Reverse Bankart repair with posterior capsular plication | advanced
- Posterior instability is often subtle - recurrent subluxation and pain rather than frank dislocation. The jerk test and Kim test are the key provocative manoeuvres; a positive posterior drawer with reproduction of symptoms confirms the diagnosis.
- At-risk populations include contact athletes (football linemen), weightlifters (bench press), and patients with seizures or electrical injury. Bilateral involvement occurs in up to 50 percent of atraumatic cases.
- Posterior glenoid bone loss greater than 20 percent or glenoid retroversion greater than 15 degrees changes the operative plan - arthroscopic soft-tissue repair alone has high failure rates; posterior bone block augmentation is indicated.
- The posterior labral bumper must be restored with at least three suture anchors placed at the 7, 8 and 9 o'clock positions (right shoulder) or 3, 4 and 5 o'clock (left shoulder). Capsular plication is performed in the same sitting to address the redundant posterior capsule.
When & Why
Indication. Symptomatic, recurrent posterior shoulder instability - typically pain and subluxation rather than frank dislocation - with a documented posterior labral (reverse Bankart) tear on MRI or MR-arthrography, that has failed non-operative management (a minimum of 3 to 6 months of structured physiotherapy focusing on scapular stabilisation, rotator-cuff strengthening and proprioception) and a positive jerk test or Kim test reproducing the patient's symptoms. Absolute indications - Recurrent posterior subluxation or dislocation with a documented posterior labral tear on MRI or MRA.
- Failed non-operative management (a minimum of 3 to 6 months of compliant, structured physiotherapy).
- A positive jerk test or Kim test reproducing symptoms with corresponding labral pathology on imaging. Relative indications - A contact or overhead athlete with functional instability limiting sport.
- A posterior labral tear with greater than 50 percent detachment, or associated posterior capsular redundancy.
- A reverse Hill-Sachs lesion of less than 20 percent of the articular surface that does not engage. Contraindications. These are the cases where an all-arthroscopic soft-tissue repair is the wrong operation and a posterior bone block (or combined procedure) is required instead. - Absolute: posterior glenoid bone loss greater than 25 percent or glenoid retroversion greater than 20 degrees (bone block augmentation required); an engaging reverse Hill-Sachs lesion greater than 25 percent of the humeral head articular surface; active infection or uncontrolled medical comorbidity.
- Relative: multidirectional instability with a predominant posterior component (consider a global capsular shift or arthroscopic pancapsular plication rather than an isolated posterior repair); poor tissue quality (Ehlers-Danlos, prior failed thermal capsulorrhaphy); a patient unable or unwilling to comply with the rehabilitation protocol. Try non-operative first. Structured physiotherapy - scapular stabilisation, rotator-cuff strengthening and proprioceptive training - resolves symptoms in approximately 50 to 70 percent of patients with first-time or low-demand posterior instability. Contact athletes and patients with significant labral detachment have lower success rates and warrant earlier surgical referral. Declare non-operative failure only after a minimum of 3 to 6 months of compliant therapy. Why arthroscopic, and when open. Modern arthroscopic capsulolabral reconstruction gives 85 to 95 percent success in properly selected patients, with lower morbidity, faster return to sport and better cosmesis than an open approach, and it permits simultaneous treatment of associated pathology (SLAP tears, rotator-cuff lesions, chondral injury). An open posterior approach is reserved for cases needing bone-block augmentation, or when arthroscopic access is limited by body habitus or prior surgery.
The default. Direct visualisation and anatomic restoration of the labral bumper, lower morbidity, faster return to sport. 85 to 95 percent success with proper selection and technique.
Reserved for posterior bone-block augmentation, or when arthroscopic access is limited by body habitus or prior surgery. Higher morbidity and a longer recovery.
Structured physiotherapy resolves symptoms in about 50 to 70 percent of first-time or low-demand cases. Declare failure only after 3 to 6 months of compliant therapy.
Consent specifically for recurrence (8 to 15 percent overall, higher in contact athletes), stiffness and loss of external rotation (5 to 12 percent), chondral injury, axillary nerve injury (less than 1 percent with correct portal placement), and the possibility of conversion to an open procedure or bone block if bone loss is greater than expected.
