Primary Dorsiflexor Rupture
- Anterior ankle mass with palpable gap + preserved toe extension = TA rupture
- Acute (less than 4 weeks) with gap less than 3cm: primary repair
- Chronic or gap greater than 3cm: EHL transfer reconstruction
- Always fuse/tenodese hallux IP joint with EHL transfer
- “Distinguish from L5 radiculopathy (weak EHL) and peroneal palsy (weak eversion)
- “EDL compensation masks diagnosis - always test heel walking
- “8 weeks immobilization minimum to prevent re-rupture
1. TA Rupture: Anterior mass + Slap foot + Toe Extension Intact. 2. L5 Radiculopathy: Foot drop + EHL Weakness + Sensory changes. 3. Peroneal Nerve: Foot drop + Eversion Weakness + 1st web space numb.
EDL Compensation: Patients can still dorsiflex using extensors/peroneals, but cannot heel walk. Always test heel walking.
Loss of Eccentric Control: Leads to 'Slap Foot' at heel strike. Swing Phase: High steppage to clear toes.
Acute (less than 4wk): Repair. Chronic: EHL Transfer (most common).
Overview
Anterior Tibial Tendon Rupture
Anterior tibial tendon (ATT) rupture is an uncommon but significant injury affecting the primary dorsiflexor of the foot. It may be acute (traumatic) or chronic (degenerative), with distinct presentations and management strategies.
Key Features:
- Third most common lower limb tendon rupture (after Achilles and patellar)
- Often misdiagnosed initially (up to 25% delayed diagnosis)
- Typically affects older patients (greater than 45 years) with degenerative ruptures
- Acute ruptures occur in younger, active patients
- Surgical repair generally recommended for active patients
Mechanisms of Rupture
Anterior tibial tendon rupture occurs through degenerative and traumatic mechanisms affecting a hypovascular zone.
Degenerative Rupture (Most Common)
- Age-related tendinosis: Collagen degeneration with mucoid changes
- Hypovascular zone: Reduced blood supply beneath extensor retinaculum
- Mechanical wear: Repetitive friction against superior extensor retinaculum
- Tibial osteophytes: Inferior anterior tibial lip spurs causing mechanical attrition
- Systemic factors: Diabetes, inflammatory arthropathy, fluoroquinolone use
- Steroid injections: Previous local corticosteroid may predispose to rupture
Traumatic Rupture
- Laceration: Direct penetrating injury to anterior ankle
- Forced plantarflexion: Eccentric loading during fall or stumble
- Avulsion injury: Sudden forceful dorsiflexion against resistance
- Iatrogenic: Surgical injury during ankle arthroscopy or anterior ankle procedures
- Ankle fracture-dislocation: High-energy trauma with tendon disruption
Chronic Attrition
The combination of intrinsic and extrinsic factors leads to gradual tendon failure:
- Intrinsic factors: Tendon degeneration, age greater than 45 years, hypovascular zone
- Extrinsic factors: Retinacular stenosis, tibial osteophytes, tight footwear
- Inflammatory conditions: Rheumatoid arthritis, seronegative spondyloarthropathy, gout
- Metabolic disorders: Diabetes mellitus, renal failure, hypercholesterolemia
Rupture Classification
- timing
- Less than 4 weeks from injury
- tendonQuality
- Usually good quality ends
- gapSize
- Variable, often less than 3 cm
- surgicalOptions
- Primary repair usually feasible
- timing
- Greater than 4 weeks from injury
- tendonQuality
- Degenerated ends, muscle retraction
- gapSize
- Often greater than 3 cm
- surgicalOptions
- Reconstruction required (transfer or graft)
- timing
- Variable onset, progressive symptoms
- tendonQuality
- Intact fibers with intratendinous split
- gapSize
- Not applicable
- surgicalOptions
- Debridement and repair if greater than 50%
- timing
- Acute traumatic event
- tendonQuality
- Good tendon with bone fragment
- gapSize
- Minimal if bone fixation immediate
- surgicalOptions
- Bone reattachment with suture anchors
RUPTUREDRisk Factors for TA Tendon Rupture
Hook:What gets RUPTURED? The TA tendon in these scenarios
Surgical Indications and Timing
Surgery is the preferred treatment for most patients with complete TA tendon rupture.
Indications for Surgery
- Complete acute rupture: Less than 4 weeks old in active patients
- Symptomatic chronic rupture: Functional impairment despite conservative trial
- Young active patients: Desire for optimal functional restoration
- Failed conservative management: Progressive symptoms or inadequate compensation
- Large partial tears: Greater than 50% cross-sectional involvement
- Occupational requirement: Jobs requiring normal ankle dorsiflexion
Timing Considerations
- Acute ruptures (less than 4 weeks): Primary repair often feasible
- Subacute ruptures (4-12 weeks): May require augmentation or short reconstruction
- Chronic ruptures (greater than 12 weeks): Reconstruction with tendon transfer or allograft
- Emergency surgery: Not required unless open injury with contamination
Pre-Operative Planning
- MRI review: Assess gap size, tendon quality, muscle status
- Surgical approach selection: Based on rupture location and chronicity
- Reconstruction strategy: Primary repair vs. augmentation vs. reconstruction
- Graft/transfer planning: Identify donor tendon or arrange allograft
- Patient counseling: Realistic expectations for recovery timeline (6-12 months)
Tibialis Anterior Tendon Anatomy
The tibialis anterior is the primary ankle dorsiflexor with critical function during gait cycle.
Origin and Course
- Origin: Lateral tibial condyle, proximal two-thirds lateral tibial shaft, interosseous membrane, deep fascia
- Muscle belly: Largest and most medial of anterior compartment muscles
- Myotendinous junction: Junction occurs 5-7 cm proximal to ankle joint
- Tendon course: Crosses ankle joint beneath extensor retinaculum in medial-most tunnel
- Insertion: Medial and plantar aspect of medial cuneiform and base of first metatarsal
- Tendon width: Approximately 10-15 mm at insertion, thickest of ankle tendons
Vascular Anatomy
- Proximal blood supply: Anterior tibial artery branches to muscle belly
- Intratendinous vascularity: Longitudinal vessels within tendon substance
- Zone of hypovascularity: Beneath extensor retinaculum where rupture typically occurs
- Distal blood supply: Branches from dorsalis pedis near insertion
- Watershed zone: 2-3 cm proximal to insertion with reduced perfusion
Retinacular Anatomy
Superior, inferior, and stem components of extensor retinaculum constrain ankle tendons. Separate compartments for TA, EHL, EDL, and peroneals beneath retinaculum. TA occupies most medial tunnel beneath extensor retinaculum, susceptible to stenosis.
