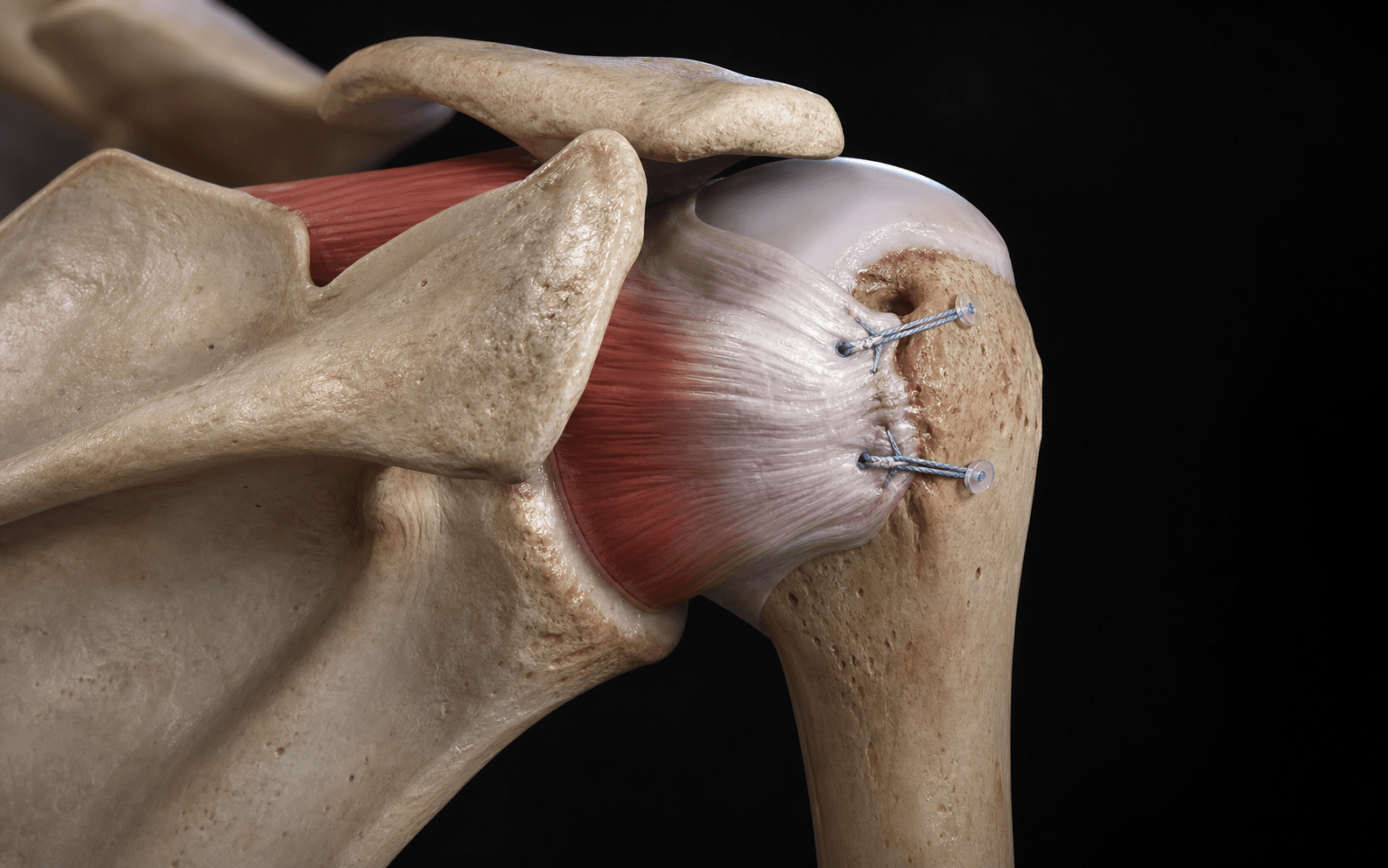
Arthroscopic posterior capsulodesis and infraspinatus tenodesis that converts an off-track engaging Hill-Sachs lesion to an extra-articular position
- Glenoid track concept (Di Giacomo, Itoi): the glenoid track is the zone of contact between the glenoid and humeral head during abduction-external rotation. A Hill-Sachs lesion is off-track (engaging) when its medial margin lies medial to the glenoid track margin — remplissage converts it to extra-articular.
