Open or arthroscopic release of a contracted lateral retinaculum for isolated excessive lateral patellar tilt without instability · intermediate
- The modern indication is narrow: an isolated, OBJECTIVELY TIGHT lateral retinaculum producing EXCESSIVE LATERAL PATELLAR TILT WITHOUT frank instability — historically termed excessive lateral pressure syndrome (lateral compression syndrome, Ficat). The patella is tilted laterally with a tight lateral facet but does NOT sublux or dislocate (negative lateral glide, no apprehension).
- CRITICAL: a lateral release does NOT correct lateral patellar instability (recurrent dislocation). Instability is driven by medial restraint deficiency (MPFL) and/or bony malalignment (increased TT-TG, trochlear dysplasia, patella alta) — for which the correct operation is MPFL reconstruction and/or tibial tubercle transfer. Isolated release for instability is a historical error and can PARADOXICALLY CAUSE iatrogenic medial instability.
- Technique: divide the lateral retinaculum from the superior pole of the patella to the tibial tubercle, SPARING the vastus lateralis tendon, and COAGULATE the superior lateral geniculate artery and vein at the superolateral corner — the principal source of post-operative haemarthrosis.
- Lateral retinacular LENGTHENING (a Z-plasty) is increasingly preferred over complete release: it corrects tilt while preserving lateral restraint, markedly reducing the risk of over-release and iatrogenic medial patellar instability.
When & Why
Indication. Lateral retinacular release (LRR) is indicated for the isolated, objectively tight lateral retinaculum producing excessive lateral patellar tilt without frank instability — historically termed excessive lateral pressure syndrome (ELPS) or lateral patellar compression syndrome (Ficat). A contracted lateral retinaculum holds the patella in lateral tilt, increasing lateral-facet contact pressure and producing lateral retropatellar pain and, over time, lateral-facet chondrosis. The one decision that matters. Before offering any lateral procedure, confirm exactly which patellofemoral problem you are treating:
Lateral tilt plus a tight lateral retinaculum plus lateral-facet overload plus NO instability. The ONE indication — treat with a lateral release or, increasingly, a lengthening.
MPFL deficiency and/or bony malalignment (increased TT-TG, trochlear dysplasia, patella alta). The correct operation is MPFL reconstruction and/or tibial tubercle transfer — NOT an isolated release.
No objective lateral tilt or tightness. Treat non-operatively — a release gives unpredictable, often poor results.
Diagnostic criteria — all should be present.
- Excessive lateral patellar tilt on axial imaging (Merchant view or CT): the patella is tilted laterally with a tight lateral facet against the lateral femoral condyle.
- Objectively tight lateral retinaculum on examination: a reduced or absent medial glide (the patella cannot be translated medially the normal one to two quadrants) and a positive patellar tilt test (the lateral border cannot be lifted or everted to a normal angle).
- No lateral instability: a non-subluxating patella with a negative lateral glide and no apprehension — the patella does not translate laterally or dislocate.
- Lateral-facet overload on MRI (lateral-facet subchondral bone-marrow oedema, lateral-facet chondral loss) consistent with chronic lateral compression.
- Normal bony alignment: no significant trochlear dysplasia, a normal TT-TG distance, and normal patellar height — instability morphology is excluded. Clinical examination.
- Patellar tilt test: with the knee extended and the quadriceps relaxed, attempt to lift the lateral border of the patella. Normally the patella can be tilted so the lateral border rises to near or above the horizontal; a fixed lateral tilt that cannot be corrected indicates a tight lateral retinaculum.
- Medial glide test: translate the patella medially. Normal medial translation is about one to two quadrants of patellar width; a markedly reduced or absent medial glide confirms lateral tightness.
- Lateral glide and apprehension: translate the patella laterally. Excessive lateral translation with apprehension indicates instability — a contraindication to isolated release.
- Compression or grind (Clarke's) test: reproduces retropatellar pain in patellofemoral overload.
- Ober's test: assesses for iliotibial band tightness, which contributes to lateral retinacular tension. Imaging.
- Merchant (axial) view at 45 degrees flexion: assess tilt and subluxation, and the sulcus and congruence angles.
- Laurin lateral patellofemoral angle: a line along the lateral patellar facet and a line across the anterior femoral condyles. The angle normally opens (diverges) laterally; parallel lines, or an angle opening medially, indicate pathological lateral tilt.