Biomechanical Function
- Primary dorsiflexor: Accounts for 80% of ankle dorsiflexion strength
- Gait importance: Essential for heel strike and toe clearance during swing phase
- Supination force: Secondary function as hindfoot invertor (synergist with TP)
- Arch support: Contributes to medial longitudinal arch stability
- Load tolerance: Can generate forces up to 3-4 times body weight
- Excursion: Approximately 25-30 mm of tendon excursion with full ankle motion
Anatomy
Tibialis Anterior Tendon Anatomy
- Lateral tibial condyle
- Upper 2/3 lateral tibial surface
- Interosseous membrane
- Deep fascia
- Most medial tendon in anterior compartment
- Passes under superior extensor retinaculum
- Passes under inferior extensor retinaculum (Y-shaped)
- Crosses ankle joint anteriorly
- Medial cuneiform (plantar and medial surfaces)
- Base of first metatarsal
- Wide footprint: 10-15mm
- Lateral: EHL tendon, deep peroneal nerve, anterior tibial artery
- Medial: saphenous vein and nerve (more proximal)
Classification
Classification by Acuity
- Timing
- less than 6 weeks
- Characteristics
- Clear injury event, definable tendon ends
- Timing
- 6-12 weeks
- Characteristics
- Delayed presentation, some retraction
- Timing
- greater than 12 weeks
- Characteristics
- Significant retraction, often degenerative
Clinical Implications:
- Acute: Primary repair often feasible
- Subacute: Repair possible but may need augmentation
- Chronic: Usually requires reconstruction (graft or transfer)
History and Symptoms
The clinical presentation varies based on acuity and degree of rupture.
Acute Rupture
- Sudden onset pain: Sharp anterior ankle pain during specific event
- Popping sensation: Audible or palpable snap at time of injury
- Immediate weakness: Inability to dorsiflex ankle or walk on heels
- Anterior ankle swelling: Visible mass from rolled-up proximal tendon stump
- Activity recall: Often occurs during plantar flexion against resistance
Chronic Rupture
- Gradual weakness: Progressive difficulty with stairs and inclines
- Slap foot gait: Foot slaps down after heel strike due to loss of eccentric control
- Toe catching: Stumbling over ground irregularities from reduced clearance
- Compensatory fatigue: EDL overuse causing anterior shin discomfort
- Delayed presentation: Often misdiagnosed as sprain or neuropathy
Functional Deficits
- Heel walking impossible: Cannot walk on heels due to absent dorsiflexion strength
- Stair difficulties: Ascending stairs requires hip and knee compensation
- Gait abnormalities: Steppage gait or circumduction to clear foot
- Running impairment: Cannot run due to loss of push-off control
- Footwear problems: Difficulty donning shoes from weak dorsiflexion
Physical Examination
Systematic examination confirms the diagnosis and assesses compensatory mechanisms.
Inspection
- Anterior ankle mass: Bulge from retracted proximal tendon stump
- Palpable gap: Defect palpable distal to extensor retinaculum
- Muscle atrophy: TA muscle wasting in chronic cases (rare due to intramuscular tear pattern)
- Gait observation: Slap foot or steppage pattern
- Toe clawing: Compensatory EDL overactivity causing toe hyperextension
Palpation
- Tendon continuity: Gap palpable 2-4 cm above insertion typically
- Rolled tendon: Proximal stump palpable as firm mass
- Point tenderness: Local pain at rupture site in acute injuries
- Distal stump: Thin or absent tendon palpable distally
Functional Testing
Ankle dorsiflexion strength typically grade 0-1 with complete rupture despite EDL compensation. Partial tears or chronic compensated ruptures may demonstrate grade 2-3 strength from EDL. Normal or increased toe extension from compensatory EDL overactivity.
Specific tests:
- Resisted dorsiflexion: Severe weakness or absent function with resistance
- Heel walking: Inability to walk on heels (pathognomonic for TA dysfunction)
- Toe dorsiflexion: Preserved or enhanced from EDL compensation
- Passive plantarflexion: May reproduce pain at rupture site if acute
- Thompson test analogue: Squeezing TA belly does not produce dorsiflexion
Differential Diagnosis Testing
- L5 radiculopathy: Check EHL strength (should be normal in isolated TA rupture)
- Common peroneal nerve: Assess ankle eversion (should be normal)
- Deep peroneal nerve: Test sensation first web space (should be intact)
- Compartment syndrome: Assess for firmness and pain with passive stretch (absent in isolated rupture)
Differential Diagnosis of Foot Drop
The single most examinable concept is separating a mechanical (tendon) cause from a neurological one. Isolated TA rupture is the only common cause with weak dorsiflexion BUT preserved toe extension and a palpable anterior mass.
- dorsiflexion
- Weak/absent (cannot heel walk)
- toeExtension
- PRESERVED (EHL/EDL intact)
- eversion
- Normal
- sensation
- Normal
- discriminator
- Palpable anterior ankle mass + distal gap; reverse Thompson negative
- dorsiflexion
- Weak/absent
- toeExtension
- Weak (EHL and EDL affected)
- eversion
- WEAK (peroneals affected)
- sensation
- Reduced lateral leg/dorsum foot
- discriminator
- Tinel at fibular neck; weak eversion is the key separator
- dorsiflexion
- Weak/absent
- toeExtension
- Weak (EHL/EDL)
- eversion
- Normal (superficial peroneal spared)
- sensation
- First web space numbness only
- discriminator
- Eversion preserved but toe extension weak - opposite of TA rupture
- dorsiflexion
- Weak
- toeExtension
- WEAK (EHL is the L5 sentinel)
- eversion
- Often weak
- sensation
- L5 dermatome (lateral leg, dorsum, hallux)
- discriminator
- Back/radicular pain, positive straight-leg raise, weak EHL and hip abduction
- dorsiflexion
- Weak (muscle ischaemia/contracture)
- toeExtension
- Weak
- eversion
- Variable
- sensation
- First web space (deep peroneal nerve)
- discriminator
- History of acute pain/swelling; pain on passive stretch acutely, fixed contracture late
The key clinical finding is a palpable anterior ankle mass with a distal gap, combined with inability to heel walk despite preserved toe dorsiflexion. This triad distinguishes TA rupture from neurological causes of foot drop. The "reverse Thompson test" (squeezing TA muscle belly produces no ankle dorsiflexion) confirms the diagnosis.
