Inferior Calcaneal Nerve Entrapment | Heel Pain Mimic | Abductor Digiti Minimi Denervation
- Inferior calcaneal nerve (Baxter's nerve) = first branch of the lateral plantar nerve
- Supplies abductor digiti minimi, lateral FDB, and calcaneal periosteum
- Pain does NOT improve with walking (unlike plantar fasciitis which warms up)
- ADM wasting is the pathognomonic clinical sign of chronic entrapment
- Diagnostic nerve block is the single most useful bedside confirmatory test
- “Baxter neuropathy is the most commonly missed cause of refractory 'plantar fasciitis'
- “Tenderness is deep to abductor hallucis, NOT at the plantar fascia origin
- “EMG showing ADM denervation confirms the diagnosis
- “Failed plantar fasciitis treatment lasting greater than 6 months should trigger nerve evaluation
Inferior calcaneal nerve = first branch of lateral plantar nerve. Courses deep to abductor hallucis fascia, between abductor hallucis and quadratus plantae. Supplies ADM, lateral FDB, and calcaneal periosteum.
Plantar fasciitis pain improves with walking. Baxter neuropathy pain does not improve and may worsen. Tenderness is deep to abductor hallucis, not at the calcaneal tuberosity insertion.
Abductor digiti minimi wasting or weakness is the pathognomonic clinical finding. Test resisted little-toe abduction. In chronic cases, visible hollowing of the lateral foot border.
Ultrasound-guided nerve block of Baxter's nerve is the most useful bedside test. Pain relief lasting longer than the local anaesthetic duration supports the diagnosis and predicts surgical success.
- Diagnosis
- Tenderness deep to abductor hallucis, ADM weakness, positive nerve block
- Treatment
- Trial orthotics and stretching first, then surgical decompression
- Key Pearl
- Most commonly missed nerve entrapment in the foot
- Diagnosis
- ADM wasting on exam, EMG showing denervation, MRI with fatty infiltration
- Treatment
- Surgical decompression of inferior calcaneal nerve
- Key Pearl
- EMG positive in approximately 80 percent of confirmed cases
- Diagnosis
- EMG of ADM and medial plantar nerve, MRI of tarsal tunnel
- Treatment
- Tarsal tunnel release including inferior calcaneal nerve branch
- Key Pearl
- Consider systemic neuropathy or S1 radiculopathy if bilateral
WARMBaxter Neuropathy Differentiation from Plantar Fasciitis
Hook:If heel pain does not WARM up with walking, think Baxter neuropathy!
ABQInferior Calcaneal Nerve Course
