Lateral position | Perforator ligation | Linea aspera exposure
- Lateral decubitus or prone positioning allows gravity to retract the vastus lateralis anteriorly once the septum is divided.
- The deep interval is posterior to the vastus lateralis, which is reflected anteriorly off the lateral intermuscular septum.
- Ligate every perforating branch of the profunda femoris as it pierces the septum — six to eight in total — because a retracted perforator is the major source of intra-operative haemorrhage.
- The linea aspera is the key bony landmark; subperiosteal elevation from it exposes the posterior femoral cortex and is the ideal plate bed.
- The sciatic nerve lies medial to the linea aspera in the proximal third — identify and protect it before any medial or posterior femoral work.
When & Why
What it exposes. The posterolateral approach gives extensile access to the femoral shaft from the greater trochanter to the lateral femoral condyle. Working the interval immediately behind the vastus lateralis and anterior to the lateral intermuscular septum delivers subperiosteal control of the linea aspera and the posterior, lateral and medial cortices through a single incision. Primary indications - Femoral shaft fractures requiring plate fixation — transverse, short oblique, or comminuted patterns unsuitable for intramedullary nailing.
- Femoral nonunion or malunion requiring open reduction, bone grafting and plate stabilisation.
- Infected nonunion requiring debridement, sequestrectomy and local antibiotic delivery.
- Tumour resection or biopsy of femoral shaft lesions.
- Revision surgery after failed intramedullary nailing when nail removal and exchange plating is planned. Why this approach is chosen. The linea aspera is the biomechanically ideal plate bed, and the exposure avoids the quadriceps mechanism anteriorly and the medial neurovascular bundle. It is extensile along almost the entire femur and can be combined with a separate anterolateral incision when dual plating or circumferential access is required. Contraindications (mostly relative) - Active infection in the surgical field (may still proceed for debridement).
- Severe soft-tissue loss or scarring that precludes closure.
- Inability to tolerate lateral or prone positioning (severe cardiopulmonary disease).
- Isolated anterior femoral lesions, which are better approached anterolaterally. Alternative approaches - Anterolateral approach — for proximal femoral fractures or when anterior plating is planned.
- Direct lateral approach — limited exposure, insufficient for long-plate constructs.
- Medial approach — rarely used; risks the femoral artery and vein.
- Posterior (Kocher–Langenbeck) approach — for acetabular or proximal pathology, not the shaft. Position & landmarks. Position the patient in lateral decubitus (affected side up) on a radiolucent table with full AP and lateral fluoroscopic access, or prone on chest rolls when bilateral posterior work is planned. Pad every pressure point (greater trochanter, fibular head, malleoli, axilla) and support the upper arm with the lower arm well padded. Slightly extend the affected hip and flex the knee 30–40 degrees to relax the sciatic nerve. Prep from the iliac crest proximally to the knee distally so the incision can extend in either direction. The palpable landmarks are the greater trochanter (proximal extent), the lateral femoral condyle (distal extent) and Gerdy's tubercle for distal orientation; the linea aspera is not directly palpable but corresponds to the posterior midline of the thigh. Soft-tissue guides are the iliotibial tract (a tight band along the lateral thigh with the knee extended), the biceps femoris tendon (posterior at the knee) and the vastus lateralis belly (anterior limit of dissection). Plan a 15–25 cm longitudinal incision along the posterior border of the iliotibial tract, centred over the pathology, allowing three to four screw holes proximal and distal to the fracture.
Lateral decubitus risks brachial plexus injury from a malpositioned axillary roll, compartment syndrome of the dependent leg, and sciatic nerve stretch if the hip is over-flexed. Pad the axilla, document every protective measure, and check the dependent leg's pulses and compartments regularly.