- Decision threshold: remplissage plus Bankart is indicated when glenoid bone loss is less than 15–20 percent and there is an off-track engaging Hill-Sachs lesion. When glenoid bone loss exceeds 15–20 percent or there is bipolar bone loss with an off-track lesion, Latarjet or other bony augmentation is preferred over isolated remplissage.
- Technique converts the defect: two to three double-loaded anchors placed in the base of the Hill-Sachs defect; sutures passed through the posterior capsule and infraspinatus tendon to tenodese the tendon into the defect, thereby filling the lesion and shifting the capsule medially.
- Typical loss of external rotation after remplissage is 5–10 degrees; patients must be counselled pre-operatively that some limitation of terminal external rotation is expected and usually well tolerated in non-overhead athletes.
When & Why
Indication. Anterior shoulder instability with an off-track (engaging) Hill-Sachs lesion confirmed on dynamic arthroscopic assessment, with glenoid bone loss less than 15–20 percent on 3D CT, that has failed non-operative management or recurred after a Bankart repair performed without significant glenoid bone loss. It is the arthroscopic soft-tissue answer to a humeral-sided bone defect when the glenoid is intact enough for soft-tissue work. Absolute indications - Anterior instability with an off-track (engaging) Hill-Sachs lesion on dynamic arthroscopic assessment.
- Glenoid bone loss less than 15–20 percent confirmed on 3D CT.
- Recurrent dislocations or subluxations despite appropriate non-operative management, or after a failed Bankart repair without significant glenoid bone loss.
- Patient preference for an arthroscopic soft-tissue procedure over open bony augmentation when glenoid bone loss is minimal. Relative indications - On-track Hill-Sachs lesion that becomes engaging after a Bankart repair (a rare intra-operative finding).
- Contact or collision athlete with minimal glenoid bone loss who wishes to avoid Latarjet hardware.
- Revision surgery after failed soft-tissue stabilisation where glenoid bone loss remains below threshold. Contraindications. Absolute: glenoid bone loss greater than 15–20 percent (Latarjet or other bony augmentation required); bipolar bone loss with an off-track lesion; glenoid bone loss of any magnitude with an inverted-pear glenoid morphology; active infection or uncontrolled medical comorbidity. Relative: an overhead throwing athlete in whom even 5–10 degrees of external rotation loss would be career-limiting; significant glenoid dysplasia or version abnormality requiring bony correction; patient inability to comply with the rehabilitation protocol. The one decision that matters. Remplissage addresses the humeral defect; it does nothing for the glenoid. So the whole operation turns on the bone-loss balance between the two sides of the joint:
- Remplissage + Bankart
- Less than 15–20 percent
- Latarjet
- Greater than 15–20 percent or bipolar
- Remplissage + Bankart
- Off-track engaging
- Latarjet
- Off-track engaging
- Remplissage + Bankart
- 5–10 percent
- Latarjet
- 2–8 percent
- Remplissage + Bankart
- 5–10 degrees
- Latarjet
- 5–15 degrees (variable)
- Remplissage + Bankart
- Anchor pull-out, posterior pain, stiffness
- Latarjet
- Coracoid non-union, hardware prominence, nerve injury
- Remplissage + Bankart
- Latarjet remains available
- Latarjet
- More complex (Eden-Hybinette, distal tibia)
- Remplissage + Bankart
- Non-overhead athlete, minimal glenoid loss
- Latarjet
- High-demand contact athlete, significant bone loss
Consent specifically for recurrence (5–10 percent), loss of external rotation (5–10 degrees), posterior shoulder pain, anchor pull-out, axillary nerve injury, stiffness, and the possibility of conversion to an open Latarjet if unexpected glenoid bone loss is encountered intra-operatively. Setup. Beach-chair position, head secured neutral, operative arm in a pneumatic arm holder (Spider or similar) so it can be moved freely through the full arc for the dynamic engagement test. General anaesthesia with an interscalene block for post-operative analgesia; hypotensive anaesthesia (systolic 90–100 mmHg) improves visualisation.
The Operation
The goal: confirm an off-track engaging lesion dynamically, restore the anterior labral bumper with a Bankart repair, then fill the Hill-Sachs defect by tenodesing the infraspinatus and posterior capsule into it so the lesion is converted from an intra-articular engaging defect to an extra-articular non-engaging one. The exposure is entirely arthroscopic — the portals and the dynamic engagement test are the whole game, and they are laid out as the first steps below.