Imaging Studies
Imaging confirms the clinical diagnosis and guides treatment planning.
Radiographs
Views: Weight-bearing AP, lateral, and oblique foot-ankle
Findings:
- Usually normal in acute ruptures
- Chronic cases may show:
- Anterior distal tibial osteophytes (site of mechanical attrition)
- Soft tissue swelling or calcification anterior ankle
- First ray elevation from loss of plantarflexion force
- Arthritic changes if inflammatory etiology
- Avulsion fracture at cuneiform or first metatarsal base (rare)
Ultrasound
Advantages: Dynamic assessment, real-time evaluation, cost-effective
Technique:
- High-frequency linear probe (10-15 MHz)
- Long-axis and short-axis imaging of entire tendon
- Compare to contralateral side
- Dynamic testing with active dorsiflexion
Findings:
- Complete tendon discontinuity with gap
- Hypoechoic or anechoic rupture site
- Proximal tendon retraction and thickening
- Hematoma or fluid in gap
- Measure gap size (critical for surgical planning)
- Partial tears show incomplete fiber disruption
MRI
Protocol: Ankle-foot protocol with T1, T2, STIR sequences in axial, sagittal, and coronal planes
Indications:
- Uncertain diagnosis
- Pre-operative planning
- Assessment of chronic ruptures
- Evaluation of tendon quality
- Identify associated pathology
Key findings:
- acute
- Complete disruption with wavy retracted ends
- chronic
- Wide gap with muscle retraction and fatty infiltration
- significance
- Determines feasibility of primary repair
- acute
- Typically 1-3 cm, measured in neutral position
- chronic
- Often greater than 4 cm with maximal plantarflexion
- significance
- Gap greater than 3 cm requires reconstruction
- acute
- Normal signal in proximal/distal stumps
- chronic
- Degenerated stumps with increased T2 signal
- significance
- Poor quality precludes primary repair
- acute
- Normal muscle bulk and signal
- chronic
- Atrophy and fatty infiltration of TA muscle
- significance
- Severe atrophy indicates poor functional recovery potential
- acute
- Intact but may show fluid/edema
- chronic
- Thickened with scarring and adhesions
- significance
- Chronic stenosis contributes to rupture
Advanced Imaging
- CT scan: Rarely needed, may help identify bony pathology
- Nerve conduction studies: If suspicion of neurological cause for foot drop
- EMG: Distinguish denervation from tendon rupture in unclear cases
GAPSMRI Findings in TA Tendon Rupture
Hook:MRI shows GAPS in ruptured TA tendon
Management Algorithm
Non-operative management is reserved for specific patient populations with acceptable functional compensation.
Indications
- Sedentary elderly patients: Minimal functional demands, acceptable gait with EDL compensation
- Severe medical comorbidities: Prohibitive surgical risk
- Patient preference: Informed decision declining surgery despite deficits
- Partial tears: Less than 50% cross-sectional area involved with good strength
- Chronic ruptures with good compensation: Well-adapted gait with minimal disability
Contraindications to Conservative Care
- Young active patients requiring normal gait mechanics
- Inability to compensate with EDL (weak toe extension)
- Progressive deformity or gait deterioration
- Patient desire for optimal functional restoration
- Occupation requiring normal dorsiflexion (e.g., driving, climbing)
Non-Operative Protocol
Phase 1 (0-6 weeks): Protection and adaptation
- AFO (ankle-foot orthosis): Articulated or fixed AFO to assist dorsiflexion
- Immobilization: Short leg cast or boot if acute and painful
- Weight-bearing: As tolerated with assistive device if needed
- Pain management: NSAIDs, ice, elevation for acute symptoms
Phase 2 (6-12 weeks): Functional adaptation
- Gait training: Compensatory strategies using EDL and hip flexors
- Strengthening: EDL and peroneals to optimize compensation
- Proprioception: Balance training to reduce fall risk
- Orthotic refinement: Adjust AFO for optimal function
Phase 3 (3-6 months): Long-term management
- Permanent AFO: Custom molded articulated AFO for daily use
- Footwear modification: Rocker bottom sole to assist heel-toe transition
- Activity modification: Avoid activities requiring heel walking or dorsiflexion
- Surveillance: Monitor for progressive deformity or gait dysfunction
Outcomes of Conservative Treatment
- Function: Acceptable for low-demand activities, limited for sports
- Gait: Persistent abnormality with slap foot or steppage pattern
- Satisfaction: Variable, depends on functional demands and expectations
- Complications: Chronic ankle pain, ankle stiffness, falls from tripping
- Long-term: May develop secondary issues (back pain from gait asymmetry)
Non-operative management of complete TA tendon rupture results in permanent functional deficit. AFO is required indefinitely for optimal gait. This approach should only be chosen after thorough discussion of limitations and with appropriate patient selection (elderly, sedentary, high surgical risk).
