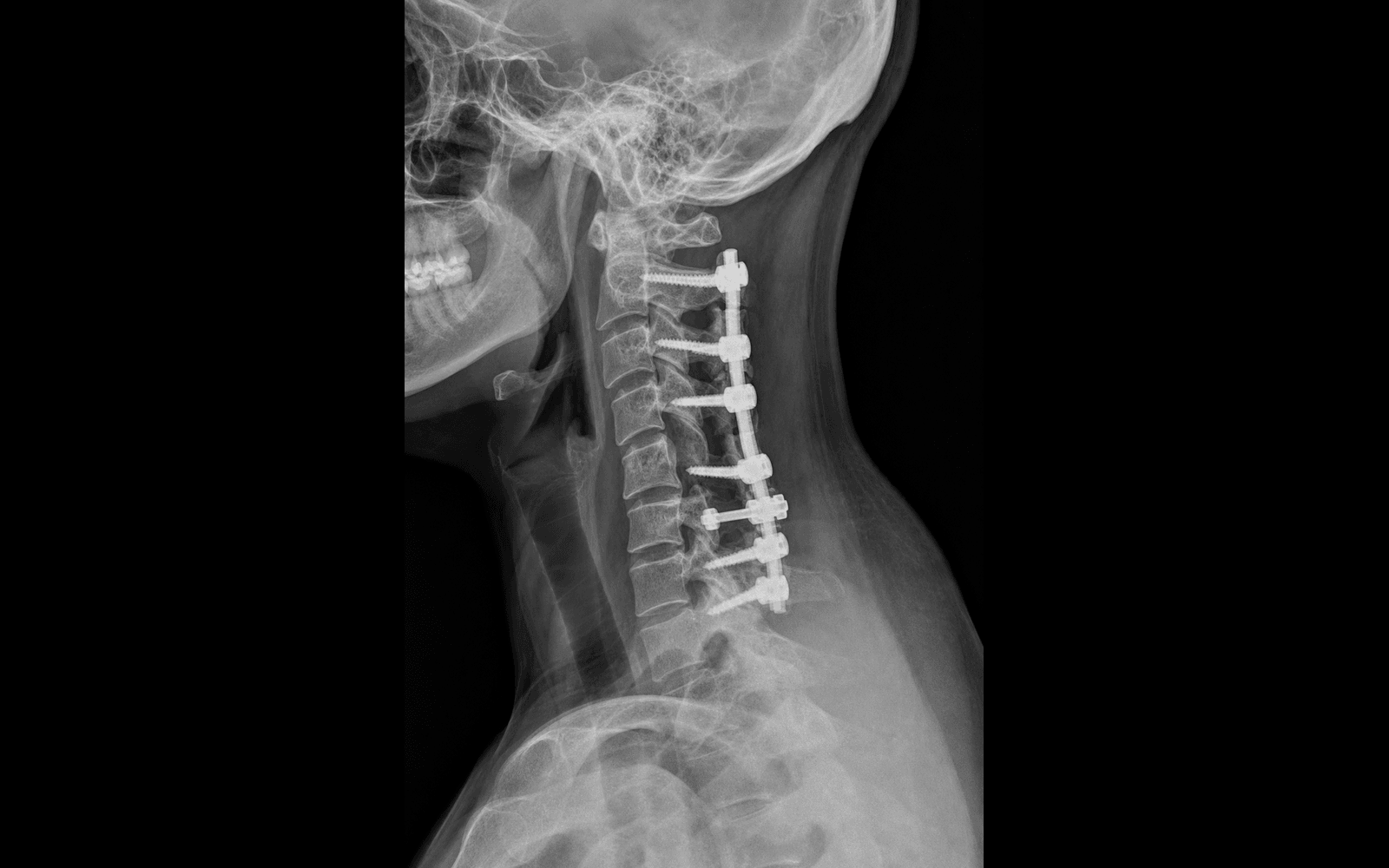
Posterior midline approach for multilevel cervical myelopathy, decompressed by laminectomy and stabilised with lateral mass screw-rod fusion · advanced
- Multilevel cervical myelopathy (more than 3 levels) is the primary indication, provided cervical lordosis is preserved — a kyphotic alignment requires an anterior or combined approach.
- Fusion is MANDATORY after laminectomy: it removes the posterior tension band, so without fusion post-laminectomy kyphosis runs at 10-20 percent in adults versus less than 2 percent with instrumented fusion.
- Insert the lateral mass screws BEFORE the laminectomy, through the centre of the lateral mass using the Magerl (25 degrees lateral, 45 degrees cephalad) or Anderson (10 degrees lateral, 30 degrees cephalad) trajectory.
- In OPLL, leave the ossified dura intact — attempting removal risks a catastrophic CSF fistula (around 50 percent leak rate if the ossified dura is violated).
- The C5 palsy (5-10 percent) is delayed 24-48 hours, driven by posterior cord drift tethering the shortest, most horizontal root — manage expectantly; 80-90 percent recover over 3-12 months.
