Lag screw fixation of reducible Type II and high Type III odontoid fractures, preserving C1-C2 rotation | advanced
- Indications require a favourable fracture line (posterior-oblique or transverse), a reducible fracture, a competent transverse atlantal ligament and adequate bone stock; anterior-oblique patterns, comminution, established nonunion and osteoporosis are contraindications.
- The screw trajectory is steep caudal-to-cranial (approximately 15-20 degrees) under simultaneous anteroposterior and lateral fluoroscopy; the entry point is at the anterior inferior C2 body aiming for the odontoid tip.
- One or two 3.5-4.0 mm partially threaded lag screws are placed; two screws provide greater rotational stability but the second screw is technically demanding and increases the risk of cortical breach.
- Intraoperative assessment of the transverse atlantal ligament (TAL) is mandatory; if the TAL is incompetent or the fracture is irreducible, the procedure must be abandoned in favour of posterior C1-C2 fusion.
- “The fracture line orientation on the lateral radiograph or CT sagittal reconstruction dictates screw suitability: posterior-oblique or transverse patterns allow compression; anterior-oblique patterns cause the screw to distract the fracture and are absolute contraindications.
- “Transverse atlantal ligament competency is confirmed on preoperative MRI (STIR sequence) or by intraoperative stress testing under fluoroscopy; an atlanto-dens interval greater than 3 mm on lateral flexion-extension views indicates TAL insufficiency.
- “Barrel chest or short neck anatomy prevents the required caudal trajectory; these patients are better served by posterior C1-C2 fusion (Harms-Goel technique).
- “Postoperative immobilisation is a rigid cervical collar for 6-12 weeks; halo vest is reserved for poor bone quality or when screw purchase is marginal — early mobilisation reduces pulmonary complications.
When & Why
Indication. Anterior odontoid screw fixation is a motion-preserving operation for an acute Type II odontoid fracture (or a high Type III fracture extending into the C2 body) with a favourable fracture line — posterior-oblique or transverse on the sagittal CT — that is reducible and has an intact transverse atlantal ligament, in a patient with adequate bone stock and a body habitus that allows the required steep caudal-to-cranial trajectory. It is chosen when preserving C1-C2 rotation (approximately 50 percent of total cervical rotation) matters — most often in younger, active patients. Absolute indications
- Acute Type II odontoid fracture with favourable (posterior-oblique or transverse) fracture line
- High Type III odontoid fracture extending into the C2 body with adequate bone stock for screw purchase
- Reducible fracture with intact transverse atlantal ligament
- Patient preference for motion-preserving surgery over C1-C2 arthrodesis Relative indications
- Selected chronic nonunions with good bone quality and favourable anatomy (requires bone grafting)
- Young patients in whom preservation of C1-C2 rotation is functionally important
- Polytrauma patients where shorter operative time and avoidance of prone positioning is desirable Contraindications. The single most important selection factor is the fracture line orientation: an anterior-oblique line lets the lag screw distract rather than compress the fragment and is an absolute contraindication. Absolute
- Anterior-oblique fracture line orientation (screw distracts rather than compresses)
- Comminuted odontoid fracture or large fracture gap
- Established nonunion with sclerotic fracture edges
- Incompetent transverse atlantal ligament (atlanto-dens interval greater than 3 mm)
- Irreducible fracture on preoperative traction or positioning
- Severe osteoporosis (T-score less than -2.5) or metabolic bone disease
- Barrel chest or short neck preventing adequate caudal trajectory Relative
- Previous anterior cervical surgery with scarring
- Active infection
- Severe dysphagia or airway compromise preoperatively Anterior screw versus posterior C1-C2 fusion — the decision. When the fracture pattern, the TAL and the anatomy all favour it, anterior screw fixation is preferred because it preserves C1-C2 rotation. When any of those fails, the answer is posterior C1-C2 fusion (Harms-Goel), which is reliable and union rates are greater than 95 percent, but it sacrifices all C1-C2 rotation.
