Deltopectoral approach · re-attachment to the lateral lip of the bicipital groove · acute and chronic rupture
- Pectoralis major has TWO heads - clavicular (superior, smaller) and sternal (inferior, larger). The sternal head typically ruptures.
- Most common mechanism: an eccentric load to a maximally contracted muscle during bench press, tackling or wrestling (bench press about 80 percent of cases).
- Sixty percent of tears occur at the musculotendinous junction, 30 percent as bone avulsion from the lateral lip of the bicipital groove, and 10 percent in the muscle belly.
- The musculocutaneous nerve pierces coracobrachialis 5-8cm distal to the coracoid - the primary nerve at risk during inferior dissection.
- TIMING: Acute repair within 6 weeks (ideally within 2 weeks) gives 85-95 percent excellent results. Chronic repair beyond 6 weeks is still worthwhile but outcomes fall to 70-80 percent.
- FIXATION: 2-4 suture anchors along the lateral lip of the bicipital groove at a 45-degree 'deadman' angle, with horizontal mattress sutures through the tendon 1cm from the edge.
- REHABILITATION: NO active pectoralis contraction for 6 weeks - protocol violations are the leading cause of re-rupture (overall re-rupture rate 5-20 percent).
When & Why
Indication. A pectoralis major tendon rupture in an active patient - sudden pain and a pop during an eccentric load, loss of the anterior axillary fold, weakness of adduction and internal rotation, and a complete (Grade III) tear confirmed on MRI - that will benefit from restoration of strength and contour. The strong driver is a high-demand patient (athlete, manual worker, military) with a complete acute rupture, where surgery gives 85-95 percent good to excellent results versus 40-60 percent persistent weakness without surgery. Absolute indications
- Complete pectoralis major tendon rupture (Grade III) in an active patient
- Acute complete rupture in athletes or high-demand workers
- Displaced bone avulsion fractures
- Failed non-operative management of partial tears with persistent symptoms Relative indications
- Symptomatic partial tears (Grade II) with weakness or pain
- Chronic ruptures (greater than 6 weeks) with cosmetic deformity and functional deficit in a motivated patient
- Revision of a failed primary repair
- High-demand occupation requiring strength (manual labour, military) Contraindications
- Medical comorbidities precluding surgery
- Low-demand elderly patients with minimal symptoms
- Complete muscle belly tears with severe retraction (poor tissue for repair)
- Significant muscle atrophy in chronic tears (greater than 6-12 months) - consider tendon transfer instead
- Active infection Workup. Confirm the diagnosis and plan the repair. The mechanism is classically an eccentric load to a maximally contracted muscle (bench press about 80 percent, wrestling/tackling 15 percent, other 5 percent), with a sudden pop or tearing sensation and immediate pain, rapid swelling and ecchymosis over the anterior chest and arm. On examination look for loss of the anterior axillary fold with an asymmetric chest contour, a palpable gap at the insertion (acute) or a retracted tendon mass medially (chronic), weakness of resisted adduction and internal rotation, and a positive modified push-up test; passive ROM is usually full. Plain radiographs (AP and axillary) are usually normal but may show a bone avulsion fragment. Ultrasound can dynamically show retraction and a gap but is operator-dependent. MRI is the gold standard - it confirms rupture, shows the location (musculotendinous versus bone), quantifies retraction, and in chronic tears demonstrates muscle atrophy. Consent specifically for re-rupture (5-10 percent acute, 15-20 percent chronic), a 5-10 percent persistent strength deficit even after a successful acute repair, residual cosmetic deformity (especially chronic repairs), infection (1-2 percent), nerve injury - most often a musculocutaneous neuropraxia (1-2 percent) - and the absolute need for 6 weeks of strict protection. Setup. Beach chair (60-70 degrees elevation) or supine with a bump under the ipsilateral scapula. The arm is draped free on a mobile arm board so it can be moved through full ROM for tensioning and testing. Prophylactic antibiotics (e.g. Cefazolin 2g IV within 60 minutes) and standard shoulder prep.
