Midline anterior-knee approach · intermediate
- Patellar tendon rupture occurs in YOUNGER patients (less than 40), contrasting with quadriceps rupture (greater than 40, systemic disease).
- AUGMENTATION is almost always required — it drops the re-rupture rate from 15–20 percent down to 2–5 percent.
- Restore PATELLAR HEIGHT to the contralateral side using the Insall-Salvati ratio (target 1.0), confirmed on intraoperative lateral fluoroscopy.
- Tie the sutures with the knee at 30 degrees flexion — tying in extension over-tensions the repair and produces patella baja.
- The rupture is typically at the inferior pole (bone-tendon junction) in 80 percent; suspect systemic disease (SLE, RA, CKD, steroids, fluoroquinolones) when the patient is older or the rupture is bilateral.
- “EXAM KEY: rupture typically at the inferior pole of the patella (the bone-tendon junction) in 80 percent of cases.
- “Insall-Salvati ratio = patellar TENDON length divided by patella length (normal 0.8–1.2).
- “Flexible suture-tape augmentation is now preferred over cerclage wire — fewer complications and no removal.
- “Suture anchors are biomechanically equivalent to transosseous tunnels; the old 'anchors are weaker' teaching is outdated.
When & Why
Indications. Repair a patellar tendon rupture when the extensor mechanism is lost — a complete rupture with loss of active knee extension, a palpable gap at the inferior pole with a high-riding patella, and an inability to straight-leg-raise. Relative indications include a partial rupture of greater than 50 percent of the tendon width with significant extensor weakness, a chronic rupture with functional limitation, and re-rupture after a previous repair. Timing drives the operation. Acute complete ruptures are repaired early, ideally within two weeks, where primary repair with augmentation gives the best tissue and the best outcomes. The subacute window (two to six weeks) may still permit primary repair depending on tissue quality and retraction. Beyond six weeks the tendon retracts, the quadriceps shortens and adheres, and the operation shifts from repair to reconstruction.
Primary repair with augmentation — the standard, best tissue, best outcomes.
Primary repair still often achievable; depends on tissue quality and retraction.
Reconstruction over repair — semitendinosus autograft, Achilles allograft or V-Y lengthening to restore length and continuity.
Contraindications. Absolute contraindications are active infection at the surgical site, a non-functional knee (pre-existing severe arthritis or a neurological deficit), and medical contraindication to surgery. Relative contraindications include severe peripheral vascular disease, uncontrolled diabetes, active malignancy requiring urgent treatment, and the non-ambulatory patient with minimal functional demand. Special situations demand a heavier hand: steroid use raises re-rupture risk and makes augmentation essential; dialysis or chronic kidney disease leaves compromised tissue that must be augmented heavily; and a rupture after total knee arthroplasty may need component revision just to gain access. Pre-operative assessment. Clinically, expect a palpable defect at the inferior pole, a high-riding patella (patella alta), an inability to straight-leg-raise and a suprapatellar haematoma, and test for associated injuries (bone avulsion, retinacular tears). Imaging: - Lateral radiograph — confirms patella alta (Insall-Salvati greater than 1.2) and may show an avulsion fragment at the inferior pole.
- Contralateral lateral radiograph — for patellar-height comparison, the single most useful planning film.
- MRI — defines rupture location, retraction and tissue quality, and is most useful for partial ruptures where the diagnosis is uncertain. Consent. Counsel for an 80–95 percent return to pre-injury activity level with an augmented repair, a re-rupture rate of 2–5 percent with augmentation versus 15–20 percent without, knee stiffness as the most common complication, and possible hardware removal if cerclage wire is used. Setup. Supine on a radiolucent table with a tourniquet on the proximal thigh (250–300 mmHg) and a bump under the knee for slight flexion. Both knees are prepped and draped so a true lateral of the contralateral knee can be obtained for patellar-height comparison — this is the critical setup step that protects the repair. General or spinal anaesthesia; a nerve block aids postoperative analgesia.
The Operation
The goal is to re-establish the extensor mechanism by reattaching the tendon to the inferior pole of the patella, restoring normal patellar height, and protecting the repair with augmentation. The exposure is laid out in full as the first steps of the sequence below.
Operative sequence
- Supine, radiolucent table, tourniquet on the proximal thigh (250–300 mmHg), bump under the knee for slight flexion.