- CT patellar tracking at 0, 15, 30 and 45 degrees flexion to confirm persistent tilt through a flexion arc.
- MRI: lateral-facet subchondral oedema and chondral loss consistent with overload, and critically to assess the MPFL, trochlear morphology and sulcus to exclude instability causes. Exclude instability morphology. The whole premise of an isolated release is that instability is absent, so the following should be normal: TT-TG distance less than 20 mm; Insall-Salvati ratio less than 1.2; sulcus angle less than 145 degrees with no crossing sign; Q angle less than 15 degrees in men and less than 20 degrees in women.
- Key finding
- Excessive lateral tilt, tight lateral retinaculum, reduced medial glide, negative lateral glide and no apprehension
- Correct procedure
- Lateral retinacular release or LENGTHENING
- Key finding
- MPFL deficiency, positive apprehension, lateral subluxation
- Correct procedure
- MPFL reconstruction (NOT isolated release)
- Key finding
- TT-TG greater than 20 mm or an excessive Q angle
- Correct procedure
- Tibial tubercle osteotomy (anteromedialisation) with or without MPFL reconstruction
- Key finding
- Insall-Salvati ratio greater than 1.2
- Correct procedure
- Tibial tubercle distalisation with or without MPFL reconstruction
- Key finding
- Lateral tilt preventing central tracking on top of MPFL deficiency
- Correct procedure
- MPFL reconstruction plus lateral LENGTHENING (avoid complete release)
- Key finding
- No objective lateral tightness
- Correct procedure
- Non-operative rehabilitation (NOT release)
Absolute indication. Symptomatic excessive lateral pressure syndrome with documented lateral tilt, an objectively tight lateral retinaculum, and no instability, that has failed an adequate non-operative programme (activity modification, quadriceps and vastus medialis obliquus rehabilitation, iliotibial band stretching, patellar taping or bracing over three to six months). Relative indications. An adjunct to a primary instability procedure (MPFL reconstruction or tibial tubercle transfer) where genuine objective lateral tightness would otherwise prevent central patellar tracking — increasingly performed as a lengthening rather than a complete release; and lateral retinacular pain with documented tilt in the setting of lateral-facet patellofemoral arthrosis. Contraindications. Absolute: patellar instability as the primary problem treated by an isolated LRR (the classic error — release does not stabilise the knee and can create iatrogenic medial instability); normal patellar tilt with no objective lateral tightness; active septic arthritis. Relative: generalised ligamentous laxity or multidirectional patellar laxity (high risk of over-release); complex regional pain syndrome tendency or hypersensitivity conditions; inflammatory arthropathy in an active flare. Consent. Counsel specifically on haemarthrosis (from the superior lateral geniculate vessel), the risk of iatrogenic medial instability if over-released, quadriceps weakness if the vastus lateralis tendon is injured, lateral hypoesthesia, and the narrowness of the indication (release will not correct instability if it coexists). Setup. Supine on a standard operating table with a lateral thigh post, the knee free to flex and extend through a full arc so patellar tracking can be assessed. A thigh tourniquet is optional. General or regional anaesthesia with local infiltration for post-operative analgesia. The release is almost always performed arthroscopically and is increasingly done as a lengthening when an isolated correction is intended.
The Operation
The goal: confirm at arthroscopy that this is genuine excessive lateral pressure syndrome, then divide the contracted lateral retinaculum from the superior pole of the patella to the tibial tubercle while sparing the vastus lateralis tendon and coagulating the superior lateral geniculate vessel, re-centring the patella without destabilising it medially. The exposure — portal placement, diagnostic confirmation and mapping the at-risk structures — is laid out inline as the first steps, because identifying the anatomy is the whole game (see also the knee arthroscopy approach).
Operative sequence
- Supine on a standard operating table with a lateral thigh post; the knee must be free to flex and extend through a full arc so patellar tracking can be assessed.
- Optional thigh tourniquet. General or regional anaesthesia with local infiltration for post-operative analgesia.
- Establish standard arthroscopy portals — anterolateral (viewing), anteromedial (working) and superolateral (the release instrument rests here, just deep to the lateral retinaculum).
- Cycle the knee through flexion and extension while viewing the patellofemoral joint: confirm lateral tilt with the lateral facet jammed against the lateral femoral condyle.