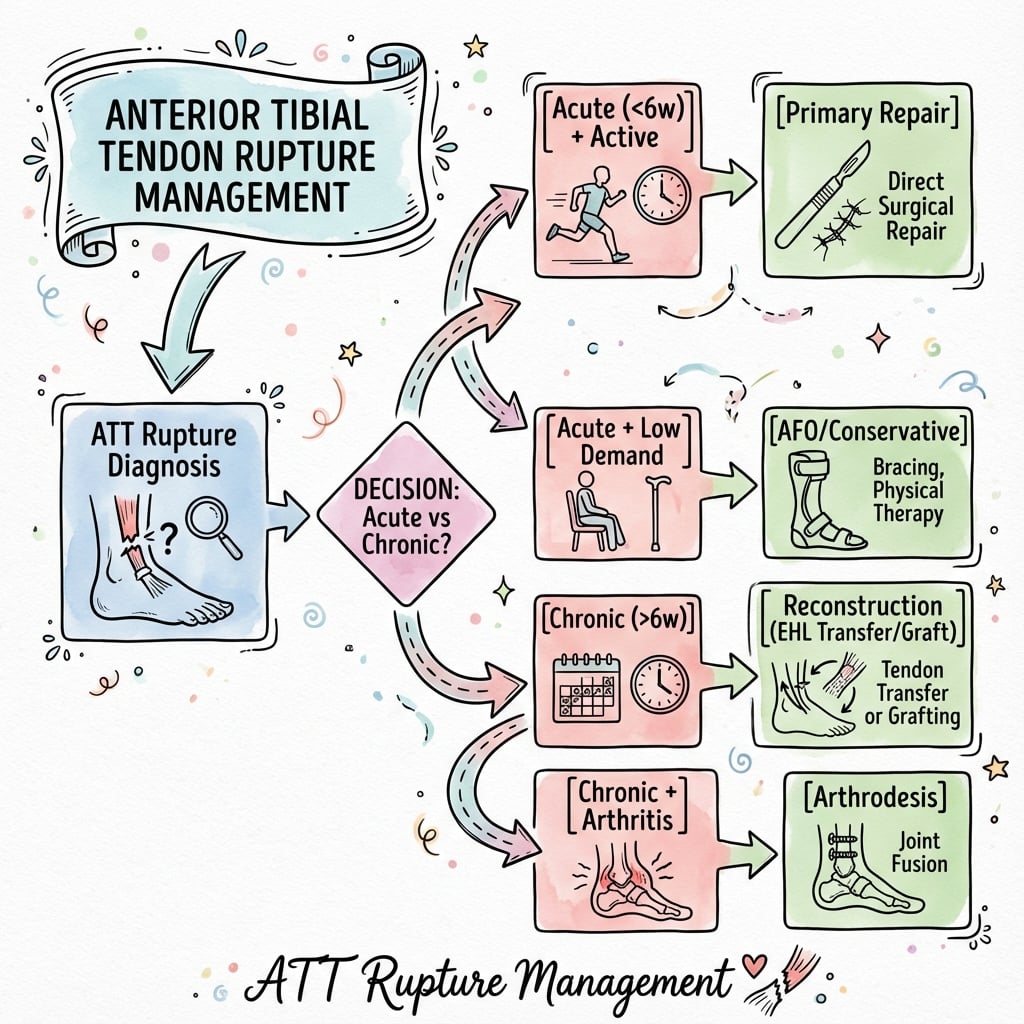
Management Algorithm
Treatment Algorithm
- Acute (less than 6 weeks)
- Primary repair
- Chronic (greater than 12 weeks)
- Reconstruction (EHL transfer or graft)
- Acute (less than 6 weeks)
- Primary repair ± augmentation
- Chronic (greater than 12 weeks)
- Reconstruction
- Acute (less than 6 weeks)
- Conservative trial
- Chronic (greater than 12 weeks)
- Conservative (AFO)
- Acute (less than 6 weeks)
- Conservative
- Chronic (greater than 12 weeks)
- Conservative
Decision Points:
- Gap size: less than 3cm = repair; greater than 3cm = reconstruction
- Tendon quality: Good = repair; Poor/degenerative = augment or reconstruct
- Muscle status: Minimal atrophy = repair; Severe atrophy = consider conservative
- Patient goals: High function = surgery; Minimal demands = conservative
Surgical Techniques
End-to-End Tendon Repair
Indications:
- Acute rupture (less than 4 weeks)
- Gap less than 3 cm with ankle in plantarflexion
- Good quality tendon ends
- No significant muscle retraction
Patient Positioning:
- Supine with bump under ipsilateral hip
- Thigh tourniquet (250-300 mmHg)
- Ensure foot mobile for intraoperative positioning
Surgical Approach:
- Longitudinal incision over anterior ankle (8-12 cm)
- Center over palpable gap or TA tendon course
- Incise skin and subcutaneous tissue
- Identify and protect superficial peroneal nerve branches
- Open extensor retinaculum along medial border
Tendon Preparation:
- Identify proximal and distal tendon stumps
- Debride degenerated or frayed tissue to healthy tendon
- Freshen ends with sharp blade (perpendicular cuts)
- Assess gap with ankle in maximal plantarflexion
- If gap greater than 3 cm, consider augmentation or reconstruction
Repair Technique:
- Krackow suture configuration: Locking stitches in each stump
- Suture material: Non-absorbable braided (FiberWire, Ethibond) size 2 or 0
- Core suture: 4-6 strand repair for optimal strength
- Tensioning: Repair with ankle in 10-15 degrees plantarflexion
- Epitendinous suture: Running 4-0 absorbable to smooth repair site
- Test repair: Ensure intact with passive ankle dorsiflexion to neutral
Augmentation Options (if tension on repair):
- Turndown flap: Proximally based TA tendon flap to bridge gap
- EHL transfer: Add EHL as side-to-side augmentation
- Plantaris graft: Harvest plantaris for interpositional graft
- EDL transfer: Transfer central EDL slip for reinforcement
Retinaculum Management:
- Excise portion of superior retinaculum to decompress repair
- Avoid complete retinaculum excision (prevents bowstringing)
- Ensure tendon glides smoothly beneath retinaculum
Closure:
- Close retinaculum loosely if intact
- Subcutaneous layer with 3-0 absorbable suture
- Skin closure with 4-0 nylon or staples
- Apply soft dressing and posterior splint in 10-15 degrees plantarflexion
Post-Operative Protocol:
- 0-2 weeks: NWB in posterior splint, plantarflexed position
- 2-6 weeks: NWB in cast or boot, gradual bring to neutral by week 6
- 6-8 weeks: Begin PWB in neutral boot, gentle AROM exercises
- 8-12 weeks: Progress to FWB, weaning from boot, start strengthening
- 3-6 months: Gradual return to activities, continue rehabilitation
- 6-12 months: Full recovery expected with return to impact activities
The superficial peroneal nerve crosses the anterior ankle and is at risk during exposure. Identify and protect throughout procedure. Excessive tension on the repair increases failure risk - if gap greater than 3 cm even in plantarflexion, consider augmentation or reconstruction rather than tensioned primary repair.
Bridging the Gap: Turn-Down Flap and Lengthening
The topic's own strongest evidence (Tickner 2019) found the split/turn-down ipsilateral tibialis anterior graft gave the BEST surgical outcome (OR 32.15) - better than any transfer or allograft - yet the body only names a "turndown flap" in one line and mentions "Z-lengthening" in passing without describing either. These autologous techniques bridge a moderate gap using the patient's own proximal tibialis anterior, avoiding a tendon transfer or allograft.