- “Cervical nerve roots exit ABOVE their pedicle (C5 exits at C4-5), the opposite of the lumbar spine.
- “The vertebral artery lies only 1.5-2mm lateral to the lateral mass edge, in the foramen transversarium.
- “A medial screw breach greater than 4mm threatens the nerve root and demands revision.
- “Reverse Trendelenburg of 15-20 degrees reduces epidural venous bleeding by 40-50 percent.
When & Why
The operation. Posterior cervical laminectomy and fusion decomposes the cervical spinal cord posteriorly across multiple stenotic levels and immediately stabilises the decompressed segments with lateral mass screws, rods and a posterolateral fusion mass. It is the workhorse posterior operation for multilevel cervical myelopathy. Primary indication. Multilevel cervical myelopathy (three or more levels) with progressive neurological deficit, where the stenosis spans too many levels for a practical anterior construct and cervical lordosis is preserved (a C2-C7 Cobb angle of 20-40 degrees). Lordosis is essential — it lets the spinal cord drift posteriorly, away from anterior pathology, after the laminae are removed. Absolute indications:
- Multilevel cervical myelopathy (three or more levels) with a progressive neurological deficit
- Cervical stenosis with preserved cervical lordosis (20-40 degree C2-C7 Cobb angle)
- OPLL (ossification of the posterior longitudinal ligament) causing cord compression
- Congenital cervical stenosis (canal diameter less than 13mm) with symptomatic myelopathy Relative indications:
- Multilevel stenosis that has failed conservative management (more than 3-6 months)
- Multilevel spondylotic myelopathy with posterior-predominant compression
- Multilevel cervical radiculopathy not amenable to an anterior approach
- Combined central and foraminal stenosis across multiple levels Absolute contraindications:
- Cervical kyphosis — the cord cannot drift back off a kyphotic vertebral body column, so anterior column support is needed first (or a combined approach)
- Primarily anterior pathology (large disc herniation, anterior osteophytes) — ACDF is better
- Active cervical spine infection (pyogenic discitis, osteomyelitis)
- Medical instability precluding prolonged anaesthesia Relative contraindications:
- Severe osteoporosis (T-score less than -3.0) — screw purchase is compromised
- Previous posterior cervical surgery with heavy scarring
- Obesity with poor posterior neck anatomy exposure
- Single or two-level disease — ACDF is preferred for limited disease
- Loss of cervical lordosis below 10 degrees — consider a combined approach Clinical assessment — confirm myelopathy before operating. Myelopathy signs (upper motor neuron): Hoffman's sign (flick the distal phalanx of the middle finger to elicit thumb flexion), the inverted radial reflex (brachioradialis tap produces finger flexion — a C5-6 lesion), hyperreflexia in the lower extremities with clonus, Lhermitte's sign (neck flexion sends an electric shock down the spine), and a spastic, broad-based, circumducting gait. Radiculopathy signs (lower motor neuron): C5 — deltoid/biceps weakness, reduced biceps reflex; C6 — wrist extension weakness, reduced brachioradialis reflex; C7 — triceps weakness, reduced triceps reflex; C8 — finger flexion weakness, reduced grip. Modified JOA score (17 points): motor function upper extremity (0-5), motor function lower extremity (0-7), sensory upper extremity (0-2), sensory trunk and lower extremity (0-2), bladder function (0-1). A score below 12 indicates moderate-to-severe myelopathy warranting surgery. Why posterior, not anterior. For multilevel disease with preserved lordosis and posterior-predominant compression, a single posterior approach decompresses everything in one field while preserving motion at C2-3 and C6-7. The AOSpine North America CSM study (Fehlings) showed anterior and posterior approaches are equivalent once patient and disease factors are controlled — so the choice rests on alignment, number of levels and where the compression sits, not on presumed superiority. Consent. Discuss a C5 palsy (5-10 percent, usually recovering 80-90 percent by a year), dural tear (5-8 percent), spinal cord injury (0.2-0.4 percent, devastating), vertebral artery injury (less than 0.5 percent, stroke risk), wound infection (1-3 percent) and an epidural haematoma (1-2 percent, a surgical emergency). Mean blood loss is 300-500mL.
The Operation
The goal is to expose the posterior cervical spine through a single midline incision, confirm the levels, insert lateral mass screws for immediate stability, remove the laminae and ligamentum flavum to decompress the cord, restore the facet-bound foraminal width, contour rods to preserve lordosis, lay down a posterolateral fusion mass, achieve meticulous haemostasis and close in layers over a drain. The exposure is the foundation — it is laid out step by step in the timeline below.