- Test tightness — a probe or the arthroscope cannot be passed beneath the tight lateral facet.
- Exclude instability and intra-articular pathology — assess the MPFL region, trochlear morphology, cartilage and menisci. If frank instability or significant malalignment is found, abandon the isolated release and revise the plan toward a medial reconstruction or a tubercle procedure.
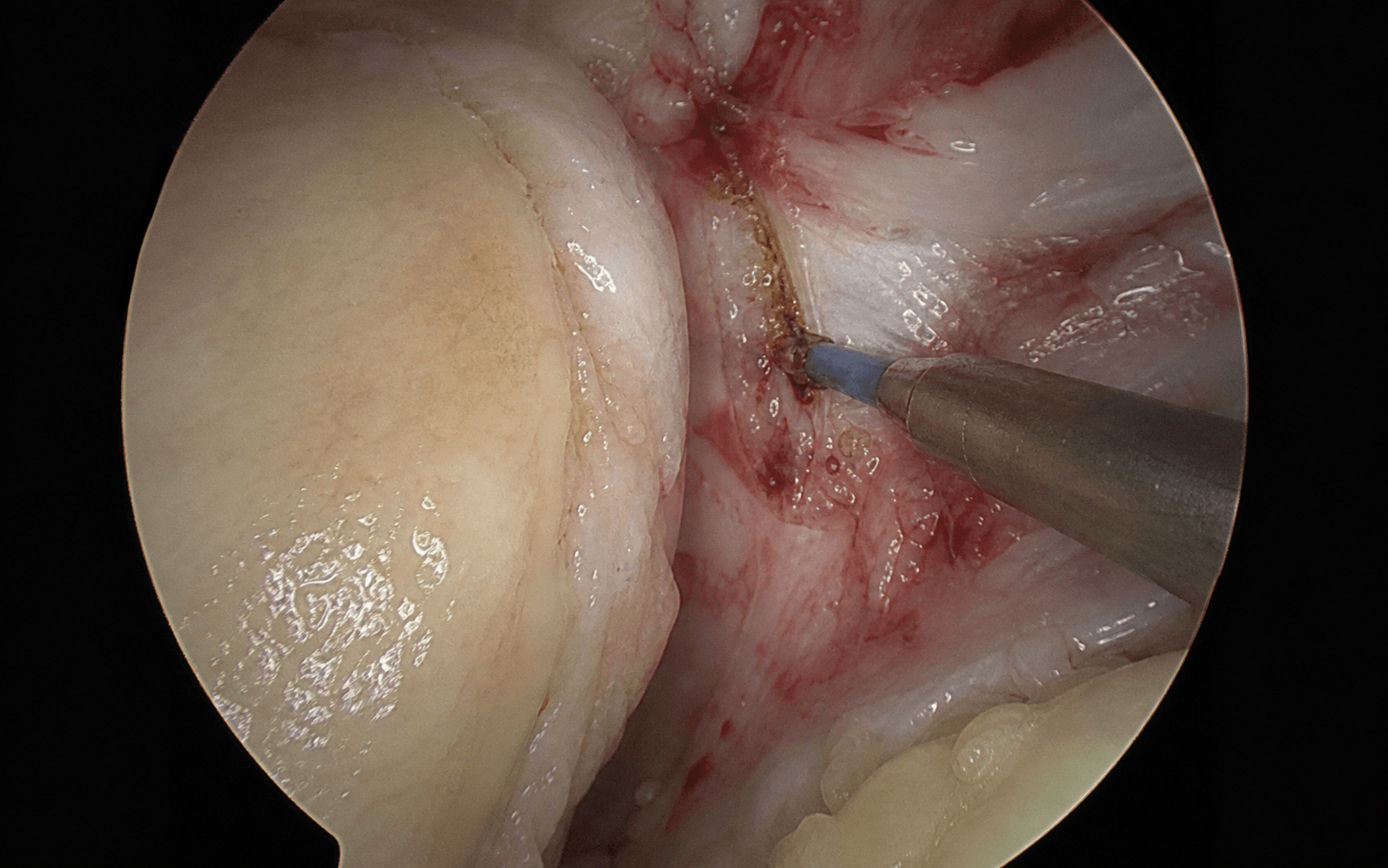
- Identify the white glistening vastus lateralis tendon at the superolateral corner of the patella — the structure you must SPARE. It blends with the proximal lateral retinaculum; cutting it weakens the extensor mechanism and removes a dynamic lateral stabiliser. Keep the release anterior and inferior to it.
