Footballer's Ankle | Anterior Osteophytes
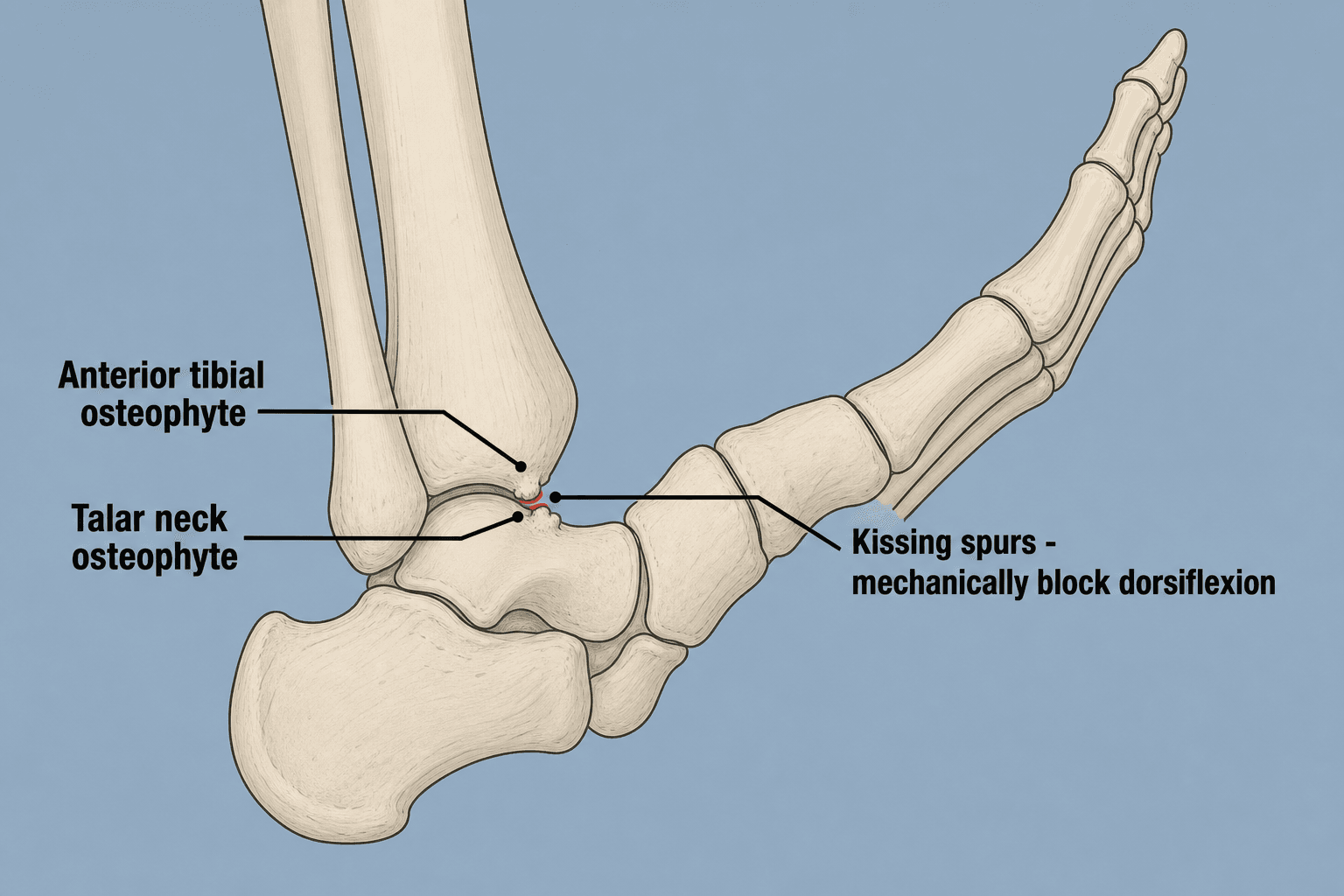
- Anterior tibial and talar osteophytes cause mechanical block
- Footballer's ankle = repeated dorsiflexion microtrauma
- Pain at end-range dorsiflexion is characteristic
- Lateral radiograph shows anterior spurs
- Arthroscopic debridement is treatment of choice
- “Kicking and forced-dorsiflexion sports (soccer, AFL, ballet)
- “Pain with kicking, squatting, stairs
- “Local anesthetic injection can confirm diagnosis
- “Outcome depends on joint-space preservation, not spur size
Repeated dorsiflexion causes microtrauma to anterior capsule and periosteum. Traction spurs develop on distal tibia and talar neck. These impinge at end-range dorsiflexion.
