Berndt-Harty Classification of Osteochondral Talar Lesions
The Berndt-Harty classification
- Pathology
- Subchondral compression
- Radiographic finding
- Compression of subchondral bone, no visible fragment
- Cartilage status
- Intact
- Pathology
- Partially detached fragment
- Radiographic finding
- Fragment partly separated from the talar dome
- Cartilage status
- Partially breached
- Pathology
- Completely detached, not displaced
- Radiographic finding
- Fragment separated but still within the crater
- Cartilage status
- Completely breached
- Pathology
- Completely detached and displaced
- Radiographic finding
- Fragment displaced from the crater — loose body in the joint
- Cartilage status
- Disrupted with loose body

CPDDThe four stages
Hook:CPDD: Compressed, Partial, Detached (in situ), Displaced (loose body).
- Medial OLTs are more common (~60%), sit posteromedially, are deep and cup-shaped, and arise from inversion + PLANTARflexion + external rotation of the tibia on the talus. They are less associated with trauma and have better bone stock for fixation.
- Lateral OLTs are less common, sit anterolaterally, are shallow and wafer-shaped, and arise from inversion + DORSIflexion (a shearing force against the fibula). They are more often associated with trauma, more often symptomatic, and more likely to displace into a loose body.
The single most-confused point in vivas: medial = plantarflexion, lateral = dorsiflexion.
MRI staging — the Hepple modification
Plain radiographs under-stage OLTs, so the Hepple modification restages the lesion on MRI, adding oedema sub-staging and a subchondral-cyst stage that refine management.
- Finding on MRI
- Cartilage thickening/signal change, no fracture line
- Berndt-Harty equivalent
- I
- Management implication
- Non-operative
- Finding on MRI
- Cartilage breach, underlying fracture, bony oedema present
- Berndt-Harty equivalent
- I–II
- Management implication
- Non-operative trial; early arthroscopy if failing
- Finding on MRI
- Cartilage breach, underlying fracture, no bony oedema
- Berndt-Harty equivalent
- II
- Management implication
- More chronic — arthroscopy likely; fragment may be unstable
- Finding on MRI
- Detached but undisplaced fragment in the crater
- Berndt-Harty equivalent
- III
- Management implication
- Fix if viable; excise and marrow-stimulate if not
- Finding on MRI
- Displaced fragment — loose body
- Berndt-Harty equivalent
- IV
- Management implication
- Arthroscopic excision plus marrow stimulation or OATS
- Finding on MRI
- Subchondral cyst, cartilage intact or breached
- Berndt-Harty equivalent
- Late-stage
- Management implication
- Cyst management (graft/retrograde drilling) plus cartilage restoration

Do not rely on plain radiographs alone to stage an OLT. MRI is essential — it reveals cartilage integrity, fragment stability, bony oedema, and subchondral cysts invisible on plain films, and a lesion that looks like stage I on X-ray may be stage III or higher on MRI. CT is useful for surgical planning (mapping fragment size, location and bone stock) but does not assess cartilage or marrow oedema.
Clinical presentation & examination
An OLT classically presents as the ankle sprain that does not get better: chronic, deep ankle pain weeks to months after an inversion injury, with weight-bearing and activity-related pain, intermittent swelling and stiffness, and catching, clicking or locking when a fragment is unstable or a loose body (stage IV) is present. The examination is often subtle - an effusion, talar-dome tenderness (palpate the anteromedial or anterolateral dome with the ankle plantar/dorsiflexed), reduced range - and can be normal. The practical lesson is that persistent pain after an "ordinary" ankle sprain should prompt suspicion of an OLT and dedicated MRI, because plain films are normal or under-read - the injury is commonly missed precisely because the early examination and radiograph look unremarkable.
Management — by stage, viability and size
- 1Stage I–II: treat non-operatively firstA trial of offloading — cast or boot, non-weight-bearing, typically around 6 weeks — with arthroscopy reserved for failure of conservative care (e.g. ongoing symptoms at ~3 months).
