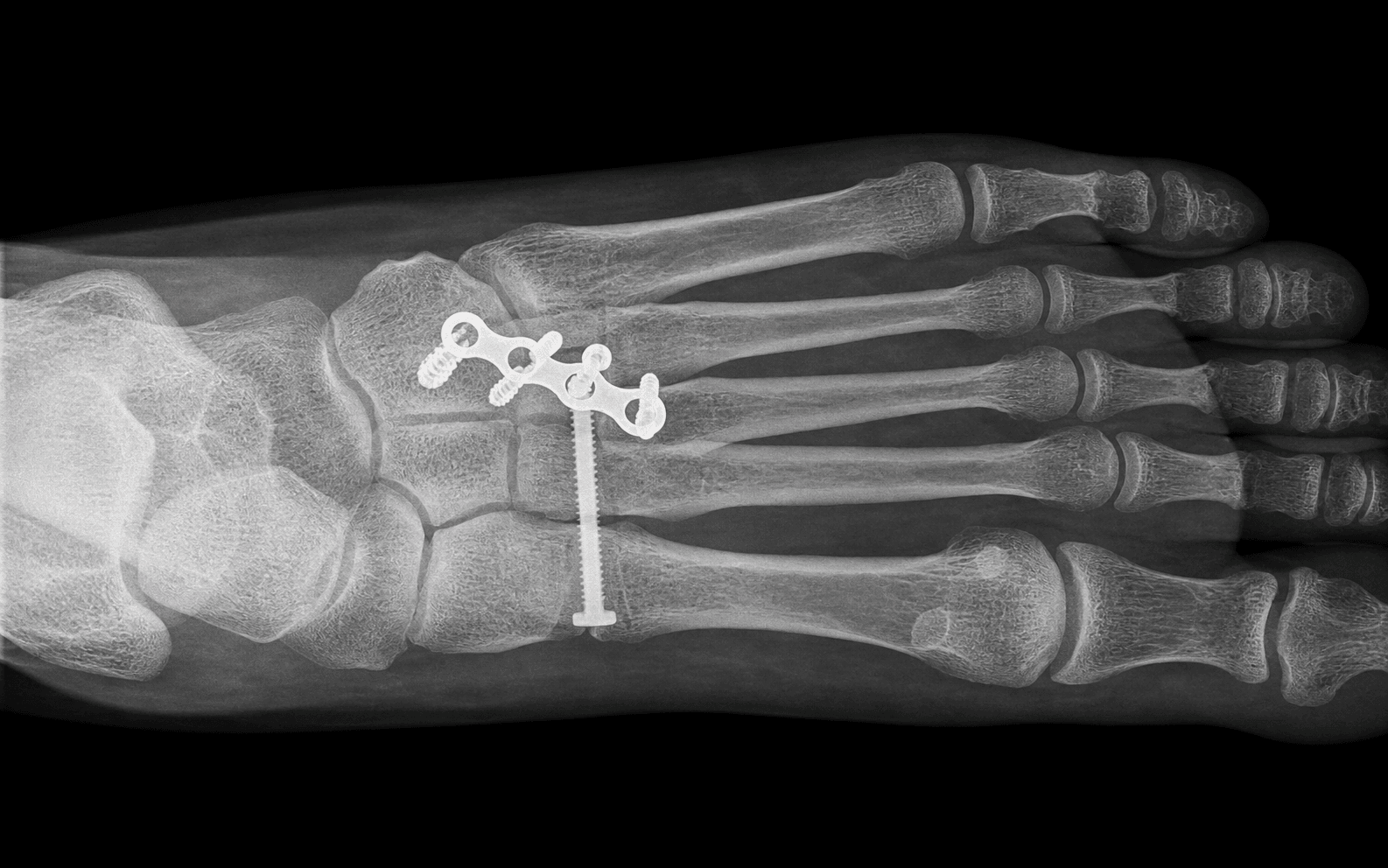
Tarsometatarsal fracture-dislocation · Myerson Type A / B / C
- Indications: a displaced Lisfranc fracture-dislocation (greater than 2mm at any TMT joint), subtle instability on weight-bearing stress radiographs, a purely ligamentous injury with instability, and open injuries once the soft tissues are controlled.
