Deltopectoral approach with subscapularis takedown and capsulolabral repair · intermediate
- Indications for open repair: failed arthroscopic Bankart (most common), revision stabilisation, glenoid bone loss 15–20%, an engaging Hill-Sachs requiring remplissage, and contact or collision athletes wanting the lowest possible recurrence rate.
- Subscapularis management has three options — lesser-tuberosity osteotomy (bone-to-bone healing, most robust construct), peel (a balanced default), and tenotomy (simplest). Comparative clinical series show similar outcomes, but peel or osteotomy is favoured biomechanically in young high-demand patients.
- The axillary nerve lies on the anterior surface of subscapularis and curves under its inferior border, lying closest to the joint at the inferior (6 o'clock) glenoid — typically within a finger-breadth of the rim, marked by the anterior circumflex humeral vessels.
- Capsulolabral repair passes sutures through the labrum AND the capsule for a shift, tied in 30–40° of external rotation to restore IGHL tension; proceed to Latarjet if glenoid bone loss is greater than 20–25%.
- “Beach-chair positioning allows intraoperative ROM testing critical for subscapularis repair assessment.
- “Taking the cephalic vein laterally with the deltoid preserves venous drainage and reduces postoperative swelling.
- “Glenoid bone loss greater than 20–25% is the threshold to abort a soft-tissue repair and convert to a Latarjet for bone reconstruction.
- “The postoperative protocol is more conservative than after arthroscopic repair because of the subscapularis: no external rotation past neutral for 6 weeks.
When & Why
Indication. Open Bankart repair is offered for symptomatic recurrent anterior glenohumeral instability with a documented anteroinferior labral (Bankart) lesion, where an open approach gives better assessment and repair of complex pathology than arthroscopy — typically after conservative management or a prior failed stabilisation has been exhausted.
Recurrent instability after an arthroscopic Bankart repair — the most common indication for open revision surgery.
Any revision shoulder stabilisation — the open approach allows better assessment and repair of complex, multi-structure pathology.
Moderate glenoid bone loss that does not yet mandate a Latarjet — open repair allows accurate intraoperative bone assessment and management.
Secondary indications. An engaging Hill-Sachs lesion requiring remplissage combined with the Bankart repair; contact or collision athletes wanting the lowest possible recurrence rate (roughly 5–10% open versus 10–15% arthroscopic); large rotator-interval laxity better addressed open with direct closure; poor tissue quality (Ehlers-Danlos, revision tissue) where open handling is advantageous; surgeon preference in some high-volume practices; and failed conservative management with multiple dislocations and a documented Bankart lesion. Contraindications. - Absolute: glenoid bone loss greater than 25% (requires a Latarjet with bone augmentation); active infection (staged treatment); and severe medical comorbidity making surgery prohibitive.
- Relative: a voluntary dislocator (a psychiatric or behavioural component requires assessment); bone loss less than 10% (arthroscopic generally preferred for primary cases); multidirectional instability (may require a capsular shift and a different approach); fixed posterior subluxation (different pathology); and significant pre-existing subscapularis pathology that may compromise the repair. Preoperative assessment. Clinically, document the instability direction, a positive apprehension test, load-and-shift grade (0–3 baseline), the sulcus sign, range of motion (especially external rotation, to set postoperative goals) and subscapularis strength (lift-off, belly-press). Imaging requires plain radiographs (AP, scapular Y, axillary lateral), a CT with 3D reconstruction to quantify bone loss (best-fit circle / bare-spot method), and an MRI or MR arthrogram for labral pathology, capsular injury and subscapularis integrity; evaluate the Hill-Sachs for size, location and engagement risk.
Glenoid bone loss greater than 20–25% is the critical threshold. Below it a soft-tissue Bankart repair is appropriate; above it bone augmentation (Latarjet) is required. The open approach allows accurate intraoperative assessment if preoperative imaging is equivocal — and proceeding with a soft-tissue repair when bone loss exceeds this threshold is the most common cause of failure.
Consent specifically for the open approach: a measurable loss of external rotation (average around 10°), subscapularis-related weakness, recurrence (5–10%), stiffness, a small risk of axillary nerve injury (1–2% transient), and infection. Setup. Beach-chair position with the head elevated 60–70°, a bump behind the medial scapula to bring the shoulder forward, and the arm free-draped so it can move through a full range for intraoperative testing. Mark the coracoid, the deltopectoral interval and the acromion. Regional or general anaesthesia with prophylactic cefazolin within 60 minutes of incision.