- Anterior odontoid screw
- Posterior-oblique or transverse only
- Posterior C1-C2 fusion (Harms-Goel)
- Any pattern
- Anterior odontoid screw
- Must be competent
- Posterior C1-C2 fusion (Harms-Goel)
- Not required
- Anterior odontoid screw
- Yes (approximately 50 percent of normal)
- Posterior C1-C2 fusion (Harms-Goel)
- No (0 degrees)
- Anterior odontoid screw
- 85-95 percent
- Posterior C1-C2 fusion (Harms-Goel)
- Greater than 95 percent
- Anterior odontoid screw
- Higher
- Posterior C1-C2 fusion (Harms-Goel)
- Lower
- Anterior odontoid screw
- Supine
- Posterior C1-C2 fusion (Harms-Goel)
- Prone
- Anterior odontoid screw
- Adequate neck extension, no barrel chest
- Posterior C1-C2 fusion (Harms-Goel)
- Any body habitus
- Anterior odontoid screw
- Collar 6-12 weeks
- Posterior C1-C2 fusion (Harms-Goel)
- Collar or halo 8-12 weeks
Consent specifically for screw malposition, vertebral artery injury, oesophageal perforation, dysphagia, nonunion, hardware failure, the possibility of intraoperative conversion to posterior fusion, and the need for a postoperative collar or halo.
The Operation
The goal: reduce the fracture, expose the anterior C2 body through the high Smith-Robinson approach at C2-C3, and drive a lag screw from the anterior inferior C2 body up into the odontoid tip under continuous biplanar fluoroscopy — compressing the fracture while protecting the vertebral artery, the oesophagus and the spinal cord. The exposure is laid out in full as the first steps below (and in depth on the Smith-Robinson anterior cervical spine approach page).
Operative sequence
- Supine on a radiolucent table, head secured in a Mayfield clamp or Gardner-Wells tongs; apply 5-10 lb of traction to reduce the fracture.
- Slight neck extension (10-15 degrees) opens the C2-C3 disc space and improves the caudal-to-cranial trajectory; confirm the chest does not obstruct the fluoroscopic beam.
- Two C-arm fluoroscopes positioned for simultaneous true lateral (odontoid in profile) and anteroposterior open-mouth views. The AP view must show the medial walls of the C2 pedicles clearly. Confirm both planes are obtainable before draping — if you cannot get the trajectory intraoperatively, do not start.
- General endotracheal anaesthesia with a nasogastric tube in place for oesophageal identification; neuromonitoring (MEP/SSEP) is optional but recommended for high-risk cases.
- Right-sided transverse skin incision at the C2-C3 level, approximately two fingerbreadths below the mandible. A right-sided approach is conventional to avoid the left recurrent laryngeal nerve looping around the aortic arch.
- Divide the platysma sharply. The prevertebral fascia is thicker at this level than in a standard subaxial Smith-Robinson exposure and will need sharp dissection later.
- Develop the avascular plane between the carotid sheath laterally and the trachea/oesophagus medially, working up to the anterior cervical spine under direct vision.
- The oesophagus and trachea lie directly medial to this high exposure; the nasogastric tube aids oesophageal identification. Place blunt self-retaining retractors and relax retraction every 15-20 minutes to reduce oesophageal pressure and dysphagia risk.
- Identify the carotid sheath laterally and protect it with blunt retractors.
- Incise the prevertebral fascia in the midline and elevate the longus colli muscles laterally to expose the anterior inferior C2 body and the C2-C3 disc.
- Confirm the entry point: the most anterior-inferior corner of the C2 body on the true lateral view. The odontoid tip is the target on both views; screw length is typically 35-45 mm depending on patient size (the odontoid tip sits approximately 15-20 mm above the C1 anterior arch).
- At risk in this exposure: the oesophagus (medial — prolonged retraction drives dysphagia), the trachea and endotracheal tube (anterior — gentle intermittent retraction), the carotid sheath (lateral), and the recurrent laryngeal nerve (right side). The vertebral artery is not directly in the field but is endangered by a laterally directed screw through the C2 lateral mass.
- Confirm fracture reduction on biplanar fluoroscopy before any bone work.
- Confirm transverse atlantal ligament (TAL) competency: preoperative MRI (STIR sequence) or intraoperative stress testing under fluoroscopy. An atlanto-dens interval greater than 3 mm indicates TAL insufficiency — if the TAL is incompetent or the fracture is irreducible, abort and convert to posterior C1-C2 fusion.
- Create a small cortical window at the anterior inferior C2 body with a high-speed burr.
- Insert the guidewire under continuous lateral fluoroscopy, aiming 15-20 degrees cephalad toward the odontoid tip.
- Check the AP view every 5-10 mm of advancement to ensure the wire stays medial to the C2 pedicle walls — never rely on lateral imaging alone, because lateral breach is how the vertebral artery is injured.
