Radical sequestrectomy to bleeding bone, Cierny-Mader staging, local antibiotic carriers and staged reconstruction | advanced
- Cierny-Mader anatomic types (I–IV) and physiologic host classes (A/B/C) dictate resection volume, reconstruction plan and perioperative optimisation — Type IV diffuse disease in a B-host needs the most aggressive debridement and usually a staged reconstruction.
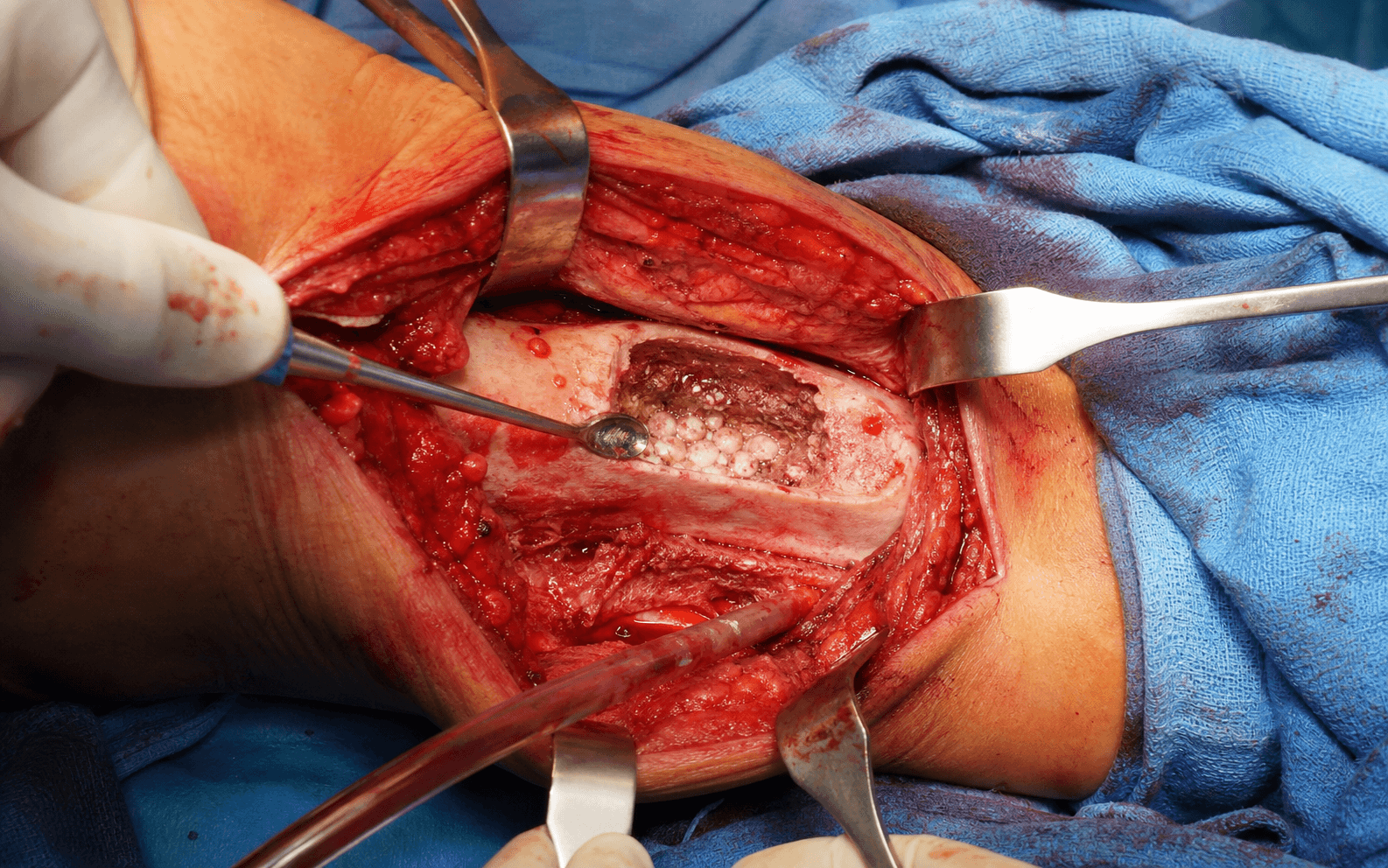
- The paprika sign — punctate bleeding from every surface of the remaining bone — is the intraoperative endpoint of adequate resection; any residual necrotic bone or sequestrum left behind is the commonest cause of recurrence.