Hook:ABQ = the nerve runs deep to Abductor hallucis, Between muscles, at the Quadratus plantae edge!
FARMSurgical Decompression Steps
Hook:FARM the heel: Fascia release, Abductor mobilized, Release nerve, Medial fascia release!
Overview and Epidemiology
Baxter neuropathy (entrapment of the inferior calcaneal nerve) is estimated to account for 15 to 20 percent of chronic heel pain cases yet remains the most commonly overlooked cause. Patients are frequently misdiagnosed with plantar fasciitis and subjected to months of ineffective stretching and orthotics. A 2020 systematic review found the average time from symptom onset to correct diagnosis exceeded 12 months. Recognising the clinical pattern early avoids unnecessary disability and guides appropriate nerve decompression surgery, which has an 80 to 90 percent success rate in properly selected patients.
- Prevalence: Estimated 15 to 20 percent of chronic heel pain
- Age: Most common between 30 and 60 years
- Gender: Slight female predominance, possibly related to footwear
- Associations: Flatfoot deformity, hypertrophied abductor hallucis (runners), tarsal tunnel syndrome
- Delayed diagnosis: Average 12 months to correct identification
- Misdiagnosed as: Plantar fasciitis (most common), calcaneal bursitis, fat pad atrophy
- Functional impact: Chronic pain limiting standing, walking, and sport
- Psychological: Frustration from failed treatments, activity restriction
Pathophysiology
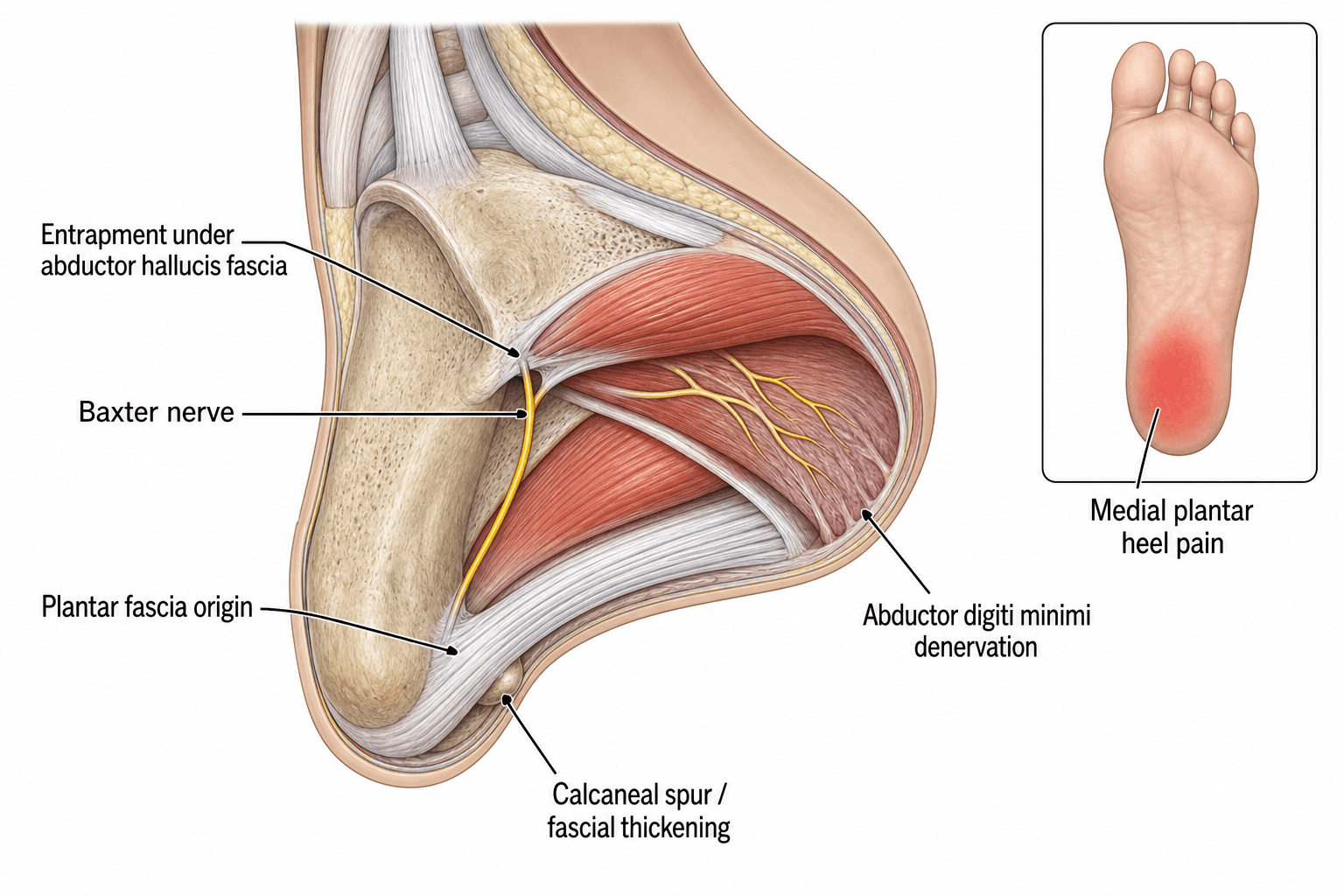
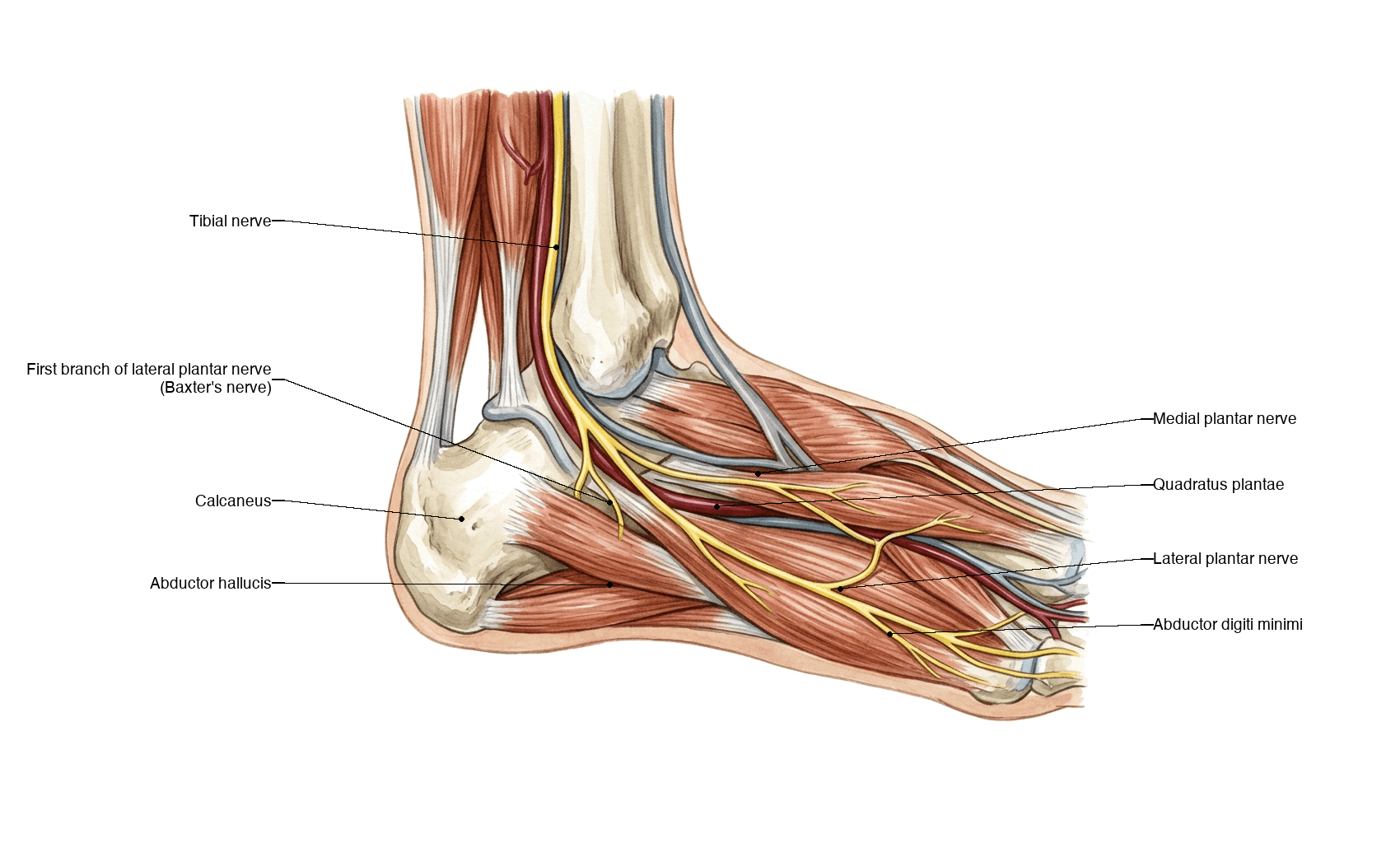
The inferior calcaneal nerve (ICN, Baxter's nerve) is the first branch of the lateral plantar nerve. In approximately 40 percent of cadaveric specimens it arises directly from the tibial nerve proximal to the bifurcation. It courses vertically downward, passing deep to the fascial edge of the abductor hallucis muscle, then runs between the abductor hallucis and the quadratus plantae muscle to reach the lateral foot. It provides motor innervation to the abductor digiti minimi (ADM) and the lateral belly of the flexor digitorum brevis (FDB), as well as sensory branches to the calcaneal periosteum and the long plantar ligament. Entrapment most commonly occurs at the sharp deep fascial edge of the abductor hallucis or between the abductor hallucis and quadratus plantae.
- Origin
- First branch of lateral plantar nerve (or direct from tibial nerve)
- Course
- Deep to abductor hallucis, between AH and quadratus plantae