- Measure screw length on preoperative CT and confirm with intraoperative fluoroscopy.
- Overdrill the near cortex only (lag technique) so the screw threads engage the odontoid fragment while the smooth shank crosses the fracture line.
- Insert one (or two) 3.5-4.0 mm partially threaded cannulated lag screw(s). Two screws provide greater rotational control but increase technical difficulty and cortical breach risk.
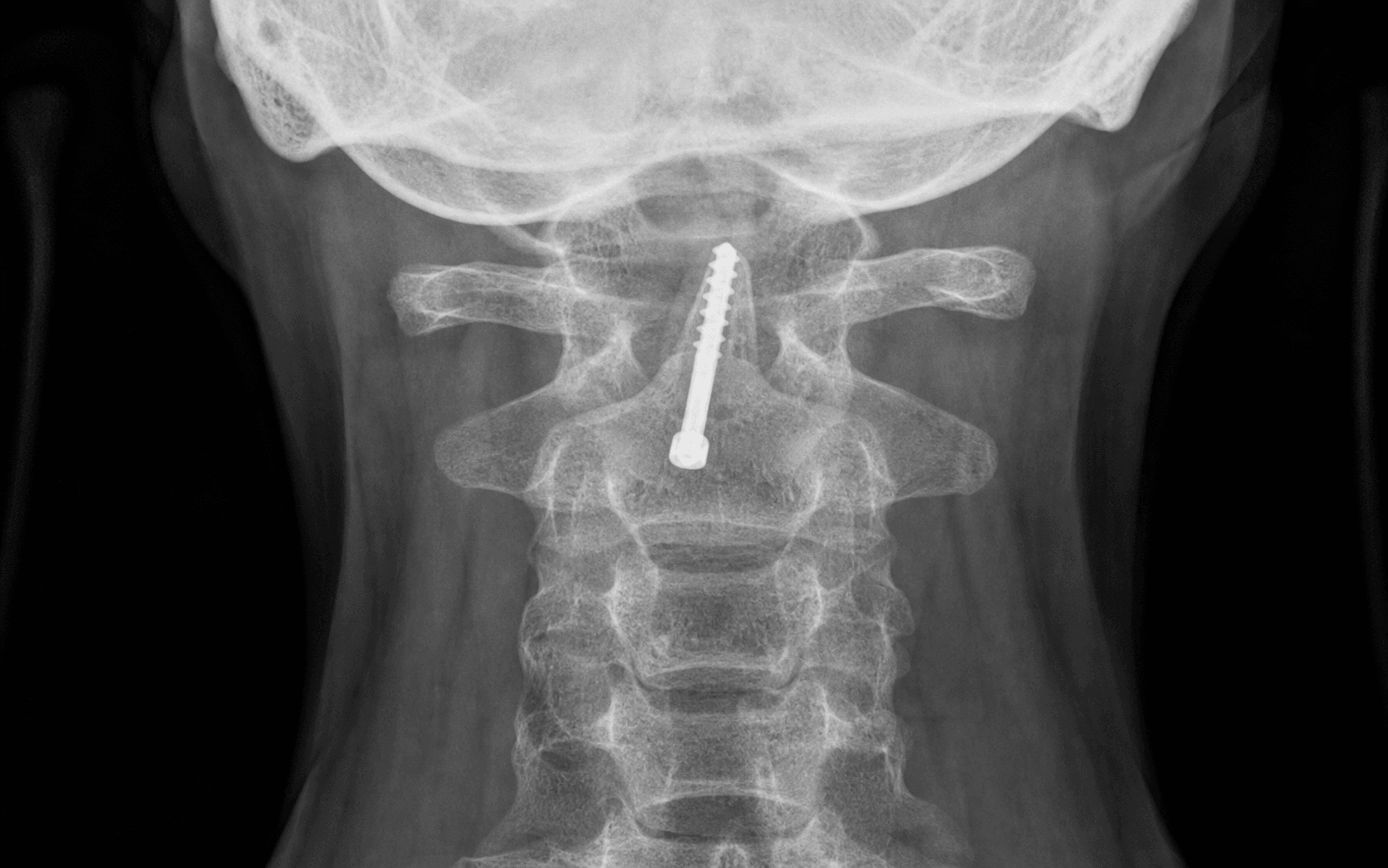
- Confirm final screw position on both AP and lateral fluoroscopy: threads engaged in the odontoid tip cortical bone, shank across the fracture, no anterior C2 cortex breach, no lateral pedicle wall breach.
