsely elevated ABI
- Microvascular disease: capillary basement membrane thickening
- Reduced tissue perfusion delays healing
- Critical ischemia: ABI less than 0.5, TcPO2 less than 30 mmHg
- Tissue hypoxia impairs fibroblast function, collagen synthesis
- Impaired angiogenesis in diabetic patients
3. Immunopathy
- Neutrophil impairment: reduced chemotaxis, phagocytosis, bacterial killing
- Macrophage dysfunction: delayed wound debridement
- Lymphocyte abnormalities: impaired cellular immunity
- Mechanism: hyperglycemia interferes with WBC function at multiple steps
- Increased infection susceptibility
- Rapid progression of soft tissue infections
- Blunted inflammatory response - may have minimal systemic signs despite severe infection
- Osteomyelitis risk: 10-15% of infected DFUs
4. Repetitive Trauma (Mechanical)
- High plantar pressure: normal walking = 300-500 kPa; DFU patients often greater than 600 kPa
- Shear stress: friction during gait cycle
- Repetitive microtrauma: 5,000-10,000 steps per day on insensate foot
- Callus formation: further elevates peak pressure by 30-50%
- High pressure point (e.g., prominent met head)
- Repetitive loading without pain feedback
- Subcutaneous hemorrhage and tissue breakdown
- Callus forms over area
- Pressure increases further under callus
- Autolysis creates fluid-filled space
- Skin ruptures → ulcer formation
Patients often present late because neuropathic ulcers are painless. The same neuropathy that allows ulcer formation also prevents pain sensation. In contrast, ischemic ulcers ARE painful (rest pain). This clinical distinction helps differentiate neuropathic from neuroischemic ulcers at bedside.
Impaired Wound Healing in Diabetes
Cellular and Molecular Abnormalities:
- Prolonged inflammatory phase: persistent neutrophil infiltration
- Impaired proliferation: reduced fibroblast migration and proliferation
- Reduced growth factors: decreased PDGF, VEGF, EGF
- Extracellular matrix abnormalities: excess MMPs (matrix metalloproteinases)
- Senescent cells: cells in wound bed stop dividing
- Biofilm formation: 60-80% of chronic wounds have bacterial biofilms
ULCERULCER - Diabetic Foot Ulcer Pathophysiology
Hook:ULCER reminds you of the five pathological processes that create diabetic foot ulcers
Classification Systems
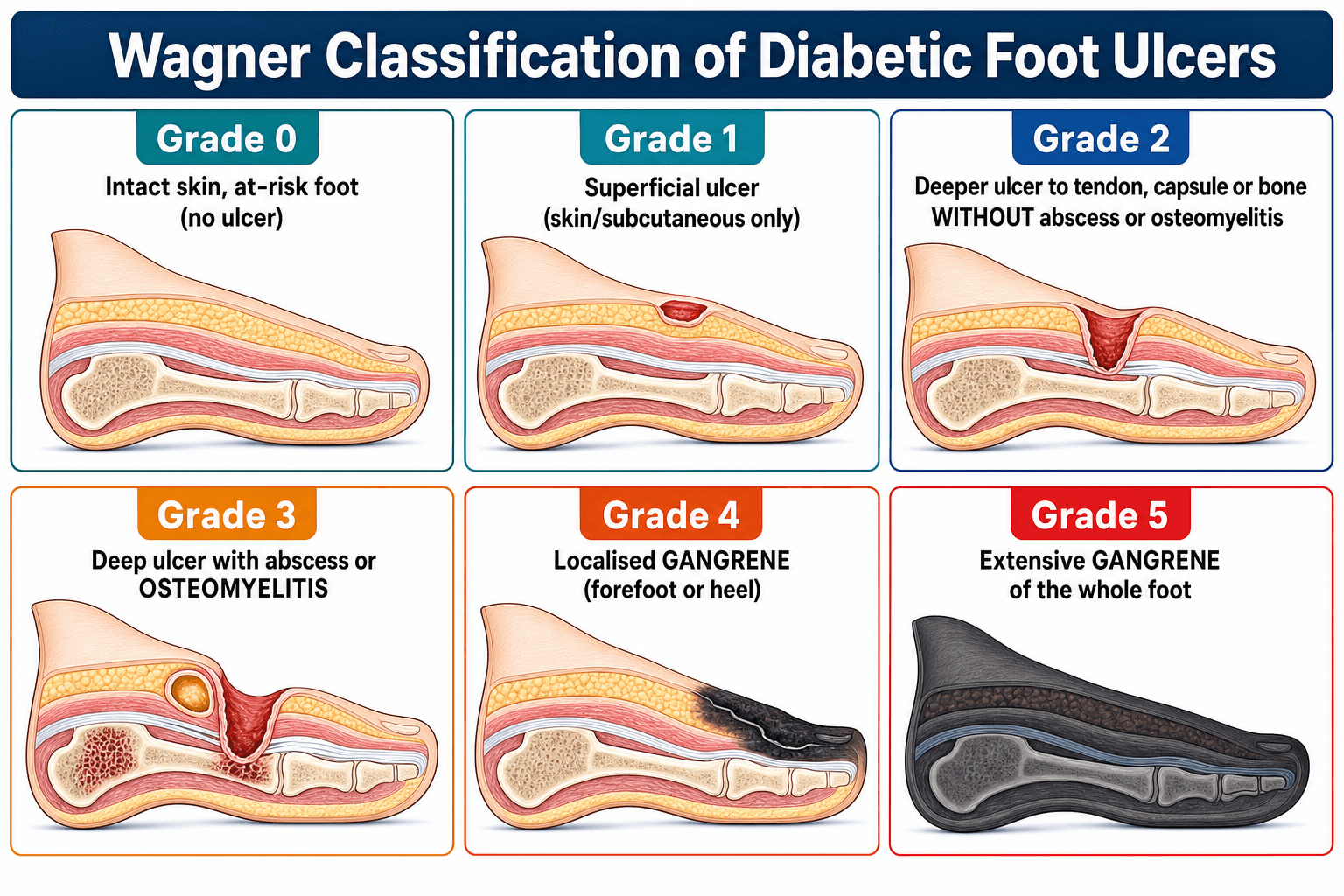
Wagner Classification (Most Widely Used)
The Wagner-Meggitt classification is the most commonly used system, grading ulcers by depth and presence of infection or gangrene (0-5).
- Description
- Intact skin, pre-ulcerative (callus, bony deformity, erythema)
- Treatment
- Prevention: orthotics, education, callus debridement
- Healing Rate
- Not applicable
- Description
- Superficial ulcer, partial/full-thickness, no deeper structures
- Treatment
- Offloading (TCC), sharp debridement, moist wound care
- Healing Rate
- 85-95% at 12 weeks with proper offloading
- Description
- Deep ulcer to tendon, bone, or joint capsule (no abscess/OM)
- Treatment
- Surgical debridement, antibiotics if infected, offloading
- Healing Rate
- 70-80% at 12-16 weeks
- Description
- Deep ulcer with abscess, osteomyelitis, or septic arthritis
- Treatment
- Surgical debridement, IV antibiotics, possible amputation
- Healing Rate
- 50-60% limb salvage with aggressive treatment
- Description
- Localized gangrene (forefoot or heel)
- Treatment
- Partial amputation (toe, ray, transmetatarsal)
- Healing Rate
- 80-90% healing of amputation site
- Description
- Extensive gangrene of entire foot
- Treatment
- Major amputation (below-knee or above-knee)
- Healing Rate
- 80-90% BKA healing; 50-60% AKA healing
- Simple and easy to remember
- Widely used in clinical practice and research
- Good inter-observer reliability
- Guides treatment escalation
- Does not separately grade ischemia and infection
- Limited prognostic value for healing
- Does not account for location
This completes the Wagner classification overview.