- Deep tissue and bone cultures must be taken BEFORE systemic antibiotics are given; superficial swab or sinus-tract cultures are unreliable and lead to inappropriate antimicrobial selection.
- Dead-space management after radical debridement is as important as the resection itself — antibiotic-loaded PMMA beads or spacers give high local concentrations while maintaining space for later definitive reconstruction.
- Type III (localised) and Type IV (diffuse) disease almost always need radical bone resection back to bleeding margins; Type I medullary and Type II superficial disease may be manageable with intramedullary reaming or superficial decortication plus targeted antibiotics.
- B-host optimisation (smoking cessation, glycaemic control, nutritional repletion, vascular reconstruction) is mandatory before major reconstruction — proceeding in an unoptimised B-host dramatically increases the failure rate.
- Antibiotic PMMA beads or spacers should be removed within 6–8 weeks; prolonged retention allows biofilm to form on the cement surface and creates a new nidus for infection.
- Stability is a prerequisite for infection clearance — external fixation or an intramedullary device is applied early to maintain length and alignment while soft-tissue and bone healing occur.
When & Why
Indication. Radical surgical debridement combined with targeted antibiotics is the cornerstone of treatment for chronic osteomyelitis. The clearest indications are chronic infection with a sequestrum or necrotic bone on imaging (Cierny-Mader Type III or IV), a septic nonunion with a mobile fracture site and a persistent sinus or drainage, recurrence after a previous debridement, and a pathological fracture through osteomyelitic bone. Cierny-Mader Type II superficial disease that has failed local wound care, and Type I medullary disease persisting after reaming and antibiotics, are relative indications. Absolute contraindications. A C-host in whom surgical morbidity exceeds the benefit of surgery (consider lifelong suppression or amputation instead), and active untreated systemic sepsis that requires immediate source control elsewhere. Relative contraindication. A B-host with unoptimised comorbidities — smoking, glycaemic control, nutrition, vascular disease — who must be optimised before any major reconstruction; and a small contained Type I lesion that may be manageable on long-term oral antibiotics alone. Pre-operative work-up:
- History: duration of drainage, previous surgeries and antibiotic courses, smoking, diabetes, vascular symptoms.
- Laboratory: CRP, ESR, white cell count, albumin, HbA1c; blood cultures if there are systemic signs.
- Imaging: plain radiographs (sinus tracts, sequestrum, involucrum), MRI (extent of marrow and soft-tissue involvement), CT (cortical detail and sequestrum mapping), angiography if a flap is planned.
- Microbiology: deep bone biopsy or sinus-tract culture if available; hold antibiotics until the samples are obtained.
- Host optimisation: smoking cessation (minimum 4–6 weeks), glycaemic control (HbA1c less than 8 percent), nutritional support (albumin greater than 3.5 g/dL), vascular assessment and revascularisation if indicated.
Obtain an MRI and a CT on every chronic osteomyelitis case. The MRI shows the full extent of marrow oedema and soft-tissue sinus tracts; the CT defines the exact location and size of the sequestrum and the quality of the involucrum. Together they let you plan the resection margins and anticipate whether a flap or bone transport will be needed.
Consent. Discuss the risk of recurrence (10–30 percent depending on host and extent), amputation, flap failure, nonunion, pathological fracture, prolonged antibiotics, and multiple staged procedures. Setup. Supine on a radiolucent table with the limb prepped free; a tourniquet is optional and used only for the initial exposure if bleeding obscures the view, with a bump under the ipsilateral hip for the lower limb. General or regional anaesthesia; avoid local infiltration until the cultures are obtained.
The Operation
The goal is to remove every last piece of necrotic, infected bone and biofilm while preserving living tissue and stability, then manage the resulting dead space and soft-tissue defect so the limb can be reconstructed. The exposure — an extensile approach that incorporates every sinus tract — is the foundation: if you cannot see all of the disease, you cannot resect it.