- Both knees prepped and draped so a true lateral of the contralateral knee can be obtained — the make-or-break comparison film for patellar height.
- Mark the patella borders, the tibial tubercle and the palpable defect at the rupture site; plan a midline incision.
- An 8–10 cm midline longitudinal incision from the inferior pole of the patella to the tibial tubercle. Midline preserves future surgical options such as total knee arthroplasty.
- Raise full-thickness skin flaps. Identify the high-riding patella (pathognomonic for complete rupture) and the defect at the inferior pole.
- Avoid extensive medial dissection to protect the infrapatellar branch of the saphenous nerve (IPBSN); stay on the midline.
- Define the tendon stumps, the medial and lateral retinaculum, and the haematoma (which carries growth factors — do not wash it all away).
- Locate the proximal stump at the inferior pole of the patella and the distal stump at the tibial tubercle.
- Assess tendon quality and look for a sleeve fracture (a bone fragment still attached to tendon) — good bone gives a secure anchor and may change the fixation strategy.
- Grade the tear (complete versus partial greater than 50 percent) and note retinacular extension.
- Debride only frayed, devitalised tissue to create healthy bleeding edges for healing.
- Do NOT over-debride — excessive shortening creates patella baja. Preserve every millimetre of tendon length.
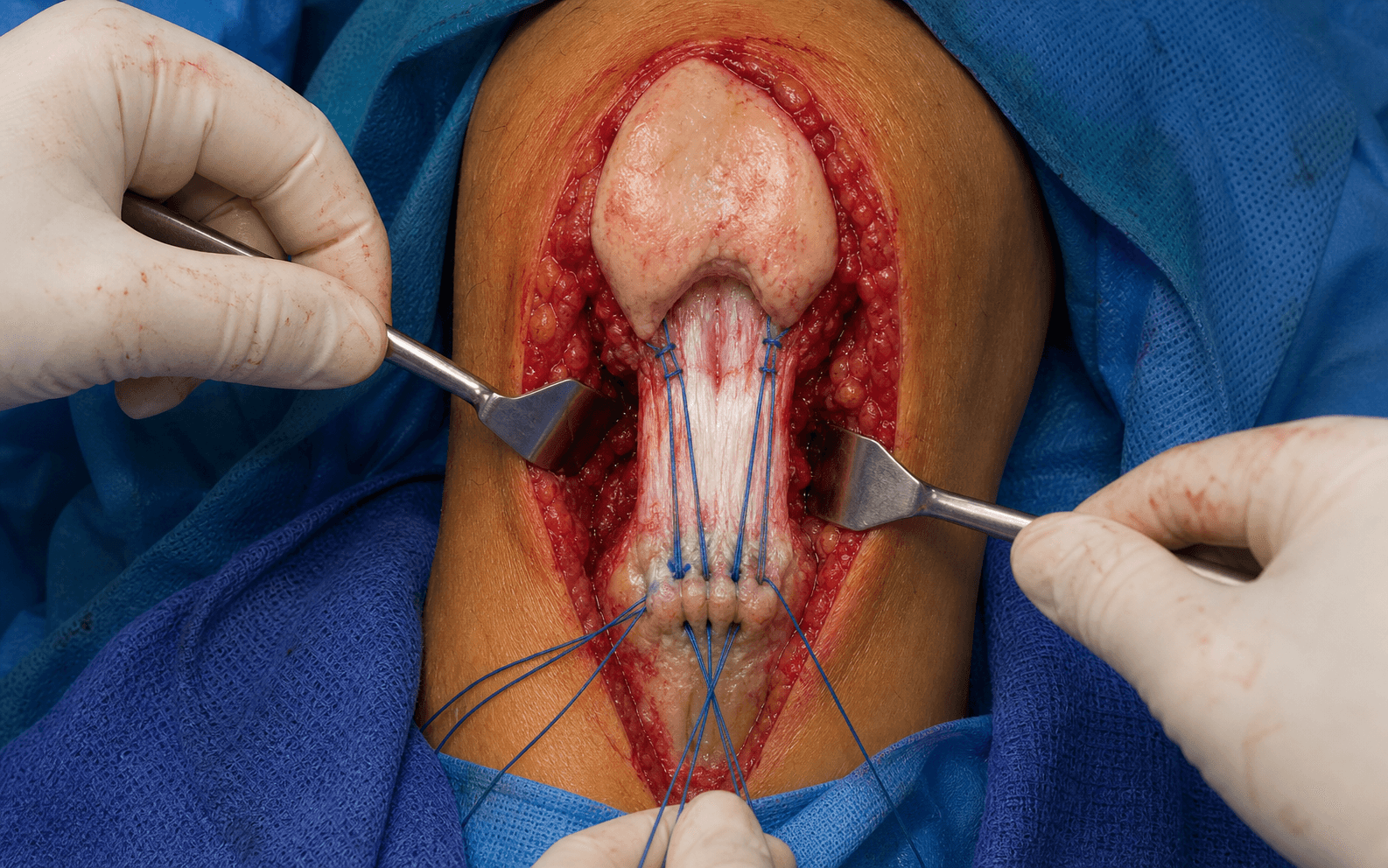
- Run a Krackow locking whipstitch through the distal stump with heavy non-absorbable suture (#2 or #5 Ethibond or FiberWire), at least four locking passes per strand for a secure grip.