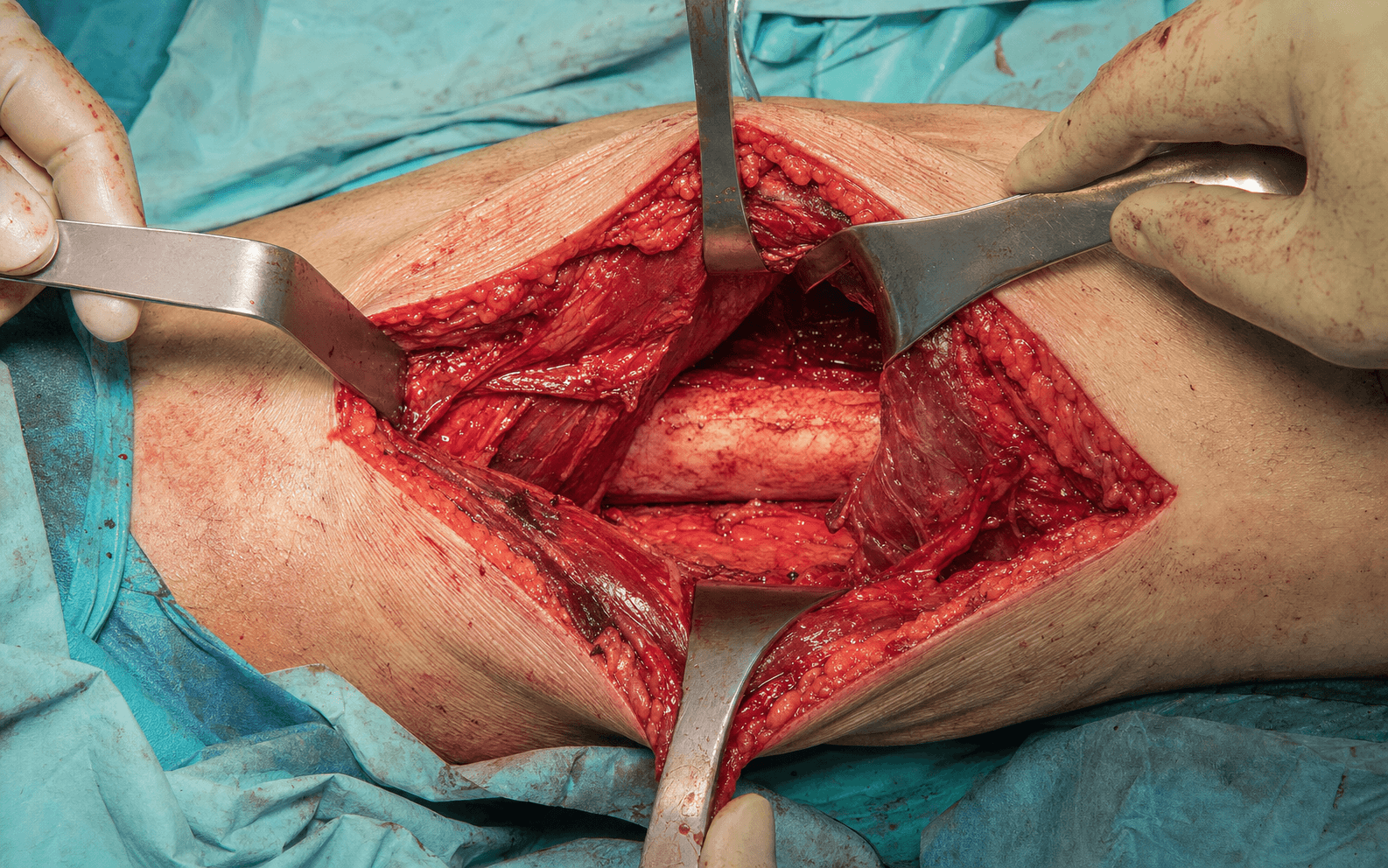
The Exposure
Work down through the layers along the posterior border of the iliotibial tract, develop the plane behind the vastus lateralis, divide the lateral intermuscular septum, ligate each perforator in continuity, and reach the linea aspera subperiosteally.
Exposure sequence
- Make a longitudinal skin incision along the posterior border of the iliotibial tract, centred over the fracture or pathology.
- Length is dictated by the required plate — typically enough for three to four screw holes proximal and distal to the lesion (15–25 cm).
- The line extends proximally along the posterior border of the greater trochanter and distally along the lateral femoral condyle, staying anterior to the biceps femoris tendon.
- Incise skin and subcutaneous tissue in line with the skin incision; identify and preserve branches of the lateral cutaneous nerve of the thigh if they cross the field.
- Incise the fascia lata in the line of the incision to expose the iliotibial tract, then open the tract longitudinally along its posterior border to reveal the vastus lateralis belly.