Arthroscopic remplissage + Bankart repair
- Portals. Standard posterior viewing portal (2 cm inferior and 2 cm medial to the posterolateral acromion corner), an anterosuperior working portal (just anterior to the biceps tendon in the rotator interval), and an anteroinferior portal (immediately superior to the subscapularis tendon). An accessory posterolateral portal is usually needed for anchor placement in the Hill-Sachs defect.
- Equipment. 30-degree and 70-degree arthroscopes, 5.0 mm cannulas, double-loaded 3.0 mm or 4.5 mm suture anchors (bioabsorbable or PEEK), knotless or knotted fixation, arthroscopic suture passers and graspers, radiofrequency ablation device, 4.5 mm shaver and burr.
- The shoulder is prepared and draped to allow full access to both the posterior and anterior aspects, because the arm must rotate freely for the engagement test.
- Perform a complete diagnostic arthroscopy through the posterior portal. Document the size and location of the Hill-Sachs lesion, the presence and extent of glenoid bone loss, the status of the anterior labrum, and any associated pathology (biceps, rotator cuff, cartilage).
- Perform the dynamic engagement test: position the arm in 90 degrees of abduction and progressive external rotation while viewing from the posterior portal. If the medial margin of the Hill-Sachs lesion rides over the anterior glenoid rim, the lesion is off-track (engaging) and remplissage is indicated.
- Switch the viewing portal to the anterosuperior portal to visualise the anterior glenoid rim. Debride the anterior labrum and glenoid neck with a shaver and radiofrequency device.
- Place two or three double-loaded suture anchors on the glenoid face at the 3, 4 and 5 o'clock positions (right shoulder) or equivalent, down to the 5 o'clock position.
- Pass the sutures through the labrum and capsule with a suture passer and tie the knots, restoring the anterior labral bumper and capsular tension. Completing the Bankart first improves visualisation of the glenoid track and humeral head position.
- Return the viewing portal to the posterior portal and identify the Hill-Sachs lesion.
- Use a shaver or burr to debride fibrous tissue and loose cartilage from the base of the defect until bleeding cancellous bone is exposed — this is what the tenodesed infraspinatus will heal against.
- Avoid over-aggressive burring, which removes excessive bone stock and weakens the humeral head.
- Place two or three double-loaded suture anchors into the base of the Hill-Sachs defect, in a medial-to-lateral or superior-to-inferior configuration depending on defect geometry.
- Confirm each anchor is fully seated with cortical purchase before passing sutures — shallow placement is the cause of later pull-out.
- Using an arthroscopic suture passer or penetrating device, pass one limb of each anchor suture through the posterior capsule and infraspinatus tendon approximately 1 cm lateral to the defect margin.
- Capture a substantial tissue bridge at least 8–10 mm thick that will tenodese the infraspinatus into the defect when the sutures are tied. Pass in a mattress or simple configuration depending on tissue quality.
- Tie the sutures with a sliding knot plus multiple half-hitches, or use a knotless device. As the sutures tension, the infraspinatus is drawn into the Hill-Sachs defect, filling it, and the posterior capsule shifts medially, reinforcing the repair.
- Reassess the dynamic engagement test. The previously engaging lesion should no longer contact the anterior glenoid rim during abduction-external rotation — the lesion is now extra-articular.
- Confirm haemostasis, close the portals with absorbable sutures, and apply a sterile dressing.
- Place the arm in a sling with an abduction pillow, external rotation limited to neutral.
The axillary nerve and posterior humeral circumflex artery lie inferior and medial to the typical remplissage portal sites. Keep every inferior anchor at least 2 cm superior to the inferior margin of the defect and use blunt dissection. Axillary nerve injury is reported in less than 1 percent of cases but is avoidable with this margin.
With the arm in 90 degrees of abduction and full external rotation, watch whether the medial margin of the Hill-Sachs lesion rides over the anterior glenoid rim. If it does not engage, do not perform remplissage even if the lesion appears large on imaging — an on-track lesion does not require filling.
Use a 90-degree suture passer to take a bite of both capsule and tendon at least 8–10 mm thick. When the sutures are tied, the infraspinatus should visibly fill the defect and the posterior capsule should shift medially, converting the intra-articular defect to an extra-articular position.