Key operative anatomy. The lateral mass is the bony block between the superior and inferior articular processes, unique to C3-C7 — roughly 10-15mm high, 8-12mm wide and 6-10mm deep (C3 is smallest and may need a 3.0mm screw; C7 is largest but carries an anterior vertebral artery course). Three structures surround it and dictate screw trajectory: the nerve root lies medial, the vertebral artery lies just 1.5-2mm lateral to the lateral mass edge in the foramen transversarium, and the carotid sheath and oesophagus lie anterior. Cervical roots exit ABOVE their pedicle (C5 exits at C4-5, the opposite of the lumbar spine), and the C5 root is shortest (25-30mm), most horizontal and least mobile — which is why it is the root most often palsied. The ligamentum flavum is normally 3-5mm of thick yellow elastic tissue (hypertrophying to 7-10mm in stenosis), with the dura immediately anterior to it (0-2mm gap).
- Entry point
- Centre of lateral mass
- Lateral angle
- 25 degrees (range 15-30)
- Cephalad angle
- 45 degrees (range 30-50)
- Safe zone
- Larger safe zone; higher pullout strength
- Trade-off
- Higher medial breach risk if angles are too steep
- Entry point
- Centre of lateral mass
- Lateral angle
- 10 degrees (range 0-15)
- Cephalad angle
- 30 degrees (range 20-40)
- Safe zone
- Smaller zone; more parallel to facet
- Trade-off
- Safer for the nerve root; slightly less purchase
Operative sequence
- Prone in a Mayfield 3-pin head holder (pins four finger-breadths above the ears, 1cm above the supraorbital ridge to spare the supraorbital nerve), neck in neutral — avoid flexion (cord compression) or extension (narrows the canal).
- Reverse Trendelenburg 15-20 degrees to drop epidural venous pressure and bleeding by 40-50 percent; shoulder tape traction caudally exposes C7-T1.
- Confirm neutral alignment on lateral fluoroscopy; mark the midline over the palpable spinous processes.
Excessive flexion can compress the cord intraoperatively. Count levels carefully from C2 (the first palpable bifid spinous process below the occiput) — wrong-level surgery is a never event, and palpation alone is wrong about 40 percent of the time in obese patients, so confirm with fluoroscopy.
- Midline incision through skin and subcutaneous tissue to the nuchal ligament — the avascular midline raphe between the trapezius muscles.
- Subperiosteal dissection with a Cobb elevator, staying on bone: detach semispinalis cervicis and multifidus from the spinous processes and laminae.
- Expose the lateral masses bilaterally out to the lateral edge of the facet joint — going further lateral risks the vertebral artery (1.5-2mm beyond the lateral mass edge).
- Preserve the C2 nerve root (greater occipital nerve) if exposing C1-2; self-retaining retractors maintain the field.
Subperiosteal dissection preserves segmental muscle innervation and reduces bleeding. The lateral dissection limit is the LATERAL EDGE OF THE FACET JOINTS — beyond it lies the vertebral artery. Violating the C2 nerve (greater occipital nerve) causes occipital neuralgia in 15-20 percent.
- Place a radiopaque marker (spinal needle or instrument) on a spinous process and confirm the level on lateral C-arm fluoroscopy.
- Remember cervical roots exit ABOVE their vertebra (C5 exits at C4-5); C8 exits at C7-T1 (eight roots, seven vertebrae).
- Identify C2 (bifid) and C7 (longest, non-bifid) and count carefully from C2; mark the planned laminectomy levels with electrocautery on the laminae.
- Wrong-level laminectomy — a medicolegal catastrophe; confirm every level with fluoroscopy before decompression.
- Misidentification of C2 versus occiput or C1.
- Radiation exposure to surgeon and staff (lead, distance).
- Insert the lateral mass screws BEFORE laminectomy, while the posterior elements are intact, for maximum stability. Entry point: the centre of the lateral mass between the superior and inferior articular processes.
- Use the Magerl trajectory (25 degrees lateral, 45 degrees cephalad toward the opposite eye socket) or the Anderson trajectory (10 degrees lateral, 30-40 degrees cephalad, parallel to the facet).
- Drill to 12-14mm; palpate all four walls with a ball-tip probe checking for breach; typical screw is 3.5mm diameter (3.0mm if the lateral mass is small). Bicortical purchase is not required. Start at the lowest level and work cephalad.
Magerl 25/45 has a larger safe zone but a medial breach greater than 4mm injures the nerve root. A lateral breach injures the vertebral artery (only 1.5-2mm from the lateral mass edge). Palpate all four walls before placing the screw.
- Start at the most stenotic level. Use a high-speed burr with a footplate attachment to thin the lamina from midline laterally to eggshell thickness, staying in the epidural space.
- Identify the ligamentum flavum — thick yellow elastic tissue, hypertrophied to 7-10mm in stenosis — with the dura immediately anterior (0-2mm gap).
- Complete the laminectomy with Kerrison rongeurs, removing lamina, spinous process and ligamentum flavum, working cephalad to caudad.