- Palpate the firm fascial plane posterior to the vastus lateralis — this is the lateral intermuscular septum, continuous with the linea aspera.
- Develop the plane between the posterior surface of the vastus lateralis and the anterior surface of the septum with blunt dissection.
- Incise the lateral intermuscular septum longitudinally with scissors or diathermy.
- Reflect the vastus lateralis anteriorly off the septum and the linea aspera with a Cobb or periosteal elevator, working so that gravity (in lateral decubitus) assists the retraction.
- Multiple perforating arteries will now be seen piercing the septum from posterior to anterior — do not divide any until it is controlled.
- Identify each perforator as it emerges through the septum, isolate it with a right-angled clamp, apply two ligatures or vascular clips, and divide between them.
- There are usually six to eight perforators along the femur from the profunda femoris; each must be controlled before it is cut.
- A vessel that is divided without ligation retracts into the posterior compartment, where bleeding is profuse and difficult to control.
- With all perforators controlled, continue subperiosteal elevation around the posterior, medial and lateral cortex to expose the linea aspera fully.
- The nutrient artery (a branch of the second perforator) enters near the linea aspera in the middle third and may bleed briskly — control it with bone wax or diathermy.
- Circumferential exposure allows plate placement on the lateral (tension-side) or posterior surface as biomechanics demand.
The posterolateral approach is one of the few true internervous exposures in the lower limb. The deep plane runs between the vastus lateralis (femoral nerve) anteriorly and the short head of biceps femoris (sciatic nerve, tibial division) posteriorly. Because the short head of biceps is small and the dissection stays lateral to it, no muscle is functionally denervated. The technical keys are to stay immediately posterior to the lateral intermuscular septum and to ligate every perforating vessel before it retracts into the posterior compartment.
Anatomy that governs the exposure - Bone: the femoral shaft is triangular in cross-section in the middle third, with the linea aspera forming the posterior apex. The shaft bows anteriorly with an average anterior bow of 10–15 degrees, and the nutrient foramen lies near the linea aspera in the middle third, entering from posterior.
- Muscle: the vastus lateralis arises from the linea aspera and the lateral intermuscular septum and is the only quadriceps muscle encountered. The lateral intermuscular septum separates the anterior compartment (vastus lateralis) from the posterior compartment (short head of biceps femoris and adductor magnus).
- Vessels: the perforating arteries (six to eight) arise from the profunda femoris, pierce the adductor magnus and the lateral intermuscular septum, and supply the vastus lateralis — each must be ligated.
- Nerve: the sciatic nerve lies in the posterior compartment, medial to the linea aspera in the proximal third, at risk during medial retraction; the femoral artery lies anteromedially and is shielded by the vastus medialis unless dissection is carried aggressively medial.
Missed or inadequately ligated perforating arteries are the most common cause of intra-operative blood loss in this approach. A single uncontrolled perforator can bleed 50–100 mL per minute, and a divided vessel retracts into the posterior compartment where it is hard to see. Ligate every perforator in continuity before cutting, working systematically from one end of the exposure to the other.