- Supplies
- ADM, lateral FDB, calcaneal periosteum
- Clinical Relevance
- Entrapment causes chronic heel pain and ADM wasting
- Origin
- Tibial nerve (proximal to tarsal tunnel)
- Course
- Superficial to abductor hallucis fascia
- Supplies
- Medial heel skin (sensory only)
- Clinical Relevance
- Entrapment causes medial heel numbness and burning
- Origin
- Tibial nerve bifurcation (within tarsal tunnel)
- Course
- Deep to flexor retinaculum, into medial plantar aspect
- Supplies
- FDB (medial), FHL, lumbricals 1-2, medial plantar skin
- Clinical Relevance
- Jogger's foot: entrapment at knot of Henry
- Origin
- Tibial nerve bifurcation (within tarsal tunnel)
- Course
- Courses laterally deep to ADM and FDB
- Supplies
- ADM (via ICN), QP, adductor hallucis, lateral plantar skin
- Clinical Relevance
- Tarsal tunnel syndrome affects this nerve and its branches
Primary site: Sharp deep fascial edge of abductor hallucis
Secondary site: Between abductor hallucis and quadratus plantae
Tertiary site: Against medial calcaneal border or bony ridge
Contributing factors: Hypertrophied abductor hallucis (runners, flatfoot), plantar fascia tightness, calcaneal spur encroachment
Result: Ischaemic nerve injury causing demyelination and eventual axonal loss in ADM
Shared anatomy: ICN supplies the calcaneal periosteum near the plantar fascia origin
Pain location: Medial plantar heel (overlap with plantar fascia insertion pain)
Activity relationship: Worse with weight-bearing and standing
Key difference: Pain does NOT have the classic first-step pattern of plantar fasciitis
Coexistence: Both conditions may coexist, complicating diagnosis
Classification and Types
Classification by Entrapment Site
- Site of Compression
- Deep fascial edge of abductor hallucis
- Mechanism
- Sharp fascial band compresses nerve during muscle contraction
- Surgical Target
- Release deep abductor hallucis fascia
- Site of Compression
- Between abductor hallucis and quadratus plantae
- Mechanism
- Hypertrophy of either muscle compresses nerve in tight space
- Surgical Target
- Release muscle edge and decompress nerve course
- Site of Compression
- Medial calcaneal border or bony ridge
- Mechanism
- Nerve compressed against bone or calcaneal spur
- Surgical Target
- Nerve transposition, possible spur excision
Multiple entrapment sites can coexist, and thorough surgical decompression must address all potential compression points along the nerve course.