The Operation
The goal is to re-establish the anteroinferior labral bumper and capsular tension through a deltopectoral exposure, taking down and then securely repairing the subscapularis, while protecting the axillary nerve throughout. The exposure — developing the deltopectoral interval, opening the clavipectoral fascia lateral to the conjoint tendon, and mobilising the subscapularis off the capsule — is laid out as the first steps of the sequence below (and in depth on the deltopectoral approach to the shoulder page).
Operative sequence
- Beach chair, head elevated 60–70°, bump behind the medial scapula, arm free-draped for full ROM testing.
- Mark the coracoid, the deltopectoral interval and the acromion for orientation.
- Prep the entire shoulder girdle including the neck and chest to the nipple line; ensure sterile access to the anterior shoulder and axilla; avoid excessive traction on the brachial plexus.
- A standard deltopectoral incision from the coracoid extending 8–10 cm distally along the deltopectoral groove (follows natural skin lines; an axillary-crease incision is a more cosmetic alternative but gives harder inferior access).
- Incise skin and subcutaneous tissue to the clavipectoral fascia and identify the cephalic vein in the interval.
- Take the cephalic vein laterally with the deltoid to preserve venous drainage and reduce postoperative swelling (taking it medially with pectoralis is the alternative); ligate and cauterise if injured.
- Identify the conjoint tendon (short head of biceps and coracobrachialis), the clavipectoral fascia overlying subscapularis, and the coracoacromial ligament superiorly.
- Incise the clavipectoral fascia lateral to the conjoint tendon — this protects the musculocutaneous nerve, which enters the conjoint 3–8 cm (average 5 cm) distal to the coracoid; extend from the coracoid to the inferior border of subscapularis.
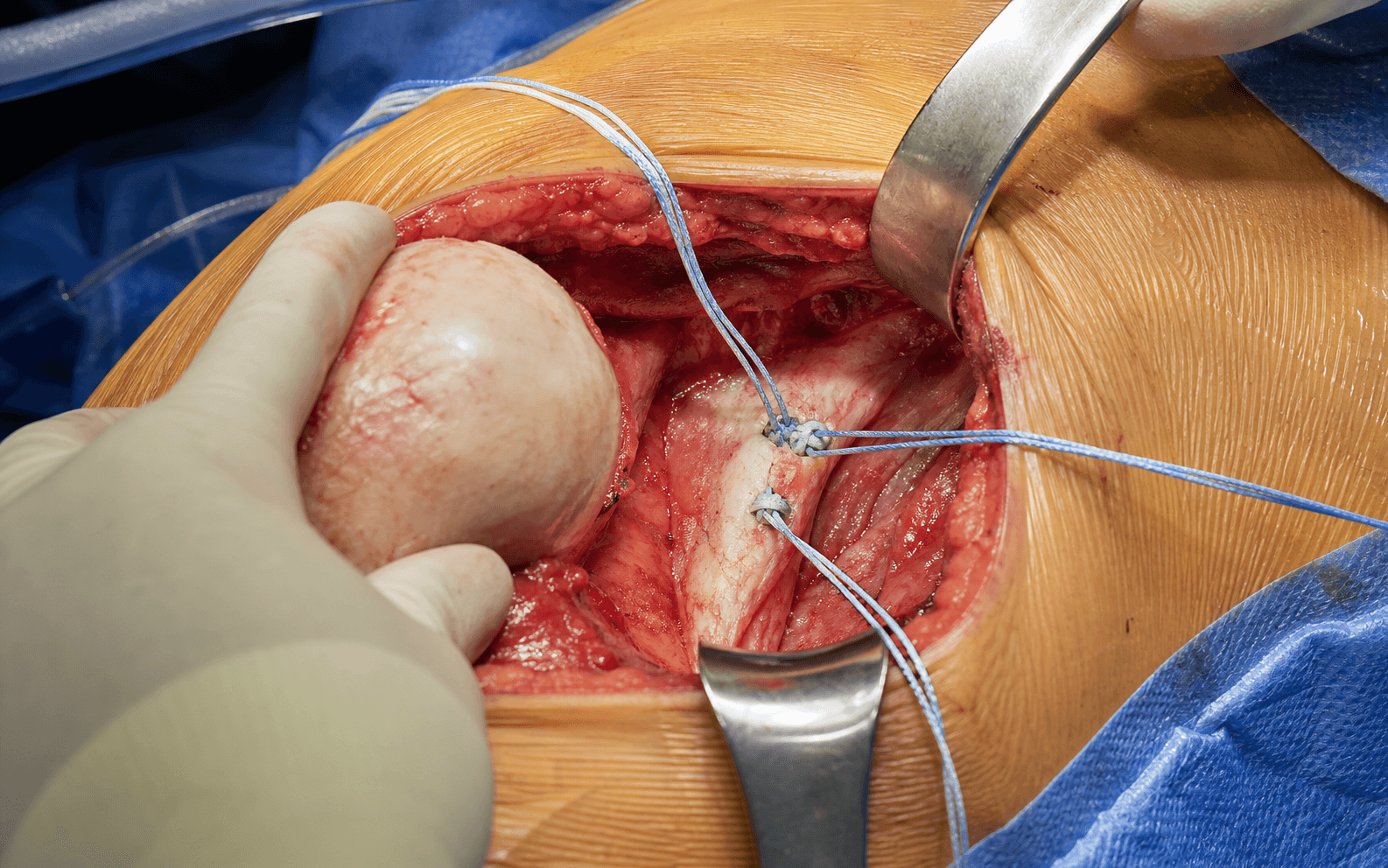
- Place a self-retaining retractor; retract deltoid laterally and pectoralis medially; identify the subscapularis tendon, the long head of biceps in its groove (lateral landmark), and the anterior circumflex humeral vessels ("three sisters") at the inferior subscapularis border — these mark the level of the axillary nerve.
- Three options (compared in the table below): lesser-tuberosity osteotomy, subscapularis peel, or tenotomy. Peel is a reasonable default; osteotomy for the highest-demand construct; tenotomy the simplest.
