Posterior (Moore/Southern) approach · end-stage hip osteoarthritis · intermediate
- The posterior (Moore/Southern) approach is the most common worldwide. Split gluteus maximus in line with its fibres — the only TRUE internervous plane in hip surgery (dual innervation by the superior and inferior gluteal nerves), so all motor function is preserved.
- Tag every short external rotator tendon and capsular flap with heavy sutures BEFORE you cut. Meticulous posterior soft-tissue repair at closure reduces dislocation roughly 3-4 fold, from 3-5 percent down to under 1 percent (Pellicci 1998).
- Seat the cup in the Lewinnek safe zone — 40-45 degrees inclination and 15-20 degrees anteversion — where dislocation runs 1.5 percent versus 6.1 percent outside it (Lewinnek 1978). Refine with combined anteversion: cup plus stem version totalling 25-45 degrees.
- Supplemental screws go POSTEROSUPERIOR only. Anteroinferior screws endanger the external iliac vessels, which lie 15-25 mm anterior to the acetabular wall — a potentially fatal injury.
- Broach handle LATERAL to avoid varus, and protect the sciatic nerve throughout — it lies 2 cm posterior to piriformis and 20-30 mm behind the capsule. Limit leg lengthening to less than 4 cm.
When & Why
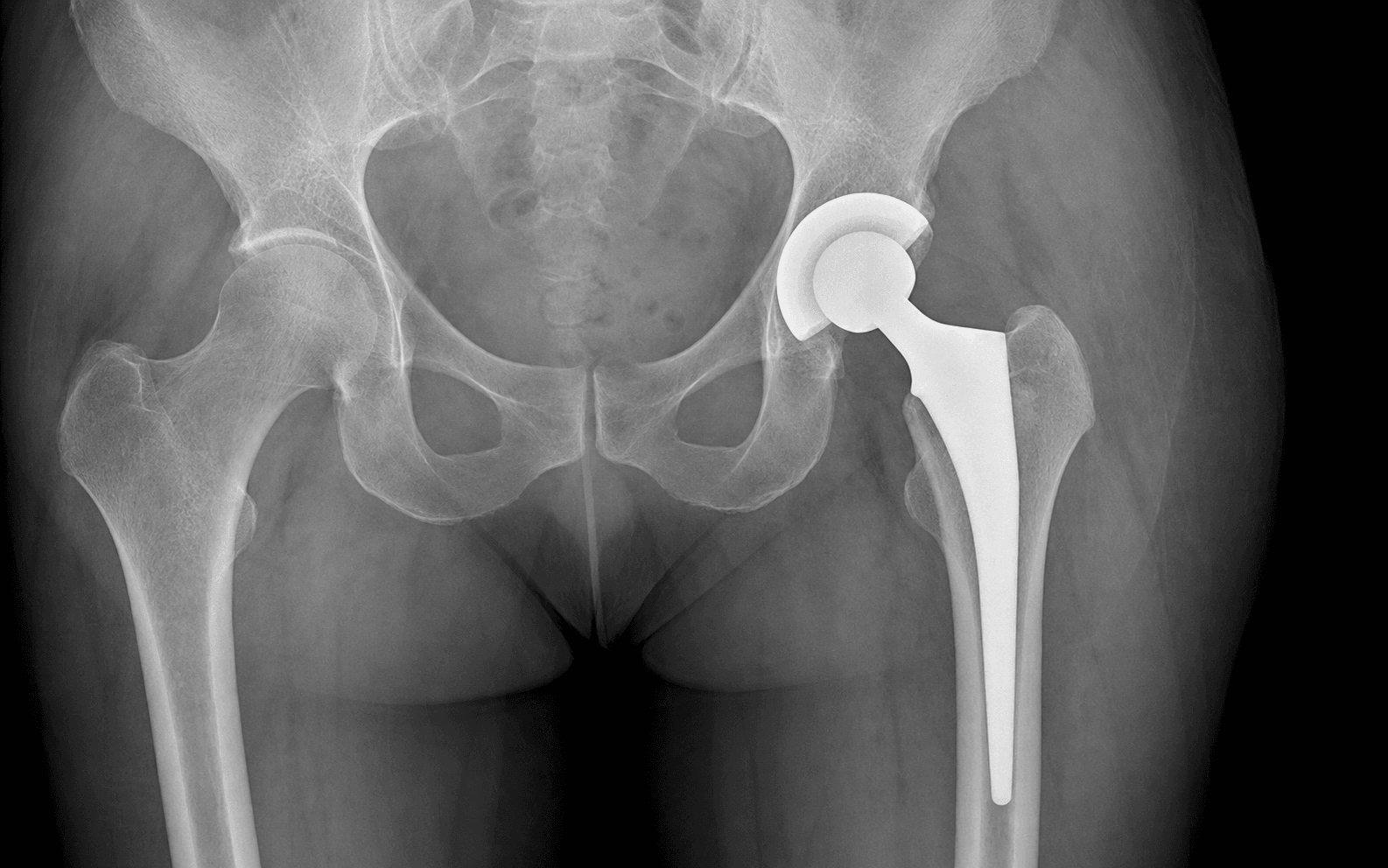
Indication. End-stage hip arthritis with pain limiting daily activities, night pain and functional decline that has failed conservative management (analgesia, activity modification, physiotherapy, weight loss). Radiographs show the triad of osteoarthritis — joint-space loss, osteophytes and subchondral sclerosis with cyst formation. Primary idiopathic osteoarthritis is the most common elective indication. The same operation serves a broad set of secondary causes: - Secondary osteoarthritis — developmental dysplasia of the hip (DDH; demands careful templating and often specialist cups), avascular necrosis, post-traumatic arthritis after acetabular or femoral fracture, and the adult sequelae of SUFE or Perthes disease.
- Inflammatory arthritis — rheumatoid arthritis (often bilateral, poor bone stock, younger patients) and ankylosing spondylitis (a fixed spinal deformity alters cup positioning and spinopelvic mobility).
- Acute fracture — a displaced intracapsular neck-of-femur fracture in an active, independent elderly patient with good life expectancy, where total hip arthroplasty outperforms hemiarthroplasty. Contraindications
- Examples
- Active local or systemic infection; inadequate soft-tissue cover; severe peripheral vascular disease with an ischaemic limb; Charcot (neurogenic) arthropathy with a high failure rate