Thin the lamina with the burr to eggshell BEFORE using the rongeur, to avoid a dural tear. If OPLL is present, leave the ossified dura intact — attempting removal risks a catastrophic CSF fistula (around 50 percent leak rate if the ossified dura is violated); decompress around it (floating technique).
- Dural tear (5-8 percent; higher in revision or OPLL).
- Spinal cord injury from an instrument penetrating anteriorly.
- Epidural venous plexus bleeding (Batson's valveless plexus, engorged if positioning is inadequate).
- Inadequate lateral decompression leaving residual foraminal stenosis.
- Undercut the medial aspect of the facet joints bilaterally with Kerrison rongeurs — remove the medial 25-50 percent of the facet to open the foramen.
- Nerve roots exit ABOVE the pedicle at each level (C5 exits above the C5 pedicle in the C4-5 foramen).
- Confirm adequate decompression by passing a micro nerve hook into the foramen — it should slide freely without resistance.
Cervical foraminal stenosis is often driven anteriorly by uncovertebral joint (Luschka) osteophytes — if the compression is predominantly anterior, ACDF may be needed. Stay on bone laterally (the vertebral artery is 1.5-2mm away) and never resect more than 50 percent of the facet, or iatrogenic instability results.
- Contour the rods to match the patient's cervical lordosis (normal 20-40 degree C2-C7 Cobb angle). The goal is to maintain or restore lordosis — kyphotic alignment gives poor outcomes and swan-neck deformity.
- Connect the rods to the lateral mass screws bilaterally, seat them fully in the screw heads, then compress across levels to load the bone graft.
- Avoid excessive compression, which can cause foraminal stenosis.
Post-laminectomy kyphosis occurs in 10-20 percent without fusion. The rod (typically 3.5mm titanium) must hold 20-40 degrees of lordosis; compression across the levels loads the graft and closes the laminectomy defect.
- Decorticate the lateral masses bilaterally with a burr or osteotome to expose bleeding cancellous bone — remove the outer cortex only, preserving the medial wall adjacent to the canal.
- Pack morselised graft (local autograft from the removed lamina and spinous processes, plus allograft or demineralised bone matrix) over the lateral masses and between the screws.
- Aim for a continuous posterolateral fusion mass connecting the instrumented levels. BMP (rhBMP-2) is off-label posteriorly and is generally avoided here because of dysphagia, airway swelling, seroma and ectopic bone risk.
Fusion is required after laminectomy to prevent progressive kyphosis (up to 21 percent without fusion versus 0-2 percent with). Local autograft is excellent but limited in volume (30-50cc); supplement with allograft. Smoking drops fusion rates from 90 to 60 percent.
- Perform final tightening of all set screws and locking caps sequentially to avoid construct strain; torque to manufacturer specification (typically 80-100 in-lb for 3.5mm systems).
- Obtain intraoperative lateral and AP fluoroscopy to confirm screw position, rod alignment, maintained lordosis and no hardware prominence.
- Address malpositioned screws immediately — a medial breach greater than 4mm requires revision.
Inadequate final tightening is a common cause of hardware failure. A post-op CT is often performed to verify screw position. The C5 palsy can manifest late (24-48h) — monitor motor function hourly for 24 hours.
- Achieve haemostasis with bipolar electrocautery on the epidural venous plexus, muscle edges and bone surfaces; thrombin-soaked gelfoam over exposed dura; bone wax sparingly on bleeding bone edges (it inhibits fusion).
- Consider tranexamic acid (1g load plus 1g over 8h) to reduce blood loss by 30-40 percent; irrigate copiously with antibiotic solution (1g vancomycin in 1L saline).
A cervical epidural haematoma compressing the cord is a surgical emergency (1-2 percent incidence). Risk factors: multilevel surgery, bleeding disorders, venous engorgement, inadequate haemostasis. Any post-op neurological deterioration needs urgent MRI and emergent decompression within 6 hours to avoid permanent deficit.
- Place a 10Fr round drain in the epidural space if dissection was extensive or oozing (more than 5 levels, revision, BMP use); bring it out through a separate lateral stab incision.
- Close in layers: muscle and nuchal ligament with 0 Vicryl (restore the posterior tension band), deep dermis with 2-0 Vicryl, subcuticular 3-0 Monocryl, then skin glue or steri-strips.
- Keep the drain 24-48h or until output is below 50mL/24h. A rigid collar is optional — many surgeons omit it with an instrumented, immediately stable construct.
A drain reduces haematoma risk but slightly raises infection risk — use it selectively for multilevel cases (more than 4 levels), revision or BMP cases. Early mobilisation on day 1 reduces complications; cervical fusion takes 3-6 months (faster than lumbar).
- Neurological checks hourly for the first 24 hours, focusing on motor and sensory function in all four limbs.
- Watch for the C5 palsy — the most common nerve root injury after cervical decompression (5-10 percent): deltoid/biceps weakness, with or without pain, typically delayed 24-48h. Mechanism: posterior cord drift after decompression tethers the shortest, most horizontal root.