- Exposure is through two dorsal longitudinal incisions — medial between the 1st and 2nd metatarsals (8–10cm) for the medial and middle columns, lateral over the 4th metatarsal (6–8cm) for the lateral column — preserving a skin bridge of at least 5–7cm.
- Reduce MEDIAL COLUMN FIRST: the 1st TMT, then the 2nd TMT (the keystone, recessed proximally between the cuneiforms), then the 3rd, then the lateral column.
- The dorsalis pedis artery runs between MT1 and MT2 only 0–5mm deep to skin — the highest-risk structure; identify it early beneath the extensor hallucis brevis and protect it with a vessel loop throughout.
- Anatomic reduction is the goal — less than 2mm residual displacement on AP, oblique and lateral views. Even 2–3mm means poor outcomes and accelerated arthritis. Transarticular screws must be removed at 4–6 months; consider primary arthrodesis for purely ligamentous injuries.
When & Why
Indication. Operative fixation is indicated for any injury that leaves the tarsometatarsal (TMT) complex unstable or incongruous: a displaced fracture-dislocation (greater than 2mm at any TMT joint), subtle instability on weight-bearing stress radiographs, a purely ligamentous injury with instability, and open injuries once the soft tissues have been controlled. Stable, non-displaced sprains that line up on weight-bearing films are managed non-operatively in a cast or boot. Work the injury up before you cut. Confirm the pattern and plan fixation with:
- Weight-bearing AP, oblique and lateral radiographs of BOTH feet (comparison views) — the global standard. Look for 1st–2nd intermetatarsal diastasis, loss of the medial MT2 / medial cuneiform line, and the "fleck sign" (an avulsed Lisfranc ligament fragment).
- CT for bony detail, occult fractures and surgical planning.
- MRI when the radiographs are normal but a purely ligamentous injury is suspected — it shows the Lisfranc ligament directly. The one decision that matters. Once you have decided to operate, the core manoeuvre is the same — an anatomic reduction of the medial and middle columns. What varies is how you hold it:
The traditional standard. 3.5–4.0mm cortical screws from the metatarsal base into the cuneiform cross the joint and give strong fixation, but they damage articular cartilage and MUST be removed at 4–6 months to restore motion.
Low-profile locking plates span the TMT joint dorsally, staying extra-articular. No routine removal is needed and the cartilage is spared, at the cost of hardware prominence on the thin dorsum.
For PURELY LIGAMENTOUS injuries, fusing the 2nd and 3rd TMT (preserving the 1st and lateral column if stable) gives equivalent or better outcomes with a far lower reoperation rate. Not for reconstructable bony fracture-dislocations.
Consent specifically for post-traumatic arthritis (the most common late problem, 20–50 percent over 5–10 years even after anatomic fixation), wound problems over the skin bridge or prominent hardware, dorsalis pedis injury and foot ischaemia, compartment syndrome, and a likely second operation to remove transarticular screws. Many patients never regain full pre-injury performance — set realistic expectations. Setup. Supine with a bump under the ipsilateral hip (15–20 degrees) to neutralise the limb's external rotation; radiolucent table; thigh tourniquet (250–300mmHg, or about systolic plus 100mmHg). A thigh (not ankle) tourniquet is preferred because the deep dissection is dorsal and proximal. Foot at the end of the table or on a radiolucent triangle for full fluoroscopic access. Confirm and document the dorsalis pedis and posterior tibial pulses and the neurology before inflation. Loupe magnification helps nerve and vessel identification in the 1st–2nd intermetatarsal space.
The Operation
The goal: reduce every TMT joint anatomically through two dorsal incisions, protecting the dorsalis pedis artery and deep peroneal nerve, and hold the reduction with screws, plates or a selective fusion. The exposure — two dorsal longitudinal incisions with a generous skin bridge — is laid out in full below (and in depth on the dorsal approach to the midfoot page).
Operative sequence
- Supine, ipsilateral hip bump (15–20 degrees) to neutralise external rotation; radiolucent table; thigh tourniquet (250–300mmHg, or systolic plus 100mmHg).
- Foot at the end of the table or on a radiolucent triangle so the image intensifier can reach AP, oblique and lateral views of the whole midfoot.
- Confirm and document the dorsalis pedis and posterior tibial pulses and the neurology before inflating the tourniquet.