Clinical Assessment
- Pain character: Deep, aching medial heel pain, may be burning
- Onset: Insidious, progressive over months
- Activity relationship: Worsens with prolonged standing or walking (does NOT improve)
- Failed treatments: Orthotics, calf stretching, night splints, steroid injections all ineffective
- First-step pain: Absent or not predominant (key differentiation from plantar fasciitis)
- Radiation: May radiate laterally along the lateral foot border
- Inspect: Standing arch (flatfoot?), ADM bulk (hollowing in chronic cases), medial heel swelling
- Palpate: Tenderness deep to abductor hallucis (just above the plantar fascia origin), NOT at the calcaneal tuberosity
- Resisted testing: Weak little-toe abduction (ADM weakness)
- Tinel sign: May be positive over the tarsal tunnel or along the nerve course
- Nerve stretch: Passive heel valgus and forefoot abduction may reproduce symptoms
- Sensory exam: Medial heel skin usually normal (medial calcaneal nerve separate)
Technique: Under ultrasound guidance, inject 2 to 3 mL of local anaesthetic (without steroid) around the inferior calcaneal nerve at the medial heel, deep to the abductor hallucis fascia.
Positive result: Significant pain relief within 5 to 10 minutes confirms Baxter neuropathy as the pain generator.
Predictive value: Patients who respond well to the diagnostic block have the highest success rate with surgical decompression.
Key caveat: Ensure the injection is deep to the abductor hallucis fascia, not subcutaneous. Superficial injection may block the medial calcaneal nerve instead, giving a false-positive result.
- Plantar Fasciitis
- Classic hallmark
- Baxter Neuropathy
- Absent or minimal
- Discriminating Value
- High: presence strongly favours plantar fasciitis
- Plantar Fasciitis
- Improves after warm-up
- Baxter Neuropathy
- Worsens or persists
- Discriminating Value
- High: Baxter neuropathy does NOT warm up
- Plantar Fasciitis
- Calcaneal tuberosity (plantar fascia origin)
- Baxter Neuropathy
- Deep to abductor hallucis, superior to fascia origin
- Discriminating Value
- High: different anatomical site
- Plantar Fasciitis
- Absent
- Baxter Neuropathy
- Present (chronic cases)
- Discriminating Value
- Pathognomonic for Baxter neuropathy
- Plantar Fasciitis
- Often improves with calf and fascia stretching
- Baxter Neuropathy
- No improvement or worsening
- Discriminating Value
- Moderate: failure of stretching regimen raises suspicion
- Plantar Fasciitis
- No relief (or only plantar fascia steroid effect)
- Baxter Neuropathy
- Immediate relief with anaesthetic block
- Discriminating Value
- High: diagnostic gold standard
The page rightly calls abductor digiti minimi (ADM) wasting "pathognomonic" - but that is the sign of established, chronic axonal denervation. Baxter's nerve also carries a large sensory supply to the calcaneal periosteum and long plantar ligament, so the earliest and sometimes only presentation is pain alone - deep medial heel pain that does not warm up - before any detectable motor weakness or wasting appears. Little-toe abduction is also genuinely hard to assess clinically, so subtle weakness is easily missed.
The consequence is a false-negative trap: a patient with classic Baxter symptoms but normal ADM strength, a normal EMG and a normal MRI still has Baxter neuropathy until proven otherwise. The diagnosis is clinical and confirmed by the diagnostic nerve block, not by waiting for motor signs to declare themselves - and waiting for ADM wasting before acting means waiting until denervation is irreversible (which is exactly why symptom duration over 12 months predicts permanent motor deficit). Quote it as: ADM wasting confirms chronic Baxter neuropathy, but its absence never excludes it - act on the pain pattern and the block.
- Key Features
- Deep medial heel pain, ADM weakness, no first-step pattern
- Discriminating Finding
- Tenderness deep to abductor hallucis, positive nerve block
- Investigation
- EMG (ADM denervation), MRI (ADM oedema)
- Key Features
- Inferior heel pain, classic first-step pain, improves with walking
- Discriminating Finding
- Tenderness at calcaneal tuberosity, normal ADM
- Investigation
- Ultrasound (fascia thickening greater than 4 mm)
- Key Features
- Burning medial ankle and sole, multiple nerve territories
- Discriminating Finding
- Positive Tinel over tarsal tunnel, sensory loss in plantar distribution
- Investigation
- EMG/NCS of tibial nerve and branches, MRI tarsal tunnel
- Key Features
- Lateral or diffuse heel pain, recent increase in impact activity
- Discriminating Finding
- Squeeze test positive, pain on medial-lateral calcaneal compression
- Investigation
- X-ray (may be normal early), MRI (bone marrow oedema)
- Key Features
- Radiating pain from back, neurological deficit in S1 distribution
- Discriminating Finding
- Positive straight leg raise, reflex changes, proximal symptoms
- Investigation
- Lumbar MRI, EMG of paraspinals and distal muscles
- Key Features
- Burning medial heel, sensory changes (numbness, tingling)
- Discriminating Finding
- Sensory deficit over medial heel skin, no motor involvement
- Investigation
- Nerve conduction studies (sensory branch)
Bilateral Baxter neuropathy is uncommon and should prompt evaluation for systemic causes including peripheral neuropathy (diabetic, alcoholic), inflammatory polyneuropathy, or bilateral S1 radiculopathy. Isolated unilateral Baxter neuropathy is typically mechanical. Always check glucose, B12, and consider neurology referral if bilateral or atypical features present.
