Restoration of wrist, finger and thumb extension in irreparable radial or posterior interosseous nerve palsy · advanced
- Prerequisites before transfer: full passive range of motion at wrist, MCP and IP joints; donor muscle strength MRC grade 4 or greater; an expendable donor with a synergistic action preferred; an intact median and ulnar nerve; and a motivated patient who understands the 6 to 12 month re-education programme.
- Classic set: pronator teres (PT) to extensor carpi radialis brevis (ECRB) for wrist extension; flexor carpi radialis (FCR) to extensor digitorum communis (EDC) for finger extension; palmaris longus (PL) routed to extensor pollicis longus (EPL) for thumb extension. FCU is spared whenever possible to preserve ulnar deviation power and grip.
- Tensioning sequence is critical: set the wrist in 30 to 40 degrees extension when tensioning every transfer; finger MCP joints in full extension with slight IP flexion; thumb in full extension and abduction. Over-tensioning causes an intrinsic-plus posture; under-tensioning fails to correct the drop.
- Re-education begins immediately: the patient practises donor activation (pronation for wrist extension, wrist flexion for finger extension) while the therapist guides the new function; full cortical re-mapping may take 6 to 12 months.
- “Wrist extension is the highest-priority transfer — without it, finger and thumb extension transfers are mechanically ineffective because the tenodesis effect is lost.
- “FCU should be spared when possible; its loss removes the only remaining ulnar deviator and weakens grip. Prefer FCR to EDC when both donors are available and strong.
- “EPL rerouting must pass through a smooth subcutaneous tunnel radial to the radial styloid (or through an enlarged third compartment) — avoid acute angulation that causes attrition rupture.
- “Post-operative splint holds the wrist in 30 to 40 degrees extension, MCP joints in full extension, thumb in extension and abduction for 4 weeks; active donor activation begins at 4 weeks under therapy supervision.
When & Why
Indication. Symptomatic, irreparable radial nerve or posterior interosseous nerve (PIN) palsy with absent wrist, finger and/or thumb extension that has no realistic prospect of recovery — established clinically and electrophysiologically — in a hand with supple joints, strong expendable donors and intact median and ulnar function, in a patient motivated to complete a 6 to 12 month re-education programme. Absolute indications - Irreparable high radial nerve injury (complete transection with a gap greater than 4 cm, or a failed primary repair with no recovery at 12 to 18 months)
- Established PIN palsy with no clinical or EMG recovery after 9 to 12 months and confirmed irreparable damage on exploration
- High radial nerve palsy with absent wrist, finger and thumb extension and supple joints
- Failed nerve grafting or nerve transfer with persistent complete palsy at greater than 18 months Relative indications - Patient preference for earlier reconstruction when nerve recovery is unlikely (for example a very proximal injury with a long gap)
- Combined nerve injuries where median or ulnar function is intact but radial function is permanently lost
- Established drop wrist with secondary contracture risk despite therapy Prerequisites — must all be met before any transfer - Full passive range of motion at the wrist (greater than 40 degrees extension), the MCP joints (full extension) and the thumb CMC and IP joints
- Donor muscle strength MRC grade 4 or greater against resistance
- An expendable donor (PT, FCR and PL preferred; FCU only when FCR is unavailable)
- Intact median and ulnar nerve function (the flexors and intrinsics must power the transfers)
- A motivated patient willing to commit to a prolonged re-education programme (6 to 12 months)
- No active infection or uncontrolled medical comorbidity Contraindications - Absolute: a fixed joint contracture greater than 20 degrees that cannot be corrected pre-operatively; donor muscle strength less than MRC 4; a non-functional hand (absent median or ulnar motor function); a patient unable or unwilling to comply with therapy and re-education.