- The locking throw is what resists pull-out in degenerated tendon; FiberTape may be added for greater strength.
- Keep the strands organised (medial, central, lateral) for even tension later.
- Drill two to three vertical transosseous tunnels in the inferior pole of the patella with a 2.0–2.5 mm bit, exiting at the superior pole — single pass per tunnel to avoid patellar fracture.
- Suture anchors are an equivalent alternative: pooled biomechanical data show anchors give EQUAL ultimate load to failure and LESS cyclic gap formation than transosseous sutures (Imbergamo 2022; Ettinger 2013), so the old teaching that anchors are "weaker" is outdated. Choose by bone quality and familiarity; in osteoporotic bone, augmentation matters more than the tunnel-versus-anchor choice.
- Thread the Krackow strands through the tunnels (inferior to superior) and draw the tendon to its anatomic footprint.
- Bring the knee to 30 degrees flexion and tension the repair to restore NORMAL patellar height, confirmed against the contralateral knee on lateral fluoroscopy (Insall-Salvati ratio 1.0).
- ALWAYS compare to the other side. Under-tension equals patella alta (weak extension, re-rupture risk); over-tension equals patella baja (stiffness, patellofemoral pain).
- Tie all sutures over the superior pole of the patella with the knee held at 30 degrees flexion — multiple throws, knots buried.
- Tying in extension over-tensions the repair as soon as the knee flexes; tying at 30 degrees protects it during early range of motion.
- Augment almost every patellar tendon repair — unlike quadriceps repair, augmentation is the rule, not the exception. It drops re-rupture from 15–20 percent to 2–5 percent.
- Suture tape (preferred): FiberTape passed through a patellar tunnel and the tibial tubercle, tensioned to limit flexion to 90 degrees initially — low profile, no hardware removal.
- Cerclage wire (alternative): a figure-of-eight 1.2–1.6 mm wire from patella to tibial tubercle, removed at 3–6 months.
- Confirm active extension — the patient should straight-leg-raise on the table.
- Repair the medial and lateral retinacular tears, which contribute to extensor function.
- Document final patellar height on a lateral radiograph; layered closure over a drain.
Patella baja (over-tension) causes stiffness and patellofemoral pain and is far harder to correct secondarily than patella alta; patella alta (under-tension) leaves a weak repair and a persistent extensor lag that raises re-rupture risk. Always compare to the contralateral side on intraoperative lateral fluoroscopy, tie with the knee at 30 degrees flexion (never in extension), and check height BEFORE applying augmentation.
AUGMENTATION is almost always needed for patellar tendon repair — unlike quadriceps repair. Re-rupture falls from 15–20 percent to 2–5 percent with it. Flexible suture tape is preferred over cerclage wire (fewer complications, no removal). Omitting augmentation is the classic avoidable failure.
The infrapatellar branch of the saphenous nerve (IPBSN) crosses medially and is at risk with medial extension of the incision — injury causes anterior knee numbness. Stay midline and avoid extensive medial dissection.
Chronic rupture — when repair becomes reconstruction A rupture older than six weeks retracts and shortens, the quadriceps adheres and contracts, and simple end-to-end repair is rarely possible. The goal shifts to reconstructing the extensor mechanism and restoring patellar height, with the patient counselled for prolonged rehabilitation and possible secondary procedures.
