Displaced bicolumnar (AO 13-B/C) distal humerus fracture · chevron olecranon osteotomy for articular visualization
- The indication is a displaced intra-articular distal humerus fracture (AO 13-B and 13-C) needing anatomical reduction and stable fixation. A chevron olecranon osteotomy at the bare area of the sigmoid notch gives the best view of the trochlea for complex bicolumnar patterns.
- Identify and protect the ulnar nerve FIRST in every case — never leave it compressed under a medial plate. Transpose it anteriorly only if hardware will overlie the nerve, the cubital tunnel floor is destroyed, or there is pre-operative ulnar neuropathy.
- Reduce the ARTICULAR SURFACE FIRST — reconstruct the trochlea anatomically before attaching the articular block to the columns. A step-off of less than 2 mm is the acceptable threshold.
- Two plates are MANDATORY for a bicolumnar fracture. Parallel plating and 90-90 (perpendicular) plating are both evidence-supported and biomechanically equivalent — the only RCT found no difference in outcome.
- Early motion from day 1–3 is the single most important factor in preventing stiffness, the most common complication (20–50 percent).
When & Why
Indication. A displaced intra-articular distal humerus fracture — AO/OTA 13-B (partial articular, single column) and 13-C (complete articular, bicolumnar) — that needs anatomical reduction and stable fixation, plus complex B2/B3 patterns requiring trochlear visualization. Extra-articular (type A) fractures usually do not need an olecranon osteotomy and are fixed through a lateral or medial approach. Why an olecranon osteotomy. For a bicolumnar fracture the articular surface is the whole game, and the olecranon blocks the view of the trochlea from behind. A chevron osteotomy at the bare area of the sigmoid notch reflects the olecranon and triceps proximally and gives an unparalleled view of the articular surface — the exposure that makes an anatomical articular reduction possible. For simple patterns a triceps-sparing or triceps-splitting approach may avoid the osteotomy, but for a C-type fracture the osteotomy is the workhorse. Assess before you cut. Document the skin and the neurovascular status — especially ulnar nerve function — and obtain a CT for any C-type fracture to delineate the articular fragments and comminution. Aim to operate within 24–48 hours, before swelling peaks. The fixation decision — parallel versus 90-90 (perpendicular) plating. Both constructs are valid; the choice rests on fracture pattern, bone quality and surgeon preference, not dogma.
- Plate position
- Medial plate on the medial column; lateral plate on the posterolateral column — plates at 90 degrees, a box-like construct
- Best for
- Comminuted medial column; allows more distal medial fixation
- Plate position
- Both plates on the posterior surface, one medial and one lateral, in the sagittal plane; long interdigitating screws create an arch-like fixed-angle construct
- Best for
- Osteoporotic bone; maximises distal screw number and length
The Operation
The goal: expose the articular surface through a posterior approach and a chevron olecranon osteotomy, identify and protect the ulnar nerve, reduce the trochlea anatomically (articular first), fix both columns with parallel or perpendicular plates and long interdigitating screws, fix the osteotomy, and confirm a full arc of motion — so the elbow can be mobilized early. The exposure is laid out as the first steps below (and in depth on the posterior approach to the elbow page).
Operative sequence
- Lateral decubitus with the arm over a padded bolster (allows full elbow extension), or prone on chest rolls; arm draped free. Sterile tourniquet on the upper arm.
- Posterior midline incision 15–20 cm centered on the olecranon tip, curved laterally around the olecranon to avoid a scar directly over the bony prominence; raise full-thickness skin flaps. Protect the medial cutaneous nerve of the forearm in the subcutaneous fat (injury causes medial forearm numbness).
- ULNAR NERVE IS THE FIRST PRIORITY — find it in the posterior compartment, behind the medial epicondyle in the cubital tunnel, before any deep dissection.
- Trace the ulnar nerve from the arcade of Struthers proximally to the first motor branch in FCU distally; protect with a vessel loop.
- In-situ protection if hardware will not overlie the nerve; anterior subcutaneous transposition if a plate will compress the cubital tunnel, the tunnel floor is destroyed, or there is pre-operative ulnar neuropathy (submuscular for revision or severe scarring).