- Examples
- Poor bone stock (severe osteoporosis, prior irradiation); skeletal immaturity; medical comorbidities precluding surgery; likely non-compliance with precautions; progressive neurological disease affecting the limb
Preoperative planning. Calibrated templating of an AP pelvis and a lateral femur determines cup size and position (restoring the centre of rotation at the teardrop), stem size, neck length and offset, and the planned leg-length restoration (teardrop to lesser trochanter, bilaterally). Identify bone defects that need augmentation. Approach selection — four options, one default.
The most common approach worldwide. True internervous plane (split gluteus maximus), excellent exposure, abductors preserved. Higher dislocation risk than anterior — controlled by meticulous soft-tissue repair.
Muscle-sparing. Lowest dislocation rate, but needs a traction table and fluoroscopy and carries a steeper learning curve; the lateral femoral cutaneous nerve is at risk.
Splits the abductor mechanism. Low dislocation rate, but abductor weakness and a Trendelenburg gait are the trade-off.
Works between TFL and gluteus medius. Low dislocation with some abductor risk; versatile exposure.
Fixation and bearing — a global registry picture. Cementless acetabular components dominate in nearly every high-volume registry (roughly 90 percent of primary cups). Femoral fixation diverges by region: cementless stems predominate in Australia and North America, while the UK NJR and the Nordic registries retain a substantial share of cemented and hybrid stems, particularly in patients over 70-75 years and in osteoporotic bone — because cemented stems virtually eliminate early periprosthetic femoral fracture in the elderly. Ceramic-on-highly-cross-linked-polyethylene and metal-on-XLPE are the dominant bearings; metal-on-metal has been abandoned. Consent specifically for dislocation (and the precautions that prevent it), leg-length discrepancy, sciatic nerve injury (foot drop), periprosthetic fracture, infection (PJI), VTE, and the long-term reality that roughly 58 percent of hips last 25 years on registry data. Setup. Lateral decubitus with the pelvis perpendicular to the floor and securely supported at the sacrum and symphysis (position is the commonest cause of cup malposition). Regional anaesthesia preferred. Mark the greater trochanter, ASIS, PSIS and the femoral shaft axis, and drape the leg free so it can be manoeuvred for dislocation.