- Locate the superior lateral geniculate artery and vein in the superolateral corner, near the vastus lateralis tendon — the leash you must COAGULATE. Division without coagulation is the principal cause of post-operative haemarthrosis.
- Appreciate the two layers you will divide — the superficial oblique layer (from the iliotibial band — the layer most often contracted) and the deep transverse layer (the deeper restraint). A complete release divides both; a lengthening preserves their continuity.
- With the knee in about 30 degrees of flexion, introduce arthroscopic scissors or an electrothermal hook probe through the superolateral portal, resting the instrument just deep to the lateral retinaculum at the level of the superior pole.
- Begin the release at the superolateral corner of the patella and carry the division distally along the lateral border of the patella, through the superficial oblique and deep transverse layers, to the level of the tibial tubercle and Gerdy's tubercle.
- Deliberately keep the cutting instrument against the retinaculum rather than diving into the subcutaneous fat (where the nerve branches run).
- Perform only the extent of release needed to correct the tilt — a limited release reduces the risk of over-release.
- The patella should now be easily tilted up (everted) to around 90 degrees and the medial glide restored to normal (one to two quadrants).
- Arthroscopically the lateral facet lifts off the lateral femoral condyle and the patella tracks centrally through the flexion arc.
- Avoid excess — if the patella can be dislocated medially, the release is too extensive.
- Re-check the superolateral corner under arthroscopic vision and confirm the geniculate vessels are sealed.
- Close the portal sites in the standard fashion and apply a compressive dressing.
- A longitudinal incision along the lateral border of the patella exposes the retinaculum directly.
- Divide the retinaculum in layers under direct vision from the superior pole to the tibial tubercle, with the same care to spare the vastus lateralis tendon and coagulate the geniculate vessel.
- Reserve the open approach for a combined open tubercle or reconstruction procedure, where it allows a precise, graduated release.
- Where an isolated lateral procedure is needed, a lengthening is increasingly preferred over a complete release because it corrects tilt while preserving lateral restraint, markedly reducing the risk of iatrogenic medial instability.
- Perform a Z-lengthening: divide the deep layer on one side and the superficial layer on the other, slide the two leaves apart to lengthen the retinaculum, and repair in the lengthened position.
- The result is a continuous but lengthened lateral retinaculum that re-centres the patella without leaving it unstable — the technique of choice when any element of instability or laxity is present.
- Cutting the vastus lateralis tendon — causes extensor weakness and iatrogenic medial instability; identify and protect it at the superolateral corner.
- Failing to coagulate the superior lateral geniculate vessel — the principal cause of post-operative haemarthrosis.
- Over-releasing distally and posteriorly — removes the lateral stabilising restraint and produces medial patellar instability.
- Releasing for instability rather than for tilt — the underlying medial deficiency is unaddressed and the knee is made worse.
Confirm at arthroscopy AND on the pre-operative imaging that this is genuine excessive lateral pressure syndrome — a tilted but non-subluxating patella with a tight lateral retinaculum and an intact medial side. If there is apprehension, a deficient MPFL or an increased TT-TG, an isolated release is the wrong operation: it will not help, and may harm, the patient.
Release from the superior pole downward, staying just lateral to the patella, holding the cutting instrument against the retinaculum rather than diving into the subcutaneous fat. Identify the white glistening vastus lateralis tendon at the top and keep the release below it, and coagulate the geniculate leash at the superior corner — this single step prevents most post-operative haemarthroses.