Remplissage addresses humeral-sided bone loss by rendering the defect extra-articular; it does not restore glenoid bone stock. It therefore fails when glenoid bone loss is underestimated or left untreated — the single most important concept on this topic.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Motion & therapy | |-------|--------|----------------|------------------| | 1 — Protection | 0–6 weeks | Sling with abduction pillow (removed only for hygiene and pendulum exercises) | Passive forward flexion/abduction to 90 degrees; external rotation limited to neutral; no active external rotation, no forced passive external rotation, no cross-body adduction, no lifting | | 2 — Motion recovery | 6–12 weeks | Sling discontinued at 6 weeks if healing confirmed | Full passive and active-assisted forward flexion/abduction by week 10; external rotation to 30–45 degrees by week 12; light rotator-cuff and periscapular theraband from week 8–10 | | 3 — Strengthening & function | 12–24 weeks | None | Progressive resistance for rotator cuff, deltoid and scapular stabilisers; closed-chain and proprioceptive work; sport-specific drills from week 16 | | Return to sport | ~6 months | None | Full pain-free range of motion, greater than 90 percent strength symmetry, sport-specific testing passed; contact sport typically cleared at 6 months | Long-term considerations. Document the external rotation deficit at 6 months — most patients adapt; a persistent symptomatic deficit greater than 15 degrees may warrant tenodesis release (rare). Return to overhead sport is individualised; many non-elite athletes return successfully, but elite throwers may need a modified technique. Radiographs at 6 months and 1 year assess anchor position and joint health.
Post-operative rehabilitation must protect the infraspinatus tenodesis for the first 6 weeks. Limit active external rotation and avoid forced passive external rotation beyond neutral in the early phase — loading the tenodesis before it heals is how the repair fails early.
Complications
- Incidence
- 5–10 percent (higher if glenoid bone loss underestimated)
- Recognition
- Recurrent dislocation or subluxation, positive apprehension, patient-reported instability
- Prevention & management
- Quantify glenoid bone loss pre-operatively on 3D CT; perform the dynamic engagement test; do not do isolated remplissage when bone loss exceeds 15–20 percent. Manage with revision to Latarjet or other bony augmentation, addressing residual bone loss
- Incidence
- 5–10 degrees expected; greater than 15 degrees uncommon
- Recognition
- Reduced active and passive external rotation versus the other side; difficulty with overhead or throwing activities
- Prevention & management
- Counsel pre-operatively; avoid overtensioning the tenodesis. Manage with capsular-stretching physiotherapy; most adapt; rarely, release of the tenodesis
- Incidence
- 10–15 percent, usually transient
- Recognition
- Aching posterior shoulder pain, worse with resisted external rotation or cross-body adduction
- Prevention & management
- Avoid overtensioning; ensure a smooth filled contour. Activity modification, NSAIDs, physiotherapy; most resolve by 6 months; persistent pain may need diagnostic injection or revision
- Incidence
- Less than 2 percent
- Recognition
- Sudden loss of stability, palpable or audible pop, radiographic anchor displacement
- Prevention & management
- Confirm bone quality and full anchor seating; use appropriate anchor size and material. Revision with larger anchors or alternative fixation
- Incidence
- Less than 1 percent
- Recognition
- Deltoid weakness, sensory loss over the lateral shoulder, positive EMG
- Prevention & management
- Keep portal trajectory at least 2 cm superior to the inferior defect margin; blunt dissection. Observe for neuropraxia; explore and repair if no recovery by 3 months
- Incidence
- 5–8 percent
- Recognition
- Progressive loss of motion, pain with all movements, global restriction
- Prevention & management
- Early supervised physiotherapy; avoid immobilisation beyond 4 weeks. Aggressive physiotherapy; consider manipulation under anaesthesia or arthroscopic capsular release if refractory at 6 months
- Incidence
- Less than 0.5 percent
- Recognition
- Erythema, warmth, effusion, raised CRP and ESR, positive joint aspiration culture
- Prevention & management
- Sterile technique, prophylactic antibiotics. Urgent arthroscopic washout, IV antibiotics for 4–6 weeks, culture-directed therapy
Viva & Exam Focus
TRACKTRACK — glenoid track concept and decision making
HILL-SACHSHILL-SACHS — operative decision framework
The trap: treating every Hill-Sachs lesion with remplissage without calculating the glenoid track — many are on-track, do not engage, and remplissage only causes unnecessary external rotation loss. The fix: use the Di Giacomo formula. If the medial margin of the Hill-Sachs lies medial to the glenoid track margin, the lesion is off-track (engaging) and remplissage is indicated when glenoid bone loss stays less than 15–20 percent.