- Whatever the choice, tag the tendon with 2-0 or 0 Ethibond horizontal-mattress sutures (3–4 for a secure hold) to use as handles for retraction and later repair.
- Use sharp dissection to separate subscapularis from the anterior capsule — this preserves the capsule for later repair and avoids lengthening the subscapularis (blunt dissection tears the capsule and lengthens the muscle).
- Mobilise medially enough to allow retraction; release from the anterior scapula only if needed.
- The axillary nerve runs on the anterior surface of subscapularis — gentle handling, no aggressive anterior or inferior dissection.
- Externally rotate and slightly extend the arm to bring the anterior capsule into view.
- A vertical capsulotomy (longitudinal, parallel to the glenoid edge) is preferred — it preserves the IGHL inferiorly and is easier to close without overtightening; a T-capsulotomy adds a horizontal limb at the inferior border for better inferior exposure.
- Place a Fukuda retractor on the anterior glenoid neck and a Darrach retractor on the posterior rim; keep the inferior retractor tip on bone — driving it deep or inferior endangers the axillary nerve.
- Assess the Bankart lesion (typically 2 to 6 o'clock on a right shoulder; fresh versus chronic; medial displacement onto the glenoid neck).
- Quantify glenoid bone loss with the bare-spot method (distance from the bare spot to the anterior rim versus the posterior rim) and direct comparison to the intact posterior glenoid.
- Assess the Hill-Sachs lesion (width, depth, engagement in abduction-external rotation; on-track versus off-track using the glenoid track versus the Hill-Sachs interval) and capsular laxity (drive-through sign).
- Mobilise the labrum from the glenoid neck with a periosteal elevator, starting inferiorly at 6 o'clock and working to 12 o'clock, freeing it 5–10 mm medially — complete mobilisation is essential for a tension-free repair.
- Release scarred, chronically adherent labrum and capsule sharply until the tissue is mobile enough to advance without tension.
- Prepare the glenoid rim to a bleeding bone surface with a curette or small burr (remove 1–2 mm of edge cartilage); preserve glenoid stock.
- Place 3–4 suture anchors (2.9–3.0 mm bioabsorbable or PEEK) on the glenoid face at the articular margin, starting inferiorly at 5–6 o'clock and spacing 4–5 mm apart — not on the neck.
- Angle each anchor at 45° to the glenoid face (the deadman angle) for optimal pullout strength.