The Operation
The goal: expose the insertion through the deltopectoral approach, retrieve and mobilise the retracted tendon, prepare the lateral lip of the bicipital groove, re-attach the tendon under correct tension with suture anchors at the 45-degree deadman angle, and protect the musculocutaneous, pectoral and axillary nerves throughout. The exposure is laid out in full below (and in depth on the deltopectoral approach to the shoulder page).
Operative sequence
- Palpate the coracoid process medially and the deltopectoral groove; in acute ruptures a defect is often palpable at the anterior axillary fold.
- Make an 8-12cm incision along the deltopectoral groove, starting 2cm below the clavicle at the coracoid level and extending toward the axilla - centred on the anticipated pectoralis insertion (the lateral lip of the bicipital groove).
- Incise skin and subcutaneous tissue; identify the cephalic vein in the groove - preserve and retract it laterally with the deltoid (preferred) to avoid venous congestion, or ligate and divide if necessary.
- This is a true internervous plane - deltoid (axillary nerve, C5-6) lateral, pectoralis major (medial and lateral pectoral nerves) medial; no motor nerve crosses it, making it safe for dissection.
- In an acute rupture, evacuate the haematoma obscuring the anatomy, then develop the interval with blunt finger dissection.
- Retract deltoid laterally and pectoralis major medially with a self-retaining retractor; visualise the conjoint tendon (coracobrachialis and short head of biceps), the long head of biceps in the groove, and the pectoralis insertion site deep.
- Acute rupture (less than 6 weeks): the tendon is retracted 3-5cm medially, surrounded by haematoma - palpate medially to find the stump; tissue quality is good.
- Chronic rupture (greater than 6 weeks): retracted 5-10cm, scarred to the chest wall, with muscle atrophy and friable tissue - extensive mobilisation is required, extending exposure medially and inferiorly to retrieve the stump.
- Assess the rupture location (musculotendinous junction 60 percent, bone avulsion 30 percent, muscle belly 10 percent) and which head is torn - typically the sternal head, with the clavicular head possibly intact.
- Release adhesions and scar so the tendon reaches the insertion without excessive tension.
- Identify the lateral lip of the bicipital groove - the anatomic insertion, a 5-8cm footprint starting about 5cm distal to the greater tuberosity.
- Abduct and externally rotate the arm to visualise the footprint; create a 2-3cm wide contact area.