Why it fails: when glenoid bone loss exceeds 15–20 percent the glenoid track is narrowed enough that even a filled lesion may still engage, and overall bony stability is compromised. The numbers: isolated remplissage with greater than 15–20 percent glenoid bone loss carries recurrence of 20–40 percent. Measure bone loss on 3D CT; if it exceeds the threshold or is bipolar, proceed to Latarjet.
The trap: static imaging alone overestimates engagement. An on-track lesion may look large but never engages because the glenoid track covers it through the arc of motion. The fix: perform dynamic arthroscopic assessment in the beach-chair position with the arm in 90 degrees abduction and full external rotation, and visualise whether the lesion engages the anterior glenoid rim. Only off-track engaging lesions need remplissage.
The combination: significant glenoid bone loss (greater than 15 percent) plus an engaging Hill-Sachs is bipolar bone loss — the combined defects narrow the glenoid track dramatically. The implication: remplissage addresses only the humeral defect. When glenoid loss is substantial the track stays too narrow and recurrence is high. Latarjet or other glenoid bony augmentation is required; remplissage may be an adjunct but is not the primary solution.
Why it happens: tenodesing the infraspinatus into the defect shifts the posterior capsule and tendon medially, reducing the external rotation arc by roughly 5–10 degrees. The implication: overhead athletes and throwers notice the deficit most. Document pre-operative external rotation, and counsel that the deficit is usually well tolerated for daily living and non-overhead sport but may affect elite overhead performance — those patients may need an alternative procedure.
The pattern: the most common cause of failure after remplissage is underestimation of glenoid bone loss — the procedure does not restore glenoid bone stock. The fix: if recurrence occurs, obtain repeat 3D CT. Many apparent remplissage failures are actually cases where bone loss exceeded 15–20 percent and Latarjet should have been done. Failed remplissage with substantial bone loss needs revision to a bony procedure; repeat soft-tissue surgery has low success.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old rugby player has recurrent anterior shoulder dislocations. 3D CT shows 12 percent glenoid bone loss and a large Hill-Sachs lesion whose medial margin lies 4 mm medial to the calculated glenoid track margin. Describe your surgical plan and the reasoning behind your choice of procedure.”
“A 22-year-old student underwent arthroscopic Bankart repair with remplissage 18 months ago for an off-track Hill-Sachs lesion with 10 percent glenoid bone loss. She now presents with recurrent instability after a new traumatic dislocation during a fall. CT shows the previous anchors in position and glenoid bone loss still measuring 10 percent. How do you manage this patient?”
“A 35-year-old recreational tennis player is 6 months post remplissage and Bankart repair. He has full forward flexion and abduction but lacks the final 15 degrees of external rotation compared with his other shoulder. He reports difficulty serving and is concerned about his return to competitive play. How do you counsel and manage him?”