PEDISPEDIS - IWGDF Classification System
Hook:PEDIS is the comprehensive assessment framework recommended by International Working Group on Diabetic Foot
Clinical Assessment
History
Key Questions:
- Duration of diabetes and glycemic control (HbA1c)
- Previous ulcers or amputations (strongest risk factor)
- Claudication, rest pain (vascular symptoms)
- Sensory symptoms: numbness, tingling, burning (neuropathy)
- Trauma or precipitating event (often forgotten by patient due to neuropathy)
- Footwear: what do they wear at home? (many patients wear inappropriate slippers)
- Self-care ability: can they see their feet? Can they reach to inspect?
Physical Examination
- Pulses: dorsalis pedis, posterior tibial (compare sides)
- Pallor: elevation pallor test (Buerger test)
- Perfusion: capillary refill time (normal less than 3 seconds)
- Paresthesias: neuropathic symptoms
- Pain: rest pain suggests critical ischemia
- 10g monofilament testing: 9 sites on plantar foot (hallux, met 1-5, mid-arch, heel)
- Loss of sensation at ANY site = loss of protective sensation
- Sensitivity 90%, specificity 80% for ulcer risk
- Vibration perception: 128 Hz tuning fork at hallux IPJ
- Ankle reflexes: absent in peripheral neuropathy
- Pinprick: assesses small fiber function
- Foot deformities: claw toes, hallux valgus, Charcot neuroarthropathy
- Ankle range of motion: equinus (less than 10° dorsiflexion) increases forefoot pressure
- Muscle strength: intrinsic atrophy, inability to spread toes
- Gait analysis: observe pressure pattern
- Location: plantar (neuropathic), margins/dorsum (ischemic), interdigital (mixed)
- Size: measure in cm² (length × width)
- Depth: probe to bone test
- Base: granulation tissue (red = healthy), slough (yellow), eschar (black)
- Edges: callused, undermined, macerated
- Surrounding skin: erythema (measure distance), warmth, edema
- Exudate: amount, color, odor
- Sterile metal probe inserted into debrided ulcer
- Positive: hard, gritty resistance = bone felt
- In the original hospitalised, infected cohort (Grayson, JAMA 1995): sensitivity 66%, specificity 85%, positive predictive value 89%, negative predictive value 56%
- Test performance is prevalence-dependent: in high-risk infected wounds a positive probe is highly predictive of osteomyelitis; in lower-risk outpatients a negative result is more reassuring
- A positive probe in a moderate-to-severe DFU warrants treatment for osteomyelitis pending MRI/bone biopsy; a negative result does not exclude it if clinical suspicion is high
Differential Diagnosis
Not every wound on a diabetic foot is a simple neuropathic ulcer. Distinguishing the dominant mechanism (and excluding mimics) changes management entirely.
- Typical location / look
- Plantar, over met head or heel; punched-out with callused rim
- Pain
- Painless
- Pulses / perfusion
- Normal (warm, bounding)
- Key discriminator
- Loss of protective sensation, high plantar pressure point
- Typical location / look
- Margins, tips of toes, dorsum; little callus, dry/necrotic
- Pain
- Often painful (rest pain)
- Pulses / perfusion
- Reduced/absent; cool, hairless
- Key discriminator
- ABI less than 0.9 or TBI less than 0.7, low TcPO2; needs vascular workup
- Typical location / look
- Hot, swollen, deformed midfoot - usually NO ulcer early
- Pain
- Painless or mild
- Pulses / perfusion
- Normal (warm, often bounding)
- Key discriminator
- Temperature difference greater than 2°C vs other foot, fragmentation on X-ray; no portal of entry
- Typical location / look
- Spreading erythema, warmth, sometimes purulence
- Pain
- Variable (tender)
- Pulses / perfusion
- Usually intact
- Key discriminator
- Systemic signs, raised inflammatory markers, responds to antibiotics
- Typical location / look
- Gaiter area, irregular, exudative; haemosiderin, oedema
- Pain
- Aching, relieved by elevation
- Pulses / perfusion
- Pulses usually present
- Key discriminator
- Chronic venous insufficiency signs; not a pressure point
- Typical location / look
- Non-healing, rolled/everted edges, atypical granulation
- Pain
- Variable
- Pulses / perfusion
- Variable
- Key discriminator
- Failure to heal despite optimal care - biopsy the edge
Both present as a hot, red, swollen foot. Elevation test: in acute Charcot the erythema and warmth substantially settle after a few minutes of limb elevation, whereas infective erythema does not. No ulcer/portal of entry and fragmentation on X-ray favour Charcot. When uncertain, immobilise and offload while excluding infection - treating a non-existent infection is less harmful than missing acute Charcot.
Red Flags Requiring Urgent Action:
- Systemic signs: fever, tachycardia, hypotension (sepsis)
- Gas in tissues: crepitus on exam or air on X-ray (gas gangrene)
- Rapidly spreading erythema: necrotizing fasciitis
- Bullae or skin necrosis: limb-threatening infection
- Foul odor: anaerobic infection
- Critical ischemia: rest pain, ABI less than 0.5, tissue loss
These indicate limb- or life-threatening infection requiring same-day surgical consultation.