- Turn-down flap. A proximally-based strip of the proximal TA tendon (raised from the healthy proximal stump) is flipped distally (180 degrees) and sutured into the distal stump or the medial cuneiform, extending the reach of the native tendon to span the defect. A split turn-down takes only part of the tendon width, leaving the remainder in continuity.
- V-Y (or Z) lengthening. Where retraction is modest, a V-Y advancement or Z-lengthening cut in the proximal muscle-tendon unit lets the tendon be drawn distally to reach the distal stump for a direct repair - useful for a gap that is just too wide for simple end-to-end apposition but where the tendon quality is otherwise good.
- When to use them. These suit an acute-to-subacute rupture with a moderate gap (roughly 3-5 cm) and good tendon quality - closing the defect with native tissue and no donor morbidity, which is why the pooled evidence ranks the turn-down graft so highly. A very large chronic gap with degenerate ends still needs a transfer or allograft.
Q: At surgery the gap is 4 cm even in maximal plantarflexion but the tendon is good quality - what native-tissue options bridge it? A: A turn-down (or split turn-down) flap - a proximally-based strip of the proximal TA tendon flipped 180 degrees distally to reach the distal stump/cuneiform - or a V-Y advancement / Z-lengthening of the proximal muscle-tendon unit to draw the tendon distally for a direct repair. Both use native tissue with no donor morbidity; the pooled meta-analysis (Tickner 2019) ranked the split/turn-down TA graft as the BEST reconstruction (OR 32.15). Reserve transfer/allograft for very large chronic gaps with degenerate ends.
Surgical Complications
Understanding and preventing complications is essential for optimal outcomes.
Intraoperative Complications
- Neurovascular injury: Superficial peroneal nerve (2-3%), anterior tibial artery (rare)
- Deep peroneal nerve: At risk with deep dissection, causes first web space numbness
- Inadequate gap closure: Excessive tension on repair leading to early failure
- Incorrect tension: Over-tight (equinus contracture) or under-tight (weak dorsiflexion)
- Donor site injury: EHL laceration during harvest, hallux devascularization (rare)
Early Post-Operative Complications
- incidence
- 5-8%, higher in diabetics
- presentation
- Delayed healing, dehiscence, superficial infection
- management
- Local wound care, oral antibiotics, revision closure if severe
- incidence
- 4-6% overall, higher with primary repair of chronic ruptures
- presentation
- Acute pain, loss of dorsiflexion, palpable gap recurs
- management
- Revision surgery with reconstruction (EHL transfer or allograft)
- incidence
- Less than 1% with prophylaxis
- presentation
- Calf swelling, positive D-dimer, PE symptoms
- management
- Anticoagulation, may require admission for PE
- incidence
- Rare (less than 0.5%)
- presentation
- Severe pain, tense leg, pain with passive stretch
- management
- Emergency fasciotomy if confirmed by pressure measurement
Late Complications
- Persistent weakness: Incomplete strength recovery, more common with reconstructions
- Ankle stiffness: Limited dorsiflexion from prolonged immobilization or adhesions
- Hallux deformity: Cock-up hallux after EHL transfer without IP fusion/tenodesis
- Gait abnormalities: Persistent slap foot or steppage despite intact repair
- Chronic pain: Anterior ankle pain from adhesions, nerve injury, or arthrofibrosis
- Tendon adhesions: Scarring to retinaculum limiting gliding
- Equinus contracture: From excessive plantarflexion during immobilization
Specific Complication Management
Re-Rupture:
- Diagnosis: Clinical examination, ultrasound or MRI confirmation
- Timing: Usually within first 3 months post-operatively
- Causes: Excessive tension, premature weight-bearing, poor tendon quality
- Management: Revision surgery with reconstruction (EHL transfer preferred)
- Prevention: Adequate immobilization (8 weeks minimum), appropriate tension, patient compliance
Persistent Weakness:
- Evaluation: Compare to contralateral ankle dorsiflexion strength
- Acceptable: 70-80% strength after EHL transfer, 90%+ after primary repair
- Causes: Muscle atrophy, incomplete healing, adhesions, inadequate rehabilitation
- Management: Prolonged physiotherapy (6-12 months), AFO if severe
- Consider: Revision surgery if less than 50% strength and daily impairment
Nerve Injury:
- Superficial peroneal nerve: Numbness dorsum of foot, usually resolves 3-6 months
- Deep peroneal nerve: First web space numbness, persistent but not functionally limiting
- Painful neuroma: Rare, may require neuroma excision or nerve decompression
- Prevention: Careful dissection, protect nerve branches throughout
The most significant complication is re-rupture, which occurs in 4-6% of cases. Risk factors include chronic ruptures treated with primary repair under tension, inadequate immobilization duration, and premature return to activities. Ensure 8 weeks of strict immobilization and gradual progression through rehabilitation phases to minimize risk.
Multicentre Cohort: Acute vs Delayed Surgical Repair
- Prospective multicentre cohort of 48 surgically treated tibialis anterior ruptures across 4 foot-and-ankle units (Level II)
- Most ruptures occurred at the distal avascular 5-30 mm of the tendon from degenerative change
- No significant difference in VAS-FA patient-reported outcome between acute and delayed (chronic) repair
- Chronic ruptures had significantly higher pre-operative VAS-FA (more symptomatic) than non-traumatic ruptures
- Counter-intuitively, younger patients rated outcomes more critically ('fair') than older patients
Complications
Early Complications (0-6 weeks)
- Incidence
- 3-8%
- Management
- Oral/IV antibiotics, debridement if deep
- Incidence
- 2-5%
- Management
- Dressings, secondary closure, skin graft
- Incidence
- 5-10%
- Management
- Observation (usually transient)
- Incidence
- less than 1%
- Management
- Prophylaxis, treatment anticoagulation
- Incidence
- 2-3%
- Management
- Aspiration or evacuation
Wound Problems:
- Higher risk in chronic ruptures with poor tissue
- Diabetes and PVD increase risk
- Careful tissue handling essential
Recovery Timeline and Expectations
Understanding the prolonged recovery process is essential for patient counseling.