- Manage expectantly — most recover 80-90 percent by a year. Obtain day-1 AP and lateral cervical radiographs to confirm alignment and hardware; mobilise early unless the palsy is severe.
Aftercare & Complications
Immediate post-operative (0-24h). Hourly neurological checks (motor and sensory, all extremities). Watch for the C5 palsy (delayed deltoid/biceps weakness at 24-48h) and an epidural haematoma (acute neurological deterioration = emergency MRI). Elevate the head of the bed 30-45 degrees to reduce swelling; monitor drain output (remove below 50mL/24h, typically 24-48h). Multimodal analgesia: paracetamol, NSAIDs, opioids as needed. Early mobilisation (1-7 days). Mobilise on day 1 with physiotherapy — no collar is needed with an instrumented fusion. Log-roll for comfort in the first 48h. Deep breathing and incentive spirometry prevent atelectasis. VTE prophylaxis: sequential compression devices, early mobilisation, and chemical prophylaxis (enoxaparin 40mg daily) if bleeding risk is low. Day-1 AP and lateral radiographs confirm alignment and hardware. Discharge and rehabilitation (2-5 days typical). Discharge when the patient mobilises independently, pain is controlled on oral medication, there is no neurological deterioration, the drain is out and the wound is dry. BLT precautions (bending, lifting more than 5kg, twisting) for 6 weeks. Keep the wound dry for 10 days; remove sutures/staples at 10-14 days. Red flags: fever above 38.5 degrees Celsius, wound drainage, neurological change, severe pain. Follow-up at 2 weeks (wound check), 6 weeks, 3 months, 6 months and 1 year. Rehabilitation protocol:
- Weeks 0-6: BLT precautions; gentle active range-of-motion exercises, no resistance
- Weeks 6-12: progressive strengthening, isometric cervical exercises
- Month 3 onward: full activity as tolerated if fusion is progressing on imaging
- Return to work: sedentary at 4-6 weeks, manual labour at 3-6 months (after fusion is confirmed)
- Driving: when comfortable turning the head, off opioids — typically 2-4 weeks Imaging follow-up and fusion assessment:
- Day 1: AP and lateral radiographs (baseline alignment, hardware)
- 6 weeks: cervical radiographs (alignment, hardware, early fusion)
- 3 months: CT cervical spine (bridging bone across the fusion mass)
- 6 months: flexion-extension radiographs (dynamic stability)
- Radiographic fusion = bridging bone across the levels on CT; dynamic fusion = less than 2mm translation or less than 5 degrees angulation on flexion-extension. Time to fusion is 3-6 months in the cervical spine (faster than lumbar); pseudarthrosis is defined as no bridging bone at 12 months on CT.
- Recognition
- Delayed deltoid/biceps weakness 24-48h, with or without radicular pain; EMG at 3 weeks shows denervation if axonal; MRI shows root oedema, no compression
- Prevention
- Avoid excessive posterior cord shift, limit decompression to symptomatic levels, consider prophylactic C4-5 foraminotomy, avoid over-correction into hyperlordosis
- Management
- Expectant — 80-90% recover over 3-12 months; physical therapy, pain management; surgery NOT indicated (no compression); EMG at 3 weeks, repeat at 3 months
- Recognition
- Intraop clear fluid/pulsatile flow; post-op clear drainage, positional headache; beta-2 transferrin positive
- Prevention
- Thin lamina with burr before rongeur, identify the yellow ligamentum flavum, leave ossified dura intact in OPLL, gentle technique in revision
- Management
- Primary repair with 4-0 Nurolon, watertight closure, fibrin glue, muscle/fat patch; post-op leak — bed rest and lumbar drain 5-7 days; persistent leak — surgical repair
- Recognition
- Acute neurological decline in the first 24h, severe neck pain; urgent MRI shows epidural collection compressing the cord
- Prevention
- Meticulous haemostasis, reverse Trendelenburg positioning, TXA, drain for multilevel cases, correct coagulopathy
- Management
- SURGICAL EMERGENCY — emergent decompression within 6h; delay risks permanent deficit; ICU monitoring post-revision
- Recognition
- Intraop brisk arterial bleeding from lateral dissection or screw breach; post-op vertebrobasilar stroke (ataxia, diplopia, dysarthria)
- Prevention
- Limit lateral dissection to the facet edge, Magerl trajectory 25 degrees lateral (not more than 30), palpate four walls, CT angiography if anomalous VA
- Management
- Bone wax and gelfoam packing, muscle/fascia patch; avoid ligation (stroke risk); endovascular coiling if persistent; post-op stroke — neurology, antiplatelet, rehab