- Decorticate to bleeding bone with a rongeur, curette or rasp, but do NOT over-decorticate - preserve bone stock for anchor purchase.
- Excise residual tendon fibres to leave a clean bony surface; note the long head of biceps lies in the groove medially and the anterior humeral circumflex vessels run inferiorly.
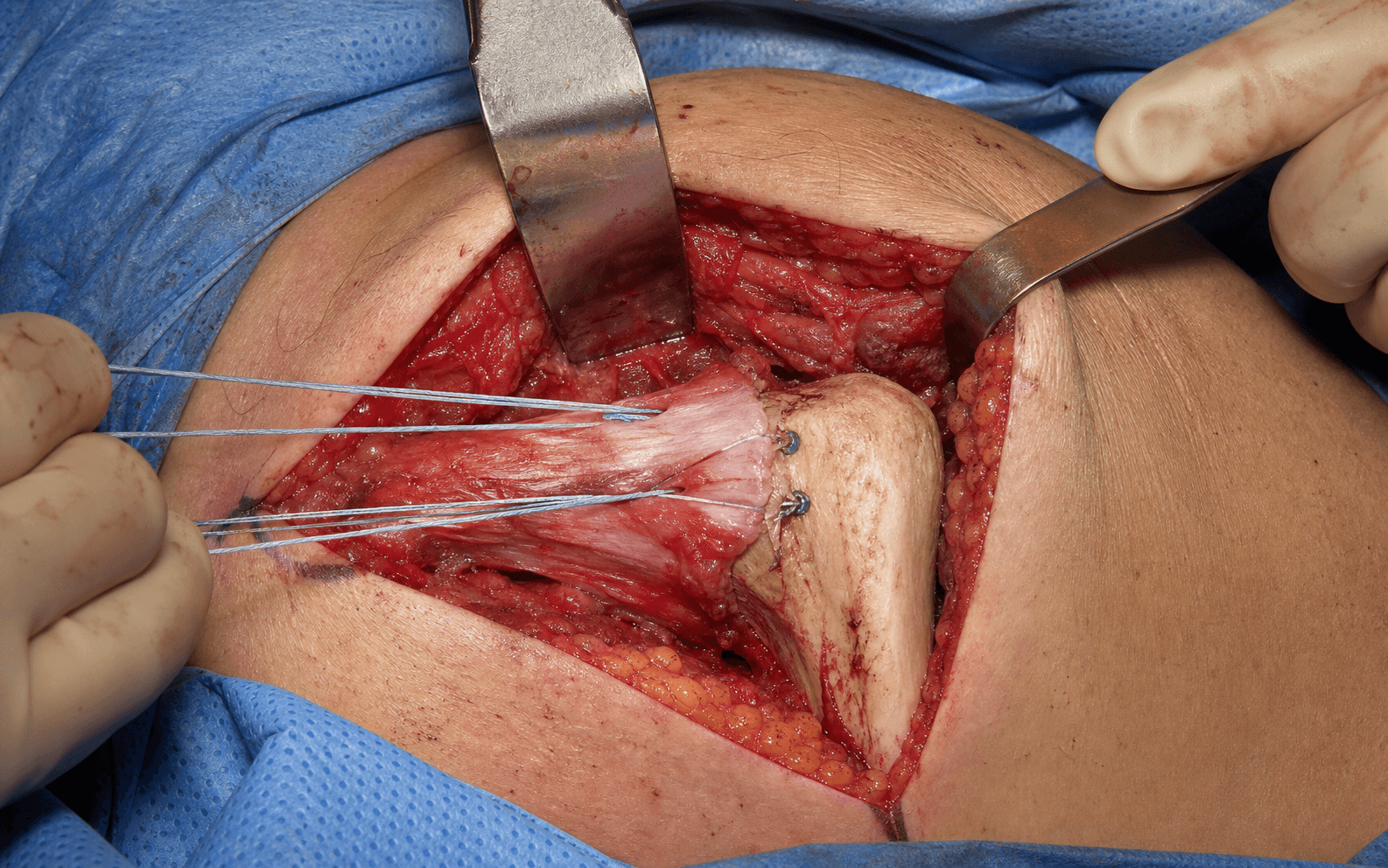
- Place 2-4 suture anchors (typically 3) along the lateral lip of the bicipital groove, 1-1.5cm apart, recreating the normal footprint.
- Insert at the 45-degree 'deadman' angle, directed distally to resist the proximal pull of the tendon.
- Use 5.0-5.5mm metal or PEEK anchors, double-loaded with number-2 high-strength suture; ensure each anchor is fully seated (not proud) and test its purchase before loading it.
- Mobilise the tendon so it reaches the insertion without excessive tension; gently stretch contracted muscle in chronic cases.
- Whipstitch the tendon end with number-2 high-strength suture using a Krackow (locking running) technique through robust tissue.
- In poor-quality (chronic, friable) tendon, incorporate more proximal muscle-tendon junction; confirm the tendon reaches the insertion with the arm in neutral without excessive tension - inadequate mobilisation is a leading cause of repair failure.
- Pass the anchor sutures through the tendon in a horizontal mattress configuration, about 1cm from the tendon edge.
- Space the mattress sutures along the tendon width for even load distribution; take good bites (at least 1cm of tendon substance).
- The mattress configuration is superior to simple sutures - it distributes force and resists cut-through; keep the multiple suture limbs organised with clamps.
- Position the arm in 30-45 degrees of abduction and neutral rotation (the functional length) and reduce the tendon to the bone footprint.
- Tie knots sequentially from the proximal to the distal anchor using a sliding-locking knot (e.g. SMC, surgeon's sixth) backed with half-hitches; aim for snug tendon-bone contact without strangulating the tissue.
- Verify the repair is flat against bone with even contact and no gaps, then test with gentle passive ROM - the repair should remain secure without gapping.
- Consider augmentation in chronic tears (greater than 6 weeks), poor tissue quality, revision surgery, or high-demand athletes.
- Graft augmentation: semitendinosus autograft, allograft or dermal graft woven through the tendon substance and secured to bone with additional anchors - it load-shares during healing.
- Internal brace: high-strength suture tape from tendon to bone parallel to the repair, acting as an internal splint.