- For transposition: mobilize roughly 10 cm of nerve with surrounding vascular tissue (do not strip the adventitia — no internal neurolysis), release the intermuscular septum and FCU fascia to prevent kinking, transpose anterior to the medial epicondyle and hold with a fascial sling. NEVER leave the nerve under hardware.
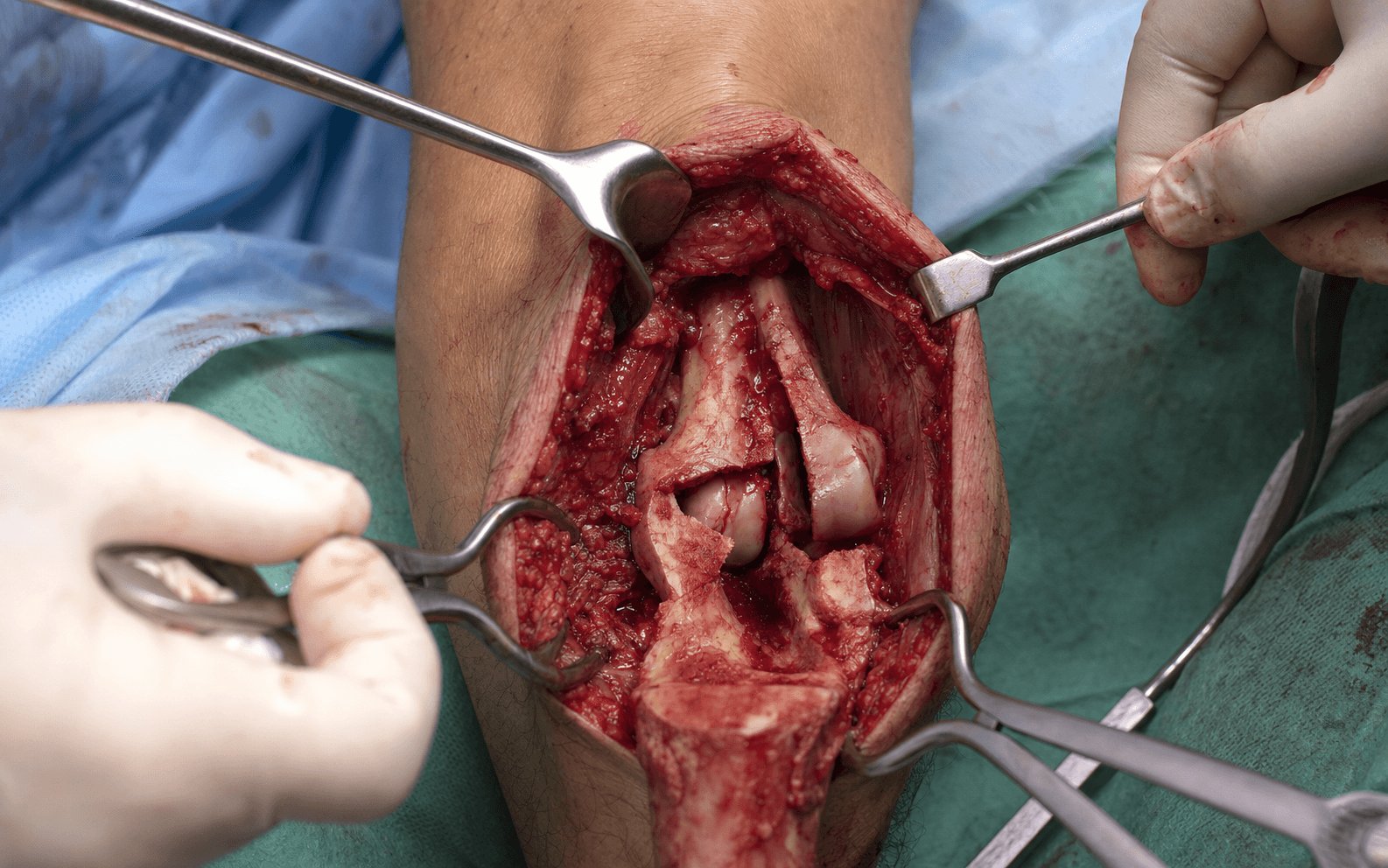
- Chevron (inverted-V) osteotomy at the bare area of the sigmoid notch — the apex of the trochlear notch, about 2 cm distal to the tip, where there is no articular cartilage. The chevron gives the best visualization plus rotational stability for later fixation.