- Mark the two dorsal longitudinal incisions: (1) medial, between the 1st and 2nd metatarsals, 8–10cm centred on the TMT joint line; (2) lateral, over the 4th metatarsal, 6–8cm.
- Preserve a skin bridge of at least 5–7cm between them to avoid dorsal skin necrosis.
- The medial incision exposes the medial and middle columns (1st, 2nd, 3rd TMT); the lateral incision exposes the lateral column (4th and 5th TMT).
- Deep to the skin in the 1st–2nd intermetatarsal space run the dorsalis pedis artery and deep peroneal nerve — only 0–5mm deep, covered by the thin extensor hallucis brevis (EHB) belly.
- Identify and elevate the EHB to expose the neurovascular bundle, sling the artery and nerve with vessel loops, and retract gently throughout. This is done before any bone work.
- Expose the 1st, 2nd and 3rd TMT joints subperiosteally; assess the fracture pattern, displacement, cartilage damage and any soft-tissue interposition (capsule, tendon) that blocks reduction.
- Clear haematoma and debris from the 1st TMT (medial cuneiform to 1st metatarsal base).
- Reduce with bone clamps or K-wires: longitudinal traction on MT1, direct pressure on the base; confirm the lateral border of MT1 aligns with the lateral border of the medial cuneiform on the oblique view.
- Provisionally pin. The 1st TMT is mobile (10–15 degrees of sagittal motion) so ORIF aims to preserve motion; fuse only if the joint is unstable or the cartilage is destroyed.
- Reduce the 2nd TMT (intermediate cuneiform to 2nd metatarsal base) — the keystone, recessed proximally between the cuneiforms and the most commonly injured joint.
- Restore the medial border of MT2 in line with the medial border of C2 on the AP view; confirm the 1st–2nd intermetatarsal space is less than 2mm (no diastasis).
- Provisionally pin. For a purely ligamentous injury, decide now between ORIF and primary 2nd/3rd TMT fusion.
- Transarticular screws (3.5–4.0mm cortical, metatarsal base to cuneiform), dorsal bridge plates (extra-articular), or primary fusion of the 2nd/3rd TMT for ligamentous injuries.
- Confirm no articular penetration on fluoroscopy before final tightening.
- Through the lateral incision over the 4th metatarsal, protect the superficial peroneal nerve branches and expose the 4th and 5th TMT (cuboid to MT4 and MT5).
- The lateral column often reduces indirectly once the medial and middle columns are fixed, because the intermetatarsal ligaments are intact; assess stability with gentle stress under fluoroscopy.
- Fix only if unstable — K-wires usually suffice; avoid over-fixation, which restricts gait motion. Confirm the medial border of MT4 aligns with the medial border of the cuboid.
- Comprehensive fluoroscopy in AP, oblique and lateral. Goal: less than 2mm residual displacement at every joint.
- If any view shows greater than 2mm, take the fixation down and re-reduce — accept only anatomic reduction.
- Irrigate, close in layers (capsule and periosteum where possible, deep fascia, subcutaneous to eliminate dead space, skin with nylon or staples), minimising bulk over prominent hardware.
- Inspect the skin bridge for ischaemia. Apply a well-padded below-knee splint with the foot in neutral (slight plantarflexion is acceptable to relax the dorsal soft tissues).
- Strict elevation for 48–72 hours; watch for compartment syndrome.
Runs between MT1 and MT2, only 0–5mm deep, beneath the EHB belly. Identify it early, sling it with a vessel loop, retract gently. Injury risks foot ischaemia requiring immediate vascular repair.
Accompanies the dorsalis pedis artery in the 1st–2nd space. Protect it with the artery; injury causes 1st web space numbness (usually a temporary neuropraxia if retraction-related).
The intermediate and medial dorsal cutaneous branches cross the dorsum superficially and are at risk in both incisions. Careful subcutaneous dissection under loupe magnification; retract gently, avoid transection.
A minimum 5–7cm bridge between the medial and lateral incisions prevents dorsal necrosis. Monitor it intra- and post-operatively; full-thickness loss may need flap coverage.