- 2Stage III: decide on viabilityThe grey zone. An acute fragment with viable, bleeding subchondral bone is a fixation candidate (bioabsorbable pins / headless screws). A chronic, sclerotic or cystic fragment is better excised with marrow stimulation of the base.
- 3Stage IV: remove the loose bodyA displaced fragment will not heal — arthroscopic excision plus marrow stimulation (microfracture/drilling) of the defect base.
- 4Let size choose the cartilage procedureMarrow stimulation works well for smaller lesions; lesions larger than about 15 mm (or over 150 mm²), and cystic or revision lesions, do better with osteochondral grafting (OATS/allograft) or cell-based techniques (ACI/MACI).
~15 mmsize threshold is the widely-cited cut-off: at or below it, bone-marrow stimulation gives good results; above it (or for cystic/revision lesions) osteochondral grafting is generally preferred.
For a completely detached but undisplaced fragment, expect to discuss both options and justify your choice: fix an acute, viable fragment with good subchondral bone; excise and marrow-stimulate a chronic, sclerotic or cystic one. Intra-operative assessment frequently upstages the pre-operative classification — Ferkel found that arthroscopic stage (not radiograph/CT/MRI stage) correlated with outcome.
Where the lesion sits dictates the approach, and this is a favourite operative-viva point. Anterior and anterolateral lesions are reachable by standard anterior ankle arthroscopy or an anterolateral arthrotomy. The posteromedial dome - the commonest location - is the hardest to reach for an open osteochondral graft, and frequently requires a medial malleolar osteotomy (a pre-drilled chevron/step-cut osteotomy, reduced and fixed with screws) to expose it; very posterior lesions may instead be approached posteriorly or with non-invasive joint distraction. A malleolar osteotomy carries its own risks - nonunion, malunion, an intra-articular step and hardware irritation - so it is reserved for procedures (OATS/grafting) that genuinely need open exposure, whereas arthroscopic marrow stimulation avoids it altogether. This is why a small, accessible lesion is treated arthroscopically while a posteromedial lesion needing a graft becomes a substantially bigger operation.
Limitations & modern context
- The original classification is from 1959, based on plain radiographs and surgical observation. MRI staging (Hepple 1999) adds precision, but Berndt-Harty remains the shared language.
- Stage III is inherently subjective — whether a detached fragment is truly in situ depends on imaging quality and timing, and arthroscopy often upstages it.
- Chronicity matters more than stage alone — an acute, viable stage III is for fixation; a chronic sclerotic/cystic stage III is for excision and cartilage restoration.
- Lesion size is not part of Berndt-Harty but critically affects outcome — larger (over ~15 mm / over 150 mm²) and cystic lesions do worse with marrow stimulation alone and favour OATS/allograft.
- Newer techniques (MACI, particulated juvenile cartilage, scaffolds) expand the options for large or failed lesions but sit beyond the classic classification.
- It applies to the talar dome only — lesions of the tibial plafond, navicular or other tarsals are not staged by this system.
What it classifies, and why it matters
Berndt and Harty described, from cadaveric experiments and clinical cases, a four-stage progression of "transchondral fractures" of the talar dome. It remains the universal language for OLTs because the stage maps cleanly onto management: an undisplaced compression heals with offloading, whereas a displaced loose body never will. The two things the classification does not capture — chronicity/viability of the fragment and lesion size — turn out to drive the modern operative decision, so a good answer always layers those on top of the stage.
Exam & revision
Everything below condenses the classification for revision and viva practice.
- Four stages: I compression → II partial detachment → III complete detachment undisplaced → IV displaced loose body.
- Medial = plantarflexion + inversion + ext rotation, posteromedial, deep/cup-shaped, commoner; lateral = dorsiflexion + inversion, anterolateral, shallow/wafer-shaped, more traumatic and more likely to displace.