Aftercare & Complications
Rehabilitation principles. The goals are to prevent re-tethering of the released retinaculum, restore balanced quadriceps (especially vastus medialis obliquus) control, and offload the lateral facet while the patella re-centres. Phase 1 (weeks 0 to 2). Weight-bearing as tolerated with crutches for comfort, weaning as quadriceps control returns; early full active and passive range of motion; medial glide mobilisation exercises to prevent re-adhesion of the released retinaculum (a specific priority after release); quadriceps isometrics, straight-leg raise and vastus medialis obliquus retraining in pain-free ranges; ice and elevation for swelling with simple analgesia. Phase 2 (weeks 2 to 6). Progressive closed-chain quadriceps and hip-abductor strengthening; stationary cycling with the seat high to limit patellofemoral compression, progressing as pain allows; proprioception and balance work; continue patellar mobilisation and iliotibial band stretching (Ober stretch) if tight. Phase 3 (weeks 6 to return to sport). Sport-specific rehabilitation, a running progression and plyometrics. Return-to-sport criteria: pain-free with full range of motion, quadriceps strength at least 80 to 90 percent of the contralateral side, and no effusion. Bracing. A simple patellar-stabilising sleeve or brace may be used for comfort early on; prolonged rigid bracing is not required for an isolated release. When LRR is combined with another procedure. If the release is performed as an adjunct to MPFL reconstruction or a tibial tubercle osteotomy, rehabilitation is dictated by the primary procedure — protected range of motion, brace use, and weight-bearing or sport restrictions specific to the reconstruction or osteotomy. In the combined setting a lengthening is generally preferred over a complete release to protect the reconstructed medial restraint. Outcomes. In correctly selected patients (true excessive lateral pressure syndrome, no instability), release or lengthening reliably improves lateral retropatellar pain and lateral-facet overload. Outcomes are poor and unpredictable when the indication is broadened to nonspecific anterior knee pain or instability — which is why the indication is kept narrow. Complications
- Recognition
- Most common early complication — rapid knee swelling and tightness, pain and reduced flexion within hours
- Prevention and management
- Prevention: coagulate the superior lateral geniculate artery and vein at the superolateral corner; apply a compressive dressing. Management: most settle with elevation and ice; a tense haemarthrosis is aspirated under sterile conditions and re-compressed; occasional washout for refractory swelling
- Recognition
- The most feared late complication of over-release — medial patellar pain, a sensation of the patella falling medially or giving way, medial subluxation on examination, a reverse (medial) apprehension
- Prevention and management
- Prevention: keep the indication narrow; prefer a lengthening over a complete release; confirm the patella cannot be dislocated medially at the end. Management: rehabilitation plus lateral-support taping or bracing initially; for refractory cases, lateral retinacular reconstruction with a tendon graft or iliotibial band sling
- Recognition
- Persistent extensor lag and reduced quadriceps strength when the vastus lateralis tendon is injured; subjective weakness on stairs
- Prevention and management
- Prevention: identify and spare the vastus lateralis tendon at the superolateral corner. Management: structured quadriceps rehabilitation; tendon repair if transected and recognised intra-operatively
- Recognition
- Incomplete release — ongoing lateral retropatellar pain and persistent tilt on post-operative imaging
- Prevention and management
- Prevention: confirm adequacy intra-operatively (patella everts, medial glide restored, facet lifts off). Management: confirm the original diagnosis was correct; repeat non-operative measures; revision release only if there is unequivocal residual tightness
- Recognition
- Numbness or dysaesthesia over the lateral patella and proximal lateral leg
- Prevention and management
- Prevention: stay within the retinacular layer and avoid sweeping widely in the subcutaneous fat. Management: usually resolves or accommodates; a symptomatic neuroma rarely requires excision
- Recognition
- Disproportionate pain, swelling, stiffness and skin changes out of proportion to the procedure
- Prevention and management
- Prevention: avoid an over-extensive release; encourage early mobilisation; use multimodal analgesia. Management: early recognition, physiotherapy, desensitisation and pain-team input
- Recognition
- Low — clean arthroscopic surgery; erythema, warmth, discharge, fever
- Prevention and management
- Prevention: meticulous sterile technique. Management: wound swab and oral antibiotics such as cefalexin; arthroscopic washout if a deep infection is suspected
- Recognition
- Low — lower-extremity arthroscopy; calf pain and swelling, confirmed on ultrasound
- Prevention and management
- Prevention: early mobilisation and mechanical prophylaxis; chemoprophylaxis only for high-risk patients. Management: anticoagulation per protocol
Viva & Exam Focus
LATERALLATERAL — indication and assessment
DANGERDANGER — operative dangers and pitfalls
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old woman is referred requesting a lateral release for recurrent patellar dislocation — she has dislocated her right patella three times, most recently six weeks ago. Her MRI shows a deficient medial patellofemoral ligament and a TT-TG distance of 22 mm. How do you counsel her about the lateral release she is asking for?”