PPPThe 3 P's of Diabetic Foot Assessment
Hook:The 3 P's are the essential bedside tests every diabetic foot needs
Investigations
Laboratory Tests
Baseline Blood Tests:
- HbA1c: glycemic control over 3 months (target less than 7%)
- Inflammatory markers: CRP, ESR (elevated in osteomyelitis, may be normal in acute infection)
- WBC: may be normal despite infection (blunted response)
- Renal function: many diabetics have CKD
- Blood cultures: if systemic signs
Vascular Assessment
Ankle-Brachial Index (ABI):
- Normal: 0.9-1.3
- PAD: less than 0.9
- Critical ischemia: less than 0.5
- Falsely elevated (calcified vessels): greater than 1.3 (use toe pressures instead)
Toe-Brachial Index (TBI): less affected by calcification
- Normal: greater than 0.7
- Critical ischemia: less than 0.5
Transcutaneous oxygen pressure (TcPO2):
- Greater than 40 mmHg: good healing potential
- 30-40 mmHg: borderline
- Less than 30 mmHg: poor healing, revascularization needed
Duplex ultrasound: if ABI abnormal, map disease for revascularization
CT angiography or MR angiography: if revascularization planned
Imaging for Osteomyelitis
- Sensitivity
- 54-68%
- Specificity
- 68-75%
- Advantages
- Cheap, widely available, detects gas
- Disadvantages
- Insensitive early (2-3 weeks delay), cannot assess soft tissue
- Sensitivity
- 90-95%
- Specificity
- 70-85%
- Advantages
- Best for bone marrow edema, soft tissue abscess
- Disadvantages
- Expensive, cannot if metal implants, lower specificity
- Sensitivity
- 74-100%
- Specificity
- 68-90%
- Advantages
- Functional imaging, specific for infection
- Disadvantages
- Time-consuming, radiation, may miss chronic OM
- Sensitivity
- Gold standard
- Specificity
- Gold standard
- Advantages
- Histology + culture, definitive diagnosis
- Disadvantages
- Invasive, may seed infection, patient refusal
- Bone marrow edema (low T1, high T2/STIR signal)
- Cortical destruction
- Soft tissue abscess or sinus tract
- Contrast enhancement
- Periosteal reaction
- Cortical erosion
- Bone destruction
- Soft tissue gas (indicates gas-forming organisms)
Microbiology
- Do NOT swab superficial wound - this only cultures colonizers
- Deep tissue culture AFTER debridement:
- Curette or bone biopsy for best yield
- Send for aerobic, anaerobic, and fungal cultures
- Specify "diabetic foot infection" to lab (alerts to polymicrobial nature)
- Uninfected/mild: Staphylococcus aureus, Streptococci (monomicrobial)
- Moderate/severe: polymicrobial
- Gram-positives: S. aureus (including MRSA), Streptococci, Enterococci
- Gram-negatives: E. coli, Proteus, Klebsiella, Pseudomonas
- Anaerobes: Bacteroides, Peptostreptococcus (foul odor, necrosis)
Management Algorithm
Multidisciplinary Team Approach
Evidence: Multidisciplinary foot care teams reduce amputation rates by 49-85% compared to standard care.
Essential Team Members:
- Diabetologist or endocrinologist (glycemic control)
- Podiatrist (wound care, debridement, orthotics)
- Vascular surgeon (revascularization)
- Orthopaedic or plastic surgeon (reconstruction, amputation)
- Infectious disease specialist (complex infections, osteomyelitis)
- Orthotist (custom footwear, AFOs)
- Diabetes nurse educator (self-care, prevention)
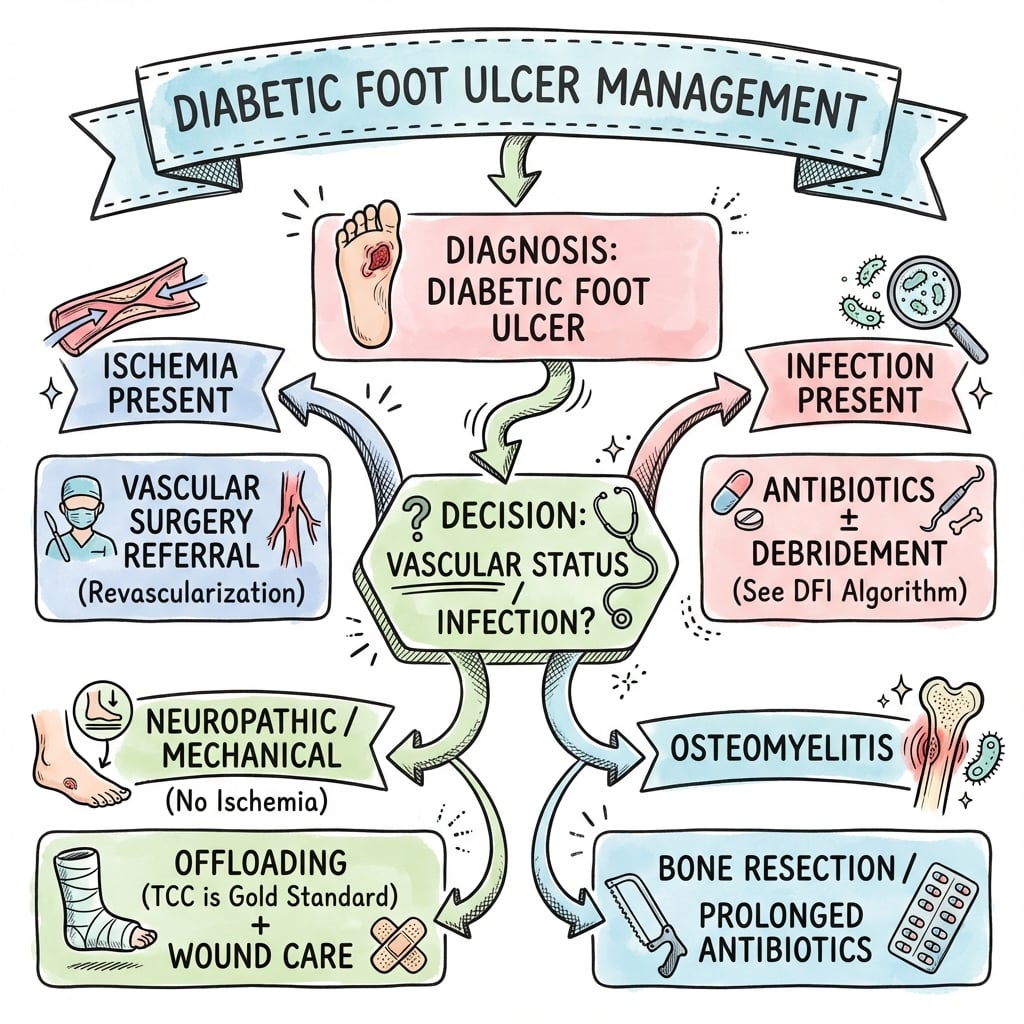
The 5 Pillars of DFU Management
1. Offloading (CRITICAL) 2. Debridement 3. Infection Control 4. Vascular Assessment and Revascularization 5. Metabolic and Wound Environment Optimization
Offloading (Pillar 1)
Offloading is THE critical treatment for plantar neuropathic DFUs. No amount of antibiotics, dressings, or growth factors will heal an ulcer if repetitive pressure continues. In comparative studies, offloading alone heals 85-95% of superficial neuropathic ulcers within 12 weeks.