Operative sequence
- Supine on a radiolucent table, limb prepped free; tourniquet optional, used only for the initial exposure if bleeding obscures the view. Bump under the ipsilateral hip for lower-limb work.
- General or regional anaesthesia — no local infiltration until cultures are obtained.
- Equipment ready: high-speed burr, curettes, rongeurs, osteotomes, pulsatile lavage, antibiotic-loaded PMMA (typically 2–4 g vancomycin plus 2–4 g gentamicin or tobramycin per 40 g cement batch), external fixator set, fluoroscopy.
- Use an extensile approach (for example the anteromedial approach to the tibial shaft) that incorporates all sinus tracts so that nothing infected is left outside the field.
- Excise the sinus tracts en bloc down to bone, and send the tract tissue for culture and histology — a long-standing sinus must be checked for squamous-cell carcinoma (Marjolin's ulcer).
- The exposure has to give complete visualisation of and access to every sinus and sequestrum; a limited incision that hides disease is the first step to failure.
- Remove all loose or infected hardware; send the implant and surrounding tissue for culture.
- Debride all necrotic or fibrotic soft tissue back to healthy, bleeding margins.
- Identify the sequestrum and resect it with osteotomes or a saw.
- Use a high-speed burr and curettes to clear all sclerotic, non-bleeding bone from the cortical surfaces, the endosteal canal and the medullary cavity.
- Continue until every surface demonstrates the paprika sign — multiple punctate bleeding points from healthy bone. Any grey or white non-bleeding bone left behind is the commonest reason for early recurrence.
- Obtain at least five deep samples from different locations: sequestrum, involucrum bed, medullary canal, soft-tissue membrane, and any remaining suspicious tissue.
- Label each and send for aerobic, anaerobic, fungal and mycobacterial culture.
- Do NOT administer systemic antibiotics until all samples are secured.
- Copious pulsatile lavage with 3–9 L of saline.
- Achieve haemostasis, but avoid excessive electrocautery that creates further necrosis.
- For defects less than 2–3 cm, or patients not fit for major reconstruction, place antibiotic-loaded PMMA beads or a spacer.
- For larger defects in an optimised host, plan a staged Masquelet reconstruction or bone transport (see reconstruction options below).
- Apply an external fixator or other stable construct if the debridement has created or revealed instability. Stability is a biologic requirement for infection clearance.
- If the soft-tissue envelope is deficient, plan immediate or delayed flap coverage (local muscle flap or free flap) after the debridement and before definitive bone grafting.
Local antibiotic carriers maintain the dead space, deliver very high local antibiotic concentrations, and — for PMMA — induce a membrane for later grafting:
Vancomycin 2–4 g plus gentamicin/tobramycin 2–4 g per 40 g cement batch; local concentrations greater than 100 times the MIC for 4–6 weeks; maintains dead space and prevents haematoma colonisation. Remove at 6–8 weeks — prolonged retention risks biofilm on the cement.
Absorbable composite carrier giving high local antibiotic levels with no removal needed; useful when a second stage is not planned.
Antibiotic-impregnated fleece for smaller cavities. The choice of carrier depends on defect size, the structural support needed, and the planned timing of definitive reconstruction.
- Indication
- Defects up to 10–15 cm with a healthy soft-tissue envelope; the workhorse for 4–6 cm defects in optimised hosts
- Technique
- Stage 1 radical debridement plus antibiotic spacer; Stage 2 at 6–8 weeks — remove spacer, preserve the induced membrane, fill with cancellous autograft (often RIA) mixed with antibiotic
- Notes
- Two-stage; the membrane provides vascularised containment and a growth-factor environment
- Indication
- Larger defects (greater than 5–6 cm) or when autograft donor sites are insufficient
- Technique
- External fixator or intramedullary transport nail; transport at 1 mm/day after a latency period; graft the docking site if needed
- Notes
- Long treatment time (1–2 months per cm) but excellent for large segmental loss
- Indication
- Defects greater than 6 cm with poor local vascularity
- Technique
- Microsurgical free flap requiring healthy recipient vessels
- Notes
- Provides immediate structural support and living bone
- Leaving residual sequestrum or sclerotic bone — the most common cause of treatment failure.