Investigations
Investigation Protocol
Views: Lateral and axial (Harris) views of the calcaneus
Look for: Calcaneal stress fracture (sclerosis or fracture line), calcaneal spur (may contribute to nerve compression), bone lesions (tumour, infection)
Note: X-rays are typically normal in Baxter neuropathy; they serve to exclude other causes
Protocol: Non-contrast foot and ankle with dedicated heel sequences
Key findings: ADM fatty infiltration (T1 hyperintensity) or oedema (STIR hyperintensity), signal change within the inferior calcaneal nerve at the compression point, evaluation of tarsal tunnel contents, assessment of plantar fascia
Sensitivity: ADM signal change present in approximately 70 to 85 percent of confirmed cases
Indication: Confirm nerve involvement and exclude tarsal tunnel syndrome or S1 radiculopathy
Findings: Denervation potentials in ADM (fibrillations, positive sharp waves), prolonged distal motor latency to ADM, normal medial plantar nerve conduction (differentiates from tarsal tunnel)
Sensitivity: Approximately 80 percent sensitivity for confirmed surgical cases; normal EMG does not exclude the diagnosis
Technique: Ultrasound-guided injection of 2 to 3 mL local anaesthetic around the ICN deep to abductor hallucis
Interpretation: Greater than 50 percent pain relief within 10 minutes strongly supports the diagnosis
Predictive value: Best predictor of surgical success; include in pre-operative workup
Advantage: Dynamic assessment of nerve compression during foot movements
Findings: Nerve hypertrophy at entrapment site, loss of normal fascicular pattern, perineural oedema
Role: Adjunct to MRI, useful for guiding diagnostic blocks and intraoperative localisation
No single test is diagnostic in isolation. The diagnosis of Baxter neuropathy is clinical and supported by a combination of examination findings (ADM weakness, deep tenderness), a positive diagnostic nerve block, and confirmatory imaging (MRI with ADM signal change) or electrodiagnostics (ADM denervation). EMG sensitivity is only approximately 80 percent, so a normal EMG does NOT exclude the diagnosis if clinical suspicion is high.
The flip side of imaging: isolated fatty atrophy or denervation oedema of the abductor digiti minimi is a common INCIDENTAL finding on foot MRI in people without heel pain - reported in a substantial minority of asymptomatic feet (it is the most frequently denervated intrinsic foot muscle on routine MRI). So ADM signal change is a sensitive but not specific sign: finding it does not prove that Baxter neuropathy is the source of this patient's pain.
The practical traps:
- Do not attribute heel pain to Baxter neuropathy on the strength of an ADM signal change alone - the finding must correlate with the clinical pattern (no first-step pain, tenderness deep to abductor hallucis) and ideally a positive diagnostic nerve block.
- An incidental ADM atrophy in a patient whose pain is actually plantar fasciitis, a calcaneal stress fracture or S1 radiculopathy will lead to an unnecessary, and likely unsuccessful, nerve decompression.
- Conversely (see the clinical pearl above), a normal ADM does not exclude early Baxter neuropathy.
Exam point: ADM denervation on MRI is non-specific (frequent incidental finding) - it supports the diagnosis only when it matches the clinical picture and the block; imaging never replaces the clinical/block-based diagnosis.
Management Algorithm
Conservative Management (First 3 to 6 Months)
Goal: Reduce nerve compression and inflammation through offloading, stretching, and targeted injections
Conservative Protocol
Activity modification: Reduce prolonged standing, walking on hard surfaces, and running
Orthotics: Medial arch support to offload the nerve, heel lift to reduce stretch on tibial nerve branches
Stretching: Calf stretching (gastrocnemius and soleus), plantar fascia stretching (even though not the primary pathology)
Footwear: Avoid flat, unsupportive shoes; use lace-up shoes with medial arch support
NSAIDs: Trial of oral anti-inflammatory medication for pain modulation
Physiotherapy: Nerve gliding exercises for tibial nerve and branches, abductor hallucis massage and fascial release
Corticosteroid injection: Ultrasound-guided injection around the ICN (may provide temporary relief; response supports diagnosis)
Night splint: Ankle dorsiflexion splint to maintain nerve excursion overnight
Re-evaluate: If significant improvement, continue conservative care
Nerve block: If still symptomatic, perform diagnostic ICN nerve block to confirm pain generator
EMG and MRI: Obtain if not already done to confirm diagnosis and exclude mimics
Refer: For surgical decompression if confirmed Baxter neuropathy with failed conservative management
Conservative management should be trialled for 3 to 6 months in all patients before surgical decompression. However, the key error is treating presumed plantar fasciitis conservatively for 12 or more months without ever considering Baxter neuropathy. If heel pain does not have the classic first-step pattern and does not respond to plantar-directed treatments within 3 months, reassess for nerve entrapment.