- Stage I–II non-operative; stage IV always operative; stage III is the grey zone (fix viable, excise non-viable).
- MRI is essential (Hepple modification) — plain films under-stage; arthroscopic stage correlates with outcome (Ferkel).
- Size ~15 mm separates marrow stimulation from osteochondral grafting.
NCFFManagement by stage
Hook:NCFF by stage: Non-op, Conservative trial, Fix-or-excise, Free fragment out.
Medial PLD, Lateral DSAMedial vs lateral
Hook:Medial = PLantarflexion + Deep; Lateral = Dorsiflexion + Shallow (the most-muddled point).
Exam viva
Practise clinical reasoning and management decisions out loud
“A 28-year-old netballer presents with persistent right ankle pain six months after an inversion injury. MRI shows a 10 mm osteochondral lesion on the posteromedial talar dome with a completely detached but undisplaced fragment. How would you classify and manage this?”
“A 35-year-old runner had arthroscopic excision and marrow stimulation of a lateral talar OLT (Berndt-Harty Stage IV, 12 mm) two years ago. She now has recurrent pain and new MRI shows a subchondral cyst at the same site with intact overlying cartilage. How do you classify this, and what is the management?”
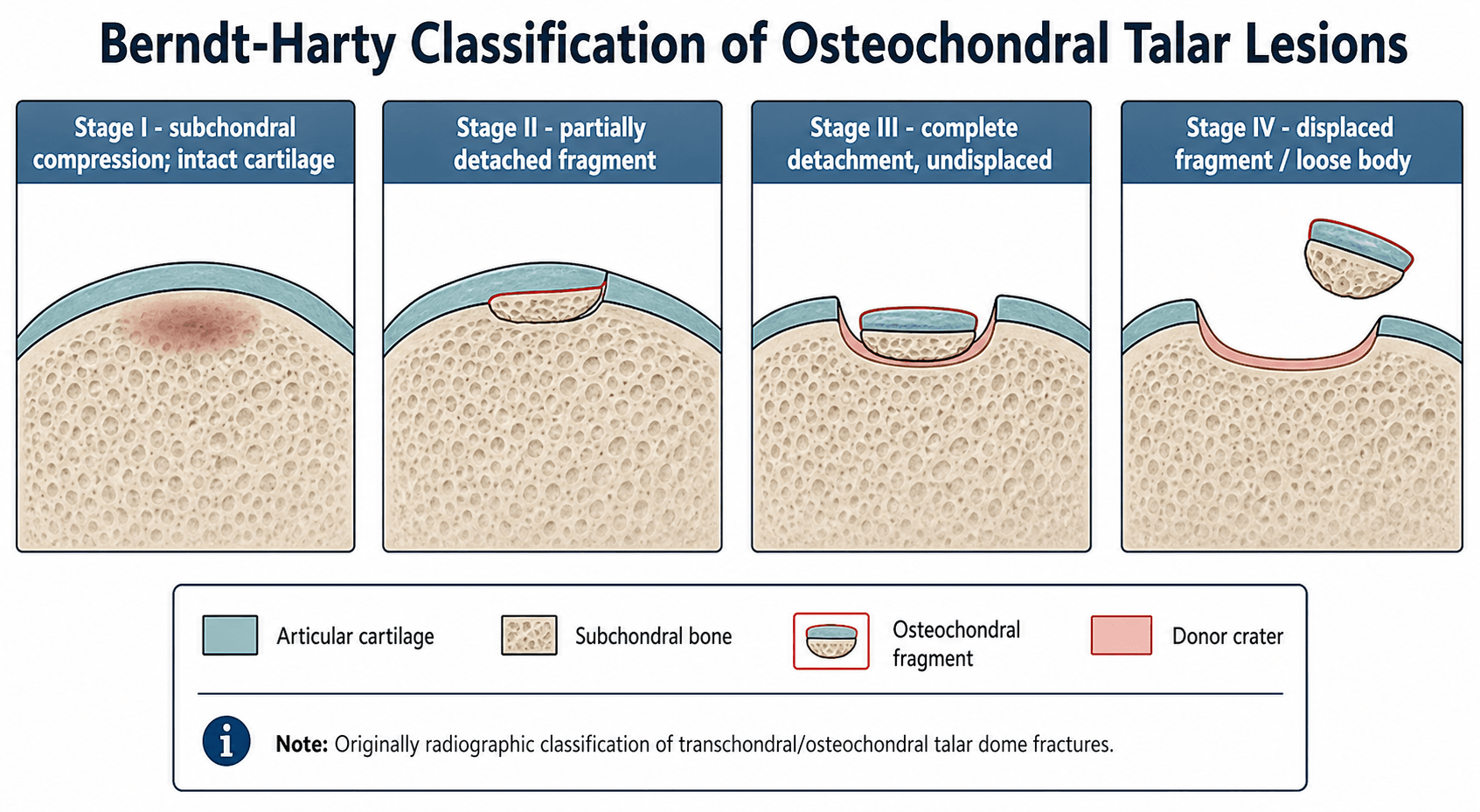
The four stages
- Stage I: subchondral compression — cartilage intact, no visible fragment
- Stage II: partial detachment — fragment partly separated from the dome
- Stage III: complete detachment, fragment still in crater (not displaced)
- Stage IV: complete detachment with displacement — loose body in the joint
Medial vs lateral patterns
- Medial (~60%): posteromedial, cup-shaped, deep — inversion + PLANTARflexion + external rotation
- Lateral (~40%): anterolateral, wafer-shaped, shallow — inversion + DORSIflexion (shearing)
- Lateral lesions are more traumatic, more often symptomatic and more likely to displace
- Medial lesions have better bone stock for fixation when caught before displacement
Management by stage and size