- Over-resection that creates excessive bone loss in a B-host who may not tolerate major reconstruction.
- Neurovascular injury during aggressive burring near major vessels or nerves.
- Thermal necrosis from a high-speed burr used without irrigation.
Work systematically from proximal to distal and from superficial to deep. Stop only when you see the paprika sign on the cut surface, the medullary canal walls and the opposite cortex. Any grey or white non-bleeding bone is left behind at the patient's peril — that is the commonest reason for early recurrence.
Aftercare & Complications
Post-operative antimicrobial therapy - Duration: typically 6 weeks of pathogen-specific intravenous antibiotics followed by 2–6 months of oral suppression, guided by infectious diseases and microbiology.
- Route: intravenous initially for severe or resistant organisms, with an early switch to oral when the clinical response and oral bioavailability allow.
- Monitoring: weekly CRP, renal function (for aminoglycosides/vancomycin), and drug levels as indicated.
- Multidisciplinary input: a mandatory infectious-disease consultation for complex or resistant infections. Rehabilitation | Phase | Timing | Weight-bearing & activity | Monitoring & milestones | |------|--------|---------------------------|--------------------------| | Early | 0–6 weeks | Maintain external fixation or cast; non-weight-bearing or touch weight-bearing until soft-tissue healing; gentle ROM of adjacent joints, isometrics | Daily pin-site care; watch for pin-site infection | | Intermediate | 6–12 weeks | Progressive weight-bearing as transport or graft incorporates; transition to a removable brace once stability allows | Remove PMMA spacer/beads at 6–8 weeks if Masquelet planned and graft at the same sitting | | Late | 3–12 months | Full weight-bearing once radiographic union is confirmed; strengthening, gait training, proprioception | Surveillance imaging and CRP every 3 months for the first year, then annually | | Return to function | — | Sedentary work 3–6 months; manual labour 6–12 months or longer with transport; high-impact sport individualised, often permanently restricted | Individualised counselling | Complications
- Incidence context
- 10–30 percent depending on host class and resection adequacy
- Recognition
- Return of sinus, rising CRP, positive cultures, new sequestrum on imaging
- Prevention and management
- Prevent with radical debridement to the paprika sign, complete local antibiotic delivery, host optimisation and stability. Manage with repeat debridement, culture-directed antibiotics; consider amputation in a refractory C-host
- Incidence context
- 5–15 percent after wide cortical resection
- Recognition
- Sudden pain, deformity, loss of alignment through the debrided segment
- Prevention and management
- Prevent with prophylactic stabilisation (external fixator or locked plate) when resection creates a stress-riser. Manage with revision fixation, bone grafting, consider Masquelet or transport
- Incidence context
- 15–25 percent in transport or large defects
- Recognition
- Persistent pain, lack of radiographic healing at 6–9 months
- Prevention and management
- Prevent with stable fixation, adequate graft volume, compression at the docking site. Manage with revision grafting, exchange nailing, additional transport
- Incidence context
- 5–15 percent in complex soft-tissue reconstruction
- Recognition
- Partial or total flap necrosis, exposed bone, recurrent sinus
- Prevention and management
- Prevent by timing the flap after debridement but before grafting, microsurgical planning, smoking cessation. Manage with urgent re-exploration, repeat debridement, alternative flap or skin graft
- Incidence context
- 5–15 percent in severe or recurrent cases, higher in C-hosts
- Recognition
- Uncontrolled infection, non-reconstructible defect, patient request after multiple failures
- Prevention and management
- Prevent with early host optimisation, realistic counselling, a staged approach. Manage with below- or above-knee amputation and prosthetic rehabilitation
- Incidence context
- Rare but classic in decades-long sinuses
- Recognition
- Enlarging mass, bleeding, change in drainage character
- Prevention and management
- Prevent by excising long-standing sinus tracts and sending for histology. Manage with wide local excision or amputation with oncology input
Viva & Exam Focus
CIERNYCIERNY — staging & planning
DEBRIDEDEBRIDE — operative principles
- Why it matters
- Treating all osteomyelitis the same — inadequate resection in Type III/IV or unnecessary wide excision in Type I/II
- Prevention / fix