- Perform gentle flexion-extension stress testing to confirm stability; supplement with a collar or halo if purchase is marginal.
- Irrigate thoroughly. Close the platysma with absorbable suture and the skin with a subcuticular absorbable suture or staples.
- A drain is not routinely required. Apply a rigid cervical collar before emergence.
- Rigid cervical collar for 6-12 weeks. Serial radiographs at 2, 6 and 12 weeks; CT at 12 weeks to confirm union before discontinuing immobilisation.
- Halo vest is reserved for marginal screw purchase or poor bone quality.
- Anterior-oblique fracture line: the screw will distract rather than compress — abort and convert to posterior fusion.
- Incompetent TAL: stress testing under fluoroscopy or preoperative MRI is mandatory; if the atlanto-dens interval is greater than 3 mm, abort.
- Lateral screw trajectory: risks vertebral artery injury — confirm the medial wall of the C2 pedicle on the AP view throughout.
- Inadequate odontoid tip purchase: measure screw length precisely; the tip must engage cortical bone.
Obtain true lateral and open-mouth AP views before making the skin incision. The entry point is the most anterior-inferior corner of the C2 body on the lateral view. Advance the guidewire under continuous lateral imaging and check the AP view every 5-10 mm to stay medial to the C2 pedicle walls. If the required caudal-to-cranial angle cannot be achieved because of chest morphology, abort immediately and reposition for posterior C1-C2 fusion.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Activity & monitoring | |-------|--------|----------------|------------------------| | 1 | Day 0 to 2 weeks | Rigid collar (Philadelphia or Miami J) at all times except for hygiene | Sit up day of surgery; ambulate with assistance day 1; formal speech-therapy swallow assessment before oral intake; day-1 lateral radiograph and CT before discharge | | 2 | 2 to 6 weeks | Collar full-time; remove only for supervised showering | Light activity; no lifting greater than 5 kg; no driving; 2-week wound check and radiograph | | 3 | 6 to 12 weeks | Discontinue at 6-12 weeks if radiographs show stable fixation and fracture-line blurring | CT at 12 weeks to confirm union; gentle range-of-motion after collar removal; avoid forced flexion-extension for 3 months | | Return to function | — | — | Light work at 6-8 weeks; manual work or contact sport at 3-6 months after CT-confirmed union; annual flexion-extension radiographs for 2 years to monitor for late instability | Complications
- Incidence
- 3-6 percent
- Recognition
- Immediate postoperative CT shows screw breaching the C2 pedicle or transverse foramen; vertebral artery injury may present with stroke or bleeding
- Prevention and management
- Prevention: continuous biplanar fluoroscopy; stay medial to the C2 pedicle wall on the AP view. Management: if recognised intraoperatively, redirect the screw or convert to posterior fusion; postoperative vertebral artery injury requires urgent angiography and possible embolisation or stenting
- Incidence
- 2-4 percent
- Recognition
- Screw tip or shank breaches the anterior C2 cortex; may cause oesophageal erosion or infection
- Prevention and management
- Prevention: confirm entry point and trajectory on the true lateral view; do not over-advance. Management: if recognised intraoperatively, redirect; if postoperative oesophageal injury is suspected, urgent contrast swallow and ENT consultation
- Incidence
- 1-3 percent
- Recognition
- Intraoperative perforation recognised by air leak or nasogastric-tube visualisation; postoperative dysphagia, fever, neck swelling, crepitus
- Prevention and management
- Prevention: right-sided approach, intermittent retractor relaxation, nasogastric-tube identification. Management: intraoperative repair if recognised; postoperative perforation requires urgent exploration, drainage, antibiotics and possible diversion
- Incidence
- 10-15 percent
- Recognition
- Difficulty swallowing solids or liquids; aspiration risk; weight loss
- Prevention and management
- Prevention: gentle retraction, high approach technique, early mobilisation. Management: speech therapy, modified diet, nasogastric feeding if severe; most resolve by 6-8 weeks; persistent dysphagia warrants ENT evaluation
- Incidence
- 5-15 percent
- Recognition
- Persistent fracture line at 3 months; screw cut-out or breakage; increasing atlanto-dens interval
- Prevention and management
- Prevention: appropriate patient selection (acute fracture, good bone quality, competent TAL); two-screw construct in marginal bone. Management: revision anterior surgery with bone grafting or conversion to posterior C1-C2 fusion with autograft