- Augmentation may reduce re-rupture from 15-20 percent to less than 10 percent in high-risk cases; acute tears with good tissue do not routinely need it.
- Confirm the repair is secure without gapping through a gentle passive ROM, full passive elevation and rotation, adequate haemostasis, and no tethered or injured neurovascular structures.
- Copious irrigation; place a closed-suction drain if there is significant dead space (remove on day 1-2).
- Close the deltopectoral fascia if divided, subcutaneous tissue in layers with 2-0 Vicryl, and skin with staples or subcuticular 3-0 Monocryl.
- Apply a sterile dressing and a sling in neutral rotation; counsel the patient before they leave theatre: strict protection, NO active pectoralis contraction for 6 weeks minimum.
The musculocutaneous nerve pierces coracobrachialis 5-8cm (range 3-10cm) distal to the coracoid - it is the most commonly injured nerve; avoid inferior dissection beyond the conjoint tendon and use only gentle retraction of the conjoint. The lateral pectoral nerve enters the deep surface of pectoralis major 2-4cm from the clavicle with the thoracoacromial vessels - gentle superior retraction only. The medial pectoral nerve pierces pectoralis minor to reach the sternal head - stay superficial to pec minor during medial mobilisation of a chronically retracted tendon. The axillary nerve lies inferior to subscapularis in the quadrangular space, about 5-7cm below the acromion - stay superior to the surgical neck and place no retractors inferiorly. The anterior humeral circumflex vessels run along the surgical neck inferior to subscapularis - control if encountered during inferior decortication. If bleeding is met during chronic tendon mobilisation, suspect the anterior humeral circumflex or thoracoacromial branches: pressure for control, extend exposure, cauterise small vessels, and ligate larger ones.
Anchor the tendon at 45 degrees. The deadman angle - anchors inserted pointing distally at about 45 degrees to the cortex - lets the tendon pull along the line of the anchor rather than against it, resisting cut-out under the proximal pull of a contracting pectoralis. Space 3-4 double-loaded 5.5mm anchors 1-1.5cm apart along the lateral lip of the bicipital groove, fully seated, and test each for purchase before loading it.
In an acute tear the tendon retracts only 3-5cm with good tissue and minimal adhesions - retrieval is easy and 85-95 percent excellent results are achievable. In a chronic tear it retracts 5-10cm, scars down to the chest wall, atrophies, and the tissue is friable; expect only 70-80 percent good results and plan a larger exposure, aggressive mobilisation, and a low threshold for graft augmentation. Both are still markedly superior to non-operative care.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Activity | |-------|--------|----------------|----------| | 1 Protection | 0-6 weeks | Sling at all times (except hygiene/therapy) | CRITICAL: no active pectoralis contraction (no pushing, pressing, lifting, reaching). Passive ROM only - pendulums, passive elevation to 90 degrees, passive ER to neutral. Elbow/wrist/hand active ROM and grip | | 2 Early active motion | 6-12 weeks | Sling weaned | Active-assisted ROM (week 6-8), light active ROM (week 8-10). No resisted adduction or internal rotation until week 12 | | 3 Strengthening | 12-16 weeks | None | Progressive resistance - elastic bands and light dumbbells (2-5 lbs) up to about 50 percent of the contralateral side | | 4 Return to activity | 4-6 months | None | Sport-specific training and functional drills; bench press progressed to 50-60 percent of pre-injury max | | 5 Full activity | 6-12 months | None | Non-contact sport at 6 months; contact sport, heavy bench press and maximal loading at 9-12 months | Most patients return to desk work by about 6 weeks and heavy manual work by 4-6 months. Expect a 5-10 percent strength deficit versus the uninjured side even after a successful acute repair (acceptable); chronic repairs may carry a 20-30 percent deficit. Return to contact sport and heavy bench press is delayed to 9-12 months to minimise re-rupture risk. Complications
- Recognition
- Sudden pop or pain during rehabilitation, return of the anterior axillary fold defect, weakness with adduction/IR; MRI confirms a gap at the repair