Harvest the ipsilateral semitendinosus, route it through patellar and tibial tunnels, and augment with the remaining native tendon.
Bone block fixed to the tibial tubercle, tendon woven and sutured to the patella — provides length for retracted, short gaps.
For 2–4 cm gaps with a retracted quadriceps: a V-incision in the quadriceps, slide distally, close as a Y to gain length.
Chronic ruptures need RECONSTRUCTION, not repair. The key is restoring patellar height and extensor-mechanism continuity. Prepare the patient for prolonged rehabilitation and possible secondary procedures.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | 0–2 weeks | Hinged brace locked in extension; weight-bear as tolerated in the brace | Passive ROM 0–30 degrees only; straight-leg-raise and quad isometrics | | 2 | 2–6 weeks | Unlock the brace, progress flexion to 0–90 degrees | Active-assisted ROM; continued quad strengthening; pool therapy once healed | | 3 | 6–12 weeks | Discontinue brace once good quad control | Progress to full ROM; closed-chain strengthening; stationary cycling | | 4 | 3–6 months | — | Light activities; sport-specific training; wire removal if symptomatic | | 5 | 6+ months | — | Return to full activity once full ROM, quad strength greater than 80 percent of the other side, no pain or instability, and healing on imaging | Most patients return to sport at 6–9 months. With an augmented repair, 80–95 percent return to their pre-injury activity level. Complications
- Recognition
- Sudden pain, loss of extension, palpable gap
- Prevention
- Augmentation, protected ROM, avoid early flexion beyond 90 degrees
- Management
- Revision repair with graft augmentation
- Recognition
- Anterior knee pain, stiffness, limited flexion
- Prevention
- Intraoperative comparison to the contralateral side; do not over-tension
- Management
- Difficult to correct — may need tendon Z-lengthening
- Recognition
- Extensor lag, weak extension, quadriceps insufficiency
- Prevention
- Restore normal Insall-Salvati ratio (1.0)
- Management
- Revision with appropriate tensioning
- Recognition
- Limited ROM at follow-up, especially flexion
- Prevention
- Early protected ROM; avoid excessive immobilisation
- Management
- Aggressive physiotherapy; may need MUA or arthroscopy
- Recognition
- Palpable wire ends, local irritation
- Prevention
- Prefer suture tape; remove wire early
- Management
- Remove broken wire; assess tendon healing
- Recognition
- Palpable wire or anchor, skin irritation
- Prevention
- Bury knots; use low-profile augmentation
- Management
- Hardware removal once healed
- Recognition
- Intraoperative or postoperative patella fracture
- Prevention
- Small drill bits, single pass per tunnel, protect with augmentation
- Management
- ORIF if displaced; may need cerclage
- Recognition
- Erythema, drainage, fever
- Prevention
- Prophylactic antibiotics, aseptic technique
- Management
- Debridement and antibiotics; retain the repair if possible
Viva & Exam Focus
JUMPJUMP — risk factors for patellar tendon rupture
PATCHPATCH — steps of patellar tendon repair
Risk during tunnel drilling. Use small drill bits (2.0–2.5 mm), a single pass per tunnel, and an eccentric path in osteopenic bone. Protect the construct with augmentation.
A saphenous nerve branch at risk with medial extension of the incision — injury causes anterior knee numbness. Stay midline.
Over-tensioning creates patellofemoral pain and stiffness. Verify height with fluoroscopy against the contralateral side and tie at 30 degrees flexion.
Under-tensioning leaves a weak repair and a persistent extensor lag, increasing re-rupture risk. Restore the normal Insall-Salvati ratio.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old male basketball player presents to ED after landing awkwardly from a jump. He felt a pop in his knee and cannot straighten it. On examination there is a palpable defect below the patella and he cannot perform a straight-leg-raise. X-ray shows patella alta. How would you manage this patient?”
“During patellar tendon repair, you are tensioning the repair and notice the patella appears lower than the contralateral side on the lateral radiograph. What is the concern and how do you address it?”
“A 52-year-old diabetic woman on long-term steroids for rheumatoid arthritis presents with a patellar tendon rupture. How does her medical history influence your surgical approach?”