- Incidence
- Less than 1 percent
- Recognition
- Intraoperative bleeding from lateral breach; postoperative stroke, Horner syndrome or subarachnoid haemorrhage
- Prevention and management
- Prevention: strict adherence to the AP medial-wall landmark; preoperative CT angiography to map the vertebral artery course. Management: immediate tamponade, reversal of anticoagulation, urgent angiography; endovascular or open repair as indicated
- Incidence
- 1-2 percent
- Recognition
- Progressive neck swelling, stridor, desaturation in recovery
- Prevention and management
- Prevention: meticulous haemostasis, drain if bleeding risk is high, close observation in recovery. Management: immediate re-intubation, surgical exploration and evacuation of the haematoma
- Incidence
- Less than 2 percent
- Recognition
- Wound erythema, drainage, fever, elevated CRP or white cell count
- Prevention and management
- Prevention: prophylactic antibiotics, meticulous sterile technique. Management: superficial infection — oral antibiotics; deep infection — surgical washout, IV antibiotics, possible hardware removal if loose
Special case — intraoperative conversion to posterior C1-C2 fusion. Convert when the fracture is irreducible after positioning, the TAL is incompetent on stress testing (atlanto-dens interval greater than 3 mm), an anterior-oblique fracture line is discovered on final fluoroscopy, screw purchase in osteoporotic bone is inadequate, or a barrel chest prevents an acceptable trajectory. Technique: close the anterior wound temporarily, flip to prone on a Jackson table with the Mayfield clamp, perform Harms-Goel C1-C2 posterior fusion (C1 lateral mass screws, C2 pedicle or pars screws, rod fixation) with iliac crest autograft, then close the anterior wound. Special case — chronic odontoid nonunion. Anterior screw fixation alone has lower union rates (60-70 percent) in established nonunions. Consider anterior screw plus autograft (from iliac crest or the C2 body) packed into the fracture site. If bone quality is poor or the TAL is incompetent, prefer primary posterior C1-C2 fusion with autograft. Preoperative CT assesses the fracture gap and sclerosis; MRI confirms TAL status.
Viva & Exam Focus
S.C.R.E.W.S.C.R.E.W. — patient selection for anterior odontoid screw
T.R.A.J.E.C.T.T.R.A.J.E.C.T. — critical intraoperative steps
The trap: assuming any Type II fracture is suitable for anterior screw fixation. Only posterior-oblique or transverse fracture lines allow lag-screw compression; anterior-oblique patterns push the odontoid fragment superiorly and are an absolute contraindication — convert to posterior C1-C2 fusion.
Location: the TAL runs behind the odontoid and is the primary restraint to anterior atlanto-axial subluxation. Undiagnosed rupture allows persistent instability even after a technically perfect screw; the construct fails in flexion. Always obtain a preoperative MRI or perform intraoperative stress fluoroscopy.
Location: the vertebral artery ascends in the C2 transverse foramen and lies lateral to the intended screw path. A laterally directed or excessively long screw can breach the C2 lateral mass or transverse foramen, causing vertebral artery injury, stroke or death. Use simultaneous biplanar fluoroscopy and stay within the medial C2 pedicle walls on the AP view.
The trap: proceeding when the required caudal trajectory cannot be achieved. These patients have an unacceptably steep screw angle that risks anterior C2 body breach or inadequate odontoid purchase — convert to posterior Harms-Goel C1-C2 fusion.
Severe osteoporosis (T-score less than -2.5) or metabolic bone disease compromises screw purchase in the odontoid tip and C2 body — high risk of cut-out, nonunion or hardware failure. Consider posterior fusion with C1 lateral mass and C2 pedicle or pars screws, or augment with bone graft and longer immobilisation.
Location: the high anterior cervical approach places the oesophagus and trachea immediately medial to the exposure. Retraction injury, perforation or postoperative dysphagia is more common than in standard Smith-Robinson exposures because of the high level (C2-C3) and prolonged retraction. Use a right-sided approach, intermittent relaxation of retractors and a nasogastric tube for identification.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old man sustains a Type II odontoid fracture after a fall from height. Sagittal CT shows a posterior-oblique fracture line at the base of the dens with 3 mm displacement. MRI confirms an intact transverse atlantal ligament. He has no chest deformity and good bone density. What is your surgical plan and why?”
