Medial utility incision | Saphenous protection | Artery of the tarsal canal | Medial malleolar osteotomy option
- The medial utility incision runs in the internervous interval between tibialis anterior (deep peroneal nerve) and tibialis posterior (tibial nerve).
- The saphenous vein and nerve lie about 1 to 2 cm anterior to the incision — identify and protect them throughout; injury causes medial foot numbness and a painful neuroma.
- The artery of the tarsal canal, a branch of the posterior tibial artery, is the dominant blood supply to the talar body — avoid aggressive dissection in the tarsal canal or you risk osteonecrosis.
- Preserve or repair the deltoid ligament — its deep fibres carry the deltoid branch that contributes to talar vascularity and to medial ankle stability.
- A medial malleolar osteotomy (oblique, from the malleolar tip into the plafond, fixed with two parallel 3.5 mm or 4.0 mm screws) extends exposure to the entire medial talar dome.
When & Why
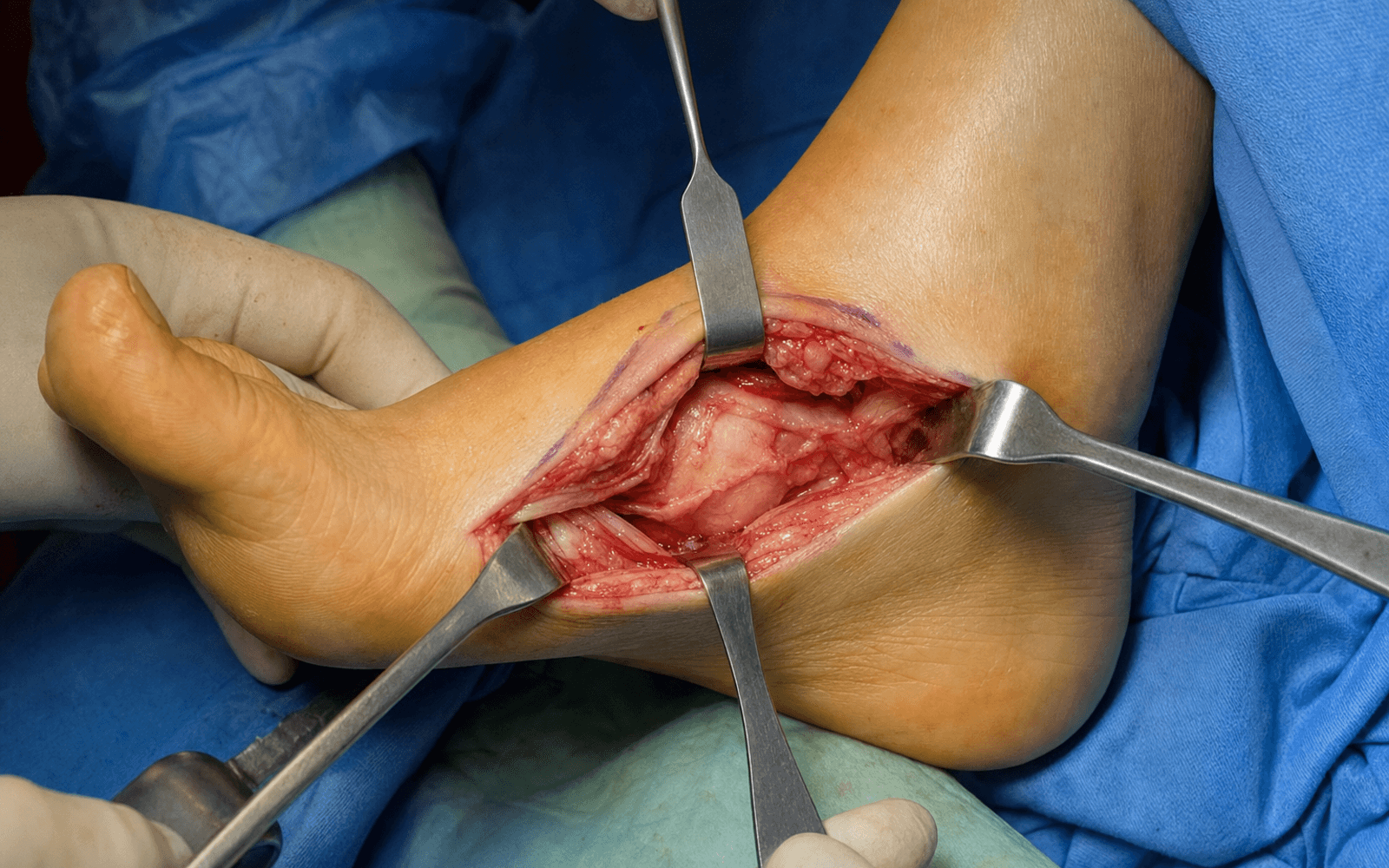
What it exposes. The medial utility incision gives direct access to the talar neck, the medial talar body and dome, the talonavicular joint and the navicular, with the option of a medial malleolar osteotomy to reach the medial talar dome. It is the workhorse medial exposure for talar neck ORIF, medial talar dome osteochondral lesions, talonavicular arthrodesis and navicular fracture fixation. Why medial. Displaced talar neck fractures commonly have medial comminution and a varus deformity that a lateral approach alone cannot fully control; the medial incision lets you see and buttress the medial neck directly. It is frequently combined with a lateral (Ollier) or anterolateral approach for complete exposure of comminuted patterns. Position & landmarks. Supine with a bump under the ipsilateral hip to internally rotate the foot, the knee slightly flexed (20 to 30 degrees), a tourniquet high on the thigh or below the knee, and the C-arm brought in from the contralateral side. Palpate and mark the medial malleolus, the navicular tuberosity, the tibialis anterior and posterior tibial tendons (the two borders of the incision), and the saphenous vein just anterior to the malleolus — the incision runs midway between the two tendons, from 2 cm proximal to the malleolar tip to the navicular tuberosity.
The Exposure
Work down through the layers between tibialis anterior and tibialis posterior, protecting the saphenous vein and nerve superficially and the artery of the tarsal canal deep, then open the capsule to display the talar neck, body and navicular.
Exposure sequence