The Operation
The goal is to expose the hip through the posterior approach, remove the arthritic femoral head, implant an acetabular cup in the safe zone and a femoral stem at the correct version and offset, confirm stability, and close with a meticulous capsular and short-rotator repair that protects against dislocation. The exposure — the heart of the operation — is laid out as the first steps below.
Operative sequence (posterior approach)
- Lateral decubitus, affected hip up, pelvis perpendicular to the floor; secure at the sacrum and symphysis with padded supports.
- Dependent leg flexed at hip and knee to relax the sciatic nerve; pillow between the legs.
- Mark the greater trochanter (centres the incision), ASIS, PSIS and the femoral shaft axis.
- Curved incision 10-15 cm centred on the greater trochanter, extending proximally toward the PSIS and distally along the femoral shaft axis.
- Incise the fascia lata in line with the skin; identify the oblique fibres of gluteus maximus beneath.
- Split gluteus maximus bluntly IN LINE with its fibres — the only true internervous plane in hip surgery (superior third supplied by the superior gluteal nerve, inferior two-thirds by the inferior gluteal nerve, so splitting preserves all motor function).
- Stay in the distal two-thirds; the inferior gluteal neurovascular bundle enters proximally.
- Do not extend the split more than 5 cm above the trochanter — the superior gluteal nerve exits the sciatic notch 25-40 mm proximal to the trochanter tip.
- Place Hohmann retractors anterior and posterior to expose the rotators; palpate the sciatic nerve 2 cm posterior to piriformis and protect it throughout.
- Identify the short external rotators from superior to inferior: piriformis, superior gemellus, obturator internus, inferior gemellus, quadratus femoris.
- Tag each tendon with a heavy suture BEFORE dividing it — essential for anatomic repair at closure.
- Detach piriformis and the conjoined tendon (superior gemellus plus obturator internus plus inferior gemellus); preserve quadratus femoris where possible to protect the medial femoral circumflex artery.
- T-shaped capsulotomy; tag the flaps with heavy absorbable sutures and preserve as much capsule as possible — do not excise, just incise.
- Dislocate by flexing to 90 degrees, adducting across the midline and internally rotating with gentle posterior force.
- Remove the femoral head with a corkscrew; inspect the wear pattern and osteophytes and send the head for histology and microbiology.
- Make the cut at the templated level — approximately 1 cm above the lesser trochanter, perpendicular to the shaft in the coronal plane.
- Preserve the calcar (medial cortical thickening) for stem stability; inspect the cut surface for occult fracture lines (if present, consider a cemented stem or prophylactic cerclage).
- Protect the posterior soft tissues and the sciatic nerve as the saw exits.
- Three retractors for a 360-degree view: anterior (over the anterior column, on bone), posterior (over the ischium, protecting the sciatic nerve), and inferior (blunt Hohmann into the obturator foramen).
- Excise the labrum circumferentially, clear osteophytes (especially inferior), and identify the transverse acetabular ligament (inferior extent) and the fovea (anatomic centre).
- Ream medially to bleeding subchondral bone, progressing in 2 mm increments, aiming for the anatomic centre of rotation at the teardrop with peripheral rim contact. The final reamer size plus 1-2 mm sets the press-fit cup size.
- Impact the cup at 40-45 degrees inclination and 15-20 degrees anteversion (radiographic), referenced to the transverse ligament and the patient's position; fluoroscopy can confirm.
- Aim for peripheral rim contact and solid seating (a change in the pitch of the impaction sound); supplement with screws only if stability is suboptimal.
- Screws POSTEROSUPERIOR only — into the ilium or posterior column. Never place anteroinferior screws: the external iliac vessels lie 15-25 mm anterior to the wall.
- Deliver the proximal femur; open the canal with a box chisel in the piriformis fossa, directing the handle LATERALLY to prevent varus.
- Broach progressively without skipping sizes, each advancing 2-3 mm deeper, until cortical contact and metaphyseal fill are achieved.