Key indications
- Complete patellar tendon rupture with loss of straight-leg-raise
- Palpable gap at the inferior pole plus patella alta on the lateral radiograph
- Younger patients (less than 40) — contrast with quadriceps (greater than 40)
Critical anatomy
- Insall-Salvati ratio = patellar tendon length divided by patella length (normal 0.8–1.2)
- Rupture at the inferior pole (bone-tendon junction) in 80 percent
- Risk factors: jumpers knee, steroids, fluoroquinolones, RA, SLE
Critical steps
- Krackow locking sutures through the distal tendon stump
- Two to three transosseous tunnels in the inferior pole of the patella
- Restore patellar height — compare to the contralateral side (Insall-Salvati 1.0)
- Tie the sutures with the knee at 30 degrees flexion
- AUGMENTATION essential — suture tape preferred over wire
Danger zones
- Patella baja (over-tension) — stiffness, patellofemoral pain
- Patella alta (under-tension) — re-rupture risk
- Patellar fracture from drilling
- Infrapatellar nerve medially
Post-op pearls
- Brace locked in extension for two weeks, ROM to 90 degrees by six weeks
- Wire removal at 3–6 months if used
- Return to sport at 6–9 months
- Re-rupture 2–5 percent with augmentation versus 15–20 percent without
Exam tips
- AUGMENTATION differentiates this from quadriceps repair
- Younger patients (less than 40) versus quadriceps (greater than 40)
- Suture tape is now preferred over cerclage wire
- A chronic rupture needs reconstruction, not repair
Background & Evidence
Tendon anatomy. The patellar tendon is the continuation of the quadriceps mechanism passing over the patella: it originates at the inferior pole of the patella and inserts on the tibial tubercle, measuring roughly 4–5 cm in length, 3 cm in width at the insertion and 3–5 mm in thickness. Blood supply. The inferior pole is supplied by branches of the inferior genicular vessels and the tibial insertion by recurrent tibial vessels, with a relatively avascular mid-substance watershed area — the zone most vulnerable to degeneration and rupture. Rupture location. The inferior pole of the patella (the bone-tendon junction) accounts for 80 percent of ruptures; mid-substance ruptures (10 percent) suggest underlying tendinopathy (jumpers knee); and tibial tubercle avulsion (10 percent) is seen especially in adolescents. Insall-Salvati ratio. The patellar tendon length divided by the patellar length, measured on a true lateral radiograph. It is the intraoperative target for restoring height (aim for 1.0, matching the contralateral side).
- Interpretation
- Normal
- Interpretation
- Patella alta — tendon too long, or a high-riding patella
- Interpretation
- Patella baja — tendon too short, or a low-riding patella
Epidemiology. Patellar tendon rupture is much less common than quadriceps rupture and tends to affect younger, active patients (typically less than 40), often athletes with a history of jumpers knee, in contrast to the quadriceps rupture of older patients with systemic disease. Systemic risk factors — SLE, rheumatoid arthritis, chronic kidney disease, diabetes, steroid use and fluoroquinolones — weaken the tendon and should be suspected whenever the demographic is atypical or the rupture is bilateral (a frequently missed diagnosis). ### Guidelines, registries and global practice There is no single national-society guideline dedicated to patellar tendon repair; practice is driven by Level III–IV evidence and biomechanical studies that are consistent worldwide. Key points of global consensus and where practice genuinely varies: | Question | Global consensus | Where practice differs | |----------|------------------|------------------------| | Timing | Acute complete ruptures repaired early (ideally within two weeks) — uniform across AAOS, BOA and AO Foundation teaching | The subacute window (2–6 weeks) tolerance varies by surgeon and tissue quality | | Bone-side fixation | Transosseous tunnels OR suture anchors are both acceptable and biomechanically equivalent | North American and European sports units increasingly favour suture anchors and suture-tape internal bracing; transosseous remains common globally and in resource-limited settings | | Augmentation | Augmentation protects the repair and lowers re-rupture | Flexible suture tape is now preferred over cerclage wire where available; cerclage or wire is still widely used where suture-tape implants are cost-prohibitive | | Rehabilitation | Protected progressive ROM in a hinged brace | A trend toward earlier ROM in well-augmented constructs, balanced against meta-analysis evidence (Serino 2017) that early mobilisation raises adverse events | Resource-setting note. Transosseous tunnel repair with heavy non-absorbable suture and a stainless-steel cerclage or Mersilene-tape frame remains an entirely valid, low-cost technique with comparable mechanical resistance — important globally where proprietary suture-anchor and suture-tape implants are unavailable.
