Supine position · subcutaneous medial surface · saphenous nerve at risk · tension-free closure
- Supine positioning on a radiolucent table with C-arm access from the contralateral side.
- The saphenous nerve and long saphenous vein lie just medial to the incision and must be identified and protected throughout.
- Dissection is a direct subperiosteal elevation of the thin periosteum off the broad, flat anteromedial surface — there is no true internervous plane.
- The thin soft-tissue envelope makes wound healing the dominant clinical concern — never place the incision directly on the crest.
- This approach cannot address the posterior compartment — plan a combined posteromedial or posterolateral approach if needed.
When & Why
What it exposes. The anteromedial approach gives direct access to the subcutaneous anteromedial surface of the tibial shaft — the broadest and flattest face of the bone, and an ideal plate-bearing surface. It is the workhorse exposure for plate fixation of tibial shaft fractures, bone grafting of nonunions and defects, medial opening-wedge high tibial osteotomy, and debridement for osteomyelitis. Why this approach is chosen. The medial surface of the tibia is subcutaneous along its whole length from the tibial tuberosity to the medial malleolus, so the approach is technically straightforward. It allows direct visualisation and reduction of medial fragments and plate application on a flat surface, and is particularly useful when the fracture pattern or soft-tissue injury precludes intramedullary nailing (medial comminution, bone loss, or a narrow canal). Because the medial compartment is subcutaneous, it demands meticulous soft-tissue technique. Primary indications. - Tibial shaft fractures requiring plate fixation (medial comminution, bone loss, or narrow canal)
- Open tibial fractures with a medial wound requiring direct access
- Nonunion or malunion surgery requiring bone grafting and plate revision
- High tibial osteotomy (medial opening wedge)
- Proximal or distal third fractures needing plate augmentation
- Bone grafting for cystic lesions or osteomyelitis Contraindications. - Severe anteromedial soft-tissue compromise, or an open wound directly over the planned incision
- Active infection
- When posterior column access is required (use a posteromedial or posterolateral approach) Alternative approaches. A lateral approach for the lateral compartment or when medial skin is compromised; a posteromedial approach for posterior column fractures or posteromedial tibial plateau; an anterolateral approach for the lateral plateau or when combining with fibular fixation. Position & landmarks. Supine on a radiolucent table with the C-arm brought in from the contralateral side for AP and lateral views. Slight knee flexion (10 to 15 degrees) relaxes the gastrocnemius; a small bump under the ipsilateral hip helps maintain neutral rotation and the foot is kept accessible