- A longitudinal incision from about 2 cm proximal to the tip of the medial malleolus, extending distally to the navicular tuberosity (about 8 to 10 cm).
- Place it midway between the tibialis anterior tendon (anterior) and the posterior tibial tendon (posterior), slightly anterior to the malleolar tip, so it can be extended proximally along the tibia or distally to the first ray.
- Incise skin and subcutaneous tissue and identify the saphenous vein and nerve, which run about 1 to 2 cm anterior to the incision.
- Retract the neurovascular bundle gently anteriorly and protect it with a vessel loop; avoid ligating the main vein and avoid aggressive retraction that risks a painful neuroma.
- Incise the deep fascia in line with the skin and deepen the interval between tibialis anterior (deep peroneal nerve) anteriorly and tibialis posterior (tibial nerve) posteriorly.
- Retract tibialis anterior anteriorly and the posterior tibial tendon posteriorly — this is the safe internervous plane leading down to the capsule.
- Incise the capsule of the talonavicular joint and the medial ankle longitudinally, preserving the deltoid ligament attachment (detach only what is necessary for exposure and repair it at closure).
- The talar neck and body are exposed proximally and the navicular distally; protect the artery of the tarsal canal by avoiding aggressive dissection in the tarsal canal inferior to the talar neck.
- For access to the medial talar dome (osteochondral lesions, medial body fractures), perform an oblique medial malleolar osteotomy starting at the malleolar tip and directed proximally into the tibial plafond.
- The osteotomy is extra-articular and the deltoid ligament stays attached to the fragment, which is reflected inferiorly on this deltoid hinge to expose the entire medial talar dome.
- Distract or plantarflex the ankle to display the full medial talar dome, neck and the talonavicular and subtalar articular surfaces — ready for ORIF, OCD management or arthrodesis.
- Confirm reduction and fixation on fluoroscopy, aiming for less than 2 mm articular step-off and anatomic alignment of any osteotomy.
The artery of the tarsal canal, a branch of the posterior tibial artery, is the dominant blood supply to the talar body and enters the tarsal canal inferior to the talar neck; its deltoid branch runs through the deltoid ligament. Aggressive medial dissection that strips or ligates these vessels risks talar osteonecrosis. Superficially, the saphenous nerve lies only 1 to 2 cm anterior to the incision and is the structure most often injured — identify and protect it to avoid medial foot numbness and a painful neuroma.