Total Contact Casting (Gold Standard)
- Redistributes pressure from ulcer site to entire plantar surface and lower leg
- Reduces peak plantar pressure by 80-90% at ulcer site
- Immobilizes ankle (reduces shear stress)
- Non-removable - ensures compliance (patients cannot cheat)
- Apply minimal padding over ulcer and bony prominences
- Mold cast intimately to foot and leg (total contact)
- Extend to just below fibular head
- Heel rocker on bottom for gait
- Change weekly initially (edema reduction), then every 2 weeks
- Healing rate: 85-95% at 12 weeks for Wagner 1-2 ulcers
- Healing time: 6-8 weeks average (vs 12-16 weeks in removable devices)
- Recurrence rate: 30-50% at 2 years (need long-term footwear)
- Active infection (moderate or severe)
- Critical ischemia (ABI less than 0.5)
- Excessive edema (unstable limb volume)
- Non-compliant patient (fall risk)
- Suspected Charcot neuroarthropathy (acute phase)
Instant Total Contact Cast (iTCC Walker)
Alternative to TCC:
- Removable cam walker rendered non-removable with cohesive bandage or fiberglass
- Prefabricated device with custom foam padding
- Similar efficacy to TCC (75-90% healing) IF rendered non-removable
- Allows wound inspection without cast removal
Advantage: Can be temporarily removed for wound care by healthcare provider Disadvantage: If patient can remove it (non-compliance), efficacy drops to 30-50%
Other Offloading Devices
- Healing Rate
- 85-95%
- Compliance
- 100% (non-removable)
- Indications
- Gold standard for plantar neuropathic ulcers
- Cost
- $$
- Healing Rate
- 75-90%
- Compliance
- 95% (cohesive wrap)
- Indications
- Alternative if TCC unavailable or infection present
- Cost
- $$$
- Healing Rate
- 30-50%
- Compliance
- 20-30% (poor)
- Indications
- Non-compliant patients, acute Charcot
- Cost
- $$
- Healing Rate
- 30-40%
- Compliance
- 40-60%
- Indications
- Post-op amputation, forefoot offloading
- Cost
- $
- Healing Rate
- 40-60%
- Compliance
- 70-80%
- Indications
- Temporary measure, outpatient debridement
- Cost
- $
- Healing Rate
- Prevention
- Compliance
- 80%
- Indications
- Healed ulcers, prevention, redistribution
- Cost
- $$$
Key Principle: Non-removable greater than removable. Studies show patients wear removable devices only 20-30% of the time when alone at home, despite reporting "full compliance."
The same neuropathy that caused the ulcer also removes the pain signal that would remind patients to protect the foot. They genuinely forget because it doesn't hurt. This is why non-removable devices are essential - they provide external memory.
Surgical Offloading
- Indication: Equinus contracture (ankle dorsiflexion less than 10°)
- Mechanism: reduces forefoot pressure by 25-30%
- Technique: percutaneous triple hemisection
- Outcomes: 60-80% reduction in recurrence vs standard care
- Risks: overlengthening → calcaneal ulcers
- Indication: recurrent plantar ulcer under prominent met head
- Single met resection (usually met 2 or 3)
- Avoid multiple adjacent mets (transfer lesions)
- Shortens metatarsal, elevates met head
- Healing rate: 80-90%
Debridement and Wound Care (Pillar 2)
Sharp Debridement (Essential)
- Removes necrotic tissue, callus, and biofilm
- Converts chronic wound to acute wound (restarts healing cascade)
- Reduces bacterial burden by 90-99%
- Exposes healthy bleeding tissue
- Weekly debridement until healed (at minimum)
- Use scalpel to remove all hyperkeratosis (callus) around wound edges
- Debride to healthy, bleeding tissue (Spongey-bleeding base indicates dermis)
- Saucerize edges (bevel wound edges to prevent undermining)
- Send tissue for culture (NOT swab)
Evidence: Weekly sharp debridement associated with 2-3x higher healing rates vs episodic debridement.
Wound Dressing Principles
Goal: Maintain moist wound environment (improves epithelialization by 50% vs dry wounds)
Dressing Selection by Wound Characteristics:
- Exudate
- Minimal
- Dressing
- Hydrogel
- Mechanism
- Autolytic debridement
- Exudate
- Moderate
- Dressing
- Hydrocolloid or foam
- Mechanism
- Absorb exudate, protect
- Exudate
- Light
- Dressing
- Hydrocolloid, alginate
- Mechanism
- Maintain moisture
- Exudate
- Minimal
- Dressing
- Film or hydrocolloid
- Mechanism
- Non-adherent, protect
- Exudate
- Heavy
- Dressing
- Antimicrobial (silver, iodine) + foam
- Mechanism
- Infection control + absorption
Dressing Change Frequency:
- Infected wounds: daily
- Clean granulating: every 3-7 days
- Goal: minimize wound disruption
Advanced Wound Therapies
- Indications: post-surgical wounds, deep wounds after debridement
- Mechanism: removes exudate, reduces edema, promotes granulation
- Evidence: 30-50% faster healing vs standard dressings in diabetic wounds
- Contraindications: untreated osteomyelitis, exposed vessels, malignancy
- Platelet-derived growth factor (becaplermin): 50% increase in healing vs placebo (NNT = 7)
- Apply daily after debridement
- FDA-approved for diabetic neuropathic ulcers
- Living cell therapy: human fibroblast/keratinocyte sheets (Apligraf, Dermagraft)
- Healing: 56% vs 38% with standard care at 12 weeks
- Expensive (USD 1000-2500 per application)
- Controversial evidence: some RCTs show benefit, others don't
- Mechanism: increases tissue oxygenation, enhances WBC function, angiogenesis
- Indications (if available): Wagner 3-4 with failed standard care
- Regimen: 90-120 minutes at 2.0-2.5 ATA, 30-40 sessions
- Cochrane review: insufficient evidence to recommend routinely
Infection Control (Pillar 3)
IDSA/IWGDF Infection Criteria
Diagnosis of Infection (NOT just colonization):
- Purulence (pus), OR
- 2 or more inflammatory signs:
- Local warmth
- Erythema (greater than 2 cm from wound edge = moderate infection)
- Lymphangitis
- Edema
- Pain or tenderness (unusual in neuropathic patients - ominous if present)
Severity Grading:
- Clinical Features
- No signs of infection
- Treatment
- No antibiotics - wound care and offloading only
- Setting
- Outpatient
- Clinical Features
- Erythema less than 2cm, superficial, no systemic signs
- Treatment
- Oral antibiotics, outpatient debridement
- Setting
- Outpatient
- Clinical Features
- Erythema greater than 2cm OR deep tissue involved, no systemic signs
- Treatment
- IV or oral antibiotics, surgical debridement often needed
- Setting
- Inpatient or close outpatient
- Clinical Features
- SIRS present OR limb-threatening (necrotizing infection, gangrene)
- Treatment
- IV broad-spectrum antibiotics, urgent surgery, ICU if septic
- Setting
- Inpatient (ICU if unstable)
Antibiotic Therapy
Principles:
- Treat infection, NOT colonization - all chronic wounds are colonized
- Empiric therapy based on severity and previous cultures
- Narrow to culture results after 48-72 hours
- Duration: 1-2 weeks for soft tissue; 4-6 weeks for osteomyelitis
Empiric Regimens (IDSA Guidelines):
Mild Infection (outpatient, oral):
- Cephalexin 500mg QID, OR
- Amoxicillin-clavulanate 875mg BID, OR
- Clindamycin 300mg TID (if penicillin allergy)
- Duration: 1-2 weeks
Moderate Infection (inpatient or close outpatient):
- Ampicillin-sulbactam 3g IV Q6H, OR
- Ceftriaxone 2g IV daily PLUS metronidazole 500mg IV Q8H, OR
- Ertapenem 1g IV daily (if MRSA risk, add vancomycin)
Severe Infection (inpatient, broad-spectrum):
- Vancomycin 15mg/kg IV Q12H (trough 15-20) PLUS
- Piperacillin-tazobactam 4.5g IV Q6H, OR
- Meropenem 1g IV Q8H
- Consider antifungal if prolonged antibiotics or immunosuppressed
MRSA Coverage (add if risk factors: previous MRSA, healthcare exposure, failed cephalosporin):
- Vancomycin, OR
- Linezolid 600mg PO/IV BID, OR
- Daptomycin 6mg/kg IV daily
Osteomyelitis Management
- Probe-to-bone positive (high PPV in infected wounds)
- MRI: bone marrow edema + cortical destruction
- Bone biopsy (gold standard): histology + culture
- Remove all infected, necrotic bone until bleeding viable bone
- Send bone for culture and histology
- IV antibiotics for 4-6 weeks based on bone culture
- Cure rate: 60-80% for non-heel, 40-60% for heel
- Indications: poor surgical candidate, patient refuses, minor bone involvement
- 6-12 weeks IV or highly bioavailable oral (fluoroquinolone, linezolid)
- Cure rate: 60-70% (similar to surgery in some studies)
- Requires close follow-up
- Indications: extensive bone destruction, failed conservative treatment, limb not salvageable
- May be curative if removes all infected tissue
After adequate surgical debridement removing all infected bone, 2-4 weeks of antibiotics may suffice. If residual infected bone remains or antibiotics-only treatment, 6 weeks minimum. Recent evidence suggests shorter courses equally effective after adequate debridement.