Rehabilitation Phases
Immobilization in plantarflexion gradually brought to neutral. Non-weight bearing progressing to partial weight bearing.
Active range of motion, progressive weight bearing, gait normalization. Begin gentle strengthening.
Progressive resistance exercises, proprioception training, functional activities. Return to low-impact activities.
Sport-specific training, gradual return to full activities. Complete recovery expected by 12 months.
Functional Outcomes
- primaryRepair
- Normal gait by 3-4 months
- ehlTransfer
- Normal gait by 4-6 months
- nonOperative
- Permanent slap foot gait, AFO dependent
- primaryRepair
- Full function by 4-6 months
- ehlTransfer
- Near-normal by 6-9 months
- nonOperative
- Permanent difficulty, uses handrail
- primaryRepair
- Return to running 6-9 months
- ehlTransfer
- Return to running 9-12 months
- nonOperative
- Usually not possible
- primaryRepair
- Full return 9-12 months, 90% performance
- ehlTransfer
- Most sports 12+ months, 75-85% performance
- nonOperative
- High-impact sports not feasible
Strength Recovery
- Primary repair: 90-100% contralateral strength if successful
- EHL transfer: 70-80% contralateral strength (functionally adequate)
- EDL transfer: 60-70% contralateral strength (may limit high-level sports)
- Allograft: 70-85% strength once fully incorporated (12-18 months)
- Non-operative: 20-30% strength from EDL compensation alone
Patient Satisfaction
Studies report high satisfaction rates across surgical interventions:
- Primary repair: 90-95% satisfied with outcome
- EHL transfer: 85-90% satisfied despite some weakness
- Revision surgery: 70-80% satisfied (lower due to complications/reoperations)
- Non-operative: 40-60% satisfied, limited by persistent functional deficits
Return to Work
- Sedentary work: 6-8 weeks with protected weight-bearing
- Light duty: 12-16 weeks with gradual transition
- Heavy labor: 6-9 months minimum, may require job modification
- Driving: Right foot 3-4 months once off immobilization and adequate strength
Prognostic Factors
Favorable outcomes:
- Acute rupture (less than 4 weeks) treated with primary repair
- Good quality tendon and muscle
- Young patient with good rehabilitation compliance
- Non-smoking, non-diabetic, healthy weight
- Appropriate surgical technique and post-operative protocol
Poor prognostic factors:
- Chronic rupture (greater than 6 months) with muscle atrophy
- Failed prior surgery
- Diabetes, smoking, obesity
- Poor compliance with immobilization or rehabilitation
- Inflammatory arthropathy affecting healing
Interpositional Allograft for Chronic Irreparable Ruptures
- 11 patients with chronic tibialis anterior ruptures and large segmental defects treated with intercalary allograft
- Mean post-operative dorsiflexion strength 4.8/5; mean AOFAS Ankle-Hindfoot score 84.3; mean VAS pain 0.8
- No infections, no reruptures, and no reoperations at mean 43.8 months
- Only complication was transient superficial peroneal nerve neuritis
- Avoids the donor-site morbidity of tendon transfer or autograft harvest
Outcomes
Functional Outcomes by Treatment
- Primary Repair
- 85-95
- EHL Transfer
- 80-90
- Non-operative
- 60-70
- Primary Repair
- 90-100%
- EHL Transfer
- 70-80%
- Non-operative
- 20-30%
- Primary Repair
- 95%
- EHL Transfer
- 85%
- Non-operative
- less than 50%
- Primary Repair
- 90-95%
- EHL Transfer
- 85-90%
- Non-operative
- 40-60%
- Primary Repair
- 85-90%
- EHL Transfer
- 70-80%
- Non-operative
- Limited
Timeline to Recovery:
- Normal walking: 3-4 months (repair), 4-6 months (transfer)
- Running: 6-9 months (repair), 9-12 months (transfer)
- Full sport: 9-12 months (repair), 12+ months (transfer)
Hamstring Autograft Reconstruction (Minimally Invasive)
- 8 patients reconstructed with hamstring (semitendinosus/gracilis) autograft via a minimally invasive approach
- Foot and Ankle Outcome Score, VAS and SF-12 all improved post-operatively
- Restored ankle range of motion and inversion strength; residual dorsiflexion strength deficits on isokinetic testing
- All patients ambulated without a brace, avoiding long-term bracing or local tendon sacrifice
Insertional Anatomy & Clinical Series (Cadaveric Study)
- Dissection of 53 feet defined three tibialis anterior insertion patterns
- Most common (36 feet): dual insertion onto medial cuneiform AND base of first metatarsal
- 13 feet inserted onto the medial cuneiform only; 4 had an accessory slip
- Three accompanying clinical cases: surgery advised for acute ruptures and high-demand patients; conservative care acceptable for chronic, low-demand patients
Narrative Review: Acute & Chronic TA Rupture and Tendinopathy
- Synthesises presentation, examination, non-operative and surgical options for tibialis anterior rupture
- Reinforces that diagnosis is frequently delayed because long extensors compensate for lost dorsiflexion
- Algorithm: tension-free direct repair for acute ruptures; reconstruction (transfer or graft) for chronic gaps
Cock-Up Hallux After EHL Transfer: Mechanism and Prevention
The topic repeatedly warns that an EHL transfer needs a hallux IP fusion or tenodesis to prevent a "cock-up hallux", and a viva followUp asks what happened when one develops - but the deformity's mechanism is never explained.
- Why it happens. The extensor hallucis longus is the hallux's only long extensor of the interphalangeal (IP) joint and a major MTP extensor. Harvesting and transferring it to the cuneiform removes active hallux extension. The unopposed flexor hallucis longus then flexes the IP joint while the MTP is pulled into hyperextension (by extensor digitorum brevis/intrinsics and the tented soft tissues) - the classic cock-up (MTP hyperextension plus IP flexion) deformity, which is painful, catches in shoes and weakens push-off.
- Prevention at the index operation. (1) First IP joint arthrodesis - the gold standard - fuses the IP so it cannot claw, and lets the transferred EHL power dorsiflexion without deforming the toe. (2) Tenodesis of the distal EHL stump to the extensor hallucis brevis or into the first metatarsal neck, preserving some MTP extension without an IP fusion (favoured in younger patients who want to keep IP motion). (3) In a low-demand elderly patient, simply accepting the loss of hallux extension is reasonable.