- PRE-DRILL for fixation (a 6.5 mm cannulated screw or plate holes) before cutting — you cannot drill accurately after the osteotomy.
- Mark the line with electrocautery, score the cortices with an oscillating saw to 2–3 mm (avoiding the articular surface), then complete the cut with a thin osteotome to protect the cartilage at the edges.
- Reflect the olecranon with the attached triceps proximally to expose the distal humeral articular surface — a view unmatched by any other approach.
- Assess the pattern under direct vision, irrigate, and remove small loose fragments. Identify every articular fragment.
- REDUCE THE ARTICULAR SURFACE FIRST — reconstruct the trochlea anatomically, reducing the condyles to each other, and hold with provisional K-wires.
- Aim for an anatomic reduction: a step-off of less than 2 mm is the acceptable threshold; more than that leads to post-traumatic arthritis. Consider bone graft or substitute for central comminution. Do not miss posterior fragments — common and easily overlooked.
- Attach the reconstructed articular block to the metaphysis and diaphysis.
- Apply pre-contoured anatomical plates: medial plate on the medial column ridge, lateral plate on the posterolateral column. Two plates are MANDATORY for a bicolumnar fracture — a single plate is insufficient.
- Use a 90-90 (perpendicular) or parallel configuration (see When & Why). Plates must be long enough to span metaphysis to diaphysis with at least 2–3 screws in each major fragment.
- Place long interdigitating screws through the distal plate holes across the articular block — one from the medial plate into the lateral condyle and one from the lateral plate into the medial condyle — creating a stable fixed-angle arch (the O'Driscoll principle).
- Check under fluoroscopy that no screw penetrates the articular surface or the olecranon fossa (a posterior screw here blocks extension). Ensure screws avoid the ulnar nerve course.
- Aim for at least 5–6 screws per plate, minimum two in each major fragment.
- Reduce the olecranon osteotomy anatomically and fix with one of: 1. Tension band wiring — a figure-of-8 wire anterior to the axis of rotation converts triceps extension force into compression; two parallel K-wires from the olecranon tip into the anterior ulnar cortex. Bury the K-wire tips to reduce prominence. 2. 6.5 mm cannulated screw with washer — less prominent, good for a simple chevron. 3. Pre-contoured olecranon plate — for a comminuted or osteoporotic osteotomy, or revision.
- Take the elbow through full ROM on the table: full extension (to 0 degrees unless there is a pre-existing contracture), flexion to 140 degrees, full pronation and supination.
- Confirm no impingement from screws or plates. Verify the ulnar nerve is not compressed in any position and the osteotomy is stable through the arc. Any block to motion must be corrected before closure.
- Final fluoroscopy — AP, lateral and oblique — confirm an anatomical articular reduction, adequate plate position and length, and no intra-articular or olecranon-fossa hardware (the lateral view is key for fossa clearance).
- Irrigate copiously (at least 3 L), release the tourniquet and achieve meticulous hemostasis, place a drain deep to the triceps. If transposed, confirm the ulnar nerve lies in a subcutaneous position without tension.
- Close the triceps fascia, subcutaneous tissue and skin; apply a well-padded splint in 45–90 degrees of flexion for comfort.
Identify the ulnar nerve before any deep dissection and protect it throughout. It is at risk from traction, devascularization during over-aggressive mobilization, kinking if the intermuscular septum is not released during transposition, and compression if left under a medial plate. Post-operative ulnar neuropathy of some degree is reported in roughly 10–25 percent of cases; most are transient neuropraxias resolving over 3–6 months. Pragmatic rule: protect in situ unless hardware will overlie the nerve, the cubital tunnel floor is destroyed, or there is symptomatic pre-operative neuropathy.