Revascularisation and the Neuroischaemic Foot (Pillar 4)
Vascular assessment and revascularisation is listed as the fourth pillar of management and appears as a branch in the algorithm, but it deserves to be developed because perfusion is frequently the rate-limiting step: roughly half of patients with a diabetic foot ulcer have peripheral arterial disease, and an ischaemic or neuroischaemic ulcer will not heal with offloading, debridement and antibiotics alone until inline blood flow to the foot is restored. Inadequate perfusion is the dominant driver of non-healing and of major amputation.
When to suspect ischaemia and investigate
Use the perfusion findings already covered: absent pedal pulses, a cool/hairless foot, ABI less than 0.9 (or non-compressible greater than 1.3 from medial calcification — fall back to toe-brachial index, toe pressure or TcPO2), monophasic Doppler waveforms, and TcPO2 less than 30 mmHg. Any ulcer that fails to progress despite optimal wound care, or any clinically ischaemic/neuroischaemic ulcer, warrants prompt vascular imaging (arterial duplex, then CT or MR angiography, or catheter angiography) and a vascular surgery referral. Healing-potential thresholds worth targeting after intervention are TcPO2 greater than 40 mmHg and restoration of at least one patent tibial/pedal vessel to the foot.
Staging limb threat
Beyond Wagner/Texas/PEDIS, the SVS WIfI classification (Wound, Ischaemia, foot Infection) grades each of those three axes (0–3) to estimate the threat to the limb, the likely benefit of revascularisation and the risk of major amputation. It is the vascular-surgery counterpart to the ulcer-depth systems and is increasingly used to decide who needs urgent perfusion restoration.
Choosing the revascularisation strategy
- Best suited to
- High-comorbidity patient, focal/short infrapopliteal lesions, no suitable vein conduit
- Advantages
- Minimally invasive, low periprocedural risk, repeatable, short recovery
- Limitations
- Higher restenosis and reintervention rate; durability of inline flow more limited
- Best suited to
- Fit patient with good-quality saphenous vein, long occlusions, durable distal target needed
- Advantages
- Most durable inline flow; superior limb salvage when adequate vein is available
- Limitations
- Larger operation, conduit/wound complications, higher upfront physiological cost
Both restore perfusion; the choice is individualised to patient fitness, lesion anatomy and conduit availability. The landmark randomised trials informing this debate are BASIL and BEST-CLI: the overall message is that a durable surgical bypass with a good-quality autologous (great saphenous) vein tends to give the best limb-salvage and the fewest reinterventions in patients fit for surgery, whereas an endovascular-first strategy is favoured for higher-risk patients, suitable focal lesions, or when no adequate vein is available. In the foot itself, the angiosome concept (Attinger) holds that directing flow to the specific source artery supplying the angiosome containing the ulcer (direct/angiosome-targeted revascularisation) may improve healing and limb salvage; where the target vessel cannot be reached, indirect revascularisation through collaterals can still heal many wounds.
Sequencing with infection and the salvage-vs-amputation decision
In the infected ischaemic foot, urgent source control comes first — drain pus and debride necrotic/infected tissue without delay — then revascularise promptly; do not let angiography planning hold up control of spreading sepsis. If perfusion cannot be restored, or the foot is not functionally salvageable (extensive tissue loss, non-ambulatory patient, unreconstructable disease), a primary amputation at a healing level may give a better, faster functional outcome than repeated failed salvage attempts (see Surgical Management).
For a neuropathic plantar ulcer, offloading is the priority. For a neuroischaemic or ischaemic ulcer, perfusion is the priority — wound care and a total contact cast will fail (and compressive casting can worsen ischaemia) until blood flow is restored. Quote the thresholds: ABI less than 0.5 or TcPO2 less than 30 mmHg means urgent vascular referral; aim for TcPO2 greater than 40 mmHg and at least one patent vessel to the foot. State that you would obtain source control of any infection first, then revascularise.
Surgical Management
Indications for Surgery
- Necrotizing soft tissue infection
- Gas gangrene (crepitus, gas on X-ray)
- Sepsis or severe infection with systemic toxicity
- Compartment syndrome of foot
- Wet gangrene with systemic signs
- Osteomyelitis (surgical debridement)
- Deep abscess requiring drainage
- Non-healing ulcer despite 6-12 weeks optimal conservative care
- Recurrent ulceration requiring prophylactic surgery (ATL, exostectomy)
- Dry gangrene (scheduled amputation once demarcated)
This section covers surgical indications and timing.
Charcot Neuroarthropathy
Definition and Pathophysiology
Charcot neuroarthropathy (Charcot foot) is a progressive destructive arthropathy of the foot and ankle in patients with peripheral neuropathy, resulting in bone and joint destruction, fractures, and deformity.
0.1-0.4% of diabetics; up to 30% in high-risk diabetic populations
- Neurovascular theory: autonomic neuropathy → increased blood flow → bone resorption
- Neurotraumatic theory: loss of protective sensation → repetitive microtrauma → fractures
Eichenholtz Classification (Stages)
- Warm, swollen foot
- NO X-ray changes yet
- Mimics cellulitis or DVT
- Critical to diagnose - treat now to prevent deformity
- X-ray: fractures, fragmentation, joint dislocation
- Clinically: warm, swollen, erythematous
- Most important stage to immobilize
- X-ray: absorption of debris, early healing
- Clinically: edema decreases, warmth decreases
- Continue immobilization
- X-ray: bony remodeling, sclerosis, deformity is now fixed
- Clinically: cool, stable
- Transition to protective footwear/AFO
Clinical Patterns
- Tarsometatarsal joints (Lisfranc)
- Rocker-bottom deformity
- High risk of plantar ulceration at apex
- Subtalar, talonavicular, calcaneocuboid joints
- Valgus or varus deformity
- Tibiotalar joint
- Unstable, high amputation risk
- Calcaneal fracture
- Loss of heel height
Management
- Non-weight bearing in total contact cast
- Cast changes every 1-2 weeks (monitor for progression)
- Serial X-rays to monitor healing
- Continue until: edema resolved, temperature difference less than 2°C compared to contralateral
- Duration: typically 3-6 months minimum
- Gradual transition to weight-bearing in CROW walker (Charcot Restraint Orthotic Walker)
- Custom AFO or CROW boot for long-term use
- Extra-depth shoes with custom orthotics
- Recurrent ulceration despite bracing
- Severe instability preventing bracing
- Techniques: exostectomy, osteotomy, arthrodesis (fusion)
- High complication rate (nonunion, infection, Charcot recurrence)
Do NOT confuse acute Charcot with infection! Both present with warm, red, swollen foot. Key differences:
- Charcot: NO ulcer (unless late), X-ray shows fractures/dislocation, CRP/ESR elevated but WBC normal
- Infection: ulcer present, purulence, systemic signs, WBC elevated
When in doubt, immobilize and observe - treating infection that doesn't exist is less harmful than missing Charcot.