“You are performing anterior odontoid screw fixation on a 35-year-old woman. After guidewire placement you notice on the AP fluoroscopic view that the wire has drifted 3 mm lateral to the medial wall of the C2 pedicle. What do you do?”
“A 68-year-old man with a Type II odontoid fracture undergoes successful anterior odontoid screw fixation. At 12-week follow-up CT shows a persistent fracture line with 2 mm screw cut-out. How do you manage this nonunion?”
Key indications
- Acute Type II or high Type III odontoid fracture with posterior-oblique or transverse fracture line
- Reducible fracture with competent transverse atlantal ligament (atlanto-dens interval less than 3 mm)
- Good bone quality (T-score greater than -2.5) and suitable body habitus (no barrel chest)
- Young patient in whom preservation of C1-C2 rotation is functionally important
- Contraindications: anterior-oblique pattern, comminution, nonunion, TAL rupture, osteoporosis, poor trajectory anatomy
Critical anatomy
- Odontoid blood supply enters via the alar and apical ligaments; the base is a watershed zone contributing to nonunion
- The transverse atlantal ligament is the primary restraint; rupture allows an atlanto-dens interval greater than 3 mm
- Entry point: anterior inferior corner of the C2 body on true lateral fluoroscopy
- Trajectory: 15-20 degrees cephalad; the target is the odontoid cortical tip
- The vertebral artery lies lateral to the C2 pedicle; the AP view must keep the screw medial to the pedicle wall
Surgical approach
- Right-sided high Smith-Robinson at the C2-C3 level; transverse incision two fingerbreadths below the mandible
- Develop the plane between the carotid sheath (lateral) and the trachea/oesophagus (medial)
- A nasogastric tube aids oesophageal identification; relax retractors every 15-20 minutes
- Expose the anterior inferior C2 body; create a cortical window with a burr for guidewire entry
Operative technique — key steps
- 1. Supine with Mayfield clamp, slight neck extension, 5-10 lb traction; confirm reduction on biplanar fluoro
- 2. Two C-arms: true lateral (odontoid profile) and AP open-mouth (medial C2 pedicle walls)
- 3. Right high anterior cervical approach; identify and protect the recurrent laryngeal nerve and oesophagus
- 4. Entry at the anterior inferior C2 body; advance the guidewire 15-20 degrees cephalad under continuous lateral imaging
- 5. Check the AP view every 5-10 mm to stay medial to the C2 pedicle wall (avoid the vertebral artery)
- 6. Measure screw length; overdrill the near cortex only; insert a 3.5-4.0 mm partially threaded lag screw
- 7. Confirm final position and stability with flexion-extension stress testing before closure
- 8. Rigid collar for 6-12 weeks; CT at 12 weeks to confirm union
Danger zones
- Anterior-oblique fracture line: the screw distracts rather than compresses — absolute contraindication
- Incompetent TAL: atlanto-dens interval greater than 3 mm on stress testing — abort and convert to posterior fusion
- Lateral screw trajectory: vertebral artery injury — confirm the medial C2 pedicle wall on the AP view throughout
- Barrel chest or short neck: prevents the required caudal trajectory — convert to posterior Harms-Goel fusion
- Osteoporosis: poor purchase and cut-out risk — consider a two-screw construct or posterior fusion
Complications
- Screw malposition (lateral): 3-6 percent — vertebral artery injury; requires biplanar confirmation at every step
- Oesophageal injury: 1-3 percent — right-sided approach, nasogastric tube, intermittent retraction reduce risk
- Dysphagia: 10-15 percent — usually transient; speech therapy and modified diet; most resolve by 6-8 weeks
- Nonunion: 5-15 percent — higher in elderly, chronic fractures, marginal bone; revision to posterior fusion
- Vertebral artery injury: less than 1 percent — catastrophic; prevent with strict AP landmark adherence
Post-operative care
- Rigid cervical collar full-time for 6-12 weeks; remove only for hygiene under supervision
- Serial radiographs at 2, 6 and 12 weeks; CT at 12 weeks before collar discontinuation
- Halo vest reserved for marginal screw purchase or poor bone quality
- Light work at 6-8 weeks; contact sports at 3-6 months after CT union confirmation
- Intraoperative conversion to posterior C1-C2 fusion if the TAL is incompetent, the fracture irreducible, or the trajectory impossible
Evidence summary
- Union rate 85-95 percent for acute fractures with appropriate selection; lower (60-70 percent) for chronic nonunions
- Two-screw constructs have a lower nonunion rate but a higher technical complication rate
- Posterior C1-C2 fusion (Harms-Goel) has union greater than 95 percent but eliminates C1-C2 rotation
- MRI (STIR) is highly accurate for TAL integrity; an atlanto-dens interval greater than 3 mm is a reliable surrogate
- Overall complication rate approximately 17 percent; dysphagia, screw malposition and nonunion are most common
Background & Evidence
Classification. Odontoid fractures are classified by the Anderson and D'Alonzo system by the level of the fracture line, which is the key determinant of healing potential and the principal driver of the decision to fix anteriorly.