Make the chevron at the bare area (apex of the trochlear notch) — too distal damages articular cartilage, too proximal gives inadequate exposure. Pre-drill before cutting, score with the saw and complete with an osteotome to protect the cartilage, and do not avulse the triceps by over-retracting the reflected fragment. Olecranon non-union runs 2–5 percent and hardware prominence 40–50 percent with any technique.
The whole operation turns on two ideas: reconstruct the trochlea anatomically as a block, then fix that block to the shaft with long screws that interdigitate across it from both plates. Linking the columns with interdigitating screws creates an arch-like fixed-angle construct — the most stable option for a comminuted fracture (O'Driscoll, 2005).
Before closure, screen the lateral fluoroscopy in full extension. A posterior screw or plate sitting in the olecranon (or coronoid) fossa is the most common cause of an intra-operative extension block — replace with a shorter screw or reposition the plate. Do not accept a new extension loss that can be corrected.
Aftercare & Complications
Rehabilitation. Early motion is the single most important factor in preventing stiffness. | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | Immediate | Days 1–7 | Posterior splint in 45–90 degrees flexion for comfort | Remove splint day 1–3 for gentle active-assisted ROM; overhead elevation to reduce swelling; NO passive stretch | | Early | Weeks 1–6 | Discard splint by week 2 if stable; hinged brace if needed | Active-assisted flexion/extension and forearm rotation 5–6 times daily; target 30–130 degrees by 6 weeks; no lifting more than 1 kg | | Intermediate | Weeks 6–12 | — | Progressive strengthening; full ROM goal; dynamic splinting if stiffness developing (less than 100 degrees flexion); radiographs at 6 and 12 weeks | | Late | Months 3–6 | — | Return to sport/work; full activity by 4–6 months; hardware removal if symptomatic (40–50 percent) once healed at 12–18 months | Consider manipulation under anaesthesia if motion plateaus below 90 degrees flexion at around 3 months (provided there is no HO and fixation is stable); open arthrolysis for refractory stiffness or significant HO. Heterotopic ossification prophylaxis (reserve for high-risk cases — severe soft-tissue injury, associated head injury, burns, previous HO; the evidence for routine prophylaxis is limited and inconsistent): indomethacin 75 mg daily for around 3–6 weeks, OR single-dose radiation (commonly 700 cGy) within 72 hours if NSAIDs are contraindicated. Complications.
- Recognition
- ROM below the 30–130 degrees functional arc, difficulty with ADLs
- Prevention
- Early motion day 1–3, avoid passive stretching, adequate analgesia, therapy
- Management
- Intensive physiotherapy, dynamic splinting; MUA if less than 90 degrees flexion at 3 months; open arthrolysis if refractory
- Recognition
- Numbness in ulnar digits, intrinsic weakness, positive Froment sign, claw posture
- Prevention
- Early identification, gentle handling, transpose if hardware overlies nerve
- Management
- Most transient neuropraxia resolving over 3–6 months; EMG/NCS at 3 months if no recovery; late neurolysis or revision transposition
- Recognition
- Progressive stiffness, pain, palpable bone in soft tissues, visible on radiograph
- Prevention
- Early motion; prophylaxis for high-risk cases
- Management
- Excision once mature (12–18 months) with repeat prophylaxis
- Recognition
- Persistent pain, motion at the fracture site, progressive radiolucent lines
- Prevention
- Anatomical reduction, stable fixation with adequate plate length, avoid soft-tissue stripping
- Management
- Revision ORIF with bone grafting and longer plates; consider TEA in the elderly or severe articular damage
- Recognition
- Pain at the osteotomy site, palpable motion, hardware loosening, step on lateral radiograph
- Prevention
- Precise chevron technique, pre-drilling, proper tension band or plate fixation
- Management
- Revision fixation with plate and bone graft; excision with triceps advancement if the fragment is small
- Recognition
- Palpable hardware, pain with direct pressure, bursa, skin irritation
- Prevention
- Low-profile pre-contoured plates, bury K-wire tips, avoid olecranon prominence
- Management
- Hardware removal once union is confirmed (12–18 months) — common and expected
Viva & Exam Focus
Five structures at risk.