Before any fixation in the medial incision, identify the dorsalis pedis artery between MT1 and MT2 (only 0–5mm deep, beneath the EHB) and sling it with the deep peroneal nerve. Never clamp blindly. If it is injured: direct pressure, extend for exposure, identify both ends, repair primarily with 6-0 or 7-0 prolene or a vein graft, and call for vascular help. Document distal perfusion (dorsalis pedis and posterior tibial pulses) before and after.
The reduction sequence is medial-column first. Reduce the 1st TMT (the mobile foundation), then the 2nd TMT (the recessed keystone), then the 3rd, and assess the lateral column last — it often falls into line once the keystone is set. Reduce each joint anatomically before moving on, confirming on fluoroscopy, because each level depends on the one proximal to it.
Anatomic reduction drives outcome — the quality of reduction, not the injury pattern alone, is the single most important modifiable variable. Even 2–3mm of residual displacement at any joint is associated with post-traumatic arthritis and poor functional scores. If any view (AP, oblique or lateral) shows greater than 2mm, take the fixation down and re-reduce. Do not accept "close enough".
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Milestones | |-------|--------|----------------|------------| | 1 | 0–8 weeks | Strict non-weight-bearing in a below-knee cast or boot | Radiographs at 2, 6 and 12 weeks to confirm maintained alignment | | 2 | 8–12 weeks | Progressive weight-bearing in a boot (25 percent to 50 percent to 75 percent to full) | Transition to a supportive shoe with an arch-support orthosis at about 12 weeks | | 3 | 4–6 months | Supportive shoe and orthosis | Hardware removal if transarticular screws were used; return to ADLs | | 4 | 6–12 months | Orthosis for heavy tasks | Graded return to athletics; counsel that many never regain full performance | Transarticular screws must be removed at 4–6 months to restore TMT motion — permanent screws across these joints cause iatrogenic arthritis, the major disadvantage of screws versus plates or primary fusion. Dorsal plates can stay permanently if asymptomatic, and a primary fusion needs no second operation. Follow up at 6 months, 1 year, then annually to watch for post-traumatic arthritis; if it develops and is refractory to orthoses, activity modification and injection, a salvage fusion of the symptomatic joints (typically the 2nd and 3rd TMT, preserving the 1st and lateral column) gives good pain relief.
Lisfranc injuries, especially crush mechanisms, carry a 5–10 percent risk of compartment syndrome. Pulses are preserved until very late — rely on pain out of proportion, pain on passive toe stretch and tense compartments. If you suspect it, perform a foot fasciotomy (nine compartments) immediately: delay causes permanent muscle necrosis, contractures and amputation. A negative fasciotomy is far better than a missed one.
- Recognition
- Most common (20–50 percent over 5–10 years). Midfoot pain, stiffness, difficulty on uneven ground; joint-space narrowing and osteophytes on radiograph
- Prevention
- Anatomic reduction less than 2mm; careful cartilage handling; consider primary fusion for ligamentous injury
- Management
- Conservative: orthoses, NSAIDs, activity modification, injection. Salvage: TMT fusion of symptomatic joints (80–90 percent pain relief)
- Recognition
- 5–10 percent, higher with crush. Pain out of proportion, pain on passive stretch, tense compartments. An EMERGENCY
- Prevention
- High index of suspicion; check compartments before and after tourniquet release; low threshold for fasciotomy
- Management
- Immediate foot fasciotomy (nine compartments). Delay causes permanent necrosis, contractures, amputation
- Recognition
- 2–5 percent, the highest-risk vascular injury. Foot ischaemia, absent pulse, pallor; may cause amputation if missed
- Prevention
- Identify the artery early beneath the EHB; vessel-loop protection; gentle retraction; know the MT1-MT2 anatomy
- Management
- Immediate vascular repair or vein graft; may need amputation if irreparable. Document pre-operative vascular status
- Recognition
- 10–20 percent. Persistent pain, early arthritis; greater than 2mm displacement on any view
- Prevention
- Confirm less than 2mm on AP, oblique AND lateral; re-reduce if inadequate; do not accept 'close enough'
- Management
- Revision with re-reduction if symptomatic; salvage fusion if arthritis is established
- Recognition
- 5–10 percent. Dehiscence or necrosis, especially the skin bridge or over prominent hardware; higher in diabetes and obesity
- Prevention
- Minimum 5–7cm skin bridge; tension-free closure; optimise soft tissues before surgery; avoid prominent hardware
- Management
- Local wound care if superficial; negative-pressure therapy; flap coverage for full-thickness loss
- Recognition
- 5–10 percent, higher than many foot injuries. Burning pain disproportionate to injury, allodynia, vasomotor changes
- Prevention
- Gentle tissue handling; adequate analgesia; early protected mobilisation; avoid prolonged immobilisation
- Management
- Early recognition is critical. Multidisciplinary pain team, graded motor imagery, gabapentin, sympathetic blocks
Viva & Exam Focus
MEDIAL
LIS-FRANC
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“The examiner shows you radiographs of a 35-year-old who fell off a ladder. There is widening between MT1 and MT2 with subtle dorsolateral subluxation of the MT2 base on the lateral view. How would you classify and manage this injury?”