- Transosseous drill holes (2.5 mm bit from the anterior face through the posterior neck) are the bone-conserving, implant-free alternative but are more technically demanding.
- Pass sutures through both the labrum and the capsule (the capsulolabral shift) — labrum-only fails to restore capsular tension and the IGHL.
- Work from inferior (5–6 o'clock) to superior, taking 3–5 mm of tissue in each bite.
- Tie the knots with the arm in 30–40° of external rotation, sequentially inferior to superior, knots on the capsular side away from the articular surface — neutral rotation overtightens, excessive ER undertightens.
- Close the capsulotomy watertight with interrupted 2-0 absorbable sutures.
- Add a capsular shift only if a drive-through sign persists or the capsule is markedly redundant — overlap the leaves by 5–10 mm (lateral under medial) with the arm in 40° ER; balance stability against range of motion.
- Osteotomy: reduce the bone wafer anatomically and fix with 2–3 partially threaded 4.0 mm screws and/or heavy sutures over a bone bridge, arm in neutral rotation.
- Peel (preferred default): drill 3–4 transosseous tunnels (2.5–3.0 mm, parallel, exiting the lateral cortex) through the lesser tuberosity, pass the tagged number-2 Ethibond sutures, and tie over the lateral bone bridge in a horizontal-mattress configuration with the arm in neutral rotation.
- Tenotomy: direct tendon-to-tendon repair with multiple interrupted heavy sutures, arm in neutral rotation.
- Test the repair: passive external rotation should reach 40° comfortably (less means overtightened), with a positive lift-off and belly-press.
- Load-and-shift should be grade 1 (grade 0 will stiffen, grade 2+ will fail); apprehension negative in abduction-ER; sulcus stable.
- Range of motion: forward elevation 140–160°, external rotation at the side to 40° comfortably, internal rotation to L3–L5, abduction-ER to 90°/60° without apprehension.
- Subscapularis function: lift-off and belly-press intact; document all tests against the preoperative examination to guide postoperative expectations.
- Copious saline irrigation (3–6 L); meticulous haemostasis.
- Close the clavipectoral fascia with 0 or 2-0 absorbable suture, deep dermis with 2-0 or 3-0 absorbable, and skin with a subcuticular 3-0 or 4-0 Monocryl.
- Apply a sterile dressing and place the arm in a sling in internal rotation to relax the subscapularis repair.
- How it is fixed
- Osteotome a full-thickness bone wafer (about 1–1.5 cm) carrying the insertion; fix with 2–3 screws and/or heavy sutures over a bone bridge
- Advantages
- Bone-to-bone healing; biomechanically the most robust construct at time-zero; anatomic footprint restoration
- Disadvantages & best use
- Technically demanding; small non-union/malunion and hardware-prominence risk; higher morbidity — young high-demand contact athletes, revision cases
- How it is fixed
- Sharply elevate the insertion as a periosteal sleeve; repair through 3–4 transosseous tunnels in the lesser tuberosity
- Advantages
- Good balance of exposure and secure repair; no hardware; reliable healing; lower morbidity
- Disadvantages & best use
- More dissection than tenotomy; requires bone tunnels — the reasonable default for most cases
- How it is fixed
- Divide the tendon about 1 cm medial to its insertion, leaving a cuff; direct tendon-to-tendon repair
- Advantages
- Simplest and fastest; least dissection; no bone work
- Disadvantages & best use
- Tendon-to-tendon healing is biomechanically least robust and relies on tissue quality — older, lower-demand patients
The axillary nerve passes from the quadrilateral space across the anterior subscapularis and curves under its inferior border, lying closest to the joint at the inferior (6 o'clock) glenoid — often within a finger-breadth of the rim. Use the anterior circumflex humeral vessels to locate it, keep inferior dissection to a minimum, guard it with a finger or retractor during inferior capsular work, mobilise the subscapularis gently, and avoid a deep or aggressive inferior Fukuda retractor.
Anchors must sit on the glenoid face at the articular margin at the 45° deadman angle — not on the neck. A neck placement creates no bumper effect and the repair will fail; too medial a placement damages cartilage.