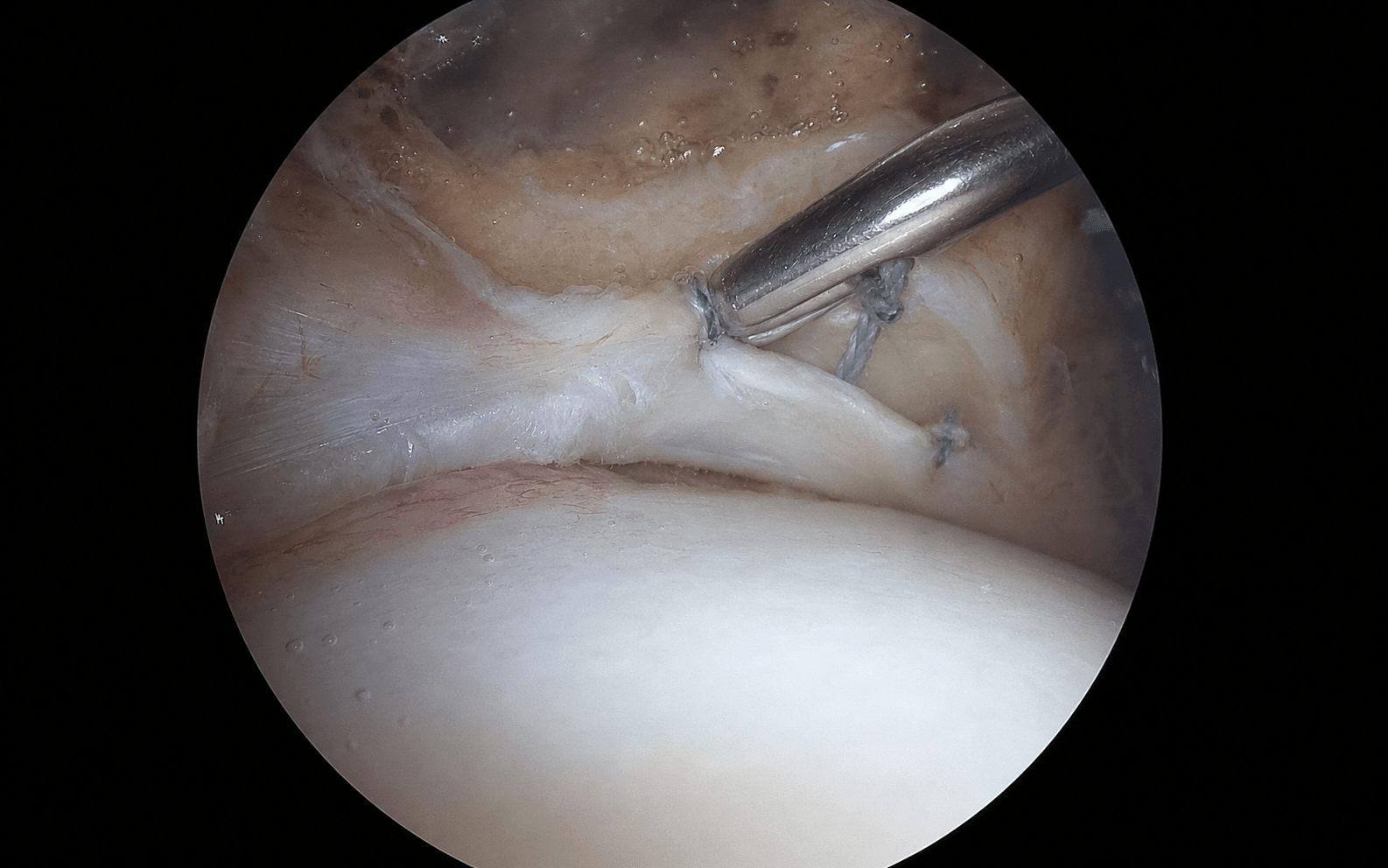
The Operation
The goal: restore the posterior labral bumper anatomically with at least three suture anchors, plicate a redundant posterior capsule, and confirm stable, congruent glenohumeral mechanics - all while protecting the axillary nerve. The exposure here is portal placement: the standard posterior and anterior-superior viewing portals are established first, then the accessory 7 o'clock working portal is added under needle localisation. The lateral decubitus position with balanced traction opens the posteroinferior joint and is what makes the inferior anchor reachable.