- Recognition
- Progressive neck pain, swan-neck deformity, neurological decline; serial lateral radiographs show loss of lordosis (Cobb below 10 degrees)
- Prevention
- Instrumented fusion mandatory (reduces to less than 2%), maintain 20-40 degrees lordosis intraop, preserve more than 50% of the facet joints
- Management
- Progressive kyphosis over 20 degrees — revision with anterior column support (corpectomy and strut graft) plus posterior instrumented fusion
- Recognition
- Loss of resistance drilling, four-wall palpation breach, new radiculopathy; post-op CT shows medial/lateral/anterior breach
- Prevention
- Anatomic entry point, correct trajectory (Magerl 25/45 or Anderson 10/30), four-wall palpation, intraop imaging
- Management
- Medial breach over 4mm — revise (nerve root risk); lateral breach — remove, bone wax, place new screw medially; anterior breach — assess vascular injury; minor breach under 2mm — observe
- Recognition
- Persistent pain, hardware failure, motion over 2mm or 5 degrees on flexion-extension; CT shows no bridging bone at 6-12 months
- Prevention
- Adequate decortication, local autograft plus allograft, smoking cessation (fusion 60% smokers vs 90% non-smokers), optimise nutrition
- Management
- Symptomatic — revision fusion with better biology (BMP, autograft), extend instrumentation, anterior column support if kyphosis; asymptomatic — observe with serial imaging
Complication rates at a glance. Neurological: C5 palsy 5-10 percent (usually recovers 80-90 percent); spinal cord injury 0.2-0.4 percent (devastating, permanent); nerve root injury 2-5 percent (from screw malposition). Haemorrhagic: epidural haematoma 1-2 percent (surgical emergency); vertebral artery injury less than 0.5 percent (stroke risk); mean blood loss 300-500mL. Mechanical: screw malposition 2-5 percent; post-laminectomy kyphosis 10-20 percent without fusion, less than 2 percent with fusion; pseudarthrosis 5-10 percent (higher in smokers); hardware failure 1-3 percent. Infectious: wound infection 1-3 percent; discitis/osteomyelitis less than 1 percent (delayed, weeks post-op); meningitis less than 0.5 percent (if dural tear). Other: dural tear 5-8 percent (higher in revision and OPLL); dysphagia rare with a posterior approach (less than 1 percent); adjacent segment disease 2-3 percent per year; axial neck pain 15-20 percent (myofascial).
Viva & Exam Focus
LORDOSISLORDOSIS — the operation at a glance
SCREW-INSCREW-IN — lateral mass screw safety
Location: immediately anterior to the lamina (0-2mm gap); cervical cord diameter about 10mm. Protection: thin the lamina with the burr before using a Kerrison, use footplate attachments, stay in the epidural space, avoid direct anterior pressure.
Location: runs in the foramen transversarium, 1.5-2mm lateral to the lateral mass edge, anterior to the C7 transverse process. Protection: stay medial during lateral mass exposure, keep the Magerl lateral angle at 25 degrees (not more than 30), palpate all four walls before screw insertion, do not dissect lateral to the facet edge.
Location: exits above the C5 pedicle (C4-5 foramen); the shortest and most horizontal cervical root, 3-5mm from the medial pedicle wall. Protection: Magerl 45 degrees cephalad (not more than 50), revise a medial breach over 4mm, keep foraminal decompression under 50 percent of the facet, gentle nerve hook palpation.
Location: valveless Batson's plexus directly anterior to the lamina (2-5mm from the dura), engorging with raised abdominal pressure. Protection: reverse Trendelenburg 15-20 degrees, thrombin-soaked gelfoam, bipolar (not monopolar) cautery, TXA, meticulous haemostasis before closure.
Location: 0-2mm anterior to the ligamentum flavum (3-5mm thick, yellow), adherent in OPLL. Protection: thin the lamina to eggshell before rongeur removal, identify the yellow ligamentum flavum, leave the ossified dura intact in OPLL, repair tears primarily with 4-0 Nurolon.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old man presents with progressive hand clumsiness, gait instability and bladder urgency. MRI shows multilevel cervical stenosis C3-C6 with cord signal change. Describe your surgical approach and technique in detail.”
“Describe the anatomy relevant to lateral mass screw insertion. What are the key differences between the Magerl and Anderson techniques?”
“A patient develops progressive deltoid weakness 24 hours after posterior cervical laminectomy C3-C6. What is your differential diagnosis and management?”