Passes behind the medial epicondyle in the cubital tunnel, then between the two heads of FCU. Identify it FIRST, mobilize with a vessel loop, and transpose anteriorly if hardware will overlie it. Never leave it compressed under a plate.
Posterior arm in the spiral groove, then pierces the lateral intermuscular septum about 10 cm proximal to the lateral epicondyle. Limit proximal dissection and palpate it if extending the approach proximally.
Within supinator, vulnerable if exposure extends laterally. Keep the forearm supinated for any lateral exposure and avoid retracting beyond the radial head.
At the osteotomy site. Use a chevron at the bare area, score with a saw and complete with an osteotome to protect the cartilage; reduce the osteotomy anatomically.
Anterior to the elbow in the cubital fossa. Avoid anterior penetration during fixation, confirm no anterior screw or K-wire penetration on fluoroscopy, and flex the elbow during posterior dissection.
COLUMNCOLUMN — bicolumnar fixation principles
ELBOWELBOW — post-operative principles
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old woman falls on her outstretched hand and presents with a painful, swollen elbow. Radiographs show a displaced bicolumnar distal humerus fracture (AO 13-C2). Describe your management.”
“During ORIF of a distal humerus fracture via olecranon osteotomy, you cannot achieve full elbow extension despite an anatomical reduction. What are the causes and how would you address this?”
“Three months after ORIF of a distal humerus fracture, your patient has a 30–100 degrees elbow ROM and is frustrated. Radiographs show a healed fracture with an anatomical reduction. How do you assess and manage this stiffness?”
Indications
- Displaced bicolumnar (AO 13-C) distal humerus fractures
- Intra-articular fractures needing articular visualization
- Complex B2/B3 patterns needing trochlear exposure
Exposure
- Posterior approach with chevron olecranon osteotomy at the bare area
- ULNAR NERVE identified FIRST in every case
- Pre-drill the olecranon before cutting
Reduction
- ARTICULAR FIRST — reconstruct the trochlea anatomically
- Less than 2 mm articular step-off is the threshold
- Provisional K-wires, then attach the block to the shaft
Fixation
- Two-plate principle MANDATORY for bicolumnar fractures
- 90-90 or parallel plating — both acceptable (RCT: no difference)
- Long interdigitating screws through the articular segment
- Check olecranon fossa clearance — no impingement
Osteotomy fixation & finish
- Tension band, 6.5 mm screw, or plate
- Confirm full ROM intra-operatively
- Splint in 45–90 degrees flexion
Rehabilitation
- Early motion day 1–3 is CRITICAL
- Active-assisted ROM, NOT passive stretching
- Target 30–130 degrees by 6 weeks (functional arc)
- No lifting more than 1 kg for 6–8 weeks
Numbers to know
- Stiffness 20–50 percent (most common)
- Ulnar nerve dysfunction 15–20 percent
- HO 5–15 percent, non-union 2–5 percent
- Hardware prominence 40–50 percent
- Functional arc 30–130 degrees flexion
Background & Evidence
Epidemiology. Distal humerus fractures have a bimodal distribution — young males (high-energy trauma) and elderly females (osteoporotic, low-energy). Type C (complete articular, bicolumnar) is the most common adult pattern requiring this approach; C3 (articular comminution) carries the worst prognosis. In children, roughly 90 percent of distal humerus fractures are extra-articular (supracondylar). AO/OTA classification of distal humerus fractures (13).
