The Missed Drop Foot
- The tibialis anterior is the principal ankle dorsiflexor and a foot inverter; its tendon inserts on the medial cuneiform and first metatarsal base.
- Rupture is rare and most often SPONTANEOUS in patients over 45; it is frequently MISSED because the long toe extensors (EHL, EDL) partly compensate for dorsiflexion.
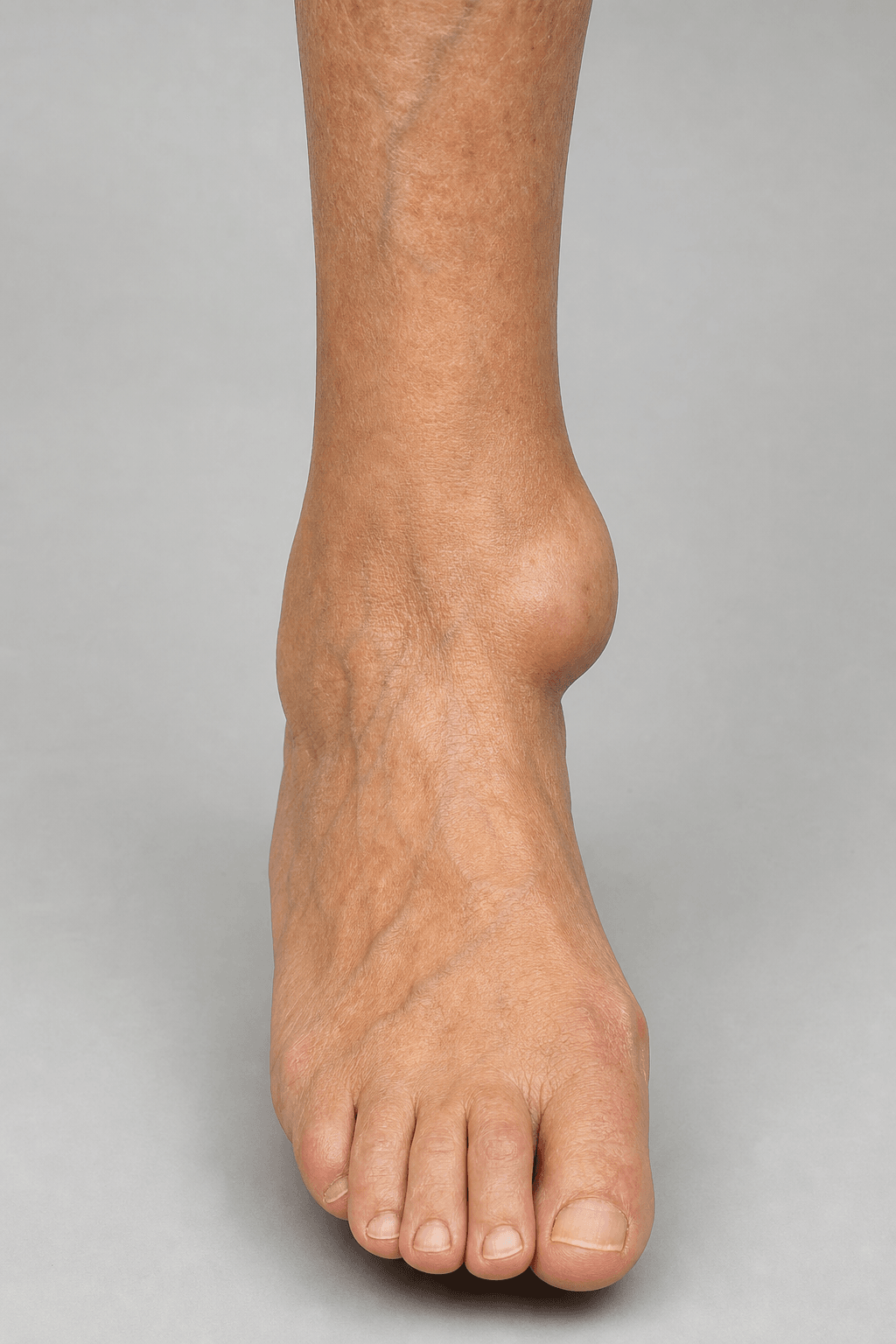
- It presents as a mechanical 'drop foot' / slap-foot gait, often with a soft-tissue bulge (pseudotumour) at the anterior ankle from the retracted tendon stump.
- Distinguish it from a NEUROLOGICAL foot drop (common peroneal palsy / L5 radiculopathy) - the tendon is absent on palpation and there is no sensory or other myotomal deficit.
- Conservative management (an ankle-foot orthosis) suits low-demand patients; surgical repair/reconstruction gives better function in active patients.