“A 38-year-old runner has a two-year history of lateral retropatellar pain. Examination shows a reduced medial glide and a fixed lateral tilt you cannot evert; there is no apprehension. Her axial radiograph shows lateral patellar tilt with a Laurin angle that opens medially; MRI shows lateral-facet subchondral oedema with an intact MPFL and a normal TT-TG. How do you manage her?”
“A 30-year-old woman is referred six months after a lateral retinacular release done elsewhere for patellofemoral pain. She now describes a new sensation of the patella falling inward, medial-sided knee pain and giving way. Examination shows the patella can be subluxed medially with little resistance. What has happened and how do you manage her?”
The narrow modern indication
- Excessive lateral pressure syndrome (lateral compression syndrome, Ficat) is the one clear indication: lateral tilt plus a tight lateral retinaculum plus lateral-facet overload plus NO instability
- All of: excessive lateral tilt on imaging, a reduced or absent medial glide, a non-subluxating patella with a negative lateral glide and no apprehension, lateral-facet overload on MRI, and normal bony alignment
- Only after failure of a documented three- to six-month non-operative programme
- The indication is deliberately narrow — broad use for anterior knee pain gave poor, unpredictable results
What LRR does NOT treat
- Lateral patellar instability (recurrent dislocation or subluxation) is NOT corrected by an isolated release
- Instability is driven by MPFL deficiency and/or bony malalignment (increased TT-TG, trochlear dysplasia, patella alta) — treat with MPFL reconstruction and/or tibial tubercle transfer
- An isolated release for instability is a historical error with high recurrence
- Isolated release can paradoxically cause iatrogenic MEDIAL patellar instability
Diagnosis of a tight lateral retinaculum
- Reduced or absent medial glide (normal is one to two quadrants medially) confirms lateral tightness
- Patellar tilt test: a fixed lateral tilt that cannot be everted indicates a tight lateral retinaculum
- Laurin lateral patellofemoral angle normally opens (diverges) laterally; parallel or medially-opening lines indicate pathological tilt
- Exclude instability: TT-TG less than 20 mm, Insall-Salvati ratio less than 1.2, sulcus angle less than 145 degrees, no apprehension
Surgical anatomy
- Lateral retinaculum has a superficial oblique layer (from the iliotibial band) and a deep transverse layer — both are divided in a complete release
- Vastus lateralis tendon inserts at the superolateral corner of the patella — SPARE it
- Superior lateral geniculate artery and vein run at the superolateral corner — COAGULATE to prevent haemarthrosis
- Iliotibial band sends fibres into the superficial layer and contributes to lateral tension (assess with Ober's test)
- Lateral femoral cutaneous nerve branches and the lateral patellar plexus are at risk of injury causing lateral hypoesthesia
Operative technique — key steps
- 1. Diagnostic arthroscopy first — confirm tilt with a tight, non-subluxating patella and exclude instability and intra-articular pathology
- 2. Map the field — identify the vastus lateralis tendon to spare and the superior lateral geniculate leash to coagulate
- 3. Arthroscopic inside-out release from the superolateral portal, beginning at the superior pole
- 4. Divide the retinaculum along the lateral patellar border to the tibial tubercle, through both layers
- 5. Confirm adequacy — the patella everts to around 90 degrees, the medial glide is restored, and the lateral facet lifts off
- 6. Avoid over-release — the patella must not be dislocatable medially
- 7. Prefer a Z-lengthening over a complete release when an isolated lateral procedure is needed
Lengthening vs release
- A Z-lengthening corrects tilt while preserving a continuous lateral restraint
- Lengthening is preferred wherever there is any element of instability, laxity, or where medial instability must be avoided
- A complete release is reserved for definite, isolated excessive lateral pressure syndrome and even then is increasingly avoided
- The shift from release to lengthening is driven by the recognised problem of iatrogenic medial instability
Dangers and complications
- Haemarthrosis from the superior lateral geniculate vessel — the most common early complication; prevent by coagulation
- Iatrogenic medial patellar instability — the most feared late complication of over-release; treat with lateral retinacular reconstruction if refractory
- Quadriceps weakness if the vastus lateralis tendon is cut — identify and protect it
- Persistent or recurrent tilt from incomplete release — confirm adequacy intra-operatively
- Lateral hypoesthesia, complex regional pain syndrome, infection and deep vein thrombosis are all uncommon
Rehabilitation
- Early full range of motion and weight-bearing as tolerated
- Medial patellar mobilisation is a specific priority to prevent re-tethering of the released retinaculum
- Vastus medialis obliquus and quadriceps retraining, plus hip-abductor strengthening
- Return to sport when pain-free with quadriceps strength at least 80 to 90 percent of the contralateral side