References
Acute and old ruptures of the extensor apparatus of the knee in adults (excluding knee replacement)
- Patellar tendon tears typically affect patients under 40, often athletes — contrasting with quadriceps tears (over 40, systemic disease)
- Surgery is mandatory in all complete patellar tendon ruptures; technique is end-to-end suture or transosseous reinsertion
- Repair is protected by tendon augmentation in most cases
- Chronic (old) lesions often require tendon graft or bone-tendon-bone graft
Failure Rates of Suture Anchor Fixation Versus Transosseous Tunnel Technique for Patellar Tendon Repair: A Systematic Review and Meta-analysis of Biomechanical Studies
- Pooled 7 biomechanical studies, 128 cadaveric specimens (66 suture anchor, 62 transosseous)
- Suture anchor fixation produced significantly LESS cyclic gap displacement than transosseous tunnels (p less than 0.001)
- No significant difference in ultimate load to failure between the two constructs (p = 0.465)
Biomechanical properties of suture anchor repair compared with transosseous sutures in patellar tendon ruptures: a cadaveric study
- 30 human cadaveric patellar tendons: titanium anchors, hydroxyapatite anchors, or transpatellar Krackow tunnels
- Suture anchor repair gave significantly less gap formation during cyclic loading (p less than 0.05)
- Suture anchor repair resisted significantly higher ultimate failure loads than transosseous sutures (p less than 0.05)
- Transosseous constructs failed by suture rupture at lower load
Patellar tendon restoration techniques: a systematic review of outcomes for repair and reconstruction methods
- 23 studies, 738 patients across acute, chronic, post-TKA and post-ACL reconstruction settings
- Acute primary repairs with and without augmentation gave comparable Lysholm scores (range 84–99.5)
- Cerclage augmentation yielded the LOWEST Lysholm scores and is no longer recommended
- In post-TKA patients, allograft reconstruction gave superior Knee Society Scores
Comparison of adverse events and postoperative mobilization following knee extensor mechanism rupture repair: A systematic review and network meta-analysis
- 23 studies, 709 patients with acute traumatic extensor mechanism ruptures
- No single repair method was biomechanically or clinically superior for adverse-event or reoperation rates
- Early or immediate mobilisation was associated with significantly higher adverse-event rates than immobilisation for at least 6 weeks (p = 0.02)
- No significant difference in muscle strength or thigh atrophy between transosseous drill holes and simple end-to-end suture
Further reading 1. Enad JG. Patellar tendon repairs. J South Orthop Assoc. 1999;8(1):20-24. 2. Bhargava SP, Hynes MC, Dowell JK. Traumatic patella tendon rupture: early mobilisation following surgical repair. Injury. 2004;35(11):1158-1160. 3. Ramseier LE, Werner CM, Heinzelmann M. Quadriceps and patellar tendon rupture. Injury. 2006;37(6):516-519. 4. Matava MJ. Patellar tendon ruptures. J Am Acad Orthop Surg. 1996;4(6):287-296. 5. Greis PE, Holmstrom MC, Lahav A. Surgical treatment options for patella tendon rupture, Part I: Acute. Orthopedics. 2005;28(7):672-679. 6. Cree C, Pillai A, Jones B, Blyth M. Bilateral patellar tendon ruptures: A missed diagnosis. Knee Surg Sports Traumatol Arthrosc. 2007;15(11):1350-1354. 7. West JL, Keene JS, Kaplan LD. Early motion after quadriceps and patellar tendon repairs: outcomes with single-suture augmentation. Am J Sports Med. 2008;36(2):316-323. 8. Rougraff BT, Reeck CC, Essenmacher J. Complete quadriceps tendon ruptures. Orthopedics. 1996;19(6):509-514. 9. Camarda L, Giannice G, Lauria M, Minacapelli A, D'Arienzo M. Surgical treatment of acute patellar tendon rupture with suture anchors. Muscles Ligaments Tendons J. 2017;7(2):294-299. 10. Bushnell BD, Tennant JN, Rubright JH, Creighton RA. Repair of patellar tendon rupture using suture anchors. J Knee Surg. 2008;21(2):122-129.