“Describe the primary fusion versus ORIF debate for Lisfranc injuries. When would you recommend each approach?”
“During surgery for a Lisfranc injury you note brisk bleeding from the medial incision between MT1 and MT2. What structure is injured and how do you manage it?”
Indications
- Displaced Lisfranc fracture-dislocation (greater than 2mm at any TMT joint)
- Subtle instability on weight-bearing stress radiographs
- Purely ligamentous injury with instability (consider primary fusion)
- Open injuries, once the soft tissues are controlled
Myerson classification
- Type A: total incongruity — all 5 TMT joints displaced the same way
- Type B1: partial medial — medial column displaced, lateral stable
- Type B2: partial lateral — lateral column displaced, medial stable
- Type C: divergent — medial and lateral displaced opposite ways (worst prognosis)
Critical anatomy
- Lisfranc ligament: medial cuneiform (plantar) to 2nd MT base — strongest midfoot ligament
- No direct ligament between MT1 and MT2 — explains 1st-2nd diastasis
- 2nd MT is the keystone — recessed, most rigid, most commonly injured
- Dorsalis pedis artery between MT1 and MT2 — highest-risk structure
Reduction sequence (MEDIAL)
- Medial column FIRST (1st TMT is the foundation)
- Evaluate the 2nd TMT (the keystone)
- Intermediate column (3rd TMT) next
- Assess the lateral column last (4th, 5th TMT)
- Lock in final fixation once all reduced
Fixation options
- Transarticular screws: 3.5–4.0mm, MUST remove at 4–6 months
- Dorsal plates: extra-articular, no routine removal
- Primary fusion: for ligamentous injuries — fuse 2nd/3rd TMT, preserve 1st and lateral
- Evidence: primary fusion gives equal or better outcomes for ligamentous injuries
Reduction criteria (less than 2mm is critical)
- AP: medial MT2 aligns with medial C2, 1st-2nd space less than 2mm
- Oblique: medial MT3 aligns with medial C3
- Lateral: no dorsal subluxation, Meary's line straight
- Any view greater than 2mm = re-reduce — do not accept 'close enough'
Danger structures
- Dorsalis pedis artery (between MT1-MT2, only 0–5mm deep) — highest risk
- Deep peroneal nerve (with the artery — 1st web numbness if injured)
- Superficial peroneal nerve branches (dorsal foot, both incisions)
- Skin bridge (minimum 5–7cm between medial and lateral incisions)
Viva essentials
- Know the Myerson classification cold — the examiner will show radiographs
- Explain Lisfranc ligament anatomy and why diastasis occurs (no MT1-MT2 ligament)
- Describe the MEDIAL COLUMN FIRST sequence with its rationale
- Discuss primary fusion versus ORIF with the evidence (Henning; Ly and Coetzee)
Background & Evidence
Epidemiology. Lisfranc injuries are uncommon — roughly 0.2 percent of all fractures, about 1 per 55,000 person-years — and notoriously under-recognised: 20–40 percent are missed or misdiagnosed at first presentation, especially low-energy athletic sprains. High-energy mechanisms (motor-vehicle crashes, falls from height, crush) produce the fracture-dislocations; subtle ligamentous injuries dominate the athletic population. Pathoanatomy — why diastasis happens. The Lisfranc ligament runs from the PLANTAR surface of the medial cuneiform (C1) to the base of the 2nd metatarsal — the strongest interosseous ligament of the midfoot. There is NO direct ligament between MT1 and MT2: the 1st metatarsal is held to the 2nd only indirectly through the cuneiforms. When the Lisfranc ligament fails, the 1st–2nd intermetatarsal space widens (diastasis) — the hallmark radiographic sign. Three columns and the keystone.