- If combined with MPFL reconstruction or a tibial tubercle osteotomy, follow the primary procedure's protocol
Background & Evidence
Pathoanatomy. The lateral retinaculum is a composite fibrous expansion anchoring the lateral border of the patella and patellar tendon to the iliotibial band and the lateral femoral condyle, with two functional layers: a superficial oblique layer (from the iliotibial band and deep fascia — the layer most often contracted in excessive lateral pressure syndrome) and a deep transverse layer (the deeper restraint, divided in a complete release). The iliotibial band attaches at Gerdy's tubercle on the tibia and sends fibres into the superficial layer; its tightness (assessed with Ober's test) contributes to lateral retinacular tension. The retinaculum balances the medial pull of the vastus medialis obliquus and the medial patellofemoral ligament; when contracted, the net lateral force tilts the patella laterally, increasing lateral-facet contact pressure and reducing medial-facet contact — the mechanism of lateral-facet overload, subchondral oedema and pain. Restoring balance by releasing or lengthening the tight lateral retinaculum re-centres the patella and offloads the lateral facet, but only when the medial restraint is intact — which is why instability must be excluded first. Small branches of the lateral femoral cutaneous nerve and the lateral patellar plexus traverse the subcutaneous tissue over the lateral retinaculum and are at risk of injury causing lateral hypoesthesia; the infrapatellar branch of the saphenous nerve is medial and not at risk in a lateral release. The shift away from broad lateral release. Early enthusiasm for lateral release across a broad range of patellofemoral complaints gave way to recognition that results are unpredictable unless the indication is restricted to true excessive lateral pressure syndrome (Fulkerson; Lattermann systematic review). For instability specifically, isolated release has been associated with high recurrence and inferior outcomes compared with medial-side reconstruction, and over-release producing iatrogenic medial patellar instability is now a recognised and difficult complication (Salvatore biomechanical study) — driving both the modern algorithm (MPFL reconstruction and/or tibial tubercle transfer for instability) and the trend toward lateral retinacular lengthening over complete release. Population-level data confirm a significant decline in isolated lateral release over the last decade (Huddleston). Non-operative treatment first. Most patellofemoral pain — including mild tilt — responds to a structured programme of quadriceps and hip-abductor strengthening, vastus medialis obliquus retraining, iliotibial band stretching, activity modification and patellar taping or bracing. Lateral release should be reserved for the small subgroup with objective lateral tilt and a tight lateral retinaculum who fail a documented three- to six-month non-operative programme.
References
Diagnosis and treatment of patients with patellofemoral pain
Defined the modern selective approach to patellofemoral disorders, emphasising that lateral release is appropriate only for objective lateral tilt; cautioned against lateral release for nonspecific patellofemoral pain, where results are unreliable; and reinforced the principle that instability is treated by medial-side reconstruction, not by lateral release.
An arthroscopic method for lateral release of subluxating or dislocating patella
The classic description of the arthroscopic lateral retinacular release performed from inside-out, establishing the minimally invasive technique that became the standard approach and defining the landmarks for an arthroscopic division of the lateral retinaculum along the lateral patellar border.
Lateral retinacular release for anterior knee pain: a systematic review of the literature
Systematic review of outcomes after lateral retinacular release for anterior knee pain, finding results are unpredictable and generally disappointing when the release is applied broadly without objective lateral tilt, supporting restriction of the indication to patients with documented excessive lateral pressure syndrome.
Lateral release with tibial tuberosity transfer alters patellofemoral biomechanics promoting multidirectional patellar instability
Biomechanical study demonstrating that lateral retinacular release combined with tibial tuberosity transfer significantly reduces patellar lateral restraint and promotes multidirectional patellar instability, quantifying the destabilising effect of over-release and supporting the trend toward lateral retinacular lengthening over complete release.
Trends in lateral retinacular release from 2010 to 2017
Population-level analysis showing a significant decline in isolated lateral retinacular release procedures over the study period, documenting the shift toward MPFL reconstruction and tibial tubercle osteotomy as preferred operations for patellofemoral instability and supporting the consensus that lateral release be reserved for true excessive lateral pressure syndrome without instability.