- Pattern
- Extra-articular
- Subgroups
- A1 avulsion, A2 simple metaphyseal, A3 comminuted metaphyseal
- Typical management
- Lateral or medial approach — osteotomy usually unnecessary
- Pattern
- Partial articular (single column)
- Subgroups
- B1 lateral (capitellum), B2 medial (trochlea), B3 coronal (Dubberley)
- Typical management
- Approach matched to the fracture pattern
- Pattern
- Complete articular (bicolumnar)
- Subgroups
- C1 simple articular/simple metaphyseal, C2 simple/comminuted metaphyseal, C3 articular comminution
- Typical management
- Posterior approach with olecranon osteotomy — the indication for this operation
Key evidence. O'Driscoll (2005) set out the principle-based objectives of distal humeral fixation and argued the perpendicular (90-90) dogma is "unsubstantiated and incorrect" — parallel sagittal-plane plates are as strong or stronger, and interdigitating screws create an arch-like fixed-angle construct. Sanchez-Sotelo, Torchia and O'Driscoll (2007) validated this clinically: 34 complex fractures (26 were C3) achieved primary union in 31 of 32 with no hardware failure. The Cochrane review (Wang, 2013) — the only randomised trial comparing perpendicular versus parallel double-plating (35 patients) — found no significant difference in Mayo score, complications or range of motion, and the ulnar nerve trial (29 patients) found no benefit of routine transposition over in-situ decompression. The consistent message: individualise the plate configuration and the ulnar nerve decision — do not be dogmatic.
References
Optimizing stability in distal humeral fracture fixation
- Articulates the technical objectives of distal humeral fixation: every distal screw through a plate engaging an opposite-column fragment also fixed to a plate, maximising screw number and length, and interdigitating/locking screws to create a fixed-angle structure with supracondylar compression on both columns
- Concluded from the biomechanical literature that the perpendicular (90-90) dogma is 'unsubstantiated and incorrect' — parallel sagittal-plane plates are as strong or stronger
- Linking the columns by interdigitating screws creates an arch-like construct, the most stable option for comminuted fractures
Complex distal humeral fractures: internal fixation with a principle-based parallel-plate technique
- 34 consecutive complex distal humeral fractures (26 AO type C3, 14 open) fixed with parallel medial and lateral plates in the sagittal plane
- No hardware failure or fracture displacement in any patient; primary union in 31 of 32 fractures followed
- Mean flexion-extension arc 99 degrees, mean Mayo Elbow Performance Score 85; 27 of 32 results graded excellent or good
Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach
- 25 patients with isolated closed intercondylar fractures fixed via a posterior approach with bicolumnar plating, mean follow-up 37 months
- Mean flexion contracture 25 degrees, mean flexion-extension arc 108 degrees; elbow flexion and extension strength reduced to around 74–76 percent of the normal side
- Mean DASH 20 (mild residual impairment); 6 of 25 (24 percent) required reoperation, half of these for prominent olecranon-osteotomy hardware
ORIF versus total elbow arthroplasty for displaced intra-articular distal humeral fractures in elderly patients (multicentre RCT)
- 42 patients over 65 with OTA type 13C fractures randomised to ORIF or semiconstrained TEA
- 5 of 21 (25 percent) randomised to ORIF were converted to TEA intra-operatively because stable fixation was unachievable
- TEA gave significantly better Mayo Elbow Performance Scores at 3, 6, 12 and 24 months; reoperation rates (TEA 12 percent vs ORIF 27 percent) were not significantly different
Surgical interventions for treating distal humeral fractures in adults (Cochrane systematic review)
- Pooled 3 randomised trials (109 patients): perpendicular versus parallel double-plating (35 patients) showed NO significant difference in Mayo score, complications or range of motion
- The trial of anterior transposition versus in-situ decompression of the ulnar nerve (29 patients) found no statistically significant difference in nerve recovery
- ORIF versus TEA data favoured TEA on Mayo score but the intention-to-treat difference did not reach significance
Precontoured parallel plate fixation of AO/OTA type C distal humerus fractures
- 32 patients with OTA type C fractures treated with a precontoured parallel (congruent) plating system, mean follow-up 27 months
- All fractures healed with no implant failures; mean flexion-extension arc 97 degrees, mean Mayo score 82, mean DASH 24
- 24 complications occurred in 17 patients (53 percent), including post-operative nerve injury in 5 patients (16 percent)