- Relative: age greater than 70 years with low functional demand (consider tenodesis or arthrodesis instead); a heavy manual worker who cannot tolerate loss of donor strength; active smoking or uncontrolled diabetes (higher infection and adhesion risk). Consent specifically for incomplete correction, over- or under-tensioning, donor morbidity (especially if FCU is harvested), infection (less than 2 percent), adhesions requiring tenolysis (5 to 10 percent) and the need for 6 to 12 months of therapy and re-education. Set-up. Supine, arm abducted 90 degrees on a hand table, forearm in neutral or slight pronation for the volar exposure. An upper-arm tourniquet (250 mmHg) is inflated after exsanguination, and loupe magnification (2.5 to 3.5x) is mandatory — tendon, nerve and vessel identification is the whole game. Regional (axillary or supraclavicular) block or general anaesthesia; WALANT is not suitable because multiple incisions and prolonged dissection are required.
The Operation
The goal is to restore wrist, finger and thumb extension using the classic three-transfer set: pronator teres (PT) to ECRB for wrist extension, FCR to EDC for finger extension, and PL to a rerouted EPL for thumb extension. The donors are exposed through the volar (Henry) approach; the recipients through a longitudinal dorsal approach. The exposure of donors and recipients is laid out in full as the first operative steps below — it is the foundation on which every transfer depends.
Operative sequence
- Supine, hand table, upper-arm tourniquet (250 mmHg), forearm neutral or slight pronation, loupes on.
- Mark three incisions: a Henry incision along the radial border of the forearm from the radial head to the wrist flexion crease; a short transverse or oblique incision at the wrist flexion crease for the FCR and PL tendons; and a longitudinal dorsal incision over the distal forearm and wrist for the recipient tendons and EPL rerouting.
- Incise skin along the Henry line and develop the internervous plane between brachioradialis (radial nerve) and FCR (median nerve).
- Identify and protect the superficial radial nerve and the radial artery — they are the structures most often injured in this approach.
- Expose the PT insertion on the radial border of the radius at the junction of its middle and distal thirds.
- At the wrist crease, confirm the FCR (the larger tendon, radial to the midline, inserting on the second metacarpal base) and the PL (the smaller midline tendon, present in about 85 percent of patients).