Complications
- Incidence
- 10 to 20 percent
- Risk Factors
- Inadequate decompression, incorrect diagnosis, central sensitisation
- Management
- Repeat diagnostic block, re-explore if block positive, pain management referral
- Incidence
- 5 to 10 percent
- Risk Factors
- Diabetes, smoking, peripheral vascular disease, location (medial heel)
- Management
- Wound care, offloading, advanced dressings, consider plastic surgery input
- Incidence
- 10 to 15 percent (if chronic denervation)
- Risk Factors
- Duration of symptoms greater than 12 months, severe axonal loss on EMG
- Management
- Physiotherapy, nerve recovery may take 12 to 18 months; some deficit may be permanent
- Incidence
- Less than 2 percent
- Risk Factors
- Anatomical variation, difficult dissection, poor exposure
- Management
- Intraoperative nerve monitoring, immediate repair if recognised, neurolysis
- Incidence
- 5 to 10 percent
- Risk Factors
- Scar tissue, uncorrected flatfoot, inadequate initial release
- Management
- Repeat decompression with neurolysis, address underlying deformity
- Incidence
- 3 to 5 percent
- Risk Factors
- Wound location on weight-bearing heel margin
- Management
- Scar massage, desensitisation, neuroma excision if refractory
The most important factor in preventing complications is correct patient selection. A positive diagnostic nerve block is the strongest predictor of surgical success. Patients with central sensitisation features (allodynia, widespread pain, disproportionate symptoms) should be counselled carefully and may benefit from pain medicine input before surgery. Operating on patients with normal nerve blocks or atypical pain patterns has the highest failure rate.
Outcomes and Prognosis
- Treatment
- Conservative or early decompression
- Expected Outcome
- 80 to 90 percent significant pain relief
- Long-term Function
- Full return to activity, ADM recovery
- Treatment
- Surgical decompression
- Expected Outcome
- 70 to 85 percent good or excellent results
- Long-term Function
- Good functional improvement, ADM may partially recover
- Treatment
- Surgical decompression
- Expected Outcome
- 60 to 75 percent pain relief, variable motor recovery
- Long-term Function
- Pain improved but ADM weakness may be permanent
- Treatment
- Combined decompression
- Expected Outcome
- 65 to 80 percent improvement
- Long-term Function
- Variable, depends on extent of nerve pathology
Best prognosis: Short duration of symptoms, positive diagnostic nerve block, no central sensitisation, isolated Baxter neuropathy (no broader tarsal tunnel involvement), EMG showing demyelination rather than axonal loss
Poor prognosis: Symptoms greater than 12 months, fixed ADM wasting with complete denervation on EMG, bilateral symptoms (suggest systemic neuropathy), failed prior foot surgery, central sensitisation features
Key threshold: Symptom duration greater than 12 months correlates with irreversible ADM changes and lower surgical success rates.
Guidelines, Registries & Global Practice
- Chronic heel pain affects approximately 10 percent of the population over a lifetime
- Baxter neuropathy is estimated to account for 15 to 20 percent of chronic heel pain, though rates vary by referral practice
- Under-diagnosed globally: Average time to diagnosis exceeds 12 months across all practice settings
- Risk factors: Running and jumping sports, standing occupations, pes planovalgus, obesity
- High-resource: MRI and EMG are readily available; ultrasound-guided diagnostic blocks standard; dedicated foot-ankle surgeons perform decompression
- Limited-resource: Diagnosis is often clinical; diagnostic blocks can be performed with palpation-guided technique; orthotics and footwear modification are first-line
- Universal principle: The diagnosis is primarily clinical; treatment success depends on correct identification of the pain generator, not on access to advanced imaging
- Surgery: Should only be offered after failed conservative care and positive diagnostic nerve block, regardless of setting
- Diagnostic Emphasis
- High index of suspicion in refractory heel pain; diagnostic nerve block recommended
- Treatment Algorithm
- 3 to 6 months conservative care (orthotics, stretching, injection) before surgery
- Surgical Indication
- Failed conservative care with positive nerve block and EMG or MRI correlation
- Diagnostic Emphasis
- Clinical differentiation from plantar fasciitis emphasised; ADM assessment mandatory
- Treatment Algorithm
- Structured rehabilitation pathway; USS-guided block as gatekeeper investigation
- Surgical Indication
- Decompression in specialist foot-ankle units after multidisciplinary assessment
- Diagnostic Emphasis
- MRI recommended before surgery to exclude other pathology and confirm ADM changes
- Treatment Algorithm
- Conservative trial mandatory; orthotics and physiotherapy first-line
- Surgical Indication
- Positive nerve block plus imaging evidence; address concurrent deformity
- Diagnostic Emphasis
- Baxter neuropathy should be considered in all heel pain lasting greater than 6 months
- Treatment Algorithm
- Conservative management as per plantar fasciitis initially; nerve block at 3 months
- Surgical Indication
- Surgical decompression with or without flatfoot correction based on deformity
There is no dedicated registry for Baxter neuropathy or inferior calcaneal nerve decompression. The evidence base consists of small case series, cadaveric anatomical studies, and expert opinion reviews. No randomised controlled trials of surgical decompression versus continued conservative care have been published. Treatment guidance is therefore principle-based: diagnose early using clinical assessment and nerve block, trial conservative care, and decompress the nerve in properly selected patients with confirmed entrapment.