- Target 10-15 degrees anteversion to match native femoral version; the broach handle should point toward the patella with the hip extended. Combined anteversion (cup plus stem) should total 25-45 degrees.
- Assemble the trial stem and head (start at a standard neck length) and the trial liner; reduce the hip.
- Test ANTERIOR stability — full extension with 40 degrees external rotation.
- Test POSTERIOR stability — 90 degrees flexion, 40 degrees internal rotation, adduction.
- Assess leg length (overlap the patellae; measure from a fixed pelvic point — aim within 5 mm of the other side) and offset; adjust head size or neck length as needed.
- Uncemented: clean and dry the canal, insert the final stem by hand, then impact to the planned depth, confirming version.
- Cemented (third-generation technique): cement restrictor at the isthmus, pulsatile lavage with 3 L saline, dry the canal, vacuum-mixed cement applied retrograde, pressurise, then insert the stem in 10-15 degrees anteversion for a uniform 2-3 mm mantle.
- Clean and dry the trunnion, impact the modular head, and reduce the hip.
- Repair the capsule and short external rotators to the posterior femur through bone tunnels or soft tissue with heavy absorbable sutures — the single most important step for stability.
- Close the gluteus maximus fascia, then the subcutaneous layer and skin; confirm haemostasis and sciatic nerve integrity.
- Posterior hip precautions for 6 weeks: no flexion beyond 90 degrees, no adduction past midline, no internal rotation.
- Sciatic nerve — 2 cm posterior to piriformis, 20-30 mm behind the capsule; the commonest nerve injured in THA (0.5-2 percent). Limit lengthening to less than 4 cm and use gentle, time-limited retraction.
- Superior gluteal nerve — exits the greater sciatic notch 25-40 mm proximal to the trochanter tip; keep the split within 5 cm of the trochanter. Injury causes an irreversible Trendelenburg gait.
- Femoral nerve and vessels — 40-60 mm anteromedial to the joint in the femoral triangle; keep anterior retractors ON BONE.
- External iliac vessels — 15-25 mm anterior to the anterior wall; threatened by anteroinferior screws and uncontrolled medial reaming. Injury is potentially fatal.
- Medial femoral circumflex artery — deep to quadratus femoris; preserve the muscle where possible to protect femoral-head blood supply.
Multiple studies show that repairing the posterior capsule and short external rotators reduces dislocation roughly 3-4 fold, from 3-5 percent to under 1 percent (Pellicci). Tag every flap and tendon before you cut so the repair is anatomic at closure — the single highest-yield step to name in a viva.
The Lewinnek safe zone (40-45 degrees inclination, 15-20 degrees anteversion) is a guide, not a guarantee. Modern stability thinking uses combined anteversion — cup anteversion plus stem version totalling 25-45 degrees — to give impingement-free range of motion. A 36 mm head adds jump distance over a 28-32 mm head (Howie RCT: 0.8 percent versus 4.4 percent dislocation), balanced against bearing-wear considerations.
Aftercare & Complications
Rehabilitation | Phase | Timing | Milestones & precautions | |-------|--------|--------------------------| | Immediate | Day 0-1 | Multimodal analgesia; VTE prophylaxis (aspirin or a DOAC/LMWH for 28-35 days); sit out of bed and mobilise full weight-bearing as tolerated (uncemented) | | Early | Weeks 1-6 | Posterior precautions (no flexion beyond 90 degrees, no adduction past midline, no internal rotation); wound review at 2 weeks; AP pelvis radiograph | | Recovery | Week 6 to 3 months | Discontinue precautions if the capsule was repaired; driving, walking, swimming; sedentary work | | Return to activity | 3-6 months | Cycling, doubles tennis, golf; avoid running, jumping and contact sports | Long-term surveillance is registry-based: review at 1, 5 and 10 years with an AP pelvis, then periodically for life, and enrol every implant in the national joint registry (NJR, AOANJRR, AJRR, SHAR and others). Complications