- Stage I–II: non-weight-bearing cast/boot ~6 weeks; arthroscopy if failing
- Stage III: fix if viable (acute, good bone); excise + marrow-stimulate if chronic/non-viable
- Stage IV: arthroscopic excision of loose body + marrow stimulation
- Size: marrow stimulation up to ~15 mm; OATS/ACI for larger or cystic lesions
Key pitfalls
- Always get MRI — plain films under-stage; Hepple staging refines it
- Medial = plantarflexion, lateral = dorsiflexion (commonly muddled)
- Stage III is the grey zone: discuss both fixation and excision with justification
- Hepple Stage 5 (subchondral cyst) needs grafting/OATS, not just marrow stimulation
Evidence
Transchondral fractures (osteochondritis dissecans) of the talus
- Original four-stage classification of transchondral (osteochondral) talar dome fractures, derived from cadaveric experiments and clinical cases.
- Stage I subchondral compression through Stage IV displaced loose body.
- Described distinct mechanisms: lateral lesions from inversion + dorsiflexion (shearing); medial lesions from inversion + plantarflexion + external rotation.
Osteochondral lesions of the talus: a revised classification
- Revised Berndt-Harty for MRI into stages 1, 2a, 2b, 3, 4 and 5, adding bony-oedema sub-staging and a subchondral-cyst stage.
- High-resolution MRI provided far greater detail of the pathological anatomy than plain radiographs.
- Distinguished cartilage-breached lesions by the presence (2a) or absence (2b) of underlying bony oedema.
According to PubMed, the staging and mechanisms come from Berndt & Harty 1959 (the original four-stage description, J Bone Joint Surg Am 1959;41-A:988-1020 - pre-DOI); the MRI restaging from Hepple et al. 1999 (DOI); the arthroscopic outcome data and the arthroscopic-stage correlation from Ferkel et al. 2008 (DOI); and the comparative treatment success rates from Zengerink et al. 2010 (DOI). The approximately 15 mm / 150 mm² size threshold for choosing osteochondral grafting over marrow stimulation is widely cited consensus from the broader OLT literature.