Record in every refractory heel pain assessment:
- Duration of symptoms and failed treatments
- Examination findings: tenderness location, ADM strength, Tinel sign
- Whether diagnostic nerve block was performed and its result
- MRI findings: ADM signal change, nerve status, plantar fascia assessment
- EMG/NCS results if obtained (ADM denervation, tarsal tunnel evaluation)
- Counselling regarding expected outcomes and recovery timeline
A missed Baxter neuropathy diagnosis resulting in 12 or more months of ineffective treatment is a common source of patient dissatisfaction and medicolegal claims. Always document the rationale for the diagnosis and the evidence supporting it.
Controversies & Areas of Uncertainty
EMG sensitivity for Baxter neuropathy is approximately 80 percent, meaning a normal study does not exclude the diagnosis. Some surgeons operate on clinical and nerve-block evidence alone, while others consider EMG mandatory. There is no consensus on whether EMG should be a prerequisite for surgical decompression or an adjunct that modifies counselling.
When Baxter neuropathy is confirmed without broader tarsal tunnel involvement, the question arises whether the tarsal tunnel should be released prophylactically. Proponents argue that releasing only the distal branch misses proximal contributing compression. Opponents cite unnecessary dissection and increased morbidity. Current evidence favours targeted release guided by clinical and electrodiagnostic findings.
Endoscopic release of the inferior calcaneal nerve has been described in small series with theoretical advantages of smaller incisions and faster recovery. However, evidence is limited to case reports and small case series, and the technique does not allow visualisation of the full nerve course or concurrent tarsal tunnel release. It remains investigational.
Whether to release the medial one-third of the plantar fascia during Baxter nerve decompression is debated. Some argue that plantar fascia tightness contributes to nerve compression and should be routinely released. Others contend that fascia release may destabilise the arch and is only indicated when the fascia is visibly compressing the nerve. No randomised data exist to guide this decision.
MCQ Practice Points
Q: What is the inferior calcaneal nerve (Baxter's nerve) and what does it supply? A: The inferior calcaneal nerve is the first branch of the lateral plantar nerve (in approximately 60 percent it arises from the lateral plantar nerve; in approximately 40 percent directly from the tibial nerve). It supplies motor innervation to the abductor digiti minimi and the lateral belly of the flexor digitorum brevis, and sensory branches to the calcaneal periosteum and long plantar ligament. Entrapment produces chronic heel pain with ADM weakness.
Q: How do you clinically differentiate Baxter neuropathy from plantar fasciitis? A: Four key differences: (1) Plantar fasciitis has classic first-step morning pain that improves with walking; Baxter neuropathy pain does not improve. (2) Tenderness in plantar fasciitis is at the calcaneal tuberosity; in Baxter neuropathy it is deep to the abductor hallucis. (3) ADM weakness or wasting is present in Baxter neuropathy but absent in plantar fasciitis. (4) A diagnostic nerve block of the inferior calcaneal nerve relieves Baxter neuropathy pain but not plantar fasciitis pain.
Q: What MRI findings support the diagnosis of Baxter neuropathy? A: Two key findings: (1) Abductor digiti minimi muscle signal change — oedema (STIR hyperintensity) in acute-subacute entrapment or fatty infiltration (T1 hyperintensity) in chronic denervation. (2) Signal abnormality within the inferior calcaneal nerve at the entrapment point between abductor hallucis and quadratus plantae. MRI also evaluates for tarsal tunnel pathology and plantar fascia status.
Q: What are the key steps in surgical decompression of the inferior calcaneal nerve? A: Approach: Medial heel curvilinear incision. Key steps: (1) Identify the tibial nerve in the tarsal tunnel and trace the lateral plantar nerve. (2) Identify the first branch (inferior calcaneal nerve). (3) Release the deep fascial edge of the abductor hallucis (primary compression site). (4) Follow the nerve between abductor hallucis and quadratus plantae, releasing all fibrous bands. (5) Ensure the nerve is free from origin to the calcaneal border. (6) Release the medial one-third of the plantar fascia if contributing to compression.
Q: Why is the diagnostic nerve block important in Baxter neuropathy? A: The ultrasound-guided diagnostic nerve block of the inferior calcaneal nerve serves two purposes: (1) Diagnostic confirmation — greater than 50 percent pain relief within 10 minutes confirms Baxter neuropathy as the pain generator. (2) Prognostic value — patients with a positive block have the highest success rate (approximately 80 to 90 percent) with surgical decompression. It is the single most useful bedside investigation.
Q: What factors predict poor outcome after surgical decompression for Baxter neuropathy? A: Poor prognostic factors: symptom duration greater than 12 months, complete ADM denervation on EMG (axonal loss rather than demyelination), negative pre-operative diagnostic nerve block, concurrent tarsal tunnel syndrome (broader nerve involvement), uncorrected flatfoot deformity, and central sensitisation features. The strongest positive predictor is a positive diagnostic nerve block.