Operative sequence
- Lateral decubitus, operative arm in 10 to 15 pounds of balanced suspension traction, positioned in 20 to 30 degrees of abduction and 20 degrees of forward flexion. This opens the posterior and inferior joint spaces and gives excellent access to the posteroinferior labrum. The beach-chair position is an acceptable alternative but limits inferior access and demands careful portal placement.
- General anaesthesia with an interscalene block for postoperative analgesia. Hypotensive anaesthesia (systolic 90 to 100 mmHg) minimises bleeding and keeps the field clear.
- Standard posterior portal: 2 cm inferior and 1 cm medial to the posterolateral corner of the acromion; it enters the joint through (or between) infraspinatus and teres minor. This is the primary viewing portal.
- Anterior-superior portal: established under direct vision in the rotator interval, localised with an 18-gauge needle. Used for viewing during posterior work and for suture management.
- The internervous plane between infraspinatus (suprascapular nerve) and teres minor (axillary nerve) is respected; the axillary nerve lies 1.5 to 2.5 cm inferior to the inferior glenoid rim.
- Perform a full 15-point diagnostic arthroscopy before committing to posterior repair.
- Assess the posterior labrum from 6 o'clock to 11 o'clock (right shoulder), the posterior capsule for redundancy, the presence and size of any reverse Hill-Sachs lesion, glenoid version, and associated pathology (SLAP tear, rotator-cuff tear, chondral injury).
- Measure glenoid bone loss with a calibrated probe; document reverse Hill-Sachs size and engagement. This prevents the surprise of significant bone loss discovered halfway through a soft-tissue repair.
- Localise the accessory posterior (7 o'clock, right shoulder) portal with an 18-gauge needle placed 1 cm lateral and 1 cm inferior to the standard posterior portal, aiming for perpendicular access to the posteroinferior glenoid rim.
- Confirm the needle enters the joint at the desired location before incising and dilating. This working portal allows the inferior anchor to be placed at the correct angle.
- Axillary nerve safety: the nerve lies 1.5 to 2.5 cm inferior to the inferior glenoid rim - stay at least 1.5 cm superior to it, and use blunt dissection only.
- Debride the torn posterior labrum to a stable edge with a shaver or radiofrequency device.
- Elevate the labrum off the glenoid rim with an elevator and create a bleeding bony bed for healing.
- Mobilise the labrum sufficiently that it reduces to the glenoid rim without tension.
- Place the most inferior anchor first (7 o'clock right shoulder / 5 o'clock left shoulder) - the most demanding position, done while the field is clearest.
- Use 2.4 to 3.0 mm bioabsorbable or all-suture anchors loaded with high-strength suture. Right shoulder: 7, 8 and 9 o'clock. Left shoulder: 3, 4 and 5 o'clock.
- Drill or punch the anchor hole at a 45-degree angle to the glenoid surface, 2 to 3 mm onto the articular face of the glenoid rim - this recreates the bumper effect. Test each anchor by pulling the sutures before proceeding.
- Pass one limb of each anchor suture through the posterior capsule and labrum with a suture passer or shuttle relay, capturing a roughly 1 cm bite of capsule plus the labrum at the level of the anchor.
- Tie arthroscopic knots (a surgeon's knot, or a sliding knot with three reversing half-hitches) to secure the labrum to the glenoid rim.
- Repeat for each anchor, progressing superiorly; after each knot, assess the labral bumper height and the capsular plication achieved.
- After labral repair, probe the posterior capsule for redundancy. Plicate using the same anchors or additional mattress sutures placed between anchors.
- Plicate in 5 to 7 mm increments, aiming for a total posterior shift of about 1 cm.