- Pre-op MRI/CT to map sequestrum, involucrum and sinuses; confirm the type intraoperatively and resect to the paprika sign; Type IV always needs stability and often a flap
- Why it matters
- Any non-bleeding bone left behind acts as a biofilm substrate and guarantees recurrence
- Prevention / fix
- Achieve the paprika sign on all surfaces — cortical, endosteal and medullary
- Why it matters
- Antibiotics before deep cultures give culture-negative or misleading results and a wrong drug choice
- Prevention / fix
- Always obtain multiple deep samples first; hold antibiotics until the cultures are secured
- Why it matters
- The empty space fills with an infected haematoma, and the sinus persists if the space is not managed
- Prevention / fix
- Use antibiotic-loaded PMMA beads or a spacer to occupy the space, deliver high local antibiotic levels and induce a membrane
- Why it matters
- B-hosts have markedly higher recurrence and nonunion rates if reconstruction proceeds unoptimised
- Prevention / fix
- Delay major reconstruction until smoking, diabetes, nutrition and vascular issues are addressed
- Why it matters
- A mobile nonunion prevents infection clearance; micromotion perpetuates the biofilm
- Prevention / fix
- Apply external fixation or an intramedullary device at the index debridement; stability is a biologic requirement for resolution
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old male smoker with poorly controlled diabetes presents with a 9-month history of a draining sinus over the mid-tibia after an open fracture treated with external fixation. MRI shows a 4 cm segmental sequestrum with surrounding involucrum — a Cierny-Mader Type IV lesion. CRP is 45. Outline your management plan including staging, host optimisation and reconstruction strategy.”
“You have performed a radical debridement of a Cierny-Mader Type III tibial osteomyelitis leaving a 5 cm defect. The patient is an A-host. Discuss your options for dead-space management and definitive reconstruction, including timing and rationale.”
“A 68-year-old woman with a 25-year history of chronic osteomyelitis of the tibia presents with an enlarging, bleeding mass at the mouth of a long-standing sinus. Biopsy confirms squamous-cell carcinoma. What is your management?”
Cierny-Mader classification
- Type I medullary: infection inside the canal — reaming or curettage often sufficient
- Type II superficial: cortical surface — decortication to bleeding bone
- Type III localised: full-thickness sequestrum with involucrum — segmental resection feasible
- Type IV diffuse: circumferential involvement, often unstable — wide resection plus stability plus flap usually required
- Host class A normal, B compromised (optimise before reconstruction), C treatment worse than disease (suppression or amputation)
Key surgical principles
- The paprika sign (punctate bleeding from all surfaces) is the endpoint of resection — any residual non-bleeding bone guarantees recurrence
- Obtain multiple deep bone and soft-tissue cultures BEFORE administering antibiotics
- Stability is a biologic requirement for infection clearance — external fixation early if debridement creates instability
- Dead-space management with antibiotic PMMA beads or a spacer is as critical as the resection itself
- Host optimisation (smoking cessation, glycaemic control, nutrition) is mandatory in B-hosts before major reconstruction
Dead-space and reconstruction options
- PMMA beads/spacer: high local antibiotic levels, maintains space, induces the Masquelet membrane; remove at 6–8 weeks
- Masquelet induced membrane: first-line for 4–6 cm defects in optimised hosts — two-stage with excellent incorporation
- Bone transport: for larger defects (greater than 5–6 cm) or insufficient autograft; 1 mm/day after latency
- Vascularised graft (free fibula): large defects with poor local vascularity; microsurgical expertise required
- Soft-tissue flap: when the envelope is deficient — timed after debridement but before definitive bone grafting
Antibiotics and monitoring
- 6 weeks of pathogen-specific IV antibiotics followed by prolonged oral suppression (ID-guided)
- CRP weekly initially, then every 3 months for the first year; a rising CRP prompts re-imaging
- Monitor renal function and drug levels for vancomycin/aminoglycosides
- Multidisciplinary ID input is essential for resistant organisms or complex cases
Complications and prevention
- Recurrence (10–30 percent): prevent by radical debridement to the paprika sign, complete local antibiotic delivery and host optimisation
- Pathological fracture: prophylactic stabilisation when resection creates a stress-riser
- Nonunion: stable fixation, adequate graft, compression at docking sites