Clinical Imaging
Baxter Neuropathy: Imaging Hallmarks
MRI is the gold standard for imaging Baxter neuropathy. Key findings include fatty infiltration or oedema of the abductor digiti minimi muscle belly (best seen on T1-weighted and STIR sequences), signal change within the inferior calcaneal nerve itself at the compression point between abductor hallucis and quadratus plantae, and often concurrent plantar fasciitis changes. Ultrasound can demonstrate nerve hypertrophy at the entrapment site and dynamic compression with foot movements.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old female runner presents with 8 months of right medial heel pain. She was diagnosed with plantar fasciitis by her GP and has completed 6 months of calf stretching, night splints, orthotics, and two ultrasound-guided steroid injections at the calcaneal tuberosity with only transient benefit. Pain is present throughout the day, worsens with prolonged standing, and does not improve with walking. On examination, there is no tenderness at the calcaneal tuberosity. Tenderness is present deep to the abductor hallucis on the medial heel. Resisted little-toe abduction is weak on the right. What is the diagnosis and how would you investigate?”
“A 55-year-old man with bilateral flexible pes planovalgus presents with 14 months of left heel pain. EMG shows fibrillation potentials in the left ADM with normal medial plantar nerve conduction. MRI demonstrates fatty infiltration of the left ADM and oedema at the inferior calcaneal nerve between the abductor hallucis and quadratus plantae. Diagnostic nerve block provides 90 percent pain relief. He asks about surgical options. How would you counsel him?”
Key Anatomy
- Inferior calcaneal nerve = first branch of lateral plantar nerve (or direct from tibial nerve in approximately 40 percent)
- Courses deep to abductor hallucis fascia, between abductor hallucis and quadratus plantae
- Supplies abductor digiti minimi, lateral flexor digitorum brevis, calcaneal periosteum
- Primary entrapment site: deep fascial edge of abductor hallucis
Clinical Differentiation from Plantar Fasciitis
- No first-step morning pain (plantar fasciitis hallmark)
- Pain does NOT improve with walking (worsens or persists)
- Tenderness deep to abductor hallucis, NOT at calcaneal tuberosity
- ADM weakness or wasting is pathognomonic
Investigations
- MRI: ADM oedema (acute) or fatty infiltration (chronic), nerve signal change at entrapment
- EMG: ADM denervation (fibrillation, prolonged distal latency); sensitivity approximately 80 percent
- Diagnostic nerve block (ultrasound-guided): best bedside test and strongest surgical predictor
- X-ray: normal in Baxter neuropathy; excludes calcaneal stress fracture
Surgical Decompression
- Medial heel incision, identify tibial nerve, trace to ICN branch
- Release deep abductor hallucis fascia (primary compression site)
- Decompress nerve between abductor hallucis and quadratus plantae
- Consider medial plantar fascia release and flatfoot correction if indicated
Outcomes and Pitfalls
- 80 to 90 percent success with positive nerve block and proper patient selection
- Duration greater than 12 months correlates with irreversible ADM damage
- Must address underlying flatfoot deformity to prevent recurrence
- Tarsal tunnel release alone does NOT reliably decompress the inferior calcaneal nerve
Evidence Base and Key Trials
Treatment of chronic heel pain by release of the first branch of the lateral plantar nerve
- Landmark study establishing inferior calcaneal nerve entrapment as a distinct cause of chronic heel pain
- 69 heels in 61 patients treated with surgical release of the first branch of the lateral plantar nerve
- Good or excellent results reported in approximately 83 percent of patients at mean follow-up of 27 months
- Identified the deep fascial edge of the abductor hallucis as the primary site of nerve compression
Heel pain syndrome: electrodiagnostic support for nerve entrapment
- Electrodiagnostic study of patients with chronic heel pain unresponsive to conservative treatment
- Demonstrated abnormal nerve conduction studies localising to the inferior calcaneal nerve in a substantial proportion
- Supported the concept that nerve entrapment is a primary pain generator in refractory heel pain
- Patients with positive electrodiagnostics had better outcomes following surgical decompression
MR imaging of entrapment neuropathies of the lower extremity. Part 2: the knee, leg, ankle, and foot
- Comprehensive review of MRI appearances of lower extremity nerve entrapments including Baxter neuropathy
- Described ADM muscle denervation oedema (T2/STIR hyperintensity) and fatty infiltration (T1) as hallmark MRI findings
- Highlighted the importance of dedicated small-field-of-view sequences for detecting inferior calcaneal nerve signal change
- MRI sensitivity for detecting nerve entrapment in the foot improved with higher field strength (3T) scanners
Sonographic visualization of the first branch of the lateral plantar nerve (Baxter nerve): technique and validation using perineural injections in a cadaveric model
- Demonstrated reliable sonographic identification of the inferior calcaneal nerve in cadaveric and clinical studies
- Described the nerve as a hypoechoic structure deep to the abductor hallucis fascia with a characteristic course
- Nerve hypertrophy and loss of normal fascicular pattern correlated with clinical entrapment
- Ultrasound-guided diagnostic blocks were more accurate than landmark-guided injections
Distal tarsal tunnel release with partial plantar fasciotomy for chronic heel pain: an outcome analysis
- Prospective outcome study of distal tarsal tunnel release with partial plantar fasciotomy for chronic heel pain unresponsive to conservative treatment
- Included release of the inferior calcaneal nerve (Baxter nerve) as a standard component of the distal tarsal tunnel release
- Significant improvement in pain and function reported at mean follow-up exceeding 12 months
- Supports the role of combined nerve decompression and fascial release in refractory heel pain