- Avoid over-constraint: intraoperative external rotation in adduction should remain at least 30 to 40 degrees after plication. Check after each plication stitch.
- Perform a final dynamic stability assessment with the arthroscope in the joint: apply posterior force to the humerus and confirm the head stays centred on the glenoid.
- Check external rotation and elevation to ensure no over-constraint.
- Close portals with absorbable sutures, apply a sterile dressing, and place the arm in a sling with an abduction pillow.
The axillary nerve lies 1.5 to 2.5 cm inferior to the inferior glenoid rim and is at risk during accessory (7 o'clock) portal placement and any inferior capsular work. Use needle localisation before every accessory portal, stay at least 1.5 cm superior to the inferior glenoid rim, and use blunt dissection only. If injured: the deficit is usually a neuropraxia - observe with EMG surveillance; explore and repair if there is no recovery by 3 months.
Place each anchor 2 to 3 mm onto the articular face of the glenoid rim at a 45-degree angle. Too medial loses the bumper effect and guarantees recurrence; too lateral or proud abrades the articular cartilage. If a drill hole lands too medial, abandon it and re-drill at the anatomic position rather than accepting a non-anatomic anchor - never force an anchor into a bad hole.
Always obtain a 3D CT with an en-face glenoid view pre-operatively and confirm bone loss intra-operatively with a calibrated probe. Arthroscopic soft-tissue repair alone in posterior glenoid bone loss greater than 20 percent (or retroversion greater than 15 degrees) fails in over 40 percent - convert to a posterior bone block.
The trap: performing the jerk test supine, or without relaxation, misses subtle posterior subluxation. The fix: do it seated with the scapula stabilised - axial load in 90 degrees abduction, then internal rotation into adduction; a clunk or reproduced apprehension confirms posterior labral pathology.
The trap: a standard axillary lateral radiograph underestimates posterior bone loss. The fix: the en-face 3D CT view with the circle (or Pico) method is mandatory before committing to an all-arthroscopic plan; greater than 20 percent loss favours a bone block.
The risk: the axillary nerve lies 1.5 to 2.5 cm inferior to the inferior glenoid rim. The fix: needle-localise the 7 o'clock portal, stay at least 1.5 cm superior to the inferior glenoid rim, and use blunt dissection only.
The trap: an anterior humeral head defect greater than 20 percent that engages the posterior glenoid rim in internal rotation causes recurrence after labral repair alone. The fix: assess size and engagement on CT or MRI pre-operatively; engaging lesions need remplissage or bone grafting at the same sitting.
The trap: excessive posterior plication reduces external rotation and can cause stiffness or anterior subluxation. The fix: limit the shift to 1 cm; check external rotation after each plication stitch and stop at 30 to 40 degrees in adduction.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation & restrictions | Therapy & goals | |-------|--------|-------------------------------|-----------------| | 1 - Protection | 0 to 6 weeks | Sling with abduction pillow; no active internal rotation or cross-body adduction | Pendulum exercises; elbow, wrist and hand ROM from day 1; passive/active-assisted forward elevation to 90 degrees only; isometric external rotation from week 4 | | 2 - Motion | 6 to 12 weeks | Wean sling at 6 weeks | Progressive active ROM in all planes (goal full ROM by 12 weeks); gentle posterior capsular stretch; scapular stabilisation; no resistance until pain-free full ROM | | 3 - Strengthening | 12 to 18 weeks | Splint for heavy tasks only | Progressive rotator-cuff and scapular strengthening; closed-chain and proprioceptive work; sport-specific drills from week 16 | | 4 - Return to sport | 5 to 9 months | Functional brace considered for contact athletes in first season | Non-contact return at 4 to 5 months (at least 80 percent contralateral strength); contact clearance at 6 to 9 months requiring full pain-free ROM, symmetric strength and negative apprehension |
- Incidence
- 8 to 15 percent overall; 12 to 20 percent in contact athletes
- Recognition
- Recurrent subluxation or dislocation; positive jerk test; MRI showing recurrent labral tear or bone loss
- Prevention & management