Indications
- Multilevel cervical myelopathy (3 or more levels) — progressive hand clumsiness, gait instability, hyperreflexia, positive Hoffman's sign
- Cervical stenosis with PRESERVED lordosis (20-40 degree C2-C7 Cobb) — kyphosis needs anterior column support
- OPLL — leave the ossified dura intact (around 50 percent CSF leak rate if violated)
- Congenital cervical stenosis (canal less than 13mm) with symptomatic myelopathy
Key anatomy
- Lateral mass: 10-15mm high, 8-12mm wide; C3 smallest (may need a 3.0mm screw), C7 largest
- Cervical roots exit ABOVE the pedicle: C5 exits at C4-5 (opposite lumbar); C8 exits at C7-T1 (8 roots, 7 vertebrae)
- C5 root: shortest (25-30mm), most horizontal, least mobile — highest palsy risk (5-10 percent)
- Vertebral artery: 1.5-2mm lateral to the lateral mass edge in the foramen transversarium C2-C6, enters at C6 in 90 percent
- Ligamentum flavum: 3-5mm normally (hypertrophies to 7-10mm in stenosis); dura 0-2mm anterior
Critical steps
- Positioning: prone Mayfield, NEUTRAL neck, reverse Trendelenburg 15 degrees (cuts venous bleeding 40-50 percent)
- Level confirmation: fluoroscopy with a marker BEFORE decompression; C2 bifid, C7 longest non-bifid, count from C2
- Lateral mass screws BEFORE laminectomy: Magerl 25/45 or Anderson 10/30, 12-14mm depth, palpate four walls
- Laminectomy: burr to eggshell, identify the yellow ligamentum flavum, Kerrison removal, undercut facets 25-50 percent
- Fusion: contour rods to 20-40 degrees lordosis, decorticate lateral masses, autograft plus allograft, meticulous haemostasis
Danger zones
- Spinal cord: 0-2mm anterior to the lamina, 10mm diameter — use a footplate burr, stay epidural
- Vertebral artery: 1.5-2mm lateral to the lateral mass, injury less than 0.5 percent but catastrophic — keep the lateral angle at 25 degrees Magerl
- C5 nerve root: 3-5mm from the medial pedicle wall — a medial breach over 4mm requires revision
- Epidural venous plexus: Batson's plexus 2-5mm from the dura — reverse Trendelenburg and bipolar cautery
- Dura: 0-2mm anterior to the ligamentum flavum, adherent in OPLL — leave the ossified dura intact
Technique pearls
- Screws: centre of the lateral mass entry, Magerl 25/45 (larger safe zone) or Anderson 10/30 (safer nerve), unicortical
- Decompression: thin the lamina with the burr to eggshell FIRST, then Kerrison — prevents dural tear
- OPLL: leave the ossified dura intact (around 50 percent CSF leak if violated), decompress around it, floating technique
- Fusion is mandatory: post-laminectomy kyphosis 10-20 percent without fusion versus less than 2 percent with fusion
Complications
- C5 palsy (5-10 percent): delayed deltoid/biceps weakness 24-48h, 80-90 percent recover over 3-12 months, expectant management
- Dural tear (5-8 percent): primary repair 4-0 Nurolon, watertight closure, fibrin glue; post-op leak — bed rest and lumbar drain 5-7 days
- Epidural haematoma (1-2 percent): surgical emergency, urgent MRI and decompression within 6h
- Screw malposition (2-5 percent): medial breach over 4mm — revise; lateral breach — bone wax, avoid ligation
- Kyphosis (10-20 percent without fusion): swan-neck deformity; revise with anterior column support plus posterior fusion
- Vertebral artery injury (less than 0.5 percent): bone wax and gelfoam packing, avoid ligation (stroke risk)
- Pseudarthrosis (5-10 percent): smoking is the major risk (60 percent vs 90 percent fusion); revise if symptomatic
Post-op protocol
- Neuro checks hourly for 24h (C5 palsy, epidural haematoma); any deterioration = urgent MRI
- Mobilise day 1 (no collar needed with instrumented fusion); BLT precautions for 6 weeks
- Drain: remove below 50mL/24h (typically 24-48h)
- Imaging: day-1 radiographs, 3-month CT (bridging bone), 6-month flexion-extension (dynamic stability)
- Fusion takes 3-6 months cervical (faster than lumbar); CT bridging bone or less than 2mm flex-ex motion = fused
Exam tips
- C5 palsy: cord drift tethers the root; 5-10 percent incidence, delayed 24-48h, 80-90 percent recover, expectant
- Cervical root anatomy: exit ABOVE the pedicle (C5 at C4-5), opposite lumbar (L5 at L5-S1)
- Fusion mandatory: laminectomy removes the posterior tension band — kyphosis 10-20 percent without fusion, less than 2 percent with
- Magerl 25/45 vs Anderson 10/30: larger safe zone vs safer nerve root
- OPLL: leave the ossified dura intact (around 50 percent CSF leak if violated)
Background & Evidence
Why lordosis matters. The cervical cord sits towards the posterior canal only when the spine is lordotic. Laminectomy removes the posterior tension band and therefore has a kyphotic tendency — in a kyphotic spine the cord drapes over the vertebral bodies and remains compressed, which is why a preserved lordosis (20-40 degree C2-C7 Cobb angle) is the single most important indication criterion, and why instrumented fusion to maintain that lordosis is mandatory. Canal dimensions. The normal cervical canal measures 14-18mm sagittally; stenosis is defined as an absolute diameter below 13mm or a Pavlov ratio below 0.8. The cord is approximately 10mm, so the "space available for the cord" is the canal diameter minus the cord diameter. The surgical target after decompression is a canal diameter greater than 13mm. Post-laminectomy kyphosis. Without fusion, kyphosis develops in 10-20 percent