- Recognition
- Sudden pain, shortening, abnormal rotation (internal for posterior, external for anterior), unable to bear weight; radiograph shows displaced components
- Prevention
- Lewinnek safe zone, capsular and rotator repair, 36 mm head, combined anteversion, patient education
- Management
- Closed reduction under sedation; confirm concentric reduction on radiograph; CT if recurrent; revision if unstable (adjust version, larger head, constrained liner)
- Recognition
- Early — drainage, erythema, fever; late — pain, loosening, raised CRP/ESR, aspirate positive (WBC greater than 3000, PMN greater than 80 percent)
- Prevention
- Cefazolin 2 g pre-incision, laminar flow, chlorhexidine-alcohol prep, glycaemic control, short operative time, minimise haematoma
- Management
- Early (less than 3 weeks) — DAIR and 6 weeks IV antibiotics; late — two-stage revision with an antibiotic spacer
- Recognition
- Foot drop, posterolateral leg numbness, lost ankle dorsiflexion and eversion
- Prevention
- Limit lengthening to less than 4 cm, gentle time-limited retraction, identify and protect the nerve
- Management
- Reduce limb length, document examination, EMG at 3 weeks for baseline, AFO and neuropathic analgesia; 60-80 percent partial recovery over 12-18 months
- Recognition
- Crack during broaching, abnormal seating, visible fracture line, disproportionate postoperative pain
- Prevention
- Gentle technique, no skipped broach sizes, prophylactic cerclage in osteoporotic or revision bone
- Management
- Undisplaced femoral — cerclage, consider a cemented stem, protected weight-bearing; displaced — ORIF with cables and plate, possible long-stem revision
- Recognition
- Uneven legs, pelvic obliquity, unequal overlapped patellae, more than 1 cm on measurement
- Prevention
- Preoperative templating, intraoperative measurement, restore the centre of rotation
- Management
- Under 1 cm — observe; 1-2 cm — shoe raise; over 2 cm and symptomatic — consider revision; document consent
- Recognition
- DVT — calf swelling and pain, positive Doppler; PE — dyspnoea, tachycardia, hypoxia, CTPA filling defect
- Prevention
- Pharmacological prophylaxis per AAOS/ACCP/NICE (aspirin or a DOAC/LMWH), mechanical compression, early mobilisation
- Management
- Anticoagulate for at least 3 months; massive PE — thrombolysis or embolectomy
- Recognition
- Activity-related and start-up pain, progressive radiolucent lines greater than 2 mm, subsidence, osteolysis
- Prevention
- Optimal fixation, highly cross-linked polyethylene, restored offset and biomechanics
- Management
- Observe if asymptomatic; revise the loose component and address bone loss with grafts, augments or cages
Heterotopic ossification occurs in 10-30 percent of cases and is graded by Brooker:
- Radiographic appearance
- Islands of bone within the soft tissues
- Clinical effect
- None
- Radiographic appearance
- Bone spurs with at least 1 cm gap between opposing surfaces
- Clinical effect
- Usually minimal
- Radiographic appearance
- Bone spurs with less than 1 cm gap between opposing surfaces
- Clinical effect
- Restricted range of motion
- Radiographic appearance
- Ankylosis — an apparent bony bridge
- Clinical effect
- A stiff, painful hip
Viva & Exam Focus
CAPSULECAPSULE — why the posterior soft-tissue repair matters
STABLESTABLE — testing hip stability intra-operatively
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old man has severe right hip osteoarthritis limiting his daily activities. Describe your assessment and management plan for a primary total hip arthroplasty.”
“You are performing a primary THA through a posterior approach. Walk me through the key anatomical structures and danger zones you encounter, from superficial to deep.”
“What is the Lewinnek safe zone and why does it matter? How do you assess and optimise stability intra-operatively?”