Anterior ankle pain at end-range dorsiflexion. Pain with squatting, stairs, kicking. Loss of dorsiflexion range. Tenderness at anterior joint line.
Lateral weight-bearing X-ray shows anterior tibial and talar spurs. CT quantifies size. MRI for soft tissue impingement. X-ray may underestimate extent.
Conservative: Activity modification, physiotherapy, injection. Surgical: Arthroscopic resection of osteophytes and soft tissue. Excellent outcomes.
SAFEArthroscopy Portal Safety
Hook:SAFE portals prevent nerve injury!
Overview
Anterior ankle impingement refers to pain and limited dorsiflexion caused by impingement of structures at the anterior ankle, typically bony spurs and/or hypertrophic soft tissue. It is also known as "footballer's ankle" due to its association with kicking sports.
Epidemiology
- Setting: a leading cause of chronic anterior ankle pain in athletes; common in kicking and forced-dorsiflexion sports
- Demographics: Peak incidence in athletes aged 20-35 years
- Sports: Soccer, Australian Rules football, ballet, basketball, gymnastics and rugby most commonly affected
- Sex distribution: Male predominance reflecting sports-participation patterns
- Antecedent injury: prior ankle sprain is common, particularly in the soft-tissue/anterolateral subtype
Classification (Scranton and McDermott)
- Description
- Synovial impingement only
- Treatment
- Conservative
- Description
- Osteophyte ≤3mm
- Treatment
- Conservative/Arthroscopy
- Description
- Osteophyte 3-5mm
- Treatment
- Arthroscopic debridement
- Description
- Osteophyte greater than 5mm or secondary arthritis
- Treatment
- Arthroscopic +/- open
Pathophysiology
Mechanism of Injury
Bony Impingement (Primary):
- Anterior tibial and dorsal talar-neck osteophytes ("kissing spurs") form at the joint margin and impinge at end-range dorsiflexion, producing mechanical block and pain
- Direct microtrauma (favoured theory): recurrent ball-strike and forced dorsiflexion drive repetitive intra-articular impact at the anteromedial joint margin, stimulating marginal osteophyte
- Capsular traction theory (now largely refuted): the classic teaching held that traction at the capsular insertion drives spur formation. Tol & van Dijk's cadaveric anatomical study showed the anterior capsule attaches several millimetres proximal to where spurs actually arise, so repetitive capsular traction does not plausibly explain spur location (PMID 15215021)
Soft Tissue Impingement (Secondary):
- Hypertrophic synovium or capsule, particularly after ankle sprains
- Bassett's lesion: Accessory fascicle of AITFL (anterior inferior tibiofibular ligament)
- Meniscoid lesions: Hypertrophic synovial folds trapped in joint
- Scar tissue from previous injury or surgery
Anatomical Considerations
Anterior Tibiotalar Recess:
- The anterior joint line is the most common site of pathology
- Space between tibial plafond and talar dome decreases with dorsiflexion
- Normal clearance of 3-5mm reduces to less than 1mm with maximal dorsiflexion
At-Risk Structures:
- Anterior tibial osteophyte (most common)
- Talar neck osteophyte
- Anterior joint capsule
- Extensor retinaculum
- Deep peroneal nerve and dorsalis pedis artery (surgical consideration)
Pathological Sequence
- Acute phase: Capsular stretch and periosteal reaction from repetitive microtrauma
- Inflammatory phase: Synovitis and capsular thickening
- Proliferative phase: Osteophyte formation at capsular insertions
- Chronic phase: Established osteophytes with secondary soft tissue changes
Anteromedial versus Anterolateral Impingement
The investigation section turns on the oblique AMI (anteromedial impingement) view, and the epidemiology flags a "soft-tissue/anterolateral subtype" — because anterior ankle impingement is really two subtypes that an examiner expects you to separate, since they differ in cause, the offending tissue and the imaging that reveals them.