- Prevention
- Strict 6-week protection; adequate mobilisation to avoid tension; secure anchor fixation; augmentation in high-risk cases
- Management
- Acute failure under 6 weeks: early revision with augmentation. Chronic failure: revise if symptomatic in a high-demand patient; counsel that revision gives 60-70 percent good results versus 85-95 percent primary
- Recognition
- Strength deficit greater than 20 percent versus contralateral; difficulty with push-up or bench press; MRI may show atrophy or a lengthened repair
- Prevention
- Acute rather than chronic repair; correct tensioning (avoid over- or under-tension); progressive strengthening from 12 weeks
- Management
- Reassure if less than 20 percent deficit and function preserved; progressive resistance to 3-6 months; consider revision if greater than 30 percent deficit in a young high-demand patient
- Recognition
- Restricted passive ROM (especially ER and abduction less than 90 degrees); pain at end-range; capsular pattern
- Prevention
- Early gentle passive ROM from week 1-2; avoid immobilisation beyond 6 weeks; progressive active-assisted ROM 6-12 weeks
- Management
- Aggressive therapy - passive stretching, joint mobilisation; NSAIDs; intra-articular steroid for adhesive capsulitis; MUA or arthroscopic capsular release if refractory at 6 months
- Recognition
- Musculocutaneous (most common): weak elbow flexion/supination, numb lateral forearm; lateral/medial pectoral: pectoralis atrophy; axillary: deltoid weakness and numbness
- Prevention
- Gentle conjoint retraction; avoid inferior dissection greater than 5-8cm from coracoid; gentle pectoralis retraction; stay superior to the surgical neck
- Management
- Most are neuropraxia - observe 3-6 months with expectation of recovery; serial EMG/NCS at 6 weeks, 3 and 6 months; document the pre- and post-op neuro exam
- Recognition
- Wound erythema, warmth, drainage, fever, raised WBC/CRP/ESR; early (less than 3 weeks) superficial versus deep; late: draining sinus, exposed anchor
- Prevention
- Preoperative antibiotics (Cefazolin 2g IV within 60 min), sterile technique, copious irrigation, haemostasis, early drain removal
- Management
- Superficial: oral antibiotics and wound care. Deep early: I&D, culture-specific IV antibiotics 6 weeks, retain anchors if well-fixed. Deep late: I&D, remove loose/infected anchors, staged reconstruction; Staph aureus most common - cover MRSA if risk factors
- Recognition
- Persistent asymmetry of the chest contour, loss of the anterior axillary fold, visible atrophy (chronic repairs)
- Prevention
- Early repair before atrophy; adequate mobilisation and secure fixation to restore anatomy; realistic preoperative counselling
- Management
- Reassure - some deformity is expected, especially chronic tears with atrophy; emphasise functional over cosmetic outcome; cosmetic revision is rarely indicated
- Recognition
- Pull-out: sudden loss of fixation and gapping; prominence: subcutaneous palpable bump, skin irritation; migration: change in position on radiograph
- Prevention
- Adequate bone stock (avoid over-decortication); full insertion depth; 45-degree deadman angle; high-quality 5.0-5.5mm anchors; test purchase before loading
- Management
- Pull-out acutely: immediate revision with new anchors in a different location, bone graft if stock poor, consider augmentation. Symptomatic prominence: excision with scar release and re-repair. Migration: remove if symptomatic and revise
Viva & Exam Focus
SLABSPECTORALIS - insertion anatomy
MLMAMLMA - nerves at risk during repair
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old powerlifter presents 3 days after an acute pectoralis major rupture during bench press. Walk me through your assessment and surgical decision-making.”
“During pectoralis major repair via the deltopectoral approach, you encounter significant bleeding from the inferomedial aspect of your dissection while mobilising a chronically retracted tendon. What has happened and how do you manage it?”
“Your patient had an excellent pectoralis major repair 4 weeks ago but now presents with a sudden pop and pain after pushing a heavy door. Examination shows return of the anterior axillary fold defect and MRI confirms re-rupture at the tendon-bone interface. How do you manage this?”