- Managing an established deformity. A symptomatic cock-up hallux after a transfer done without IP control is treated by a first IP arthrodesis (with MTP soft-tissue rebalancing as needed); a flexible early deformity may respond to a distal EHL-stump tenodesis.
Q: A year after an EHL transfer for TA rupture the hallux is developing a cock-up deformity - what happened and what are the options? A: The transfer removed the EHL's hallux extension, so the unopposed FHL flexes the IP while the MTP hyperextends - a cock-up (MTP hyperextension plus IP flexion) deformity. It is prevented at surgery by a first IP arthrodesis (gold standard) or a tenodesis of the distal EHL stump to the EHB / first metatarsal; an established symptomatic deformity is corrected by a first IP arthrodesis (with MTP rebalancing as needed).
Surgical vs Conservative Management: Systematic Review & Meta-Analysis
- 24 studies, 155 cases of isolated tibialis anterior tendon rupture pooled
- Surgery had markedly better odds of a good outcome (OR 8.40) than conservative care (OR 0.68)
- Best reconstructions: ipsilateral split/turn-down TA graft (OR 32.15), semitendinosus autograft (OR 15.25), direct repair (OR 12.57)
- Extensor hallucis longus (EHL) autograft was associated with the WORST outcomes (OR 0.27)
- Most common residual finding was mild dorsiflexion weakness (4/5) without subjective limitation; good results regardless of patient age
Guidelines, Registries & Global Practice
Global Epidemiology
- Value
- Rare; the third most common lower-limb tendon rupture after Achilles and patellar
- Notes
- Largely case-series and registry-absent literature
- Value
- 155 isolated ruptures across 24 studies (Tickner meta-analysis)
- Notes
- Reflects how uncommon the injury is worldwide
- Value
- Bimodal: degenerative ruptures cluster at over 45 years (mean 60-70); traumatic in younger, active patients
- Notes
- Degenerative type predominates
- Value
- Male predominance approximately 3:1
- Notes
- Consistent across regions
- Value
- Distal avascular 5-30 mm of tendon beneath the extensor retinaculum
- Notes
- Confirmed in multicentre cohorts
Universal risk factors (region-independent): increasing age and tendinosis, diabetes mellitus, inflammatory arthropathy (RA, gout, seronegative spondyloarthropathy), local or systemic corticosteroid exposure, fluoroquinolone use, and chronic renal disease.
Practice variation - high vs limited resource settings:
- High-resource: ready access to MRI/ultrasound, foot-and-ankle subspecialists, allograft banks, and early reconstruction. Diagnosis still delayed in approximately 1 in 4 cases due to long-extensor compensation.
- Limited-resource / remote: greater reliance on clinical diagnosis and ultrasound; allograft and subspecialty transfer access restricted, so autograft transfer, direct repair, or definitive AFO management are proportionally more common. Delayed presentation is more frequent.
Controversies & Areas of Uncertainty
The rarity of this injury means much teaching rests on small case series and tradition rather than high-level evidence. Examiners reward candidates who can articulate where the genuine uncertainty lies.
Long taught as the default reconstruction, yet the largest pooled analysis (Tickner 2019) found EHL autograft had the worst outcomes (OR 0.27), favouring direct repair, turn-down or semitendinosus grafts. The discrepancy may reflect autograft-vs-in-situ-transfer technique. State the controversy rather than dogmatically quoting EHL.
No randomised data exist. Pooled observational evidence favours surgery in active patients, but well-compensated, low-demand or high-risk patients can do acceptably with an AFO. This is a shared-decision, not a fixed rule.
A multicentre cohort (Johansen 2020) found no significant outcome difference between acute and delayed repair when reconstruction was feasible - challenging the urgency often implied by the "4-week window".
The traditional 8 weeks of immobilisation and the 3 cm gap cut-off for repair-vs-reconstruct are conventions, not trial-derived. Accelerated rehab protocols are emerging but unproven in this tendon.
MCQ Practice Points
Q: What is the typical patient demographic and mechanism for anterior tibial tendon rupture?
A: Typically affects elderly patients (60-80 years) with spontaneous or low-energy rupture. Risk factors include: diabetes mellitus, inflammatory arthritis, corticosteroid use, and chronic tendinopathy. Often occurs with minor trauma (stumbling, missing a step) in a chronically weakened tendon. The zone of relative hypovascularity at the inferior extensor retinaculum is the most common rupture site.
Q: What are the clinical features of anterior tibial tendon rupture?
A: Gait abnormality: Steppage gait (high-stepping to clear foot) or slap gait (foot slaps during heel strike). Weakness: Unable to dorsiflex ankle against resistance. Palpable defect: Gap at the anterior ankle, though swelling may obscure this. Pseudotumor: Mass from retracted tendon stump may be palpable. Foot drop: Inability to clear foot during swing phase. Differential includes common peroneal nerve palsy (sensory changes, different weakness pattern).
Q: What are the surgical treatment options for anterior tibial tendon rupture?
A: Acute ruptures (less than 6 weeks): Primary repair with end-to-end suture if possible. Chronic ruptures: Often require augmentation due to tendon degeneration and gap. Options include: EHL transfer (extensor hallucis longus) - most common; Peroneus tertius transfer; Allograft reconstruction; Free gracilis/semitendinosus graft. The tendon is repaired through an anterior ankle incision, often requiring Z-lengthening.
Q: Why is EHL (extensor hallucis longus) the preferred tendon transfer for chronic anterior tibial tendon rupture?
A: EHL is preferred because: (1) Similar line of pull to tibialis anterior; (2) Adequate strength (approximately 80% of tibialis anterior); (3) Sufficient length for transfer; (4) Minimal donor morbidity - hallux IP joint extension loss is well-tolerated. Technique involves harvesting EHL distally, weaving through tibialis anterior stump, and anchoring to medial cuneiform/navicular with interference screw or suture anchors.
Q: What is the expected functional outcome after anterior tibial tendon repair or reconstruction?
A: Good to excellent outcomes in 80-90% of cases with surgical treatment. Most patients regain independent ambulation without orthotic support. Residual findings may include: Mild weakness of dorsiflexion (grade 4/5 power), altered gait pattern with reduced push-off, and prolonged rehabilitation (3-6 months). Non-operative treatment (AFO) is reserved for sedentary elderly patients with high surgical risk.