- Prevention: accurate preoperative bone-loss assessment; adequate anchor number and placement; appropriate plication. Management: revision arthroscopy or open bone block; address missed bone loss or technical error
- Incidence
- 5 to 12 percent
- Recognition
- Loss of greater than 20 degrees external rotation versus the other side; limitation overhead
- Prevention & management
- Prevention: limit plication to a 1 cm total shift; assess external rotation after each stitch. Management: aggressive physiotherapy; capsular release if persistent and limiting beyond 6 months
- Incidence
- Less than 1 percent with correct technique
- Recognition
- Deltoid weakness; numbness over the lateral shoulder; positive EMG/NCS
- Prevention & management
- Prevention: stay greater than 1.5 cm superior to the inferior glenoid rim at the 7 o'clock portal; blunt dissection only. Management: observe for neuropraxia; explore and repair if no recovery by 3 months
- Incidence
- 2 to 5 percent
- Recognition
- Loose body; anchor on the articular surface; progressive degeneration on follow-up imaging
- Prevention & management
- Prevention: correct 45-degree anchor trajectory; assess bone stock pre-operatively. Management: remove loose anchor; chondral debridement or microfracture; bone grafting for large defects
- Incidence
- Less than 1 percent
- Recognition
- Erythema, swelling, warmth; raised CRP/ESR; positive aspirate culture
- Prevention & management
- Prevention: standard sterile technique; perioperative antibiotics. Management: arthroscopic washout and intravenous antibiotics; retain implants if stable and infection controlled
- Incidence
- 3 to 8 percent
- Recognition
- Persistent portal tenderness; ossification at portal sites on radiograph
- Prevention & management
- Prevention: meticulous portal closure; avoid excessive soft-tissue trauma. Management: local steroid injection; physiotherapy; rare surgical excision if symptomatic
Viva & Exam Focus
POSTERIORPOSTERIOR - key clinical features of posterior instability
ANCHORANCHOR - portal and anchor placement principles
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old college football offensive lineman presents with recurrent posterior shoulder subluxation during blocking drills. He has had three episodes over the past season despite a 4-month course of physiotherapy. MRI shows a posterior labral tear with 15 percent posterior glenoid bone loss. How do you manage him?”
“You are performing an arthroscopic posterior labral repair on a 28-year-old weightlifter. After placing the 7 o'clock anchor you notice the drill hole is too medial on the glenoid face. What do you do?”
“A 35-year-old man with a seizure disorder presents with recurrent posterior shoulder instability after a grand mal seizure 6 months ago. CT shows 25 percent posterior glenoid bone loss and a 22 percent reverse Hill-Sachs lesion that engages in internal rotation. What is your surgical plan?”
Diagnosis
- Presentation: recurrent subluxation and pain with bench press, blocking or seizures rather than frank dislocation
- Jerk test: axial load in 90 degrees abduction, internal rotation and adduction produces a clunk or apprehension
- Kim test: posterior force with the arm in 90 degrees abduction and 90 degrees flexion reproduces symptoms
- Posterior drawer: greater than 50 percent posterior translation with symptom reproduction is diagnostic
- Bilateral in up to 50 percent of atraumatic cases - screen the other shoulder
Imaging and bone loss
- MRI or MRA first-line for labral pathology, capsular redundancy and reverse Hill-Sachs
- 3D CT en-face glenoid view mandatory - quantify with the circle or Pico method
- Bone loss greater than 20 percent or retroversion greater than 15 degrees: consider a posterior bone block
- Assess reverse Hill-Sachs size (percent of articular surface) and engagement in internal rotation
- An axillary lateral radiograph underestimates bone loss - do not plan from it alone
Indications for surgery
- Failed 3 to 6 months of structured physiotherapy with a documented labral tear
- Recurrent subluxation or dislocation with a positive jerk or Kim test
- Contact or overhead athlete with functional limitation
- Posterior labral detachment greater than 50 percent or significant capsular redundancy
- Bone loss less than 20 percent and a non-engaging reverse Hill-Sachs less than 20 percent
Portals and danger zones
- Standard posterior portal: 2 cm inferior and 1 cm medial to the posterolateral acromion corner
- Accessory 7 o'clock portal: 1 cm lateral and 1 cm inferior to the standard posterior portal; stay greater than 1.5 cm superior to the inferior glenoid rim