In the proximal third the sciatic nerve lies immediately medial to the linea aspera, deep to gluteus maximus and adductor magnus. Identify and protect it with a medial retractor or Langenbeck before any posterior femoral exposure proximally. Most injuries are traction or compression rather than transection, but the resulting foot drop is devastating.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Lateral cutaneous nerve of the thigh
- Protection strategy
- Identify and preserve branches where possible
- Structure at risk
- Lateral intermuscular septum
- Protection strategy
- Incise longitudinally; protect the underlying muscle
- Structure at risk
- Vastus lateralis
- Protection strategy
- Reflect anteriorly off the septum; guard the belly with retractors
- Structure at risk
- Perforating arteries (6–8) from profunda femoris
- Protection strategy
- Ligate each in continuity before division
- Structure at risk
- Sciatic nerve (proximal third)
- Protection strategy
- Identify medial to linea aspera; protect with a retractor
- Structure at risk
- Nutrient artery (branch of the second perforator)
- Protection strategy
- Anticipate at the middle-third linea aspera; bone wax or diathermy
Intra-operative complications
- Prevention
- Ligate each vessel in continuity before division
- Management
- Pack and ligate at source; detach short head of biceps to access the posterior compartment; vascular consult if uncontrolled
- Prevention
- Identify early in the proximal third; protect with a retractor
- Management
- Document; primary repair if transected; EMG follow-up
- Prevention
- Anticipate at the middle-third linea aspera
- Management
- Bone wax, diathermy or ligation
- Prevention
- Plan incision length and extensile options pre-operatively
- Management
- Extend proximally or distally as required
Post-operative complications
- Incidence
- 1–3%
- Prevention
- Careful proximal dissection and retraction
- Treatment
- AFO; EMG at 3 weeks; explore if no recovery by 3–6 months
- Incidence
- 2–5%
- Prevention
- Prophylactic antibiotics; meticulous haemostasis
- Treatment
- Irrigation and debridement; antibiotics; implant removal if needed
- Incidence
- 5–10% (higher in revision)
- Prevention
- Bone graft; stable fixation; optimise biology
- Treatment
- Revision plating and grafting; consider nail conversion
- Incidence
- 5–10%
- Prevention
- Anatomic reduction; long plate with adequate working length
- Treatment
- Corrective osteotomy if symptomatic
- Incidence
- 3–8%
- Prevention
- Chemoprophylaxis; early mobilisation
- Treatment
- Anticoagulation; IVC filter if recurrent
- Incidence
- 10–20%
- Prevention
- Early ROM exercises
- Treatment
- Physiotherapy; manipulation under anaesthesia if refractory
Sciatic nerve injury management - If the nerve is found transected intra-operatively, perform a primary repair; if neurapraxia is suspected, document and refer.
- For post-operative foot drop, obtain urgent EMG/NCS at 3 weeks and consider exploration if there is no recovery by 3–6 months.
- The reconstructive option for permanent foot drop is a tibialis posterior transfer to the dorsum of the foot. Extensile options - Proximal extension — carry the incision along the posterior border of the greater trochanter, split or retract the gluteus maximus in line with its fibres, and identify the sciatic nerve medial to the proximal femur to reach the piriformis fossa and subtrochanteric region. Watch for the superior gluteal vessels and the sciatic nerve.
- Distal extension — run the incision along the lateral femoral condyle, anterior to the biceps femoris tendon, open the iliotibial tract and reflect the vastus lateralis anteriorly; the knee capsule can be opened for intra-articular extension, protecting the lateral collateral ligament and popliteus posteriorly.
- Circumferential exposure — continuing subperiosteal elevation medially exposes the medial cortex and permits dual plating (lateral with posterior or medial) through the same incision.
- Combined approaches — pair the posterolateral with an anterolateral approach (through a separate incision) for dual plating of comminuted fractures, or with a medial approach for complex nonunion with bone loss; staged repositioning (lateral then supine) may be required. Closure & post-operative care - The lateral intermuscular septum needs no formal closure; close the fascia lata (iliotibial tract) with interrupted or continuous absorbable suture, let the vastus lateralis fall back, and close subcutaneous tissue and skin over a drain if dissection was extensive.
- Confirm reduction and fixation with AP and lateral radiographs of the entire femur.
- Neurovascular checks documenting sciatic function (dorsiflexion, plantarflexion, sensation) every 2 hours for the first 24 hours, with limb elevation and DVT prophylaxis (LMWH or aspirin per protocol, minimum 4–6 weeks).
- Weight bearing: non- or touch-weight-bearing for 6–12 weeks, progressing on radiographic healing to full weight bearing at 3–6 months for nonunion or comminuted fractures.
- Range of motion: early hip and knee ROM, aiming for full knee flexion and extension by 6–8 weeks, with quadriceps and hamstring strengthening once the wound has healed.
- Follow-up: 2 weeks (wound and suture/staple removal), 6 weeks, 3 months, 6 months (confirm union), and 1 year (final review).
Procedures Through This Approach
- Femoral shaft plating — the principal operation: 4.5 mm broad or narrow DCP, LC-DCP or locking compression plate of adequate length, applied laterally (tension side) or posteriorly for buttress of posterior comminution, with cortical screws in compression diaphyseally and locking screws in poor-quality metaphyseal bone.