Indications
- Complete rupture (Grade III) in an active patient - absolute indication
- Acute rupture within 6 weeks (ideally within 2 weeks) - optimal timing, 85-95 percent excellent results
- Symptomatic partial tears (Grade II) with weakness - relative indication
- Chronic ruptures beyond 6 weeks still worthwhile if symptomatic (70-80 percent good results)
- High-demand athletes or manual labourers - strong indication regardless of timing
- Bone avulsion fractures - best prognosis for healing
- Contraindications: low-demand elderly, severe muscle belly tears, unacceptable medical risk
Key anatomy
- Two heads - clavicular (superior, smaller) and sternal (inferior, larger; tears most commonly)
- Insertion: lateral lip of the bicipital groove, 5-8cm footprint starting 5cm distal to the greater tuberosity
- Tendon twist: inferior sternal fibres insert superiorly (180-degree twist)
- Rupture location: 60 percent musculotendinous junction, 30 percent bone avulsion, 10 percent muscle belly
- Innervation: lateral pectoral nerve (C5-7) to clavicular, medial pectoral nerve (C8-T1) to sternal
- Blood supply: thoracoacromial (pectoral branch), lateral thoracic, internal mammary perforators
- Actions: adduction, internal rotation, horizontal flexion
Critical steps
- Deltopectoral approach: 8-12cm from 2cm below the clavicle toward the axilla, preserve the cephalic vein laterally
- Develop the internervous plane: deltoid (axillary) lateral, pectoralis (pectoral) medial
- Identify the ruptured tendon: acute 3-5cm retraction, chronic 5-10cm with scar and atrophy - mobilise extensively
- Prepare the insertion: decorticate the lateral lip of the bicipital groove to bleeding bone, preserve bone stock
- Place 3-4 suture anchors: 1-1.5cm apart along the footprint, 45-degree deadman angle, double-loaded 5.5mm
- Whipstitch the tendon: Krackow locking sutures; mobilise to reach the insertion without tension
- Mattress sutures: pass anchor sutures through the tendon 1cm from the edge in horizontal mattress
- Reduce and tie: arm 30-45 degrees abduction, neutral rotation, sequential knots, snug contact
- Augmentation: consider in chronic (greater than 6 weeks), poor tissue, high-demand - allograft or internal brace
- Final checks: secure repair, full passive ROM, haemostasis, sling, strict protocol counselling
Danger zones
- Musculocutaneous nerve: pierces coracobrachialis 5-8cm distal to the coracoid (PRIMARY RISK) - avoid inferior dissection, gentle conjoint retraction
- Lateral pectoral nerve: enters pec major 2-4cm from the clavicle with the thoracoacromial vessels - gentle superior retraction only
- Medial pectoral nerve: pierces pec minor to deep pec major medially - stay superficial during medial mobilisation
- Axillary nerve: quadrangular space, inferior to subscapularis 5-7cm below the acromion - stay superior to the surgical neck
- Anterior humeral circumflex vessels: surgical neck inferior to subscapularis - control if encountered
Technique pearls
- Deltopectoral approach is a true internervous plane (axillary versus pectoral nerves)
- Cephalic vein marks the interval - preserve and retract laterally preferred over ligation
- Acute versus chronic: acute has minimal retraction and good tissue; chronic has 5-10cm retraction, scar, atrophy, friable tissue
- Adequate mobilisation is critical - the tendon must reach the insertion with the arm neutral without tension
- The 45-degree deadman anchor angle resists the proximal pull of the tendon
- Mattress sutures 1cm from the edge are superior to simple sutures (resist cut-through, distribute load)
- Tensioning: 30-45 degrees abduction, neutral rotation; avoid over-tension (strangulation) or under-tension (gap)
- Augmentation reduces re-rupture in high-risk cases: chronic 15-20 percent to less than 10 percent
Complications
- Re-rupture 5-10 percent acute (20 percent if protocol violated), 15-20 percent chronic - leading cause is early active contraction
- Persistent weakness 10-15 percent acute, 20-30 percent chronic - expected, especially chronic repairs
- Stiffness 10-15 percent - early passive ROM critical; adhesive capsulitis may need MUA or capsular release
- Nerve injury 1-2 percent (musculocutaneous most common) - usually neuropraxia, observe 3-6 months
- Infection 1-2 percent - deep infection needs I&D, IV antibiotics 6 weeks, may need anchor removal
- Cosmetic deformity - persistent in chronic repairs despite functional improvement, counsel preoperatively
- Anchor complications - pull-out if over-tensioned or poor bone stock, prominence if not fully seated
Post-op protocol
- Phase 1 (0-6 weeks): STRICT PROTECTION - sling, NO active pectoralis contraction, passive ROM only (pendulums, elevation 90 degrees, ER neutral)
- Phase 2 (6-12 weeks): active-assisted ROM week 6, light active ROM week 8-10, NO resisted adduction until week 12