Complications
Local Complications
- Cellulitis: spreading erythema, warmth, edema
- Abscess: fluctuant collection requiring drainage
- Osteomyelitis: 10-15% of moderate-severe infections
- Septic arthritis: joint involvement, rapid destruction
- Necrotizing fasciitis: rare but life-threatening (mortality 20-30%)
- Gas gangrene: crepitus, systemic toxicity (requires urgent debridement)
- Biofilm formation (60-80% of chronic wounds)
- Wound edge senescence (cells stop dividing)
- Persistent inflammation
- Tissue hypoxia from PAD
- Continued mechanical stress (poor offloading compliance)
- Minor amputation (toe, ray, TMA): 50-90% healing depending on level
- Major amputation (BKA, AKA): required if limb-threatening infection or critical ischemia
- Contralateral amputation risk: 50% at 5 years after first amputation
- Occurs in 0.1-0.4% of diabetics
- Can develop during or after DFU treatment
- Rocker-bottom deformity leads to recurrent ulceration if not braced
Systemic Complications
- Diabetic foot infections are leading cause of sepsis in diabetics
- Mortality 10-40% in severe DFU-related sepsis
- Risk factors: delayed presentation, extensive necrosis, gas-forming organisms
- Infection causes insulin resistance
- Hyperglycemia worsens WBC function (vicious cycle)
- May precipitate diabetic ketoacidosis (DKA) in type 1 diabetics
- Increased MI risk during acute infection (inflammatory stress)
- DVT/PE risk from immobilization and hypercoagulability
- Diabetic nephropathy worsens with sepsis
- Antibiotic nephrotoxicity (vancomycin, aminoglycosides)
- Contrast-induced nephropathy from imaging
Psychological and Social Complications
- 40-50% of patients with diabetic foot complications have depression
- Fear of amputation
- Loss of independence
- Reduced quality of life
- Average DFU treatment cost: USD 20,000-50,000 per episode
- Major amputation with rehabilitation: USD 50,000-100,000
- Loss of employment (30-50% cannot return to work)
- Caregiver burden
- 5-year mortality after DFU: 30-40% (cardiovascular disease)
- 5-year mortality after major amputation: greater than 70% (JAMA 2023; worse than most cancers)
- 1-year mortality after major amputation: 30%
Treatment Complications
- Pressure ulcers from TCC if poorly applied (5-10%)
- Falls risk with walker devices
- Contralateral limb stress (transfer lesions)
- Equinus contracture after prolonged immobilization
- Wound breakdown: 10-30% depending on level
- Infection: 5-15% post-amputation
- Hematoma: 5-10%
- Phantom limb pain: 60-80% after major amputation
- Stump pain: 20-40%
- C. difficile infection (5-10% with prolonged antibiotics)
- Antibiotic resistance (MRSA, VRE, ESBL organisms)
- Nephrotoxicity, hepatotoxicity
- Allergic reactions
Recurrence and Long-term Outcomes
- 40% at 1 year despite initial healing
- 50% at 3 years
- 70% at 5 years
- Risk factors: poor offloading compliance, previous amputation, Charcot foot, PAD
- Multidisciplinary team approach reduces amputation by 49-85%
- Early aggressive treatment prevents progression
- Lifelong surveillance and therapeutic footwear
- Patient education and self-care
- Glycemic control (each 1% HbA1c reduction = 25% fewer microvascular complications)
The high mortality (50% at 5 years post-major amputation) reflects that DFU is a marker of severe systemic disease, not just a local problem. Patients have:
- Advanced diabetes (often 15-20 years duration)
- Severe PAD (multivessel disease)
- Cardiac disease (MI risk 3-4x higher)
- Renal failure (dialysis patients have 2-3x amputation risk)
- Multiple comorbidities
DFU is the "tip of the iceberg" - the visible manifestation of systemic atherosclerosis and metabolic disease.
Prevention Strategies
Risk Stratification and Surveillance
IWGDF Risk Categories and Surveillance Frequency:
- Category 0 (no neuropathy): annual screening
- Category 1 (neuropathy alone): 6-12 month screening
- Category 2 (neuropathy + PAD or deformity): 3-6 month screening
- Category 3 (previous ulcer or amputation): 1-3 month screening
Patient Education (Self-Care)
- Look for blisters, cuts, cracks, redness
- Use mirror if cannot see bottom of foot
- Check between toes
- If vision impaired, have caregiver inspect
- Wash with lukewarm water (test with elbow, not foot)
- Dry thoroughly, especially between toes
- Apply moisturizer (but NOT between toes)
- Check shoes for foreign objects before wearing
- Cut toenails straight across (not rounded)
- File edges smooth
- If cannot reach or see, have podiatrist cut nails
- Do NOT walk barefoot (inside or outside)
- Do NOT use heating pads or hot water bottles on feet
- Do NOT try to remove calluses or corns themselves (risk of injury)
- Do NOT smoke (impairs healing)
Footwear Prescription
- Extra-depth shoes (1/2 inch extra toe box depth)
- Custom orthotics with accommodative padding
- Rocker-sole to reduce forefoot pressure
- Most national diabetes programmes subsidise therapeutic footwear for patients with neuropathy, deformity or previous ulceration
- Continue protective footwear lifelong
- Replace every 6-12 months (breaks down with use)
- Replace orthotics annually
Home Foot-Temperature (Dermal Thermometry) Monitoring
After protective sensation is lost, the patient can no longer feel the inflammation that precedes ulceration — but it can be measured. Localised inflammation from a high-pressure "hotspot," early infection or acute Charcot raises the local skin temperature days before the skin breaks down. Daily home measurement of plantar skin temperature at matched sites on both feet detects this hotspot and turns an invisible warning into an actionable one.
- The patient measures the temperature at several matched plantar sites on each foot daily, using a handheld infrared dermal thermometer (or a temperature-sensing smart mat/insole).
- A sustained difference greater than about 2°C (roughly 4°F) between the same site on the two feet on consecutive days signals impending tissue damage.
- The response is "thermometry-guided offloading": when a hotspot is found, the patient reduces walking/activity and contacts the foot-care team until the temperatures equalise.
- In the contemporary synthesis, off-loading triggered by skin-temperature hotspots roughly halved new ulceration (18.7% vs 30.8%; relative risk 0.51, 95% CI 0.31–0.84), comparable to the benefit of pressure-relieving therapeutic footwear (13.3% vs 25.4%; relative risk 0.49, 95% CI 0.28–0.84) (Armstrong, JAMA 2023, PMID 37395769; concept also emphasised in Armstrong, NEJM 2017, PMID 28614678).