- Nonunion and malunion revision — debridement of the nonunion to bleeding bone, reduction, long-plate stabilisation with an adequate working length, and autograft (iliac crest or RIA from the contralateral femur) packed around the site; the exposure gives excellent posteromedial and posterolateral graft access.
- Infected nonunion — debridement, sequestrectomy and local antibiotic delivery with stabilisation.
- Tumour resection or biopsy of shaft lesions.
- Revision after failed intramedullary nailing — nail removal with exchange plating and grafting.
- Distal femur and Hoffa-type fractures — posterior-based plating and screw fixation through the distal extension.
Viva & Exam Focus
FEMUR PLATEFEMUR PLATE — the posterolateral exposure, step by step
LIGATELIGATE — the perforator ligation sequence
Exam viva scenarios
Practise clinical reasoning and management decisions out loud
“A 38-year-old man has a femoral shaft nonunion nine months after intramedullary nailing, with a hypertrophic nonunion and a broken distal locking screw on CT. How would you approach the revision?”
“A 55-year-old woman sustains a proximal-third femoral shaft fracture from a low-energy fall — a short oblique fracture with medial comminution extending into the subtrochanteric region. What approach would you use and what structures are at particular risk?”
“During a posterolateral approach for shaft plating, brisk bleeding erupts from a vessel that has retracted into the posterior compartment after being divided. How do you manage this?”
Patient position
- Lateral decubitus (affected side up) preferred — gravity retracts the vastus lateralis
- Alternative: prone on a radiolucent table with chest rolls
- Pad all pressure points (greater trochanter, fibular head, axilla)
- Radiolucent table with full AP and lateral fluoroscopy
- Prep from iliac crest to knee for extensile exposure
Internervous plane
- Between vastus lateralis (femoral nerve) and the short head of biceps femoris (sciatic nerve)
- A true internervous plane — no muscle is denervated
- The lateral intermuscular septum is the key landmark
- Incise the septum longitudinally to develop the plane
- Reflect the vastus lateralis anteriorly off the septum
Perforating arteries
- Six to eight perforators from the profunda femoris pierce the septum
- Ligate each vessel in continuity before division
- A retracted vessel is reached by detaching the short head of biceps femoris
- Uncontrolled perforator bleeding is the commonest intra-operative complication
- Control the nutrient artery at the mid-shaft linea aspera with bone wax
Sciatic nerve protection
- Lies medial to the linea aspera in the proximal third
- Identify it early before any medial or posterior femoral work
- Protect with a Langenbeck or Hohmann retractor proximally
- Injury causes foot drop and possible loss of knee flexion
- Most injuries are traction or compression, not transection
Linea aspera exposure
- Posterior ridge where all three vasti and the adductors attach
- Subperiosteal elevation begins here and proceeds circumferentially
- Ideal plate bed for biomechanical strength
- The nutrient foramen lies near it in the middle third
- Allows lateral or posterior plate positioning
Extensile options
- Proximal: extend to the greater trochanter; protect the sciatic nerve and gluteal vessels
- Distal: extend to the lateral femoral condyle; protect the LCL and popliteus
- Reaches from the piriformis fossa to the lateral tibial plateau
- Combine with an anterolateral approach for dual plating
- Staged repositioning may be needed for combined anterior and posterior work
References
Clinical effect of locking compression plate via posterolateral approach in the treatment of distal femoral fractures: a new approach.
- The posterolateral approach allowed direct visualisation and stable fixation of distal femoral fractures with locking compression plates.
- High union rates were achieved with low complication rates in the reported clinical series.
Biomechanics of internal fixation in Hoffa fractures — a comparison of four different constructs.
- Posterior plating constructs gave superior biomechanical stability for comminuted distal femoral fractures.
- Combined dual plating offered the greatest resistance to displacement under load.
Two and three-dimensional CT mapping of Hoffa fractures.
- CT mapping defined consistent fracture planes that inform extensile posterolateral approaches to the distal femur.
- Understanding the three-dimensional morphology improves reduction accuracy through posterior-based exposures.
Meta plate and cannulated screw fixation for treatment of type Letenneur III lateral Hoffa fracture through posterolateral approach.
- The posterolateral approach gave safe and effective exposure for fixation of lateral Hoffa fractures.
- A meta plate with cannulated screws achieved stable fixation and good clinical outcomes.