- A longitudinal dorsal incision over the distal forearm and wrist exposes ECRB, EDC and EPL. Use the Thompson approach (between ECRB and EDC) or a direct dorsal midline incision.
- Identify the ECRB (deep and central — the preferred wrist recipient because it inserts on the third metacarpal base and gives pure extension), the four EDC tendons, and the EPL in the third extensor compartment.
- Release the EPL from the third compartment and reroute it subcutaneously, radial to the radial styloid, or through an enlarged third compartment, into a smooth tunnel free of constricting retinacular edges.
- Release the PT tendon from its radial insertion with a 2 cm strip of periosteum.
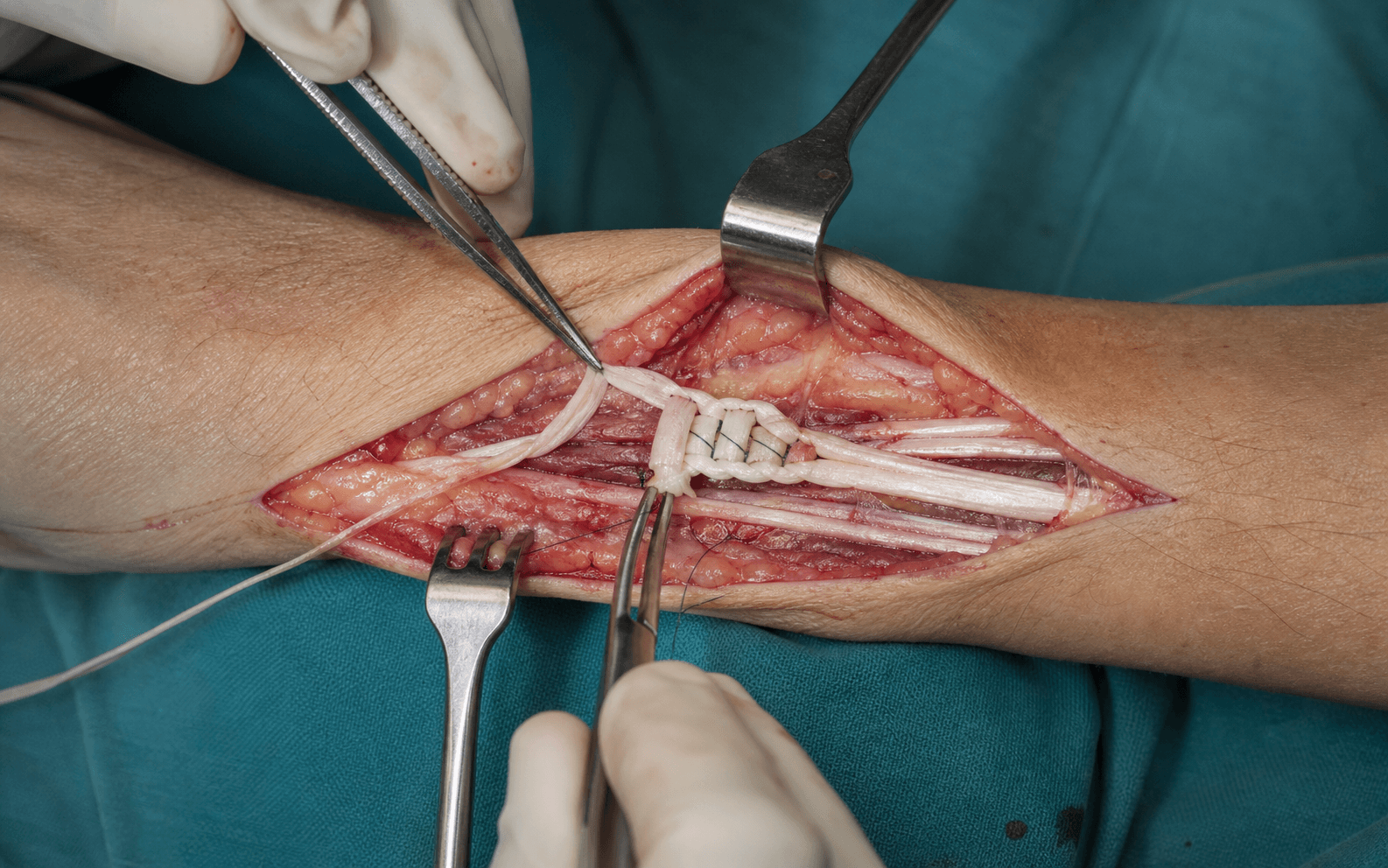
- Weave the PT into the ECRB using a Pulvertaft weave (three passes) with the wrist held in 30 to 40 degrees extension, secured with 3-0 braided permanent suture.
- Set tension so that passive wrist flexion produces strong active wrist extension (tenodesis) — the foundation on which the finger and thumb transfers depend.
- Release the FCR at the wrist crease and pass it subcutaneously (or through a tunnel) to the EDC tendons at the distal forearm.
- Weave the FCR into all four EDC tendons with the Pulvertaft technique, the wrist in 30 degrees extension and the MCP joints in full extension.
- Confirm tension by passive wrist flexion producing full MCP extension of all four fingers, with equal tension across every EDC tendon.
- If FCR is weak or previously injured, harvest FCU instead: release it from the pisiform insertion, pass it subcutaneously to the EDC and weave with identical tensioning (accepting the loss of ulnar deviation).
- Release the PL tendon at the wrist and route the rerouted EPL to lie in a straight line from the PL donor.
- Weave the PL into the EPL with the thumb in full extension and abduction and the wrist in 30 degrees extension.
- Verify tension by passive wrist flexion producing thumb extension via tenodesis, and confirm the rerouted EPL has a smooth line of pull without acute angulation at the tunnel edge.
- Tension in order — wrist first, then fingers, then thumb — never in reverse.
- Throughout, hold the wrist in 30 to 40 degrees extension, the MCP joints in full extension with slight IP flexion, and the thumb in extension and abduction.
- Equalise tension across all four EDC tendons so no finger lags or over-extends.