- Across the evidence, surgery outperforms conservative care, with best results from direct repair or a split tibialis-anterior / semitendinosus graft - EHL autograft has the worst outcomes.
- “The discriminator from neurological foot drop: an absent/abnormal tendon on palpation, an anterior-ankle pseudotumour, and NO sensory or proximal myotomal deficit.
- “Diagnosis is delayed because the patient still has some dorsiflexion (EHL/EDL) - always palpate the tibialis anterior tendon.
- “If reconstructing, do NOT sacrifice the EHL as the graft (worst outcomes) - it is a dorsiflexor you want to keep.
Drop foot with an absent/lax tibialis anterior tendon on palpation and often a pseudotumour (bunched retracted tendon) at the anterior ankle. No sensory loss, normal reflexes, and some active dorsiflexion preserved (EHL/EDL). Inversion is weak (TA).
Common peroneal palsy or L5 radiculopathy: drop foot plus a sensory deficit (dorsum/first web or L5 dermatome), often weak eversion (peroneal) and a positive Tinel at the fibular neck, or back pain and a wider myotomal pattern (L5). The tendon itself is intact and palpable.
Overview & Anatomy
The tibialis anterior is the strongest ankle dorsiflexor, but the extensor hallucis longus and extensor digitorum longus also dorsiflex the ankle. When the tibialis anterior tendon ruptures, these long extensors maintain enough dorsiflexion that the patient - and the unwary examiner - may not notice. The pain at rupture is often transient. The result is a commonly delayed or missed diagnosis of a mechanical drop foot.
- Tibialis anterior: originates from the lateral tibia/interosseous membrane (deep peroneal nerve, anterior compartment) and inserts on the medial cuneiform and base of the first metatarsal.
- Function: primary ankle dorsiflexion and foot inversion; controls foot plantarflexion at heel strike (eccentrically), preventing foot slap.
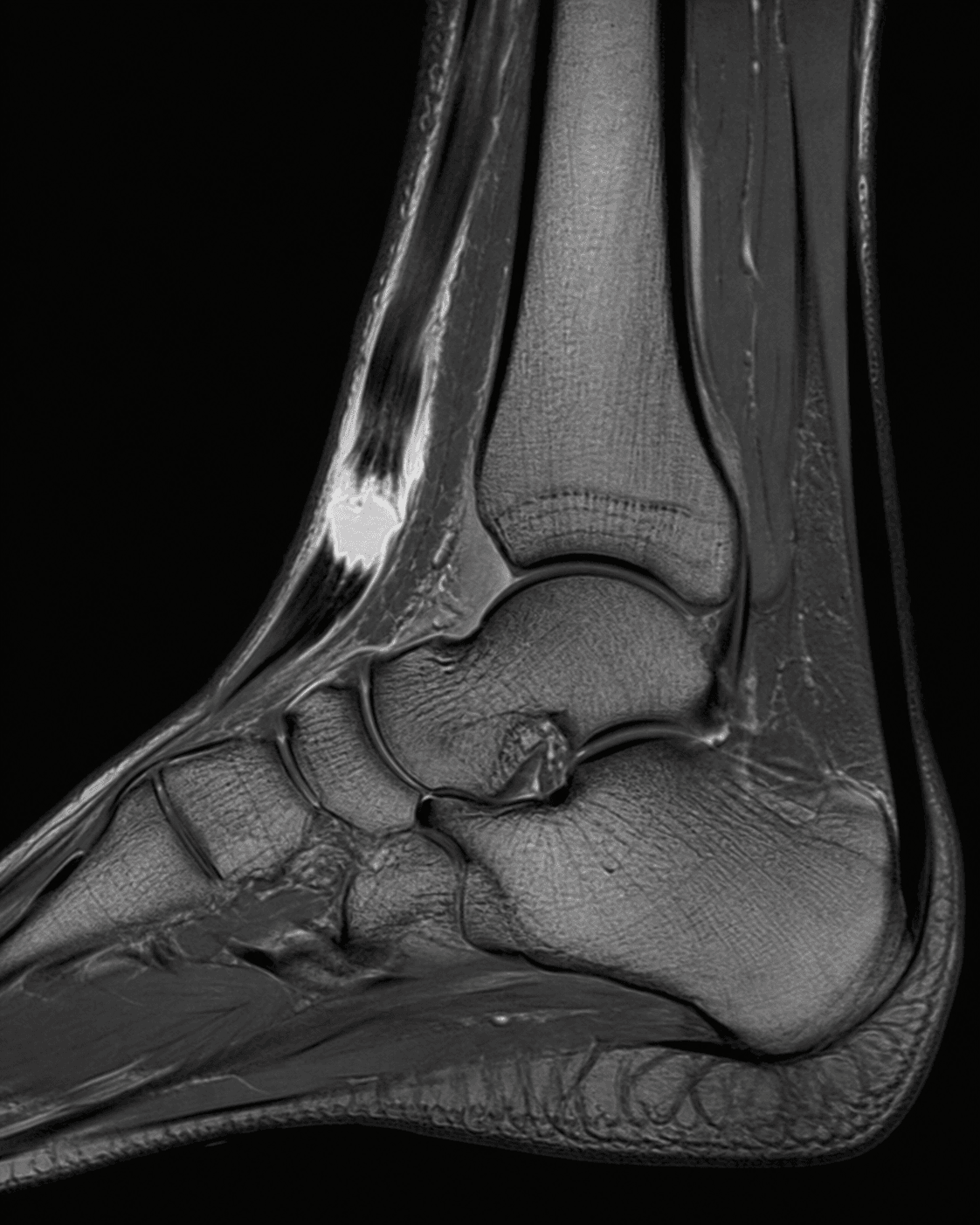
- Rupture site: typically degenerative near the insertion or beneath the superior/inferior extensor retinaculum in older patients; traumatic ruptures/lacerations occur more proximally/anteriorly.