for traction. A thigh tourniquet may be applied but, if used, is inflated only after the skin incision and nerve identification. Palpable landmarks are the tibial crest (subcutaneous anterior border, from tuberosity to medial malleolus), the tibial tuberosity (proximal limit), the medial malleolus (distal limit) and the pes anserinus insertion on the proximal medial tibia. The incision runs longitudinally, 1 cm lateral to the palpable tibial crest, centred over the pathology and typically 10 to 15 cm long; mark the course of the long saphenous vein pre-operatively if it is visible.
The Exposure
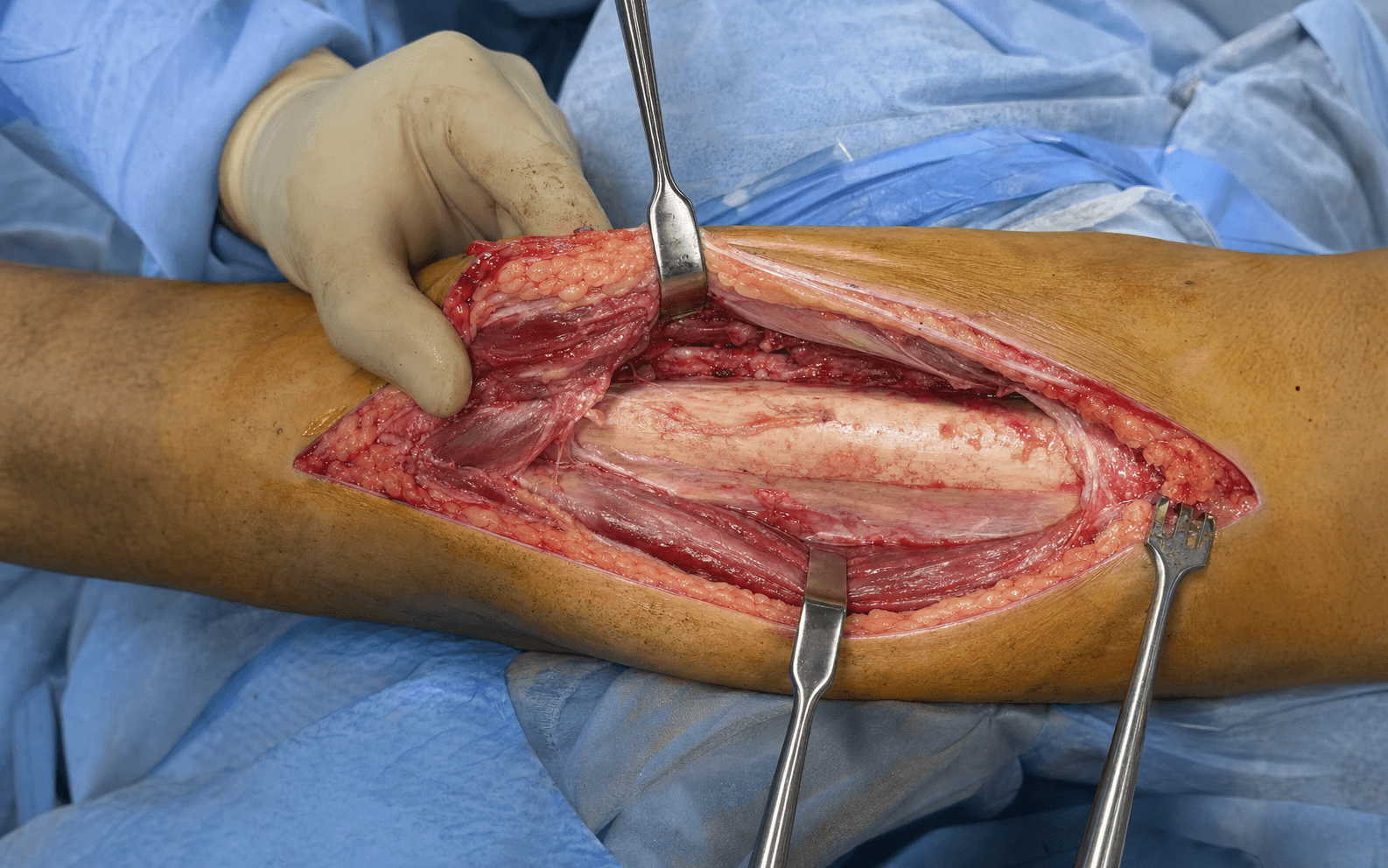
Work down through skin and subcutaneous tissue 1 cm lateral to the crest, identify and protect the saphenous nerve and vein medially, then elevate the thin periosteum directly off the flat anteromedial surface. There is no true internervous plane — the safety of the approach rests on precise incision placement and early identification of the saphenous structures.
Exposure sequence
- Supine on a radiolucent table, C-arm from the contralateral side, slight knee flexion (10 to 15 degrees); pad all pressure points including the contralateral leg.
- Palpate the tibial crest from tuberosity to medial malleolus and mark a line 1 cm lateral to the crest; mark the expected course of the long saphenous vein and saphenous nerve along the medial aspect.
- Plan a longitudinal incision long enough to expose the fracture and place a plate with at least three screws above and below — never directly over the crest.
- Incise skin and subcutaneous tissue in one layer along the marked line, 1 cm lateral to the crest.
- The saphenous nerve and long saphenous vein are encountered immediately, lying just medial to the incision in the subcutaneous plane — identify them at once.
- Place a vessel loop around the saphenous nerve for gentle medial retraction; use bipolar haemostasis.
- Do not use metal retractors on the nerve, do not divide the vein unless essential, and release retraction periodically. Document saphenous sensation before closure.
- Incise the thin fascia over the anteromedial tibia longitudinally; the periosteum is encountered immediately with minimal bleeding in this plane.
- Elevate the thin periosteum directly off the broad, flat anteromedial surface with a periosteal elevator, exposing only as much bone as is needed for reduction and the plate.
- Proximally, the pes anserinus insertion may be partially elevated if required for exposure.
- Use the flat medial surface for anatomic reduction of medial fragments with reduction clamps or cerclage wires; apply a 3.5 mm or 4.5 mm plate with at least three screws above and below the fracture.
- Confirm reduction and plate position, and rule out intra-articular hardware, on AP and lateral fluoroscopy.
- Copious saline irrigation and meticulous haemostasis — the thin envelope makes haematoma particularly problematic.