- Anterior-superior portal: rotator interval, under direct vision, for viewing and suture management
- Axillary nerve: 1.5 to 2.5 cm inferior to the inferior glenoid rim - at risk with inferior portals or aggressive inferior capsular work
- Suprascapular nerve: at risk only with medial dissection or superior labral work (rarely an issue in isolated posterior repair)
Operative technique - key steps
- Lateral decubitus, 10 to 15 lb traction, 20 to 30 degrees abduction, 20 degrees forward flexion
- Complete 15-point diagnostic arthroscopy before committing to the posterior repair
- Three suture anchors at 7, 8 and 9 o'clock (right) or 3, 4 and 5 o'clock (left)
- Anatomic labral repair recreating the posterior bumper; about 1 cm total capsular plication
- Intraoperative stability and external-rotation check (minimum 30 to 40 degrees in adduction)
- Final dynamic testing with posterior force before closure
Bone loss and bipolar lesions
- Greater than 20 percent glenoid bone loss or greater than 15 degrees retroversion: posterior bone block indicated
- Engaging reverse Hill-Sachs greater than 20 percent articular surface: remplissage or humeral-head bone graft
- Bipolar bone loss: address glenoid and humeral head at the same sitting or staged
- Posterior bone block: iliac-crest autograft or allograft fixed with two cannulated screws or a buttress plate
- Remplissage: infraspinatus tenodesis into the reverse Hill-Sachs defect with suture anchors
Complications
- Recurrence: 8 to 15 percent overall; 12 to 20 percent in contact athletes; higher with underestimated bone loss
- Stiffness: 5 to 12 percent - limit plication to a 1 cm shift; assess external rotation intraoperatively
- Axillary nerve injury: less than 1 percent with correct portals - stay greater than 1.5 cm superior to the inferior glenoid rim
- Chondral injury or anchor pull-out: 2 to 5 percent - prevented by a correct 45-degree trajectory
- Infection: less than 1 percent - standard sterile technique and perioperative antibiotics
Rehabilitation and return to sport
- Phase 1 (0 to 6 weeks): sling with abduction pillow; pendulum exercises; passive elevation to 90 degrees only
- Phase 2 (6 to 12 weeks): wean sling; progressive active ROM; scapular stabilisation; no resistance until full ROM
- Phase 3 (12 to 18 weeks): progressive strengthening; closed-chain work; sport-specific drills from week 16
- Return to non-contact sport: 4 to 5 months at 80 percent strength and full pain-free ROM
- Return to contact sport: 6 to 9 months with symmetric strength, negative apprehension and sport-specific clearance
Background & Evidence
Epidemiology. Posterior shoulder instability is far less common than anterior, and the presentation is often subtle - recurrent subluxation and pain rather than frank dislocation. At-risk groups include contact athletes (football linemen), weightlifters (bench-press loading), and patients with seizures or electrical injury. Bilateral involvement occurs in up to 50 percent of atraumatic cases, so the contralateral shoulder should always be screened. Pathoanatomy. The posterior labrum is a fibrocartilaginous ring attached to the glenoid rim that deepens the socket by approximately 50 percent and anchors the posterior capsule and the posterior band of the inferior glenohumeral ligament. Detachment of the posterior labrum (the reverse Bankart lesion) allows posterior translation of the humeral head and is the primary pathology in traumatic posterior instability. The posterior capsule is thinner than the anterior, blends with the infraspinatus tendon, and is commonly redundant - which is why plication is performed in the same sitting as the labral repair. Glenoid version and bone loss. Normal glenoid version is 0 to 7 degrees of retroversion. Retroversion greater than 15 degrees, or posterior glenoid bone loss greater than 20 percent of the glenoid width, significantly increases the risk of failure after soft-tissue repair alone. Bone loss is quantified on 3D CT using the circle (or Pico) method on the en-face glenoid view. Reverse Hill-Sachs lesion. An anterior humeral-head impaction fracture sustained when the head strikes the posterior glenoid rim during posterior dislocation. Lesions involving greater than 20 percent of the articular surface, or those that engage the glenoid rim in internal rotation, require an additional procedure (remplissage, bone grafting) at the time of labral repair.