- Medial column — the 1st TMT; the most mobile (10–15 degrees of sagittal motion), so preserving motion matters.
- Middle column — the 2nd and 3rd TMT; the keystone. The 2nd metatarsal base is recessed proximally between the cuneiforms, forming a mortise analogous to the ankle. It is the most rigid, the least mobile, and the most commonly injured — so the most important to reduce anatomically.
- Lateral column — the 4th and 5th TMT; mobile and important for gait.
- Description
- Total incongruity
- Pattern
- All 5 TMT joints displaced in the same direction (usually lateral or dorsolateral)
- Treatment implications
- Severe injury; full exposure needed
- Description
- Partial incongruity — medial
- Pattern
- Medial column displaced, lateral column stable
- Treatment implications
- A medial incision alone may suffice
- Description
- Partial incongruity — lateral
- Pattern
- Lateral column displaced, medial column stable
- Treatment implications
- Less common; may need a single lateral incision
- Description
- Divergent
- Pattern
- Medial and lateral columns displaced in opposite directions (1st MT medial, 2nd–5th lateral)
- Treatment implications
- Most severe; highest energy; worst outcomes; dual incisions required
- Lines to check
- Medial border MT2 aligns with medial border of the intermediate cuneiform; 1st–2nd intermetatarsal space less than 2mm; medial border MT4 aligns with medial border of the cuboid
- Lines to check
- Medial border MT3 aligns with medial border of the lateral cuneiform; lateral border MT1 aligns with lateral border of the medial cuneiform
- Lines to check
- No dorsal subluxation of the metatarsal bases; Meary's line (talus to 1st metatarsal axis) straight
- Global evidence and society guidance
- Roughly 0.2 percent of all fractures (about 1 per 55,000 person-years); 20–40 percent are missed initially, especially subtle athletic sprains
- Global evidence and society guidance
- Weight-bearing AP/oblique/lateral of BOTH feet (comparison) is the global standard; CT for bony detail, MRI for the Lisfranc ligament and purely ligamentous injury
- Global evidence and society guidance
- An anatomic, near-anatomic reduction (less than 2mm at any TMT joint) is the universally accepted goal across AO Foundation, AOFAS and BOA practice — it drives long-term outcome
- Global evidence and society guidance
- International debate, not country-specific: primary arthrodesis of the medial/middle columns is supported for PURELY LIGAMENTOUS injuries (Ly and Coetzee; Henning); ORIF remains standard for bony fracture-dislocations with reconstructable articular surfaces
- Global evidence and society guidance
- Global shift from transarticular screws (mandatory removal, iatrogenic cartilage injury) toward dorsal bridge plating and, for ligamentous injury, primary fusion; suture-button or flexible fixation is used selectively for isolated low-grade ligamentous (C1-MT2) instability in athletes, though long-term data are limited
- Global evidence and society guidance
- Athletes with stabilised injuries typically return at a minimum of 4–6 months; counsel that many never regain full pre-injury performance
References
- Myerson MS, Fisher RT, Burgess AR, Kenzora JE. Fracture dislocations of the tarsometatarsal joints: end results correlated with pathology and treatment. Foot Ankle. 1986;6(5):225-242. PMID: 3710321. 2. Ly TV, Coetzee JC. Treatment of primarily ligamentous Lisfranc joint injuries: primary arthrodesis compared with open reduction and internal fixation. A prospective, randomized study. J Bone Joint Surg Am. 2006;88(3):514-520. PMID: 16510816. 3. Henning JA, Jones CB, Sietsema DL, Bohay DR, Anderson JG. Open reduction internal fixation versus primary arthrodesis for Lisfranc injuries: a prospective randomized study. Foot Ankle Int. 2009;30(10):913-922. PMID: 19796583. 4. Kuo RS, Tejwani NC, DiGiovanni CW, et al. Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am. 2000;82(11):1609-1618. PMID: 11097452. 