- Close the fascia loosely or not at all to avoid a compartment syndrome.
- Tension-free skin closure is mandatory — approximate the edges without tension using interrupted sutures or staples; use relaxing incisions or delayed primary closure if the envelope is swollen.
The anteromedial approach is unique because it does not run between two muscles. Its safety depends entirely on precise incision placement (1 cm lateral to the crest) and early identification of the saphenous nerve and vein. The periosteum is thin and easily elevated off the broad flat surface that is ideal for plating; the pes anserinus may be partially elevated with proximal extension.
If a tourniquet is used, limit it to 90 to 120 minutes and inflate only after the skin incision and saphenous nerve identification (the nerve is more vulnerable to compression when inflated). Many surgeons prefer tourniquet-free surgery here to allow continuous assessment of skin perfusion. The real danger of this approach is the thin anteromedial soft-tissue envelope: even minor skin-edge necrosis exposes hardware and risks deep infection.
Dangers & Extensions
Structures at risk, by layer. The saphenous nerve and vein are vulnerable throughout; the nerve lies immediately medial to the incision and becomes more superficial (and so more at risk) with distal extension.
- Structure at risk
- Saphenous nerve with the long saphenous vein, just medial to the incision
- Protection
- Identify early; vessel loop; gentle medial retraction; no metal retractors on the nerve
- Structure at risk
- Infrapatellar branch of the saphenous nerve, crossing distal to the patella
- Protection
- Counsel that division causes sensory loss lateral to the incision; divide cleanly only if essential
- Structure at risk
- Thin periosteum on the flat anteromedial surface
- Protection
- Elevate directly with a periosteal elevator; expose only what is needed; minimal bleeding
- Structure at risk
- Thin anteromedial skin with a tenuous perforator blood supply
- Protection
- Incise 1 cm lateral to the crest; meticulous handling; tension-free closure
Saphenous nerve injury management. If the nerve is transected intra-operatively, perform a primary repair; otherwise document and observe. Post-operative medial-foot sensory loss is usually well tolerated and most patients adapt. A painful neuroma that is refractory to desensitisation may require later exploration and neurectomy.
Wound complications after anteromedial tibial plating range from 5 to 15 percent in published series — significantly higher than intramedullary nailing. Risk factors include smoking, diabetes, open fractures, and incisions placed directly over the crest. Meticulous soft-tissue technique is far more effective than treating an established complication.
- Incidence
- 5 to 15 percent
- Prevention
- Tension-free closure, meticulous handling
- Treatment
- Debridement, negative-pressure therapy, flap coverage
- Incidence
- 2 to 8 percent
- Prevention
- Prophylactic antibiotics, soft-tissue care
- Treatment
- Irrigation and debridement, antibiotics, retain hardware if stable
- Incidence
- 3 to 5 percent
- Prevention
- Careful nerve handling, vessel-loop protection
- Treatment
- Observation, neurectomy if refractory
- Incidence
- 2 to 5 percent
- Prevention
- Stable fixation, bone graft when indicated
- Treatment
- Revision ORIF with grafting
- Incidence
- 2 to 5 percent
- Prevention
- Chemoprophylaxis, early mobilisation
- Treatment
- Anticoagulation
Extensile options. Extend proximally along the medial border of the patellar tendon to reach the anteromedial tibial plateau for proximal-third or combined plateau–shaft injuries (the pes anserinus may be partially elevated; the saphenous nerve is more superficial here). Extend distally along the same line toward the medial malleolus for distal-third or pilon-variant fractures — the highest-risk zone, as the saphenous nerve crosses more superficially; consider a separate incision if extensive distal exposure is needed. For complex multi-column injuries, combine with a posteromedial approach (bicondylar plateau with medial involvement) or a lateral/anterolateral approach (lateral comminution), staged or simultaneous according to the soft-tissue condition. Closure principles. Irrigate copiously and secure haemostasis. Close the fascia loosely or not at all — tight closure in this limited-volume compartment risks a compartment syndrome and compromises skin perfusion. Skin closure must be tension-free with interrupted sutures or staples (a continuous suture can strangulate the edges); plan relaxing incisions or delayed primary closure when the envelope is swollen. Confirm reduction and plate position on AP and lateral fluoroscopy and obtain full-length films if length or alignment is in doubt.
Procedures Through This Approach
- Open reduction and internal fixation of tibial shaft fractures with a medial plate — the principal use, especially for medial comminution, bone loss, or a narrow canal where nailing is contraindicated.