- Recurrence after soft-tissue repair alone
- 8 to 12 percent
- Recommended approach
- Arthroscopic labral repair with capsular plication
- Recurrence after soft-tissue repair alone
- Greater than 40 percent
- Recommended approach
- Posterior bone block (iliac-crest autograft or allograft) with or without soft-tissue repair
- Recurrence after soft-tissue repair alone
- Soft-tissue repair contraindicated
- Recommended approach
- Open posterior bone block fixed with two cannulated screws or a buttress plate
- Success rate
- 88 to 94 percent
- Recurrence
- 6 to 12 percent
- Return to sport
- 80 to 90 percent at 6 months
- Success rate
- 55 to 65 percent
- Recurrence
- 35 to 45 percent
- Return to sport
- 50 to 60 percent
- Success rate
- 90 to 95 percent
- Recurrence
- 5 to 8 percent
- Return to sport
- 75 to 85 percent
- Success rate
- 80 to 88 percent
- Recurrence
- 12 to 20 percent
- Return to sport
- 70 to 80 percent
- Success rate
- 75 to 85 percent
- Recurrence
- 15 to 25 percent
- Return to sport
- 65 to 75 percent
Key evidence. Bradley's prospective series established arthroscopic capsulolabral reconstruction as reliable in selected patients (good-to-excellent outcomes in the great majority, low recurrence). Robinson and Aderinto's review defined the diagnostic value of the provocative tests (jerk test around 97 percent sensitive and 90 percent specific) and the central importance of bone-loss quantification. DeLong and colleagues' meta-analysis confirmed an overall recurrence near 8 percent but a clearly higher rate in contact athletes - the basis for counselling and for considering bone augmentation. Bois and colleagues quantified glenoid bone loss in posterior instability and showed the steep rise in recurrence above 20 percent that bone-block augmentation offsets. The consistent message across the literature: arthroscopic repair is effective when bone loss is modest and the lesion is non-engaging, but bone loss greater than 20 percent (or an engaging reverse Hill-Sachs) must be identified pre-operatively and augmented.
References
Arthroscopic capsulolabral reconstruction for posterior instability of the shoulder: a prospective study of 100 shoulders
- Prospective study of 100 shoulders with posterior instability treated arthroscopically with capsulolabral reconstruction
- Good to excellent results in 91 percent; return to sport at the pre-injury level in 82 percent
- Recurrence rate of 9 percent at short-to-medium follow-up
Recurrent posterior shoulder instability
- Comprehensive review of recurrent posterior shoulder instability
- The jerk test was around 97 percent sensitive and 90 percent specific for posterior labral pathology
- Patients with greater than 20 percent glenoid bone loss had significantly higher failure rates after soft-tissue repair alone
Posterior instability of the shoulder: a systematic review and meta-analysis of clinical outcomes
- Meta-analysis of 12 studies comprising 438 patients after arthroscopic posterior labral repair
- Overall recurrence 8.2 percent; return to sport 82 percent at mean 36 months follow-up
- Contact athletes had higher recurrence (around 14 percent) than non-contact athletes (around 5 percent)
Glenoid bone loss in posterior shoulder instability: quantification and clinical implications
- Retrospective review of 45 patients with posterior instability undergoing 3D CT assessment
- Mean posterior glenoid bone loss was 13.4 percent; 24 percent of patients had greater than 20 percent loss
- Patients with greater than 20 percent loss had 43 percent recurrence after soft-tissue repair versus 8 percent when a bone block was added
Long-term outcomes of arthroscopic posterior shoulder stabilisation
- Prospective evaluation of 33 patients at mean 5.2 years after arthroscopic posterior stabilisation
- ASES scores improved from 48 to 86 points; recurrence occurred in 12 percent
- External rotation loss averaged 8 degrees; 88 percent rated their shoulder good or excellent