Glenoid bone loss greater than 20–25% is an absolute contraindication to a soft-tissue Bankart alone. Quantify it intraoperatively with the bare-spot method; if it exceeds the threshold, abort and stage a Latarjet — proceeding will fail.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | 0–6 weeks | Sling in internal rotation, continuous | Pendulum exercises; elbow/wrist/hand ROM; no ER past neutral | | 2 | 6–8 weeks | Sling discontinued and weaned | Passive then active ROM; gentle subscap (IR) first, then progress ER | | 3 | 8–12 weeks | — | Progressive ROM and light strengthening | | 4 | 12+ weeks | — | Strengthening of subscapularis, rotator cuff and periscapular muscles; sport-specific | | Return to sport | 4–6 months (non-contact), 6+ months (contact) | — | Full recovery 6–9 months | The protocol is deliberately more conservative than after an arthroscopic repair because of the subscapularis: external rotation is restricted past neutral for 6 weeks (versus 3–4 weeks arthroscopically). Early aggressive external rotation causes subscapularis failure and recurrence — patient education is essential. Complications
- Rate
- 5–10%
- Recognition & prevention
- Reproduced apprehension, load-and-shift grade 2–3, repair failure or new bone loss on MRI. Prevent with accurate bone-loss assessment, a capsulolabral (not labrum-only) repair, appropriate tensioning in 30–40° ER, a secure subscap, and aborting if bone loss is greater than 25%.
- Management
- Conservative if low-demand and no bone loss. Revision — CT bone loss: under 15% revision Bankart, 15–25% consider Latarjet, greater than 25% Latarjet mandatory; address all pathology.
- Rate
- 5–15%
- Recognition & prevention
- Weak internal rotation, positive lift-off and belly-press, gap on ultrasound. Prevent with a secure peel (transosseous tunnels) or osteotomy, testing to 40° ER intraop, and protecting postop (no ER past neutral 6 weeks).
- Management
- Therapy first — many patients adapt. Revision if high-demand or contributing to recurrence: direct repair, pectoralis major transfer, or allograft augmentation.
- Rate
- 10–20% (average ~10°)
- Recognition & prevention
- ER under 40° at the side; difficulty overhead. Prevent by tying the capsulolabral repair in 30–40° ER, testing to 40° intraop, and avoiding an excessive capsular shift.
- Management
- Under 10° — reassure. 10–20° — PT and gentle capsular stretching. Greater than 20° symptomatic — gentle stretching; avoid aggressive manipulation (redislocation risk); arthroscopic release as salvage.
- Rate
- 5–10%
- Recognition & prevention
- Global ROM loss with pain on passive stretch. Prevent with balanced repair tension, early passive ROM (week 2–3), and identifying risk factors (diabetes, hypothyroidism, prior stiffness).
- Management
- PT and supervised stretching, NSAIDs, intra-articular corticosteroid, and time. Refractory — manipulation under anaesthesia or arthroscopic capsular release (carries redislocation risk).
- Rate
- 1–2% transient, under 1% permanent
- Recognition & prevention
- Deltoid weakness and sensory loss over the lateral shoulder (badge area). Prevent with anatomic knowledge (anterior circumflex landmark), minimal inferior dissection, and gentle handling.
- Management
- Most recover in 3–6 months — reassure, sling, EMG at 3–6 weeks, maintain ROM. No recovery by 6 months — consider nerve exploration.
- Rate
- 1–2%
- Recognition & prevention
- Superficial wound erythema/drainage or deep sepsis with systemic symptoms. Prevent with cefazolin within 60 min of incision, chlorhexidine shower, no shaving, meticulous technique and copious irrigation.
- Management
- Superficial — oral antibiotics (cephalexin/augmentin) and wound care. Deep — urgent debridement, retain stable anchors, remove loose hardware, 6 weeks IV antibiotics with ID input.
- Rate
- under 1%
- Recognition & prevention
- Weak elbow flexion and supination, lateral forearm numbness. Prevent by incising clavipectoral fascia lateral to the conjoint tendon and avoiding medial retraction.
- Management
- Neurapraxia (most) — observe, recovers 3–6 months with EMG surveillance. Transection — immediate or delayed exploration with repair or graft.
Recurrent instability: quantify bone loss preoperatively and abort to a staged Latarjet if it is greater than 25%; build a secure capsulolabral repair with appropriate tensioning. Subscapularis failure: use a peel with transosseous tunnels or an osteotomy (not tenotomy in high-demand patients), test to 40° ER intraop, and protect with no ER past neutral for 6 weeks. Axillary nerve palsy: limit inferior dissection, use the anterior circumflex vessels as the landmark, and handle the subscapularis gently.