Clinical Presentation
History
- Often an older patient (over 45) with spontaneous onset; may recall a minor strain or a transient "pop" with brief pain that settled.
- Slapping gait / tripping, catching the toes, difficulty clearing the foot.
- Traumatic cases: a laceration or a sudden forced plantarflexion against a dorsiflexing foot.
- Diagnosis is frequently delayed by weeks to months.
Management
Non-operative
- Suited to low-demand, elderly, or comorbid patients.
- An ankle-foot orthosis (AFO) controls the drop foot and prevents trips; physiotherapy maximises EHL/EDL compensation.
- Accepts a degree of dorsiflexion/inversion weakness; outcomes are poorer than surgery for active patients (pain and functional limitation).
MASKWhy the Drop Foot Is Missed
Hook:The long extensors MASK the lost tibialis anterior - palpate the tendon.
Evidence Base
Management of Isolated TA Rupture (Systematic Review/Meta-analysis)
- Systematic review and meta-analysis of 24 references (155 cases) of tibialis anterior tendon rupture
- Rupture is rare and most often spontaneous in patients over 45; diagnosis is often delayed because the long extensors compensate
- Surgery had a far better chance of a good outcome than conservative management (OR 8.40 vs 0.68)
- Best results with split/turn-down tibialis anterior graft, semitendinosus autograft, or direct repair; EHL autograft had the worst outcomes
Operative Treatment of TA Rupture (Objective Outcomes)
- Ten operatively treated tibialis anterior tendon ruptures (traumatic and spontaneous), with isokinetic testing
- Mean AOFAS Ankle-Hindfoot score improved from 71.9 to 89.8; all patients were satisfied and would repeat surgery
- Objective dorsiflexion and inversion strength remained lower than the uninjured side
- No significant difference between direct repair and repair with augmentation
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old reports a few months of catching the toes and a slapping gait, with a lump at the front of the ankle. There is no back or leg pain and sensation is normal. How do you assess and manage this?”
Guidelines, Registries & Global Practice
Global Practice Picture
Tibialis anterior tendon rupture is rare, so practice is guided by systematic reviews and case series rather than registries. Internationally consistent principles: think of it in any older patient with a spontaneous, painless drop foot; distinguish it from neurological foot drop by palpating the tendon and excluding sensory/myotomal deficits; manage by patient demand (AFO vs surgery); and, when operating, prefer direct repair or a tibialis-anterior/semitendinosus graft over an EHL autograft.
Side-by-Side Synthesis
- Tibialis anterior rupture
- Absent/lax + pseudotumour
- Neurological foot drop
- Intact/palpable
- Tibialis anterior rupture
- Normal
- Neurological foot drop
- Often abnormal (dorsum/L5)
- Tibialis anterior rupture
- Normal
- Neurological foot drop
- Weak (common peroneal)
- Tibialis anterior rupture
- Normal
- Neurological foot drop
- May be abnormal (L5/S1)
- Tibialis anterior rupture
- Demand-based (AFO vs repair/graft)
- Neurological foot drop
- Treat the nerve cause
Key Facts
- Rare; spontaneous in patients over 45
- TA = main dorsiflexor + invertor
- Often missed (EHL/EDL compensate)
- Anterior-ankle pseudotumour
Diagnosis
- Palpate the tendon (absent/lax)
- No sensory deficit / normal reflexes
- Exclude common peroneal palsy & L5
- Confirm with US/MRI
Management
- Low demand: AFO
- Active: direct repair or graft
- Graft: split-TA / semitendinosus (avoid EHL)
- Counsel: mild residual weakness common