of adults (and up to 50 percent of children); with instrumented fusion it falls below 2 percent. Risk factors: a multilevel laminectomy (more than 3 levels), young age (less than 25 years) and pre-existing loss of lordosis. This is the biomechanical justification for routine fusion. Lateral mass screw biomechanics. Pullout strength is 400-800N depending on bone density and trajectory. Optimal screw length is 12-14mm unicortical (16-18mm if bicortical, though bicortical is not required and risks anterior breach). Bilateral triangulation gives coronal stability; the rod-screw construct provides immediate rigid fixation, and compression across the levels loads the posterolateral graft. Key evidence. The AOSpine North America CSM study (Fehlings, 2013) showed anterior and posterior approaches are equivalent for cervical spondylotic myelopathy once patient and disease factors are controlled — the approach is chosen on alignment, level count and compression location. Heller (2001) found laminoplasty and laminectomy-with-fusion gave comparable decompression, but the laminectomy-fusion group carried more mechanical complications, underlining the need for solid instrumentation. Sakaura (2003) pooled the literature on the postoperative C5 palsy (mean 4.6 percent across techniques), establishing it as multifactorial and usually recovering. Yoshihara (2013) confirmed lateral mass screws have a very low neurovascular complication rate, and Anderson (1991) defined the original lateral mass fixation series with solid fusion and no neurovascular complications.
References
Anterior versus posterior surgical approaches for cervical spondylotic myelopathy (AOSpine North America CSM study)
- Prospective multicentre observational study of 264 patients (169 anterior, 95 posterior) across 12 North American sites
- Posterior cases had greater raw mJOA improvement (3.62 vs 2.47, P less than 0.01) but were older with more severe baseline myelopathy
- When patient and disease factors were controlled, anterior and posterior approaches showed equivalent efficacy
Laminoplasty versus laminectomy and fusion for multilevel cervical myelopathy: an independent matched cohort analysis
- Independently assessed matched cohort: 13 laminectomy-with-fusion versus 13 laminoplasty patients, mean follow-up about 26 months
- 14 complications in 9 laminectomy-fusion patients (nonunion, instrumentation failure, kyphosis, deep infection) versus none in the laminoplasty cohort
- Functional improvement (Nurick) tended to be greater after laminoplasty
C5 palsy after decompression surgery for cervical myelopathy: review of the literature
- Pooled literature (1986-2002): postoperative C5 palsy occurs in a mean of 4.6 percent of patients after cervical decompression
- Incidence did not differ significantly between anterior decompression-fusion and laminoplasty, or between CSM and OPLL
- Two competing mechanisms proposed (nerve root tethering versus segmental cord injury); prognosis generally good, with severe palsies needing longer recovery
Screw-related complications in the subaxial cervical spine: lateral mass versus cervical pedicle screws — a systematic review
- Systematic review of 10 lateral mass screw and 12 cervical pedicle screw studies (C3-C7)
- Vertebral artery injury was statistically more common with pedicle screws but extremely rare with both techniques
- Lateral mass screws trended toward more loosening, pullout and pseudarthrosis, but differences were not statistically significant
Posterior cervical arthrodesis with AO reconstruction plates and bone graft (original lateral mass fixation series)
- Prospective series of 30 unstable cervical spines fixed with lateral mass plate-and-screw constructs and autograft
- All patients achieved solid fusion at mean 17.8-month follow-up with no neurological or vascular complications
- Defined the Anderson lateral mass trajectory and demonstrated the technique where laminae and spinous processes are deficient
Radiculopathy and myelopathy at segments adjacent to a previous anterior cervical arthrodesis
- Landmark study establishing the natural history of adjacent segment disease after ACDF
- Defined the rationale that influences multilevel disease surgical planning
Stable posterior fusion of the atlas and axis by transarticular screw fixation
- Seminal description of the Magerl screw technique and the safe-zone concept
- Established the 25 degrees lateral, 45 degrees cephalad trajectory still taught today
Differences between laminectomy and laminoplasty: influence on sagittal alignment and range of motion in multilevel cervical myelopathy
- Biomechanical comparison of sagittal alignment after laminectomy versus laminoplasty
- Kyphosis rates: laminectomy without fusion 21 percent versus laminoplasty 0 percent at 2-year follow-up
Minimum 10-year follow-up after en bloc cervical laminoplasty
- Long-term outcome study of en bloc cervical laminoplasty
- Laminoplasty maintains decompression with a lower kyphosis rate than historical laminectomy without fusion
Anterior cervical decompression and arthrodesis for cervical spondylotic myelopathy: two to seventeen-year follow-up
- Classic long-term study establishing ACDF outcomes for cervical myelopathy
- Influential for determining when an anterior versus a posterior approach is indicated