- Before closing, perform a complete tenodesis test: passive wrist flexion must produce simultaneous wrist, finger MCP and thumb extension. Correct any lag or over-correction before the sutures are tied.
- Close all wounds in layers — absorbable suture for fascia, non-absorbable for skin.
- Apply a bulky dressing and a plaster splint holding the wrist in 30 to 40 degrees extension, MCP joints in full extension, the thumb in extension and abduction, and the IP joints in slight flexion.
- Maintain the splint for 4 weeks.
Before any tendon harvest, identify the radial artery and the superficial radial nerve in the Henry interval and protect them throughout. The artery courses deep to brachioradialis and crosses toward the first web; the nerve runs just deep to the superficial fascia and is easily injured. Stay in the correct internervous plane (brachioradialis versus FCR), use blunt dissection, and never mistake FCR for FCU — FCR lies radial to the midline and inserts on the second metacarpal base, whereas FCU is ulnar and inserts on the pisiform. If the artery is injured, apply direct pressure, call for vascular help and repair primarily where possible.
Always expose PT first through the Henry interval and confirm its strength by asking the patient to pronate against resistance before harvest. Release the PT with a 2 cm periosteal strip for a robust weave, then identify FCR and PL at the wrist crease. FCR is the larger, radial tendon; PL is the smaller midline tendon (confirm its presence pre-operatively — if absent, plan an alternative thumb donor such as an FCR slip).
Set the wrist in 30 to 40 degrees extension when weaving PT into ECRB and verify that passive wrist flexion now produces strong wrist extension before proceeding. If the wrist remains dropped, the transfer is too slack and must be retensioned — every subsequent transfer depends on a working wrist.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | 0 to 4 weeks | Static splint: wrist 30 to 40 degrees extension, MCP full extension, thumb extended and abducted, IP slight flexion | Elevation and oedema control; passive ROM within splint limits; education on donor-activation concepts | | 2 | 4 to 8 weeks | Removable splint for therapy sessions only; continue night splint in extension | Active donor activation begins — pronation drives wrist extension, wrist flexion drives finger and thumb extension — with verbal and tactile cues | | 3 | 2 to 6 months | Night splint only if any tendency to contracture | Progressive resistance, functional task training and cortical re-mapping drills (mirror therapy, mental imagery, repetitive donor activation) | | 4 | 6 to 12 months | None | Fine tuning; unrestricted use by 3 to 6 months in most patients; return to heavy manual work after 6 months if grip is adequate | Most patients achieve MRC 4 wrist extension and useful finger and thumb extension. PT to ECRB restores wrist extension to MRC 4 in greater than 85 percent; FCR to EDC restores finger MCP extension to MRC 3 to 4 in 80 to 90 percent; PL to a rerouted EPL restores thumb extension and abduction in 75 to 85 percent. Implants and fixation. No implants are required for the transfers themselves. Pulvertaft weaves use 3-0 or 4-0 braided permanent suture (Ethibond or equivalent); skin closure uses 4-0 or 5-0 absorbable suture. Bone-tendon fixation with small anchors or interference screws is only needed when a tendon weave is not possible. Complications
- Timing
- Early (less than 6 weeks)
- Recognition
- Erythema, discharge or wound dehiscence
- Prevention
- Meticulous technique and peri-operative antibiotics
- Management
- Oral antibiotics and wound care; surgical washout if deep
- Timing
- Early
- Recognition
- Swelling, skin tension, pain
- Prevention
- Meticulous haemostasis before closure
- Management
- Evacuate if causing skin tension or compartment pressure
- Timing
- Early
- Recognition
- Skin breakdown over bony prominences
- Prevention
- Pad all prominences; check skin at 48 hours and weekly
- Management
- Pressure relief, dressing care and splint modification
- Timing
- Intermediate (6 weeks to 6 months)
- Recognition
- Tendon fails to glide; poor active extension despite therapy