- Anteromedial impingement
- Bony — anteromedial tibial and talar-neck osteophytes
- Anterolateral impingement
- Soft tissue — meniscoid lesion, gutter synovitis, hypertrophic distal AITFL fascicle (Bassett)
- Anteromedial impingement
- Repetitive forced dorsiflexion / kicking (footballer's ankle)
- Anterolateral impingement
- After a lateral (inversion) ankle sprain
- Anteromedial impingement
- Anteromedial spurs sit behind the anterolateral tibial rim on a true lateral — need the oblique AMI view
- Anterolateral impingement
- The soft-tissue lesion is invisible on plain film — needs MRI (or arthroscopy)
- Anteromedial impingement
- Anteromedial joint line
- Anterolateral impingement
- Anterolateral gutter
This is why the plain lateral radiograph misses so many lesions (sensitivity only about 40% tibial and 32% talar) and why the AMI view and MRI are each emphasised in Investigations — they target different subtypes. The two frequently coexist (combined impingement), and arthroscopic debridement addresses both: resect the bony spurs for the anteromedial pattern and excise the synovitis/meniscoid/Bassett fascicle for the anterolateral pattern. The broader family of ankle-impingement types is catalogued in the ankle-impingement-syndromes topic, and posterior (os trigonum) impingement is a separate entity in the posterior-ankle-impingement topic.
Q: A normal lateral radiograph in suspected anterior ankle impingement — what next, and why? A: It does not exclude impingement. If you suspect a bony anteromedial lesion, add the oblique AMI view (it unmasks anteromedial spurs hidden behind the anterolateral tibial rim); if you suspect a soft-tissue anterolateral lesion (post-sprain, Bassett/meniscoid), get an MRI. The lateral film alone is roughly 40% sensitive.
SPURAnterior Impingement Features
Hook:SPUR = Spurs cause Pain, worse Uphill, Resect arthroscopically!
KICKAnterior Impingement Exam Findings
Hook:KICK ball = anterior ankle pain - check with impingement test!
Clinical Presentation
History
Athletes, particularly footballers (soccer, Australian rules) and dancers, present with anterior ankle pain. Pain is worse with activities requiring dorsiflexion: squatting, going uphill, climbing stairs, kicking. There may be a history of previous ankle sprains. Patients note limitation of dorsiflexion compared to the other side.
Examination
Inspection:
- Mild anterior swelling may be visible
- Compare to contralateral ankle
- Note any previous surgical scars
Tenderness: At the anterior joint line, over the anterior tibiotalar joint. Palpate in slight plantarflexion to access anterior structures.
Dorsiflexion Limitation: Reduced compared to contralateral side. Measure with goniometer if available. End-range dorsiflexion reproduces pain.
Impingement Test: Passive forced dorsiflexion reproduces anterior pain. A positive test strongly suggests anterior impingement.
Squeeze Test: Assess syndesmosis by compressing fibula against tibia at mid-calf level. Pain suggests syndesmotic injury rather than pure anterior impingement.
Effusion: May have mild effusion. Palpate anterior recesses.
Exclude Instability: Check for lateral ligament laxity if history of sprains using anterior drawer test and talar tilt.
Investigations
Imaging Protocol
Plain Radiographs (First-line):
- Lateral weight-bearing: standard view for anterior tibial and talar-neck spurs, but sensitivity is poor for medially located lesions (lateral XR sensitivity only 40% tibial, 32% talar; PMID 14992704)
- Oblique anteromedial impingement (AMI) view: beam tilted 45° craniocaudal with leg in 30° external rotation. Adding the AMI view to the lateral raises sensitivity to 85% (tibial) and 73% (talar) by unmasking anteromedial spurs hidden behind the anterolateral tibial rim (PMID 11904689, 14992704). High-yield exam point
- AP mortise view: assess syndesmosis and joint-space narrowing (degenerative grade)
- Limitation: a normal lateral radiograph does NOT exclude impingement — order the oblique AMI view before calling imaging negative
CT Scan:
- Indications: Surgical planning, quantify osteophyte size and location
- Better 3D assessment of kissing osteophytes
- Identifies lateral and posteromedial spurs missed on X-ray
- Essential for large Grade III-IV lesions
MRI:
- Indications: Suspected soft tissue impingement, associated pathology
- T2-weighted sequences show synovitis, effusion, bone marrow edema
- Identifies Bassett's lesion (accessory AITFL fascicle)
- Detects meniscoid lesions and capsular thickening
- Evaluates for osteochondral lesions (OCL) of talus
Diagnostic Injection
Technique:
- Fluoroscopic or ultrasound-guided injection
- 2-3ml of local anesthetic (lidocaine/bupivacaine) into anterior recess
- Pain relief confirms diagnosis
- Can combine with steroid for therapeutic effect
Interpretation:
- Greater than 50% pain relief = positive diagnostic test