- Location
- Tip of the odontoid (above the transverse ligament)
- Stability and healing
- Rare; usually stable
- Typical management
- Conservative immobilisation in most cases
- Location
- Base of the dens (junction with the C2 body) — the watershed zone
- Stability and healing
- Highest nonunion rate with non-operative treatment (up to 30-50 percent); the primary surgical indication
- Typical management
- Anterior screw fixation if the pattern is favourable, otherwise posterior C1-C2 fusion
- Location
- Extends into the C2 vertebral body
- Stability and healing
- Better blood supply; lower nonunion rate
- Typical management
- Often conservative, or fixation if displaced
Pathoanatomy. The odontoid process is the superior projection of the C2 vertebral body; it articulates with the anterior arch of C1 and the transverse atlantal ligament posteriorly. Its blood supply enters via the alar and apical ligaments (ascending pharyngeal and vertebral artery branches), leaving the base of the dens as a watershed zone — the reason Type II fractures carry the highest nonunion rate. The transverse atlantal ligament (TAL) is the primary restraint to anterior atlanto-axial translation, running behind the odontoid in the transverse groove; rupture allows an atlanto-dens interval greater than 3 mm. The alar ligaments (odontoid to the occipital condyles) and the apical ligament (odontoid tip to the foramen magnum) are secondary restraints, with the anterior and posterior atlanto-axial membranes contributing further stability. Key evidence. Apfelbaum's prospective series of 147 patients reported an overall union rate of 88 percent for acute fractures, falling to 65 percent for chronic nonunions; two-screw constructs had a lower nonunion rate than single-screw fixation, with screw malposition in 6 percent and transient dysphagia in 12 percent. The pooled systematic-review evidence (Koller) puts the overall complication rate at about 17 percent — dysphagia, screw malposition and nonunion being most common, with vertebral artery injury and oesophageal perforation rare (less than 1 percent) but potentially catastrophic. MRI (STIR) is highly accurate for TAL integrity, and an atlanto-dens interval greater than 3 mm is a reliable surrogate for insufficiency. Posterior C1-C2 fusion (Harms-Goel) achieves union greater than 95 percent but eliminates C1-C2 rotation — which is precisely why careful anterior-screw selection matters.
References
Direct anterior screw fixation for recent and remote odontoid fractures
- Prospective series of 147 patients undergoing anterior odontoid screw fixation
- Overall union rate 88 percent for acute fractures; lower (65 percent) for chronic nonunions
- Two-screw constructs had a lower nonunion rate than single-screw fixation; complications included screw malposition (6 percent) and transient dysphagia (12 percent)
Fractures of the odontoid process of the axis
- Classic classification of odontoid fractures into Type I (tip), Type II (base) and Type III (body extension)
- Type II fractures have the highest nonunion rate with non-operative treatment (up to 30-50 percent)
- Established the fracture line location as the key determinant of healing potential
Anterior screw fixation of odontoid fractures: operative technique and results in 18 patients
- Early description of the anterior odontoid screw technique in 18 patients
- Emphasised the importance of fracture line orientation and adequate bone stock
- Reported high union rates when patient selection criteria were followed
MRI assessment of the transverse atlantal ligament in odontoid fractures
- Prospective evaluation of MRI for TAL integrity in 22 patients with odontoid fractures
- MRI (STIR sequence) had 100 percent sensitivity and 94 percent specificity for TAL rupture compared with intraoperative findings
- TAL rupture correlated with an atlanto-dens interval greater than 3 mm on stress radiographs
Complications of anterior odontoid screw fixation: a systematic review
- Pooled analysis of 12 series comprising 452 patients
- Overall complication rate 17 percent; most common were dysphagia (9 percent), screw malposition (5 percent) and nonunion (8 percent)
- Vertebral artery injury and oesophageal perforation were rare (less than 1 percent) but potentially catastrophic