- Prevention
- Gentle handling and early controlled motion
- Management
- Tenolysis if no improvement after 3 months of therapy
- Timing
- Intermediate
- Recognition
- Wrist greater than 50 degrees extension, MCP hyperextension, IP flexion
- Prevention
- Tension with wrist at 30 to 40 degrees extension; verify tenodesis before knotting
- Management
- Early splint adjustment; established deformity needs release or revision transfer
- Timing
- Intermediate
- Recognition
- Wrist remains dropped and MCP extension lags despite donor activation
- Prevention
- Tension with the wrist extended; tenodesis test before knotting
- Management
- Revision tensioning or an additional transfer after 6 months
- Timing
- Late (6 to 18 months)
- Recognition
- Sudden loss of thumb extension after initial recovery
- Prevention
- Create a smooth subcutaneous tunnel with no acute angulation
- Management
- Revision with a new donor or a tendon graft
- Timing
- Late
- Recognition
- Loss of ulnar deviation, weak grip, radial-deviation posture
- Prevention
- Spare FCU and use FCR whenever it is available and strong
- Management
- Therapy and counselling regarding the permanent deficit
- Timing
- Late
- Recognition
- Poor activation despite a structurally successful transfer
- Prevention
- Select motivated patients; run an intensive re-education programme
- Management
- Prolonged therapy; accept limited function or consider revision
Viva & Exam Focus
RADIALRADIAL — prerequisites and planning
TRANSFERTRANSFER — the classic set and tensioning
The trap: transferring a donor graded MRC 3 or less — it will never generate enough force to overcome gravity or provide useful function. A transferred muscle typically loses one MRC grade, so an MRC 4 becomes MRC 3. Document donor strength pre-operatively; if only MRC 3, strengthen first or select another donor.
The trap: a wrist flexion contracture greater than 20 degrees, MCP hyperextension contracture or thumb adduction contracture renders the transfer ineffective. Transfer into a stiff joint produces no functional gain and risks rupture or elongation. Correct every fixed deformity with therapy, serial casting or preliminary surgery first.
The trap: FCU is the primary ulnar deviator and a major wrist flexor; its harvest removes the only remaining ulnar deviator in radial palsy, weakening grip and producing a radial-deviation posture. Prefer FCR to EDC; reserve FCU for cases where FCR is weak or previously injured.
The trap: wrist held in greater than 50 degrees extension with MCP hyperextension and IP flexion destroys the tenodesis effect and creates a non-functional hand. Tension with the wrist at 30 to 40 degrees extension and the MCP joints in neutral to slight flexion; verify with the tenodesis test before securing sutures.
The trap: the wrist stays dropped and the fingers fail to extend because the transfer is too slack — the most common technical error leading to revision. Set tension tight enough that passive wrist flexion produces full finger MCP extension via tenodesis, with the wrist in 30 degrees extension and the fingers fully extended.
The trap: an EPL rerouted around the radial styloid or through a tight pulley frays and ruptures late (6 to 18 months) at the point of angulation. Create a smooth subcutaneous tunnel, release any constricting fascia and never pass the tendon through a retinacular pulley without adequate enlargement.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old carpenter sustained a high radial nerve transection in a chainsaw injury 18 months ago. Primary repair was not possible due to a 5 cm gap. He has no clinical or EMG recovery, full passive range of motion and strong median and ulnar function. How do you plan his reconstruction?”
“During a tendon transfer for radial nerve palsy you have completed the PT to ECRB and FCR to EDC weaves. You are about to tension the PL to EPL transfer when the assistant asks how you will decide the correct tension. Describe your method.”
“A 42-year-old patient 9 months after high radial nerve grafting has no clinical recovery and weak (MRC 3) PT and FCR on testing. EMG shows no reinnervation. The joints are supple. What is your recommendation?”