- It is most valuable in high-risk feet (IWGDF Category 2–3, previous ulcer, Charcot) and is a particular help for patients who cannot see or reach their feet, complementing — not replacing — daily visual inspection.
Dermal thermometry is the prevention tool that exploits the same neuropathy that causes the ulcer: a greater than ~2°C side-to-side difference at matched plantar sites is an early warning of impending breakdown (high-pressure hotspot, infection or acute Charcot). Acting on it with temporary offloading reduces recurrence — the healed diabetic foot is a "foot in remission" requiring lifelong, structured surveillance, not a cure.
Glycemic Control
Evidence: Each 1% reduction in HbA1c associated with 25% reduction in microvascular complications (including neuropathy)
Target: HbA1c less than 7% (individualize based on patient factors)
Multidisciplinary Prevention Programs
Components of Successful Programs:
- Regular screening (based on risk category)
- Patient education (structured programs)
- Therapeutic footwear provision
- Podiatry for nail and callus care
- Prompt treatment of pre-ulcerative lesions
Evidence: Comprehensive prevention programs reduce:
- Ulcer incidence by 50-60%
- Amputation rates by 49-85%
- Recurrent ulcers by 35-50%
Guidelines, Registries & Global Practice
Global Epidemiology
A systematic review and meta-analysis (Zhang, Ann Med 2016; PMID 27585063) pooled a global diabetic foot ulcer prevalence of 6.3% among people with diabetes, with striking regional variation. The contemporary JAMA review (Armstrong, 2023; PMID 37395769) estimates ~18.6 million new ulcers worldwide each year.
- Figure
- 6.3% (95% CI 5.4-7.3%)
- Source
- Zhang 2016
- Figure
- 13.0% / 7.2% / 5.5% / 5.1% / 3.0%
- Source
- Zhang 2016
- Figure
- ~18.6 million
- Source
- Armstrong 2023
- Figure
- ~80%
- Source
- Armstrong 2023
- Figure
- ~30-40%
- Source
- Armstrong 2023
- Figure
- ~42% / ~65%
- Source
- Armstrong 2017, 2023
- Figure
- ~30% / greater than 70%
- Source
- Armstrong 2023
Sex (higher in men), diabetes duration, smoking, hypertension and retinopathy are consistent risk associations (Zhang 2016).
Major Guidelines, Side by Side
The dominant international standard is the IWGDF (International Working Group on the Diabetic Foot), updated as a guideline suite; IDSA governs infection; NICE NG19 (UK) and AAOS/ADA statements broadly align. Where the headline recommendations differ, the differences are modest and mostly emphasis.
- IWGDF / IDSA
- Non-removable knee-high device (TCC or irremovable walker) first-line
- NICE (UK, NG19)
- Non-removable casting unless contraindicated by infection/ischaemia
- Evidence / note
- Strong / high-quality (Armstrong RCTs, PMID 11375363, 15735186)
- IWGDF / IDSA
- Clinical IDSA/IWGDF criteria (purulence OR 2+ inflammatory signs); do not treat colonisation
- NICE (UK, NG19)
- Diagnose clinically; send deep tissue, not superficial swab
- Evidence / note
- Strong consensus; aligned
- IWGDF / IDSA
- Antibiotics alone reasonable in selected non-ischaemic forefoot OM; otherwise surgical debridement
- NICE (UK, NG19)
- Refer to multidisciplinary foot service; individualise
- Evidence / note
- Level I RCT (Lázaro-Martínez, PMID 24130347) - equivalent in selected cases
- IWGDF / IDSA
- ~1-2 wks soft tissue; ~3 wks (or shorter post-resection) to 6 wks bone
- NICE (UK, NG19)
- Shortest effective course; review with cultures
- Evidence / note
- Moderate - shorter courses after adequate debridement
- IWGDF / IDSA
- IWGDF risk category 0-3 dictates 12-monthly to 1-3 monthly review
- NICE (UK, NG19)
- Annual screen; escalate by risk to 1-2 monthly if high-risk
- Evidence / note
- Strong consensus; aligned
- IWGDF / IDSA
- Consider only after standard care optimised; evidence limited
- NICE (UK, NG19)
- Not routinely recommended
- Evidence / note
- Weak / inconsistent RCT evidence
Registry & System-Level Evidence
Diabetic foot disease is tracked through diabetes and amputation registries rather than implant registries. National audit data (e.g. the UK National Diabetes Foot Care Audit) consistently show that earlier specialist multidisciplinary assessment is associated with better healing and fewer major amputations, and that organised high-risk foot services reduce major amputation rates — concordant with the pooled estimate that multidisciplinary care lowers major amputation versus usual care (OR 0.40, 95% CI 0.32-0.51; Armstrong 2023, PMID 37395769).
Global Practice Variation
- High-resource settings: ready access to TCC, vascular imaging, endovascular revascularisation, NPWT, advanced dressings and dedicated multidisciplinary foot clinics; emphasis on limb salvage and remission care.
- Limited-resource settings: later presentation, higher proportion of severe infection and major amputation, limited revascularisation; offloading may rely on improvised felted-foam/half-shoe techniques and sandals rather than TCC. Prevention and education yield the greatest marginal benefit where surgical and vascular services are scarce.
- Across all settings the principles are invariant: offload, debride, control infection, restore perfusion, optimise metabolism, and place the healed foot in lifelong remission care.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old man with 15-year history of type 2 diabetes presents with a 3-week history of a painless wound on the plantar aspect of his right foot under the 2nd metatarsal head. He walks daily for exercise. On examination, there is a 2cm diameter ulcer with callused edges, no purulence, minimal erythema (less than 1cm), and you can probe to the dermis but not deeper structures. His foot is warm with palpable pulses. He cannot feel a 10g monofilament at 6 of 9 sites.”
“A 62-year-old woman with poorly controlled diabetes (HbA1c 10.2%) presents with a 6-week history of a malodorous wound on her right great toe. She has been treating it herself with over-the-counter creams. On examination, there is a 3cm ulcer on the plantar aspect of the hallux with purulent drainage, surrounding erythema extending 4cm proximally, and exposed bone at the base when probed. Her foot is warm but you can palpate pedal pulses. Temperature is 38.1°C, WBC 14.2, ESR 78, CRP 92.”
“A 67-year-old man with longstanding diabetes and smoking history presents with a 4-month non-healing lateral foot ulcer. The ulcer is painful (unusual for him). On examination, his foot is cool, hairless, with absent pulses. ABI on right is 0.42, left is 0.68. Monofilament testing shows loss of protective sensation bilaterally. The ulcer is 2cm, clean with poor granulation tissue. TcPO2 at the forefoot is 28 mmHg.”