4a. Smith N, Stone C, Furey A. Does open reduction and internal fixation versus primary arthrodesis improve patient outcomes for Lisfranc trauma? A systematic review and meta-analysis. Clin Orthop Relat Res. 2016;474(6):1445-1452. PMID: 26022112. 4b. Alcelik I, Fenton C, Hannant G, et al. A systematic review and meta-analysis of the treatment of acute Lisfranc injuries: open reduction and internal fixation versus primary arthrodesis. Foot Ankle Surg. 2019;26(3):299-307. PMID: 31103276. 5. Sands AK, Grose A. Lisfranc injuries. Injury. 2004;35 Suppl 2:SB71-76. 6. Philbin T, Rosenberg G, Sferra JJ. Complications of missed or untreated Lisfranc injuries. Foot Ankle Clin. 2003;8(1):61-71. 7. Mulier T, Reynders P, Dereymaeker G, Broos P. Severe Lisfranc injuries: primary arthrodesis or ORIF? Foot Ankle Int. 2002;23(10):902-905. 8. Arntz CT, Veith RG, Hansen ST Jr. Fractures and fracture-dislocations of the tarsometatarsal joint. J Bone Joint Surg Am. 1988;70(2):173-181. 9. Hardcastle PH, Reschauer R, Kutscha-Lissberg E, Schoffmann W. Injuries to the tarsometatarsal joint. Incidence, classification and treatment. J Bone Joint Surg Br. 1982;64(3):349-356. 10. Nunley JA, Vertullo CJ. Classification, investigation, and management of midfoot sprains: Lisfranc injuries in the athlete. Am J Sports Med. 2002;30(6):871-878.
Fracture-dislocations of the tarsometatarsal joints: end results correlated with pathology and treatment
- Series of 76 Lisfranc fracture-dislocations (52 patients, mean follow-up 4.2 years); only 49 percent achieved a good or excellent result
- The major determinant of an unacceptable result was the quality of the initial reduction, not the injury pattern alone
- Displacement greater than 2mm OR a talometatarsal angle greater than 15 degrees after closed reduction mandates open reduction
- Direct crush injuries did particularly poorly (only 1 of 8 good or excellent)
Outcome after open reduction and internal fixation of Lisfranc joint injuries
- 48 injuries followed a mean of 52 months after open reduction and screw fixation; mean AOFAS midfoot score 77
- Anatomical reduction was the major determinant of a good result (p = 0.05)
- 25 percent developed post-traumatic osteoarthritis and half of those required arthrodesis
- Purely ligamentous injuries trended toward poorer outcomes despite anatomic reduction and screw fixation
Treatment of primarily ligamentous Lisfranc joint injuries: primary arthrodesis compared with open reduction and internal fixation. A prospective, randomized study
- RCT of 41 patients with primarily ligamentous Lisfranc injuries (20 ORIF vs 21 primary arthrodesis of the medial two or three rays)
- Mean 2-year AOFAS midfoot score 88 (arthrodesis) versus 68.6 (ORIF), p less than 0.005
- Patients reported 92 percent of pre-injury activity after arthrodesis versus 65 percent after ORIF (p less than 0.005)
- Five of 20 ORIF patients developed deformity or osteoarthrosis and were converted to arthrodesis
Open reduction internal fixation versus primary arthrodesis for Lisfranc injuries: a prospective randomized study
- RCT of 40 patients (tarsometatarsal fractures and fracture-dislocations) randomized to ORIF or primary arthrodesis
- Secondary surgery rate (including routine hardware removal and salvage fusion) 78.6 percent for ORIF versus 16.7 percent for primary arthrodesis
- No statistically significant difference in SF-36 or SMFA functional scores at any time point
- No difference in satisfaction at a mean of 53 months
Does open reduction and internal fixation versus primary arthrodesis improve patient outcomes for Lisfranc trauma? A systematic review and meta-analysis
- Meta-analysis of randomized trials; risk ratio for hardware removal 0.23 (95% CI 0.11-0.45, p less than 0.001), favouring fusion (less hardware removal)
- No significant difference in other revision surgery (RR 0.36, p = 0.18)
- No significant difference in patient-reported outcome scores between ORIF and primary fusion
- No significant difference in the risk of non-anatomic alignment