Viva & Exam Focus
SUBSCAPSUBSCAP — subscapularis management options
Hook:Examiners expect you to compare the three subscapularis techniques with pros and cons and state your preference with rationale
REPAIRREPAIR — steps of the open Bankart technique
Hook:A systematic sequence demonstrates understanding of the critical steps — essential for the operative viva
Critical anatomy at risk
Passes from the quadrilateral space across the anterior subscapularis and curves under its inferior border, closest to the joint at the inferior (6 o'clock) glenoid — within a finger-breadth of the rim; the anterior circumflex vessels mark its level. Protect with minimal inferior dissection, a finger or retractor guard, gentle subscap mobilisation, and by avoiding a deep inferior Fukuda.
Enters coracobrachialis 3–8 cm from the coracoid tip (average 5 cm, highly variable). Protect by incising the clavipectoral fascia lateral to the conjoint tendon and avoiding aggressive medial retraction.
Lies in the deltopectoral interval, superficial to the clavipectoral fascia. Take it laterally with the deltoid to preserve venous drainage, or medially with pectoralis; ligate and cauterise if injured.
Lies in the bicipital groove lateral to the subscapularis insertion — a lateral landmark. Identify the groove and avoid taking the subscapularis down too laterally; preserve the rotator interval.
Lies posterior to the clavipectoral fascia and can be stretched by arm positioning in beach chair. Avoid excessive traction; keep the arm neutral and monitor its position throughout.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old professional rugby player has recurrent anterior shoulder instability despite an arthroscopic Bankart repair 18 months ago, with 3 redislocations. CT shows 18% glenoid bone loss and a moderate Hill-Sachs lesion. How would you manage him? Walk me through your decision-making.”
“You have taken down the subscapularis with a peel during an open Bankart repair and are now ready to repair it. Walk me through your subscapularis repair technique and how you assess its adequacy.”
“Compare and contrast the three subscapularis management options for an open Bankart repair. Which do you prefer and why? Give the specific indications, advantages and disadvantages of each.”
Indications (open vs arthroscopic)
- Failed arthroscopic Bankart (most common)
- Revision shoulder stabilisation
- Glenoid bone loss 15–20% (not enough for Latarjet)
- Engaging Hill-Sachs needing remplissage
- Contact athletes wanting lowest recurrence
- Contraindication: bone loss greater than 25% needs Latarjet
Key anatomy & danger zones
- Axillary nerve: anterior subscap, closest at the 6 o'clock glenoid — anterior circumflex landmark
- Musculocutaneous nerve: enters conjoint 3–8 cm from coracoid (avg 5 cm)
- Cephalic vein: deltopectoral interval, take laterally
- Long head biceps: bicipital groove, lateral landmark
- Brachial plexus: avoid excessive traction in beach chair
Critical operative steps
- Beach chair 60–70°, arm free for intraop ROM testing
- Deltopectoral approach, cephalic vein taken laterally
- Clavipectoral fascia incised LATERAL to conjoint
- Subscap: peel default, osteotomy for high-demand, tenotomy simplest
- Vertical capsulotomy; assess bone loss — abort if greater than 25%
- 3–4 anchors on the glenoid FACE at 45° deadman angle
- Capsulolabral shift (labrum AND capsule), tie in 30–40° ER
- Subscap repair in neutral, tested to 40° ER intraop
Numbers to know
- Recurrence roughly 5–10% open vs 10–15% arthroscopic
- Subscap failure about 5–15% (no clear difference between techniques)
- ER loss average ~10° (up to ~20% in some series)
- Axillary nerve 1–2% transient, under 1% permanent
- Bone-loss threshold 20–25%; subcritical loss above ~13.5% (Shaha)
Complications & management
- Recurrence 5–10%: accurate bone assessment, secure repair, abort if greater than 25%
- Subscap failure 5–15%: secure peel/osteotomy, test to 40°, protect postop
- ER loss 10–20%: tie in 30–40° ER, test intraop
- Axillary palsy 1–2%: minimal inferior dissection, anterior circumflex landmark
- Infection 1–2%: cefazolin within 60 min; deep needs debridement + 6 weeks IV
Postoperative protocol
- Sling in IR for 6 weeks (more conservative than arthroscopic)