- Complete relief differentiates from other causes (OCD, arthritis)
- Duration of relief guides prognosis
Differential Diagnosis
- Key Distinguishing Features
- Deep joint pain, catching, MRI findings
- Key Distinguishing Features
- Global pain, weight-bearing symptoms
- Key Distinguishing Features
- Squeeze test positive, high ankle pain
- Key Distinguishing Features
- Lateral symptoms, peroneal provocation tests
- Key Distinguishing Features
- Subtalar instability, sinus tarsi tenderness
Management

Initial Conservative Management (Grade I-II)
Activity Modification:
- Avoid provocative activities (kicking, squatting, climbing)
- Temporary cessation of sport (2-4 weeks initially)
- May need to modify training or position
Pharmacological Management:
- NSAIDs for pain and inflammation (short course)
- Topical anti-inflammatory agents
Physiotherapy Protocol:
-
Phase 1 (Weeks 1-2): Reduce inflammation, maintain ROM
- Ankle mobilization avoiding end-range dorsiflexion
- Calf stretching (gastrocnemius and soleus)
- Isometric strengthening
-
Phase 2 (Weeks 3-6): Restore ROM and strength
- Progressive dorsiflexion stretching
- Closed chain exercises
- Balance and proprioception training
-
Phase 3 (Weeks 6-12): Sport-specific rehabilitation
- Plyometrics and agility
- Progressive return to running
- Sport-specific drills
Adjunctive Treatments:
- Heel raise (5-10mm) in shoe to reduce dorsiflexion demand
- Orthotics with heel lift for symptomatic relief
- Taping for proprioceptive feedback
Corticosteroid Injection:
- Fluoroscopic or ultrasound-guided anterior joint injection
- 1ml betamethasone (or equivalent) with 2ml local anesthetic
- Provides diagnostic confirmation and temporary relief
- Can repeat once if good response
Conservative treatment is appropriate for Grade I-II lesions and as first-line for all grades. Success rates of 40-60% reported for mild cases.
Don't Miss the Osteochondral Lesion
The surgical steps say "address associated pathology (OCD, loose bodies)", the differential lists OCD of the talar dome, and the Butler evidence card reports a lateral talar dome osteochondral lesion (OCL) in roughly three-quarters of ankles that had a hypertrophic Bassett fascicle — yet the operative implication is easy to overlook.
- The hypertrophic distal AITFL fascicle (Bassett) repeatedly abrades the anterolateral talar dome in dorsiflexion, so anterolateral soft-tissue impingement and a lateral-dome OCL travel together.
- MRI is poorly sensitive for these chondral lesions (Butler; Subhas) — a clean MRI does not exclude an OCL.
- Therefore, at arthroscopy for impingement, systematically probe the talar dome (especially the anterolateral shoulder) rather than stopping once the spur or fascicle is resected.
- If an OCL is found, treat it at the same sitting — debride unstable cartilage and microfracture/marrow-stimulate small lesions, while larger or cystic lesions follow the osteochondral-lesion ladder (the detailed OCL treatment algorithm is developed in the osteochondral-lesion-talus topic).
- Counsel the patient that a co-existing chondral lesion worsens the prognosis — recall that chondral/joint-space status, not spur size, is the dominant outcome determinant (Tol).
Q: You resect a hypertrophic Bassett fascicle arthroscopically and the preoperative MRI was clean — are you done? A: No. Up to ~76% of these ankles harbour a lateral talar dome OCL that MRI frequently misses, so probe the dome and treat any lesion at the same sitting; do not rely on a normal MRI.
Complications
Complications of Anterior Ankle Impingement
Untreated Complications:
- Progressive loss of dorsiflexion (functional decline)
- Chronic pain affecting athletic performance and daily activities
- Compensatory gait abnormalities leading to proximal symptoms
- Secondary ankle arthritis from altered joint mechanics
Surgical Complications
General Complications:
- Infection (less than 1% for arthroscopic procedures)
- Deep vein thrombosis (rare in young athletic population)
- Wound healing issues (particularly with open approach)
Procedure-Specific Complications:
- Incidence
- 2-5%
- Prevention/Management
- Careful portal placement, transillumination
- Incidence
- Less than 1%
- Prevention/Management
- Avoid excessive medial traction
- Incidence
- Rare
- Prevention/Management
- Lateral portal placement
- Incidence
- 5-10%
- Prevention/Management
- Complete resection, address all pathology
- Incidence
- 2-3%
- Prevention/Management
- Early mobilization, physiotherapy
- Incidence
- 10-15%
- Prevention/Management
- Patient selection, manage expectations
Portal-Specific Nerve Anatomy
The superficial peroneal nerve crosses the anterolateral ankle ~6.5cm proximal to the lateral malleolus. Always identify by transillumination before portal placement. The dorsalis pedis artery lies between the EHL and EDL tendons medially.