At a Glance
Anterior tibial tendon rupture is a rare injury typically affecting older males with degenerative tendinopathy, occurring at the hypovascular zone beneath the extensor retinaculum. Clinical features include an anterior ankle mass (retracted tendon), palpable gap, and slap foot gait with forefoot-first contact. Diagnosis is often delayed because EDL compensation masks the dorsiflexion weakness. Differential diagnosis includes peroneal nerve palsy and L5 radiculopathy—distinguish by intact toe extension (EHL, EDL) with isolated TA loss. MRI confirms rupture location and tendon quality. Acute complete ruptures (under 4 weeks) are managed with primary end-to-end repair if tension-free. Chronic or large gaps require reconstruction using EHL transfer (most common), EDL transfer, or allograft interposition. Post-operative immobilisation for 6-8 weeks is essential.
DISSTibialis Anterior Functions
Hook:TA tendon function? Don't DISS the dorsiflexor
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old recreational runner presents to your clinic 10 days after acute onset of anterior ankle pain while running downhill. He describes a pop and immediate weakness. Examination reveals a palpable anterior ankle mass, a gap 3 cm above the TA insertion, and inability to heel walk. MRI shows complete TA tendon rupture with 2.5 cm gap in neutral position and good quality tendon ends. He is otherwise healthy and wants to return to running.”
“A 68-year-old man presents with 9 months of progressive difficulty walking and frequent tripping. He cannot recall a specific injury. He was initially diagnosed with sciatica and had lumbar spine MRI which was unremarkable. On examination, he has weak ankle dorsiflexion (2/5) but normal toe extension (5/5). He can evert the ankle normally. There is a subtle anterior ankle fullness. Ankle sensation is intact. He ambulates with a steppage gait pattern. You order an MRI which shows complete TA tendon rupture with 5 cm gap, degenerated tendon ends, and moderate TA muscle atrophy with early fatty infiltration.”
“A 74-year-old man with type 2 diabetes (HbA1c 9.2%), peripheral neuropathy and a previous local corticosteroid injection to the anterior ankle 6 months ago presents with a 3-month history of progressive foot drop and tripping. Examination shows a palpable anterior ankle gap, dorsiflexion 1/5, intact toe extension, and dry neuropathic skin over the dorsum of the foot. He lives independently, walks his dog daily, and is anxious about surgery. MRI confirms a complete tibialis anterior rupture with a 4 cm gap and degenerate ends.”
Must-Know Anatomy
- TA: primary dorsiflexor, 80% of ankle dorsiflexion power
- Origin: lateral tibia, insertion: medial cuneiform and first MT base
- Hypovascular zone beneath extensor retinaculum - rupture site
- Superficial peroneal nerve crosses anterior ankle - protect during surgery
- Three retinacular bands constrain tendons - excise superior portion for decompression
Classic Presentation
- Elderly male, often spontaneous or minor trauma
- Anterior ankle mass (rolled-up tendon) with distal gap
- Unable to heel walk despite preserved toe extension (EHL intact)
- Slap foot gait - forefoot hits ground before heel
- Often misdiagnosed as sciatica or peroneal nerve palsy
Key Differentiation
- TA rupture: weak dorsiflexion, normal toe extension (EHL), palpable mass
- L5 radiculopathy: weak dorsiflexion AND weak EHL, radicular pain
- Peroneal nerve palsy: weak dorsiflexion AND eversion, foot numbness
- Compartment syndrome: tense leg, severe pain, pain with passive stretch
- Pseudoparalysis: pain limiting function, improves with anesthesia
Imaging Essentials
- MRI gold standard: confirms rupture, measures gap, assesses muscle/tendon quality
- Acute: gap less than 3 cm, good tendon quality, no muscle atrophy
- Chronic: gap greater than 4 cm, degenerated tendon, muscle atrophy/fatty infiltration
- Ultrasound: dynamic assessment, can diagnose acute ruptures
- XR: usually normal, may show tibial osteophytes in chronic cases
Treatment Algorithm
- Acute (less than 4 weeks) + gap less than 3 cm: primary Krackow repair
- Acute but gap greater than 3 cm: augment with EHL or turndown flap
- Chronic (greater than 4 weeks) or gap greater than 3 cm: EHL transfer reconstruction
- Severe muscle atrophy or revision: consider allograft or EDL transfer
- Non-operative: AFO only for sedentary elderly with high surgical risk
Surgical Pearls
- Primary repair: Krackow locking sutures, repair in 10-15 degrees plantarflexion
- EHL transfer: hallux IP fusion/tenodesis mandatory to prevent cock-up deformity
- Tension with ankle neutral dorsiflexion, slight hindfoot inversion
- Excise portion of superior retinaculum to decompress repair site
- Post-op: 8 weeks immobilization essential, NWB initially progressing by weeks
Viva Traps
- Primary repair under tension will fail - augment or reconstruct if gap greater than 3 cm
- EHL transfer achieves 70-80% strength NOT 100% - set realistic expectations
- Muscle atrophy greater than 50% predicts poor recovery even with surgery
- Return to running needs 6-9 months minimum, full recovery 12 months
- Re-rupture risk highest with inadequate immobilization or chronic rupture primary repair
Critical Numbers
- Gap less than 3 cm: primary repair feasible if acute and in plantarflexion
- 8 weeks: minimum immobilization duration to prevent re-rupture
- 70-80%: expected strength recovery with EHL transfer
- 90-95%: good-excellent results with appropriate surgery and patient selection
- 4-6%: re-rupture rate overall, higher with tensioned repairs
Evidence Base
Key Studies - Surgical Outcomes
- Design
- Systematic review & meta-analysis
- N
- 155
- Key Finding
- Surgery superior to conservative (OR 8.40); EHL autograft had the worst outcomes
- Design
- Prospective multicentre cohort
- N
- 48
- Key Finding
- No outcome difference between acute and delayed surgical repair
- Design
- Case series
- N
- 11
- Key Finding
- Interpositional allograft reliable for large chronic irreparable gaps
- Design
- Case series
- N
- 16
- Key Finding
- Early clinical series of tibialis anterior tendon rupture
Evidence Summary:
- Level IV evidence predominates (case series)
- No RCTs comparing surgical vs non-operative
- Consistent finding: surgery superior for active patients