- Phase 3 (12-16 weeks): strengthening - elastic bands, light dumbbells, progressive resistance to 50 percent contralateral
- Phase 4 (4-6 months): sport-specific training, return to light sport or work
- Phase 5 (6-12 months): contact sport and heavy bench press at 9-12 months, gradual progression to maximal loads
- Protocol violations are the LEADING CAUSE of re-rupture - patient education is paramount
- Expect 5-10 percent strength deficit versus pre-injury (acceptable); chronic repairs may have 20-30 percent
Exam tips
- Classification: Grade I (strain, intact), Grade II (partial tear), Grade III (complete rupture) - surgery for symptomatic II and all III
- Timing matters: acute less than 6 weeks = 85-95 percent excellent, chronic greater than 6 weeks = 70-80 percent good
- Location is prognostic: bone avulsion best, musculotendinous 60 percent most common, muscle belly worst
- Mechanism: eccentric load to a maximally contracted muscle - bench press 80 percent, wrestling/tackling 15 percent, other 5 percent
- Examination: loss of the anterior axillary fold, palpable gap at insertion (acute), retracted mass medially (chronic)
- MRI is the gold standard: confirms rupture, shows location and retraction, quantifies atrophy (chronic)
- Augmentation indications: chronic greater than 6 weeks, poor tissue, revision, high-demand - reduces re-rupture 15-20 percent to less than 10 percent
- Post-op failures: mostly due to protocol violation - emphasise the 6-week strict protection
- Nerve at risk: musculocutaneous 5-8cm distal to the coracoid in the conjoint - the most common nerve injury
- Revision outcomes: 60-70 percent good results versus 85-95 percent primary - counsel realistic expectations
Background & Evidence
Epidemiology. Pectoralis major rupture is uncommon, representing roughly 1 percent of all shoulder soft-tissue injuries. It occurs overwhelmingly in men (greater than 95 percent), peaks in the 20-40 year age group, and is most frequent in weightlifters and contact athletes. The mechanism is an eccentric load to a maximally contracted muscle - bench press about 80 percent, wrestling and tackling 15 percent, other 5 percent. Use of anabolic steroids is a recognised risk factor. Pathoanatomy. The muscle has two heads - clavicular (superior, smaller) and sternal (inferior, larger). The tendon twists 180 degrees so that the inferior sternal fibres insert most superiorly and the superior clavicular fibres insert inferiorly; the sternal head ruptures most commonly. The footprint lies on the lateral lip of the bicipital groove, a 5-8cm array beginning about 5cm distal to the greater tuberosity. Sixty percent of tears are at the musculotendinous junction, 30 percent are bone avulsions (the best prognosis for healing), and 10 percent are intramuscular (the worst prognosis).
- Type / Grade
- I
- Description and significance
- Muscle contusion or strain; fibres intact; full strength - non-operative
- Type / Grade
- II
- Description and significance
- Partial tear; some function preserved; pain with activity - surgery if symptomatic
- Type / Grade
- III
- Description and significance
- Complete rupture; no function; visible deformity - surgical
- Type / Grade
- Bone avulsion (30 percent)
- Description and significance
- From the lateral lip of the bicipital groove - best prognosis for healing
- Type / Grade
- Musculotendinous junction (60 percent)
- Description and significance
- The most common location
- Type / Grade
- Muscle belly (10 percent)
- Description and significance
- Worst prognosis; poor tissue for repair
- Type / Grade
- Three-axis
- Description and significance
- Timing (acute less than 6 weeks versus chronic), location, and extent (partial versus complete) - the contemporary standard
Key evidence. The consistent message is that surgical repair is superior to non-operative treatment and that earlier repair is better. Schepsis (2000) reported subjective ratings of 96 percent (acute repair), 93 percent (chronic repair) and only 51 percent (non-operative), with isokinetic adduction strength of 102 percent, 94 percent and 71 percent respectively, with no significant difference between acute and chronic operative repair. de Castro Pochini (2010), in a prospective study of 20 athletes, found an isokinetic strength deficit of 13.7 percent after surgery versus 53.8 percent non-operative. Bak (2000), in a meta-analysis of 112 cases, showed repair within the first 8 weeks gave significantly better outcomes, independent of age or rupture location. ElMaraghy and Devereaux (2012) proposed the three-axis classification now in standard use. Butt (2015) confirmed MRI as the investigation of choice and that graft reconstruction has a role when direct repair is not achievable in the chronic setting.