Anteromedial Portal: Risk to saphenous nerve/vein and medial branch of superficial peroneal nerve
Anterolateral Portal: Risk to superficial peroneal nerve (most common injury)
Risk Factors for Poor Outcome
- Grade IV lesions with secondary arthritis
- Cartilage damage (OCD lesions)
- Significant ankle instability
- Worker's compensation claims
- Prolonged symptoms greater than 2 years pre-surgery
Guidelines, Registries & Global Practice
Global Epidemiology
- Anterior impingement is a leading cause of chronic anterior ankle pain in athletes, dominating kicking and forced-dorsiflexion sports (soccer worldwide, Australian Rules football, ballet, basketball, rugby, gymnastics).
- Peak incidence is in athletes aged 20-35, with a male predominance reflecting sports-participation patterns rather than an intrinsic sex difference.
- A prior history of ankle sprain or recurrent inversion injury is common, especially in the soft-tissue/anterolateral subtype.
Guidance Across Societies
There is no dedicated AAOS/NICE clinical practice guideline for anterior ankle impingement; management is driven by foot-and-ankle society consensus and the van Dijk/Amsterdam group's body of work. The shared international position is consistent:
- Position on anterior ankle impingement
- Trial of structured non-operative care first; arthroscopic debridement for recalcitrant cases; outcome governed by joint-space preservation
- Position on anterior ankle impingement
- Anterior arthroscopy is the standard approach; emphasis on portal safety and complete osteophyte resection
- Position on anterior ankle impingement
- Oblique AMI radiograph for diagnosis; arthroscopic resection; staging by joint-space narrowing rather than spur size alone
- Position on anterior ankle impingement
- Graduated return-to-sport with objective clearance criteria after surgery
Registry & Evidence Notes
- There is no implant involved, so arthroplasty registries (NJR, AJRR, AOANJRR) do not capture this condition; the evidence base is case-series and prospective cohort level (II-IV), not randomised.
- The single most-cited prognostic dataset remains Tol et al's 6.5-year cohort (PMID 11245545), reinforcing joint-space narrowing as the key outcome determinant globally.
High- vs Limited-Resource Practice
- High-resource settings: routine MRI/CT, arthroscopic debridement with fluoroscopy, formal return-to-sport testing.
- Limited-resource settings: diagnosis rests on clinical examination plus lateral and oblique radiographs; a diagnostic/therapeutic intra-articular local-anaesthetic injection is a high-value, low-cost confirmatory test. Where arthroscopy is unavailable, open anterior debridement remains a valid alternative with comparable osteophyte clearance, at the cost of slower recovery.
Controversies & Areas of Uncertainty
- Mechanism of spur formation: the classic capsular-traction theory is contradicted by anatomical evidence that the capsule attaches proximal to the spur origin (PMID 15215021); direct repetitive microtrauma is now the favoured explanation, but the debate is unsettled.
- Where to draw the surgical line: spur size (Scranton-McDermott) versus joint-space narrowing (Tol/van Dijk) as the dominant prognostic factor. Current evidence favours joint-space status, which can downgrade a radiographically "small spur" into a poor surgical prospect once narrowing is present.
- Significance of osteophyte recurrence: regrowth occurs in roughly two-thirds of operated ankles yet most stay symptom-free, so radiographic recurrence is a weak surrogate for clinical failure.
- Role and timing of injection: corticosteroid gives diagnostic confirmation and short-term relief, but durable benefit and the optimal number of injections before surgery are not standardised.
- Open vs arthroscopic for very large or Grade IV lesions: arthroscopy is standard, but for extensive spurs or established arthritis the marginal benefit over open debridement (and whether either alters the arthritic trajectory) is uncertain.