- NO ER past neutral for 6 weeks — protects the subscap
- Pendulum immediately; passive ROM weeks 2–3
- Active ROM 6–8 weeks; strengthening 12 weeks
- Non-contact sport 4–6 months, contact 6+ months, full recovery 6–9 months
Background & Evidence
Open versus arthroscopic Bankart. Open repair carries a lower recurrence rate (roughly 5–10%) than modern arthroscopic repair (10–15%), at the cost of greater morbidity (subscapularis takedown, stiffness). Arthroscopy is preferred for primary cases without significant bone loss; open repair is preferred for revision cases, bone loss of 15–20%, engaging Hill-Sachs lesions, and contact athletes. The long-term Pelet series (29-year follow-up) shows durable stability but a measurable loss of rotation and secondary osteoarthritis in a substantial minority. Glenoid bone-loss thresholds. The amount of bone loss drives the procedure choice:
- Typical approach
- Soft-tissue Bankart adequate
- Typical approach
- Soft-tissue Bankart acceptable; consider a bone block if other risk factors
- Typical approach
- Soft-tissue possible but higher recurrence; open Bankart or Latarjet by risk profile
- Typical approach
- Critical threshold — favour a Latarjet
- Typical approach
- Soft-tissue Bankart will fail — Latarjet mandatory
References
Bankart repair for recurrent anterior glenohumeral instability: results at twenty-nine years' follow-up
- 30 shoulders followed a mean of 29 years after open Bankart repair for traumatic anterior instability
- Recurrent dislocation in 3 patients (10%), one requiring reoperation — durable stability
- Mean loss of external rotation 24 degrees and internal rotation 19 degrees versus the contralateral shoulder
- Radiographic osteoarthritis in 40% overall (including 5 patients requiring later shoulder arthroplasty)
Redefining 'critical' bone loss in shoulder instability: functional outcomes worsen with 'subcritical' bone loss
- 73 shoulders after isolated arthroscopic Bankart repair, mean follow-up 48 months
- Glenoid bone loss above about 13.5% produced WOSI scores consistent with a poor clinical outcome even without recurrence
- Mean bone loss was significantly higher in failures than in stable repairs (24.7% vs 12.8%)
- Failure rose sharply in the highest quartile (27.8% with 20–35% bone loss)
Evolving concept of bipolar bone loss and the Hill-Sachs lesion: from 'engaging/non-engaging' to 'on-track/off-track' lesion
- Introduces the glenoid track to integrate humeral (Hill-Sachs) and glenoid bone loss as bipolar loss
- An off-track Hill-Sachs lesion engages the anterior rim and predicts failure of isolated soft-tissue repair
- Glenoid bone loss of 25% or more (inverted-pear glenoid) warrants glenoid bone grafting
- Provides a quantitative, reproducible treatment paradigm combining radiographic and arthroscopic assessment
The instability severity index score: a simple pre-operative score to select patients for arthroscopic or open shoulder stabilisation
- Prospective case-control study of 131 patients after arthroscopic Bankart repair with suture anchors
- Risk factors: age under 20, competitive/contact/overhead sport, hyperlaxity, Hill-Sachs on AP radiograph, loss of glenoid sclerotic contour
- A 10-point Instability Severity Index Score (ISIS) integrates these factors
- A score over 6 carried an unacceptable 70% recurrence after arthroscopic repair
The open Latarjet procedure is more reliable in terms of shoulder stability than arthroscopic Bankart repair
- 93 matched pairs (open Latarjet vs arthroscopic Bankart), minimum 4-year (mean 6-year) follow-up
- Recurrent instability 10% after Latarjet vs 22% after arthroscopic Bankart (OR 0.39)
- Late (after 2-year) recurrence was far more common in the Bankart group
- Mean Rowe score higher after Latarjet (78 vs 68); reoperation rates were similar
Subscapularis management in stemless total shoulder arthroplasty: tenotomy versus peel versus lesser tuberosity osteotomy
- 188 shoulders compared across tenotomy, peel and lesser tuberosity osteotomy
- No significant difference in pain, AASE score or patient-reported instability at 2 years
- Active external rotation was greater after peel than after tenotomy
- No significant difference in clinical subscapularis failure between techniques