- Flap failure: smoking cessation, correct timing, microsurgical planning
- Amputation: realistic counselling in C-hosts or after multiple failures; Marjolin's ulcer in long-standing sinuses
Rehabilitation milestones
- 0–6 weeks: non-weight-bearing, pin-site care, maintain external fixation, gentle ROM
- 6–12 weeks: progressive weight-bearing, remove spacer and graft at 6–8 weeks if Masquelet planned
- 3–6 months: full weight-bearing once radiographic consolidation, strengthening
- Return to work: sedentary 3–6 months, manual labour 6–12 months or more depending on the reconstruction
Background & Evidence
Pathoanatomy. In chronic osteomyelitis a segment of devitalised cortex — the sequestrum — separates and is surrounded by reactive, living new bone, the involucrum. Pus under pressure tracks to the skin surface, forming a sinus tract. Because the sequestrum is avascular it cannot be reached by host defences or antibiotics, so it persists as a permanent nidus for infection until it is excised; a sinus tract present for decades carries a small but classic risk of malignant transformation to squamous-cell carcinoma (Marjolin's ulcer), which is why every long-standing sinus is biopsied at debridement. Cierny-Mader classification. The anatomic type describes where the disease sits and therefore how much bone must be removed; the physiologic host class describes the patient's capacity to heal and therefore whether aggressive reconstruction is justified. Together they set the resection volume, the reconstruction plan, and the perioperative optimisation.
- Description
- Intramedullary infection; reaming may suffice
- Typical resection
- Intramedullary reaming or curettage
- Reconstruction need
- Rarely required; stability if a fracture is present
- Description
- Cortical surface infection, exposed bone
- Typical resection
- Decortication to bleeding bone
- Reconstruction need
- Local wound care or a flap if there is soft-tissue loss
- Description
- Full-thickness cortical sequestrum with involucrum
- Typical resection
- Segmental resection of the necrotic bone
- Reconstruction need
- Often requires bone graft or transport for the defect
- Description
- Circumferential cortical involvement, unstable
- Typical resection
- Wide resection, often segmental
- Reconstruction need
- Always requires stability, a flap and bone reconstruction
Physiologic host classes:
- A-host — normal immune and vascular status; the best candidate for aggressive reconstruction.
- B-host — compromised locally (smoking, vascular disease, radiation) or systemically (diabetes, malnutrition, immunosuppression); requires optimisation before definitive surgery.
- C-host — the treatment risk is greater than the disease burden; consider suppression or amputation. Evidence base. Radical surgical debridement combined with targeted antibiotics remains the cornerstone of treatment for chronic osteomyelitis, and the Cierny-Mader classification guides both the extent of resection and the need for reconstruction. Modern series show that adequate resection to bleeding bone plus local antibiotic delivery and stability achieves infection-free union in 70–90 percent of cases when host factors are addressed, although exact rates vary by anatomic site and host class. The induced-membrane (Masquelet) and bone-transport (Ilizarov/Paley) techniques extended what is reconstructable after radical debridement, making limb salvage realistic even for large segmental defects.
References
A clinical staging system for adult osteomyelitis
- Described the anatomic-physiologic classification (Types I-IV and host classes A/B/C) that remains the standard framework for planning resection extent and reconstruction in chronic osteomyelitis
The concept of induced membrane for reconstruction of long bone defects
- Established the two-stage induced-membrane technique using antibiotic spacer followed by autograft within the preserved membrane as a reliable method for large bone defects
Treatment of posttraumatic bone defects by the induced membrane technique
- Large multicenter series demonstrating high union rates with the induced-membrane technique when radical debridement, membrane preservation and autograft are combined
Ilizarov treatment of tibial nonunions with bone loss
- Landmark series showing Ilizarov bone transport reliably reconstructs large segmental defects after radical debridement of osteomyelitis and septic nonunion
Comparison of bone preserving and radical surgical treatment in calcaneal osteomyelitis
- Radical surgical treatment with adequate resection margins achieved significantly higher infection-free rates than bone-preserving approaches in chronic calcaneal osteomyelitis