MCQ Practice Points
Q: What is footballer's ankle? A: Anterior ankle impingement from repeated dorsiflexion causing anterior tibial and talar osteophytes. Common in soccer and Australian Rules football.
Q: What is the treatment of choice for anterior ankle impingement? A: Arthroscopic debridement of osteophytes and impinging soft tissue. Greater than 85% good/excellent outcomes.
Q: What nerve is most at risk during anterior ankle arthroscopy? A: Superficial peroneal nerve - crosses 6.5cm proximal to lateral malleolus. Identify by transillumination before portal placement.
Q: What is Bassett's lesion? A: Accessory distal fascicle of the AITFL that can impinge on the anterolateral talar dome with dorsiflexion and cause soft tissue anterior impingement.
Q: What classification is used for anterior ankle impingement? A: Scranton and McDermott classification - Grade I (synovial only), Grade II (less than 3mm spur), Grade III (3-5mm spur), Grade IV (greater than 5mm or arthritis).
Q: What is the standard portal sequence for anterior ankle arthroscopy? A: Anterolateral first (viewing portal), then anteromedial under direct vision (working portal). Both portals are at joint line level.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old soccer player has anterior ankle pain that limits his ability to kick. Pain is worse going up stairs. How do you assess and manage him?”
“You are performing ankle arthroscopy for anterior impingement debridement. Describe your portal placement and how you would avoid neurovascular injury.”
“A patient returns 18 months after arthroscopic debridement with recurrent anterior ankle pain. How do you approach this?”
Key Facts
- Footballer's ankle
- Anterior tibial and talar spurs
- Repeated dorsiflexion microtrauma
- Pain at end-range dorsiflexion
Diagnosis
- Lateral weight-bearing X-ray
- CT for spur detail
- MRI for soft tissue
- Injection confirms diagnosis
Treatment
- Conservative: Activity mod, physio, injection
- Surgical: Arthroscopic debridement
- Greater than 85% good/excellent outcomes
- Most return to sport
Evidence Base
- Open vs arthroscopic resection of anterior tibiotalar spurs - similar operative time but shorter hospital stay and faster recovery with arthroscopy
- Proposed the Grade I-IV grading of spur formation that predicts recovery time
- Recovery to full activity: Grade I 5.0 wk, II 5.6 wk, III 6.4 wk, IV 10.0 wk
- Grade IV lesions deemed unsuitable for arthroscopic debridement
- Prospective series of 57 arthroscopic debridements, mean 6.5-year follow-up
- Excellent/good results stratified by osteoarthritis grade: 100% with no OA, 77% grade I, 53% grade II
- Osteophytes recurred in around two-thirds of grade I ankles yet most stayed symptom-free
- Joint-space narrowing did not progress in most grade II ankles at follow-up
- Cadaveric anatomical study of 8 ankles examining capsule attachment and spur origin
- Anterior capsule attaches PROXIMAL to the site where talotibial spurs originate
- Repetitive capsular traction therefore does not plausibly explain spur formation
- A triangular anterior soft-tissue component is squeezed between tibia and talus at 15 degrees dorsiflexion
- Prospective diagnostic study of 60 patients vs CT, MRI and arthroscopy reference standard
- Lateral radiograph sensitivity only 40% (tibial) and 32% (talar) for anterior osteophytes
- Adding the oblique anteromedial impingement (AMI) view raised sensitivity to 85% and 73%
- Anteromedial spurs are hidden behind the anterolateral tibial rim on a true lateral
- Prospective study of 26 athletes treated arthroscopically for anterior ankle pain
- Karlsson score improved from 66 to 92 and Tegner from 3 to 8 at mean 31 months
- 25 of 26 athletes very satisfied with return to competitive sport
- No significant outcome difference between soft-tissue and bony impingement groups
- MRI of 18 surgically proven abnormal Bassett's ligaments vs 18 controls
- Bassett's ligament identified on MRI in 94% of cases, best seen in the axial plane
- Mean thickness 2.37mm in abnormal cases vs 1.87mm in controls
- Associated talar cartilage lesions and gutter synovitis are poorly detected on conventional MRI
- Retrospective series of 32 patients with hypertrophic distal AITFL fascicle (mean MRI thickness 2.5mm)
- Lateral talar dome osteochondral lesions found arthroscopically in 75.9%
- Preoperative MRI had poor sensitivity for these chondral lesions
- FAOS and VAS improved significantly; no syndesmotic instability after fascicle resection