References
Outcome after repair of acute and chronic pectoralis major ruptures
- 17 distal pectoralis major ruptures: 13 operative (6 acute, 7 chronic) and 4 nonoperative
- Subjective outcome ratings: 96 percent acute repair, 93 percent chronic repair, only 51 percent nonoperative
- Isokinetic adduction strength: 102 percent of opposite side (acute), 94 percent (chronic), 71 percent (nonoperative)
- No significant difference between acute and chronic operative repair; both significantly better than nonoperative
Pectoralis major muscle rupture in athletes: a prospective study
- Prospective cohort of 20 male athletes: 10 surgical versus 10 nonoperative, mean follow-up 36 months
- Surgical group: 70 percent excellent, 20 percent good, 10 percent poor outcomes
- Isokinetic strength deficit at 60 deg/s: 13.7 percent surgical versus 53.8 percent nonoperative
- Total rupture in athletes had significantly better functional results after surgery
Rupture of the pectoralis major: a meta-analysis of 112 cases
- Pooled analysis of 112 cases (108 from literature plus 4 new); all patients male
- Most ruptures complete and located at the humeral insertion; work-related injuries more often at the musculotendinous junction
- Surgical treatment, preferably within the first 8 weeks, gave significantly better outcomes than conservative or delayed repair
- Prognosis was related neither to patient age nor to rupture location
A systematic review and comprehensive classification of pectoralis major tears
- Systematic review of 365 reported cases; 75 percent occurred in the preceding 20 years
- 83 percent resulted from indirect trauma, with 48 percent occurring during weight-training activities
- Proposes a three-axis classification: timing (acute versus chronic), location (origin or belly, musculotendinous junction to insertion, or bony avulsion), and extent (thickness; complete versus incomplete width)
- Standardised terminology enables meaningful comparison of techniques and outcomes
Pectoralis major ruptures: a review of current management
- MRI with dedicated sequencing is the investigation of choice for diagnosis, surgical planning and prognosis
- Early surgery is preferable, but good outcomes are achievable in the chronic setting
- Direct repair to bone via transosseous or anchor techniques is feasible in acute and most chronic cases
- When direct repair is not achievable in chronic cases, autograft or allograft reconstruction should be considered
Rupture of the pectoralis major muscle
- Surgical repair gave significantly better strength (Cybex testing) and patient satisfaction than conservative treatment
- 91 percent of patients were satisfied with surgery versus 27 percent with nonoperative care
Ruptures of the pectoralis major muscle: an anatomic and clinical analysis
- Classic anatomic study describing the pectoralis insertion and the tendon twist (inferior sternal fibres insert superiorly)
- Established the surgical technique for repair with suture anchors
Pectoralis major tears: comparison of surgical and conservative treatment
- Systematic review of pectoralis major ruptures
- Surgical repair gave 78 percent excellent outcomes versus 27 percent with conservative treatment
- Surgery recommended for complete ruptures in active patients
Epidemiology of shoulder dislocations presenting to emergency departments in the United States
- Epidemiologic data on shoulder injuries
- Pectoralis major ruptures represent about 1 percent of shoulder soft-tissue injuries
- Predominantly in men (greater than 95 percent), peak age 20-40 years, most common in weightlifters and contact athletes
Injuries to the pectoralis major muscle: diagnosis and management
- Comprehensive review of indications, techniques and outcomes
- Discusses augmentation with allograft or internal brace for chronic tears and high-demand athletes
- Reports re-rupture rates of 5-10 percent (acute) and 15-20 percent (chronic), reduced to less than 10 percent with augmentation