Indication & planning
- End-stage hip OA failing conservative care; also secondary OA (DDH, AVN, post-traumatic), inflammatory arthritis, selected fractures
- Calibrated templating — cup size and position, stem, offset, leg length
- Absolute contraindication: active infection
Approach & exposure
- Posterior most common; split gluteus maximus — the true internervous plane (dual innervation)
- Short rotators superior to inferior: piriformis, superior gemellus, obturator internus, inferior gemellus, quadratus femoris
- Tag capsule and rotators before cutting
Cup & stem
- Lewinnek safe zone — 40-45 degrees inclination, 15-20 degrees anteversion
- Screws posterosuperior only; never anteroinferior
- Broach handle lateral to avoid varus; combined anteversion 25-45 degrees
Stability & closure
- STABLE testing — anterior (extension plus 40 degrees external rotation), posterior (90 degrees flexion plus 40 degrees internal rotation plus adduction)
- Capsular repair cuts dislocation from 3-5 percent to under 1 percent
- 36 mm head over 32 mm for jump distance
Complications
- Dislocation, PJI, sciatic palsy, periprosthetic fracture, leg-length discrepancy, VTE, aseptic loosening
- Sciatic 0.5-2 percent — limit lengthening to less than 4 cm
- Quote registry survival — about 95 percent at 10 years, 58 percent at 25 years
Post-op
- VTE prophylaxis 28-35 days, early mobilisation
- Posterior precautions 6 weeks — no flexion beyond 90 degrees, no adduction past midline, no internal rotation
- Enrol every implant in the national registry
Background & Evidence
Pathoanatomy. End-stage hip osteoarthritis is progressive cartilage loss with subchondral sclerosis, cyst formation and marginal osteophytes, culminating in joint-space loss, pain and stiffness. Total hip arthroplasty replaces both the acetabular and femoral articular surfaces with durable bearings, restoring a painless, stable, mobile hip. Fixation and bearing — the global registry picture.
- Dominant practice
- Cementless (about 90 percent of primary cups in AOANJRR and AJRR)
- Regional variation
- Near-universal cementless worldwide
- Dominant practice
- Cementless in younger patients, Australia and North America
- Regional variation
- Cemented and hybrid retain a major role in the UK NJR and Nordic registries, especially over 70-75 years and in osteoporotic bone
- Dominant practice
- Ceramic-on-XLPE and metal-on-XLPE
- Regional variation
- Metal-on-metal abandoned
- Dominant practice
- Virtually eliminates early periprosthetic femoral fracture
- Regional variation
- Cementless preferred where bone quality and demand are high
Implant survival and outcomes. Pooled national-registry data (Evans, Lancet 2019) give construct survival of about 95 percent at 10 years, about 89 percent at 15 years and about 58 percent at 25 years for primary OA — figures to quote from registries rather than case series, which over-estimate survival at around 78 percent at 25 years. Roughly 90-95 percent of patients report significant pain relief and functional improvement. The leading reasons for revision are aseptic loosening, infection and dislocation. Guidelines, registries and global practice. AAOS appropriate-use criteria and NICE TA304 both endorse THA for end-stage hip OA refractory to conservative care. The major registries — NJR (UK), AOANJRR (Australia), AJRR (US), SHAR (Sweden) and the Norwegian and New Zealand registries — are the gold standard for implant surveillance; the AOANJRR (since 1999) and the Nordic registries hold the longest continuous datasets. Every implant should be enrolled in the national registry.
References
Dislocations after total hip-replacement arthroplasties (the Lewinnek safe zone)
Series of 300 total hip replacements; cups within 15 degrees anteversion (plus or minus 10 degrees) and 40 degrees lateral opening (plus or minus 10 degrees) had a 1.5 percent dislocation rate versus 6.1 percent outside the zone.
Posterior approach to total hip replacement using enhanced posterior soft tissue repair
Enhanced capsular and short-external-rotator repair cut dislocation from 4 percent to 0 percent (one surgeon) and from 6.2 percent to 0.8 percent (another) — it changed posterior-approach practice globally.
How long does a hip replacement last? Systematic review and meta-analysis of registry and case-series data
Pooled 25-year construct survival was 77.6 percent from case series but only 57.9 percent from national registries — counsel patients on the registry figure.
Large femoral heads decrease the incidence of dislocation after total hip arthroplasty: a randomised controlled trial
Multicentre RCT of 644 patients: one-year dislocation after primary THA was 0.8 percent with 36 mm heads versus 4.4 percent with 28 mm heads.
Compliant positioning of total hip components for optimal range of motion (combined anteversion)
A mathematical model showing stability depends on the combined cup and stem orientation, not the cup alone — underpins the combined-anteversion concept.
Total hip replacement and resurfacing arthroplasty for end-stage arthritis of the hip (NICE Technology Appraisal TA304)
UK guidance endorsing THA for end-stage hip OA refractory to conservative care, with a cost-effectiveness analysis.