- Bone grafting of nonunions, bone defects and cystic lesions.
- Medial opening-wedge high tibial osteotomy for medial-compartment knee osteoarthritis with varus malalignment.
- Debridement and sequestrectomy for osteomyelitis.
- Plate augmentation of intramedullary-nail constructs when additional medial stability is needed. Recovery & aftercare. Check and document saphenous nerve sensation on the medial foot and inspect the wound for tension or haematoma, with the limb elevated above heart level. Weight bearing is non- or touch-weight-bearing for 6 to 12 weeks depending on stability, progressing on radiographic healing; aim for full knee and ankle range of motion by 6 to 8 weeks. Follow-up is typically at 2 weeks (wound check, suture removal), 6 weeks and 12 weeks (radiographs and weight-bearing progression), 6 months and 1 year. DVT prophylaxis (LMWH or aspirin per protocol) continues until the patient is mobile — a minimum of 2 weeks, often 4 to 6 weeks.
Viva & Exam Focus
ANTMEDIALANTMEDIAL — the anteromedial tibial shaft exposure
Hook:ANTMEDIAL — stay 1 cm lateral to the crest and protect the saphenous nerve.
Operative Surgery viva scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old motorcyclist sustains a tibial shaft fracture with a large medial butterfly fragment on CT. How would you approach this?”
“A 48-year-old with medial-compartment osteoarthritis is planned for a medial opening-wedge high tibial osteotomy. Describe your surgical approach.”
“Ten days after anteromedial plating of a tibial shaft fracture, the patient develops wound-edge necrosis with an exposed plate. What is your management?”
Patient position
- Supine on a radiolucent table
- C-arm from the contralateral side
- Slight knee flexion (10 to 15 degrees)
- Tourniquet optional — inflate only after nerve identification
- Pad all pressure points
Incision landmarks
- 1 cm lateral to the palpable tibial crest
- Longitudinal, centred over the fracture
- Mark the saphenous vein course pre-operatively
- Proximal extension toward the tibial tuberosity
- Distal extension toward the medial malleolus
Saphenous nerve protection
- Identify early, before deep dissection
- Vessel loop or tape sling for gentle retraction
- No metal retractors directly on the nerve
- The nerve lies immediately medial to the incision
- Document sensation before and after surgery
Internervous plane and dissection
- No true internervous plane (subcutaneous surface)
- Direct subperiosteal elevation on flat anteromedial bone
- Periosteum is thin and easily elevated
- Expose only as much bone as the plate needs
- Pes anserinus may be partially elevated proximally
Wound closure principles
- Tension-free skin closure is mandatory
- Close the fascia loosely or not at all
- Avoid continuous suture — use interrupted sutures or staples
- Consider relaxing incisions or delayed closure if tense
- Meticulous skin-edge handling throughout
Complications and prevention
- Wound necrosis 5 to 15 percent — meticulous technique prevents it
- Saphenous nerve injury — identify and protect early
- Infection 2 to 8 percent — higher with open fractures
- Nonunion 2 to 5 percent — stable fixation and grafting when needed
- DVT prophylaxis until mobile
References
The epidemiology of tibial fractures
- Tibial shaft fractures are the most common long bone fracture with a bimodal distribution
- High-energy injuries predominate in young males, low-energy in elderly females
- Anteromedial plating remains relevant despite the dominance of intramedullary nailing for specific fracture patterns
Complications after tibial plateau fracture surgery
- Anatomic reduction and stable fixation are critical for outcome
- Wound complications are significantly higher with medial approaches in compromised soft tissue
- CT-based planning improves approach selection and reduces complications
Wound complications in tibial plafond fractures
- Staged management with spanning external fixation reduces wound complications
- Anteromedial skin is particularly vulnerable due to its subcutaneous position
- Tension-free closure and meticulous soft-tissue handling are essential principles
Proximal tibial varus osteotomy for osteoarthritis of the lateral compartment of the knee
- Proximal tibial osteotomy via the anteromedial approach gives reliable correction for lateral-compartment OA
- Precise surgical technique determines long-term success in HTO
- Saphenous nerve protection is critical during proximal exposure
Injury to the infrapatellar branch of the saphenous nerve in arthroscopic knee surgery
- The infrapatellar branch of the saphenous nerve is at risk in medial knee approaches
- Early identification and protection reduce permanent sensory deficit
- Most patients adapt to medial-foot sensory loss, but a painful neuroma requires intervention