Indications & prerequisites
- Irreparable radial or PIN palsy with no recovery at 12 to 18 months and supple joints
- Donor strength MRC 4 or greater — MRC 3 donors fail after transfer
- Full passive ROM: wrist greater than 40 degrees extension, full MCP and thumb motion
- Intact median and ulnar function to power the transfers
- A motivated patient willing to commit to 6 to 12 months of re-education
Classic transfer set
- PT to ECRB restores wrist extension — the foundation, do first
- FCR to EDC restores finger MCP extension (spares FCU and ulnar deviation)
- PL to a rerouted EPL restores thumb extension and abduction
- FCU to EDC is the alternative when FCR is unavailable — sacrifices ulnar deviation and grip
- Tensioning: wrist 30 to 40 degrees extension, MCP full extension, thumb extension and abduction
Tensioning principles
- Tension with the wrist in 30 to 40 degrees extension for every transfer
- Tenodesis test: passive wrist flexion must produce full extension of the transferred joints
- Equal tension across all four EDC tendons prevents differential lag
- The EPL tunnel must be smooth and free of acute angulation to prevent attrition rupture
- Over-tensioning gives an intrinsic-plus posture; under-tensioning leaves a persistent drop
Surgical approaches
- Henry approach exposes the PT insertion and the FCR/PL tendons (volar radial forearm)
- Thompson or dorsal midline exposes ECRB, EDC and EPL (dorsal forearm)
- EPL rerouting: subcutaneous tunnel radial to the styloid, or an enlarged third compartment
- Protect the superficial radial nerve and radial artery during the Henry approach
- Loupe magnification (2.5 to 3.5x) is mandatory for all tendon identification and weaving
Post-operative protocol
- Static splint for 4 weeks: wrist 30 to 40 degrees extension, MCP full extension, thumb extended and abducted
- Weeks 4 to 8: removable splint for therapy; begin active donor activation
- Months 2 to 6: progressive strengthening and functional task training
- Months 6 to 12: unrestricted use; cortical re-mapping continues up to 12 months
- Continue a night splint if any tendency to contracture
Complications
- Over-tensioning: intrinsic-plus posture (wrist greater than 50 degrees extension, MCP hyperextension)
- Under-tensioning: persistent drop wrist and finger lag
- Attrition rupture of the EPL: late (6 to 18 months) at the tunnel edge — prevent with a smooth tunnel
- Donor morbidity (FCU harvest): permanent loss of ulnar deviation and grip strength
- Adhesions: tenolysis if no improvement after 3 months of therapy
Special situations
- PIN palsy: wrist extension preserved (ECRL intact) but radially deviated — may still benefit from PT to ECRB to centralise extension
- Combined nerve injury: staged reconstruction or alternative donors; set realistic goals
- MRC 3 donor: absolute contraindication — consider arthrodesis or an orthosis instead
- Elderly or non-compliant patient: lower re-education success — consider tenodesis or arthrodesis
- Heavy manual worker: counsel regarding grip weakness if FCU must be harvested
Background & Evidence
Palsy patterns drive the plan. The transfer set is chosen according to which muscles the lesion has taken.
- Level of lesion
- Above the spiral groove
- Findings
- Loss of all radial-innervated muscles including triceps, brachioradialis, ECRL, ECRB, supinator and all finger and thumb extensors
- Transfers required
- Full set: PT to ECRB, FCR to EDC, PL to EPL
- Level of lesion
- After the branch to ECRB
- Findings
- ECRL intact so wrist extension is preserved but weak and radially deviated; finger and thumb extension lost
- Transfers required
- Finger and thumb transfers; add PT to ECRB only if wrist extension needs centralising
Donor muscles — anatomy and expendability - Pronator teres (PT): origin from the medial epicondyle and coronoid process; inserts on the radial shaft. Expendable because pronator quadratus also pronates. Strong (MRC 5) and synergistic with wrist extension via tenodesis.
- Flexor carpi radialis (FCR): origin from the medial epicondyle; inserts on the base of the second metacarpal. Expendable because FCU and PL provide wrist flexion. A strong donor with easy re-education (synergistic with finger extension via tenodesis).
- Flexor carpi ulnaris (FCU): origin from the medial epicondyle and ulna; inserts on the pisiform and fifth metacarpal base. Powerful but not expendable without consequence — its loss removes the only ulnar deviator and weakens grip.