Pathophysiology Triad
- Sensory neuropathy: loss of protective sensation (10g monofilament)
- Motor neuropathy: intrinsic atrophy, claw toes, high pressure
- Peripheral arterial disease: tibial/peroneal, foot vessels spared
- Add immunopathy: WBC dysfunction from hyperglycemia
- Result: repetitive unrecognized trauma on insensate, ischemic, infection-prone foot
Classifications (Know All Three)
- Wagner 0-5: depth-based (0=intact skin → 5=whole foot gangrene)
- Texas: 4×4 grid (depth A-D × stage 0-3 for ischemia/infection)
- PEDIS: Perfusion, Extent, Depth, Infection, Sensation
- Wagner Grade 1 = superficial; Grade 2 = to tendon; Grade 3 = osteomyelitis/abscess
Assessment (The 3 P's)
- Pulses: dorsalis pedis, posterior tibial (absent = PAD)
- Protective sensation: 10g monofilament at 9 sites (1 abnormal = loss)
- Probe to bone: sensitivity 66%, specificity 85%, PPV 89% in infected wounds (Grayson) - positive = treat for osteomyelitis
- ABI: less than 0.9 = PAD; less than 0.5 = critical; greater than 1.3 = calcified (use toe pressure)
- TcPO2: less than 30 mmHg = poor healing; need revascularization
Offloading (THE Critical Treatment)
- Total contact cast: gold standard, 85-95% healing at 12 weeks
- Reduces plantar pressure 80-90%, non-removable = compliance
- iTCC walker: acceptable alternative if rendered non-removable
- Removable devices fail (patients wear only 20-30% of time)
- Continue offloading 4-6 weeks AFTER healing to prevent recurrence
Infection Diagnosis (IDSA Criteria)
- Purulence OR 2+ signs: warmth, erythema greater than 2cm, lymphangitis, edema, pain
- Mild: erythema less than 2cm, superficial → oral antibiotics outpatient
- Moderate: erythema greater than 2cm OR deep → IV antibiotics, surgery often needed
- Severe: SIRS or limb-threatening → IV broad-spectrum, urgent surgery
- Do NOT treat colonization - all chronic wounds colonized
Osteomyelitis Management
- Diagnosis: probe-to-bone (PPV ~89% in infected wounds), MRI (bone marrow edema), bone biopsy (gold standard)
- Treatment: surgical debridement to bleeding bone + 4-6 week IV antibiotics
- OR antibiotics alone for 6-12 weeks if poor surgical candidate
- Send bone for culture AND histology
- Cure rate 60-80% for non-heel OM with adequate surgery
Amputation Healing Rates
- Toe: 90-95% healing, minimal functional loss
- Ray: 80-90% healing, narrow shoe needed
- Transmetatarsal: 50-70% healing, high equinus risk (need AFO)
- Syme: 70-80% healing, end-bearing stump
- Below-knee: 80-90% healing, good prosthetic function
- Above-knee: 85-95% healing, poor prosthetic function
Prevention (Evidence-Based)
- Risk stratification: Category 0-3 determines screening frequency
- Therapeutic footwear: extra-depth shoes + custom orthotics
- Patient education: daily inspection, appropriate footwear, no barefoot
- Glycemic control: each 1% HbA1c reduction = 25% microvascular complication reduction
- Multidisciplinary teams reduce amputation by 49-85%
Exam Pearls
- Global DFU prevalence ~6.3%; recurrence ~42% at 1y and ~65% at 5y
- Major amputation 5-year mortality greater than 70% (worse than most cancers)
- Neuropathic ulcers painless; ischemic ulcers painful (key difference)
- Weekly sharp debridement essential - converts chronic to acute wound
- TCC is treatment, not adjunct - no offloading = no healing
Evidence Base
Total Contact Casting for Offloading (Landmark RCT)
- 63 patients with superficial, non-infected, non-ischaemic plantar ulcers randomised to total contact cast (TCC), removable cast walker (RCW) or half-shoe
- 12-week healing: TCC 89.5% vs RCW 65.0% vs half-shoe 58.3% (TCC vs others P=0.026, OR 5.4, 95% CI 1.1-26.1)
- TCC patients took significantly fewer daily steps (600 vs 1462 for half-shoe), explaining superior healing through enforced activity reduction
- Established the TCC as the gold-standard offloading device for plantar neuropathic ulceration
Diabetic Foot Ulcers: Contemporary Synthesis (JAMA Review)
- Approximately 18.6 million people are affected by a diabetic foot ulcer worldwide each year; ulcers precede 80% of diabetes-related lower-extremity amputations
- Multidisciplinary care lowers major amputation rates versus usual care (3.2% vs 4.4%; OR 0.40, 95% CI 0.32-0.51)
- Only about 30-40% of ulcers heal at 12 weeks; recurrence is approximately 42% at 1 year and 65% at 5 years
- 5-year mortality is approximately 30% overall and exceeds 70% after major amputation
Antibiotics vs Conservative Surgery for Diabetic Foot Osteomyelitis (RCT)
- 52 patients with neuropathic forefoot ulcers complicated by osteomyelitis (no ischaemia, no necrotising infection) randomised to antibiotics alone (90 days) vs conservative surgery + 10 days antibiotics
- Primary healing: 75% (antibiotics) vs 86.3% (surgery), not significantly different (P=0.33)
- Median time to healing 7 vs 6 weeks (P=0.72); no difference in minor amputation rates
- 4 antibiotic-group patients (16.6%) deteriorated and required surgery; 3 surgical patients needed reoperation
Probe-to-Bone Test for Osteomyelitis (Original Description)
- 76 infected pedal ulcers in 75 hospitalised diabetic patients; osteomyelitis in 66%
- Probing to bone: sensitivity 66%, specificity 85%, positive predictive value 89%, negative predictive value 56%
- In a high-prevalence (hospitalised, infected) population a positive probe strongly predicts contiguous osteomyelitis
- Later validation in lower-prevalence outpatient cohorts found higher sensitivity but lower PPV — interpret the test in context of pre-test probability
Diabetic Foot Ulcers and Their Recurrence (NEJM Review)
- Approximately 40% of patients have a recurrent ulcer within 1 year of healing, 60% within 3 years and 65% within 5 years
- Reframes the healed ulcer as 'foot in remission' requiring lifelong surveillance rather than cure
- Pressure-relieving therapeutic footwear and structured self-monitoring (including foot-temperature monitoring) reduce recurrence
- Adherence to offloading and footwear is the dominant modifiable determinant of recurrence
Global Epidemiology of Diabetic Foot Ulceration (Meta-analysis)
- Pooled global DFU prevalence 6.3% (95% CI 5.4-7.3%) among people with diabetes
- Marked regional variation: North America 13.0%, Africa 7.2%, Asia 5.5%, Europe 5.1%, Oceania 3.0%
- Higher prevalence in men (4.5%) than women (3.5%) and in type 2 (6.4%) than type 1 (5.5%) diabetes
- Affected patients were older, had longer diabetes duration, and more hypertension, retinopathy and smoking
Irremovable Offloading Improves Adherence and Healing (RCT)
- 50 patients with University of Texas grade 1A ulcers randomised to a removable cast walker vs the same walker wrapped to render it irremovable (instant TCC)
- 12-week healing 82.6% (irremovable) vs 51.9% (removable) (P=0.02, OR 1.8, 95% CI 1.1-2.9)
- Healed ulcers closed faster with the irremovable device (41.6 vs 58.0 days, P=0.02)
- Demonstrates that adherence — not the device itself — drives offloading efficacy