All deep dissection stays on bone and extracapsular until you deliberately enter the joint. This protects the artery of the tarsal canal in the tarsal canal and keeps the deltoid ligament (and its deltoid branch) intact — preserving both medial ankle stability and talar body vascularity. When a medial malleolar osteotomy is needed, the deltoid stays attached to the fragment, so reflecting it inferiorly does not devascularise the talus.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Saphenous vein and nerve (1 to 2 cm anterior to the incision)
- Protection
- Identify early, retract gently anteriorly, vessel loop; do not ligate the main vein
- Structure at risk
- Tibialis anterior and posterior tibial tendons
- Protection
- Develop the plane between them; retract TA anteriorly and PTT posteriorly
- Structure at risk
- Deltoid ligament (deep and superficial components)
- Protection
- Preserve the attachment; detach only what is necessary and repair at closure
- Structure at risk
- Artery of the tarsal canal and its deltoid branch (dominant talar body supply)
- Protection
- Avoid aggressive dissection in the tarsal canal; stay on bone
- Structure at risk
- Talar dome and navicular cartilage
- Protection
- Blunt retractors, careful capsulotomy, protect cartilage
- Structure at risk
- Medial plantar nerve branches and posterior tibial insertion
- Protection
- Protect during navicular and first-ray exposure
Extensile options. Extend proximally along the medial border of the tibia (2 to 3 cm) to reach the medial tibial plafond and distal tibial metaphysis — useful for combined ankle and talar pathology or medial malleolar fractures. Extend distally along the medial border of the foot toward the first metatarsal base to expose the medial cuneiform and first tarsometatarsal joint for extended talonavicular fusion or midfoot reconstruction, protecting the posterior tibial insertion and medial plantar nerve branches. For comminuted talar neck fractures, combine with a lateral (Ollier or Kocher) or anterolateral approach for complete exposure and varus control. Closure. Closure is layered — repair the capsule and any detached deltoid fibres with absorbable suture, close the fascia and subcutaneous tissue, and close skin. Fix a medial malleolar osteotomy anatomically with two parallel 3.5 mm or 4.0 mm partially threaded cancellous screws directed perpendicular to the osteotomy plane and engaging the far tibial cortex, using washers in osteoporotic bone, and confirm reduction fluoroscopically with no step-off or gap. Apply a posterior splint or boot with the ankle neutral; patients are typically non-weight bearing for 6 to 12 weeks (longer for talar neck fractures and fusions), with serial radiographs to monitor healing and talar vascularity (Hawkins sign).
Procedures Through This Approach
- Talar neck ORIF — direct visualisation and reduction of medial neck comminution with medial buttress or lag screws; usually combined with a lateral approach for varus control.
- Medial talar dome OCD — microfracture, osteochondral autograft transfer (OATS) or fragment fixation, via a medial malleolar osteotomy.
- Talonavicular arthrodesis — isolated or as part of a triple arthrodesis; cartilage denudation, bone grafting and screw or plate fixation.
- Navicular fracture ORIF — body and tuberosity fractures, protecting the posterior tibial insertion.
- Medial talar body fractures and talar head or neck pathology — including tumour resection and bone grafting of cystic lesions.
Viva & Exam Focus
MEDIALMEDIAL — the talus and navicular exposure
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old male presents after a fall from height with a talar neck fracture. CT shows significant medial neck comminution and varus displacement. How would you approach this?”
“A 28-year-old athlete has a symptomatic medial talar dome osteochondral lesion that has failed conservative treatment. CT shows a 1.5 cm lesion with cystic changes. How would you access this?”
“A 55-year-old patient with talonavicular arthritis from prior trauma is indicated for isolated talonavicular arthrodesis. Describe the surgical approach and key technical points.”
References
Vascular supply to the talus
- Classic anatomic study defining the artery of the tarsal canal as the dominant blood supply to the talar body
- Described the deltoid branch contribution via the deltoid ligament
- Established the vascular basis for osteonecrosis risk after talar neck fractures
Talar neck fractures: classification and management
- Original classification of talar neck fractures into four types based on displacement and associated injuries
- Described the Hawkins sign as a radiographic indicator of talar vascularity
- Highlighted the high rate of osteonecrosis with increasing fracture displacement
Medial malleolar osteotomy for talar dome lesions
- Described the technique and outcomes of medial malleolar osteotomy for access to medial talar dome osteochondral lesions
- Demonstrated high rates of osteotomy union with screw fixation and anatomic reduction
- Emphasized preservation of the deltoid ligament attachment to maintain talar vascularity
Surgical approaches to the talus and navicular
- Comprehensive review of surgical approaches to the talus and navicular including the medial utility incision
- Discussed indications for combined medial and lateral approaches in comminuted talar neck fractures
- Highlighted the importance of protecting the artery of the tarsal canal during medial dissection
Talonavicular arthrodesis: technique and outcomes
- Described the medial approach for talonavicular joint preparation and fixation
- Reported union rates and functional outcomes after isolated talonavicular fusion
- Emphasized bone grafting and rigid internal fixation as key technical factors