- Palmaris longus (PL): present in about 85 percent of people; origin from the medial epicondyle; inserts on the palmar fascia. Completely expendable; weak but adequate for thumb extension after rerouting. Recipient tendons — anatomy and insertion - ECRB: the preferred wrist recipient because it inserts centrally on the third metacarpal base and produces pure extension without radial deviation.
- EDC: four tendons to the index through little fingers, inserting into the extensor hood at MCP level; all four must be tensioned equally to avoid differential extension.
- EPL: inserts on the distal phalanx of the thumb; it must be released from the third compartment and rerouted to avoid acute angulation after transfer. Critical landmarks. The PT insertion is on the radial border of the radius at the junction of the middle and distal thirds. The FCR is palpated radial to the FCU at the wrist flexion crease, with the median nerve lying deep and ulnar to it. The EPL is released from the third extensor compartment at the wrist and rerouted subcutaneously or through an enlarged third compartment. The dorsal sensory branch of the radial nerve crosses the radial styloid subcutaneously and must be protected during the dorsal incisions. Donor choice for finger extension — the evidence summary
- Strength
- Good (MRC 4)
- Ulnar deviation preserved
- Yes
- Re-education ease
- Moderate — synergistic with wrist flexion
- Common complications
- Radial-deviation weakness if FCR is weak pre-operatively
- Strength
- Excellent (MRC 4+)
- Ulnar deviation preserved
- No
- Re-education ease
- Easy — a strong donor
- Common complications
- Loss of ulnar deviation and grip power
- Strength
- Good
- Ulnar deviation preserved
- Yes
- Re-education ease
- Difficult — non-synergistic
- Common complications
- Donor morbidity and swan-neck risk
- Strength
- Moderate
- Ulnar deviation preserved
- Yes
- Re-education ease
- Difficult
- Common complications
- Weak donor and radial-deviation loss
Timing of nerve exploration versus early transfer. Exploration and repair or grafting within 3 to 6 months of injury remains standard when the nerve is in continuity or a clean transection is present. When the nerve is irreparable (large gap, crushed, or a failed prior repair) and there is no recovery by 12 months, tendon transfer is the reconstructive option of choice. EMG evidence of reinnervation without clinical recovery by 12 to 15 months may justify observation up to 18 months, but most surgeons proceed to transfer once the window for useful nerve recovery has closed. Classic transfer outcomes. PT to ECRB reliably restores wrist extension to MRC 4 in greater than 85 percent of patients. FCR to EDC restores finger MCP extension to MRC 3 to 4 in 80 to 90 percent; FCU to EDC produces slightly stronger extension but sacrifices ulnar deviation. PL to a rerouted EPL restores thumb extension and abduction in 75 to 85 percent, whether the reroute runs through the third compartment or a subcutaneous tunnel, provided tension is correct. Special case — PIN palsy (wrist extension preserved). When ECRL is intact, wrist extension is present but radially deviated. PT to ECRB may still be performed to centralise extension and increase power; the finger and thumb transfers proceed identically. Some surgeons omit the wrist transfer if the patient has functional wrist extension and good grip. Special case — combined nerve injuries. Radial plus median or ulnar palsy requires staged reconstruction or alternative donors (for example brachioradialis or ECRL if available). Functional goals must be realistic — a hand with multiple nerve deficits may be better served by arthrodesis or tenodesis than by multiple transfers.
References
Results of Tendon Transfers in Radial Nerve Palsies: A New Evaluation Protocol
- Prospective study of tendon transfer outcomes in radial nerve palsy using a structured evaluation protocol
Nerve Transfer Versus Tendon Transfer for Isolated Radial Nerve Palsy
- Comparative analysis of nerve transfer and tendon transfer approaches for isolated radial nerve palsy
In-silico biomechanical simulation of tendon transfers for finger extension in radial nerve palsy
- Biomechanical modelling confirms optimal tensioning parameters for finger extension transfers in radial palsy
Results of Tendon Transfers for Radial Nerve Palsy: Systematic Review and Meta-analysis
- Review of outcomes following tendon transfers for radial nerve palsy demonstrating high rates of functional recovery