Glenoid track concept
- Glenoid track width = 0.83 times glenoid diameter minus glenoid bone loss width (Di Giacomo formula)
- Off-track (engaging): the Hill-Sachs medial margin lies medial to the glenoid track margin
- On-track: the medial margin lies lateral to or at the track margin and does not engage
- Dynamic engagement test in 90 degrees abduction and full external rotation confirms engagement intra-operatively
- Remplissage converts an off-track lesion to extra-articular by infraspinatus tenodesis and posterior capsulodesis
Indications and thresholds
- Remplissage plus Bankart: off-track engaging Hill-Sachs with glenoid bone loss less than 15–20 percent
- Latarjet indicated: glenoid bone loss greater than 15–20 percent, or bipolar bone loss with an off-track lesion
- Inverted-pear glenoid morphology: absolute contraindication to isolated remplissage
- Overhead athlete: counsel regarding 5–10 degree external rotation loss; may prefer an alternative procedure
- Failed previous soft-tissue stabilisation with minimal bone loss: revision remplissage or Latarjet
Surgical anatomy
- Hill-Sachs lesion: a postero-superolateral humeral head impression fracture from anterior dislocation
- Infraspinatus tendon: tenodesed into the defect to fill it and shift the posterior capsule medially
- Axillary nerve: at risk with inferior anchor placement — maintain a 2 cm safety margin
- The glenoid track narrows as glenoid bone loss increases — explaining why remplissage fails above 15–20 percent
- Bipolar bone loss: combined glenoid and humeral defects require bony glenoid augmentation (Latarjet)
Operative technique — key steps
- 1. Beach-chair position, diagnostic arthroscopy, dynamic engagement test in 90 degrees abduction-external rotation
- 2. Complete the Bankart repair first (three anchors at 3, 4 and 5 o'clock) to restore the anterior labral bumper
- 3. Debride the Hill-Sachs base to bleeding bone; place two to three double-loaded anchors in the defect base
- 4. Pass sutures through the posterior capsule and infraspinatus 1 cm lateral to the defect margin
- 5. Tie sutures to tenodese the infraspinatus into the defect; confirm the lesion no longer engages on dynamic testing
- 6. Protect the tenodesis with a sling and external rotation limited to neutral for 6 weeks
Danger zones
- Glenoid bone loss greater than 15–20 percent: remplissage alone has 20–40 percent recurrence — perform Latarjet
- Inferior anchor placement: axillary nerve injury risk — stay 2 cm superior to the inferior defect margin
- Overtensioned tenodesis: external rotation loss greater than 15 degrees — counsel and avoid
- Underestimated glenoid bone loss: the most common cause of failure — always quantify on 3D CT pre-operatively
- Bipolar bone loss: isolated remplissage fails — requires bony glenoid restoration
Complications
- Recurrence: 5–10 percent (higher if glenoid bone loss underestimated); revision to Latarjet
- External rotation loss: 5–10 degrees expected; greater than 15 degrees uncommon but functionally significant in overhead athletes
- Posterior pain: 10–15 percent, usually transient; activity modification and physiotherapy
- Anchor pull-out: less than 2 percent; revision with larger anchors or alternative fixation
- Axillary nerve injury: less than 1 percent; observe for neuropraxia, explore if no recovery at 3 months
Rehabilitation milestones
- Weeks 0–6: sling with abduction pillow, external rotation limited to neutral, passive motion to 90 degrees flexion/abduction
- Weeks 6–12: discontinue sling, progress to full active motion except forced external rotation, begin light strengthening
- Weeks 12–24: progressive resistance, functional and sport-specific training, return to sport at 6 months if criteria met
- External rotation deficit: document at 6 months; most adapt; symptomatic greater than 15 degrees may require release
- Contact sport clearance: 6 months, full pain-free motion, greater than 90 percent strength symmetry, sport-specific testing passed
Evidence thresholds
- Recurrence after remplissage plus Bankart: 5–10 percent when glenoid bone loss is less than 15 percent and the lesion is off-track
- External rotation loss: mean 5–10 degrees across series; well tolerated in non-overhead athletes
- Failure when glenoid bone loss is greater than 15–20 percent: recurrence rises to 20–40 percent — Latarjet indicated
- Long-term arthritis risk: low when remplissage is performed for correct indications; no significant progression at 5 years
- Revision after failed remplissage: address residual bone loss; Latarjet remains available and effective
Background & Evidence
Glenoid track concept (Di Giacomo, Itoi). The glenoid track is the zone of contact between the glenoid articular surface and the humeral head during abduction-external rotation. Its width equals 0.83 times the glenoid diameter minus the width of any glenoid bone loss. As glenoid bone loss increases, the medial margin of the track moves medially and the safe zone of humeral head contact shrinks. A Hill-Sachs lesion is on-track (non-engaging) when its medial margin lies lateral to or at the medial margin of the glenoid track, and off-track (engaging) when its medial margin lies medial to the track margin. Multiple validation studies confirm that off-track lesions have significantly higher recurrence after isolated Bankart repair than on-track lesions.
Glenoid track width = 0.83 times the glenoid diameter minus the width of glenoid bone loss. An off-track lesion engages because its medial margin lies medial to this calculated track margin — the single calculation the examiner is looking for.
Hill-Sachs lesion. An impression fracture of the postero-superolateral humeral head caused by impaction against the anterior glenoid rim during anterior dislocation. The typical location is the 0–2 o'clock position on the humeral head (right shoulder, viewed from above). Engagement occurs when the lesion contacts the anterior glenoid rim during abduction-external rotation. Size is classed by the proportion of the humeral head diameter it occupies:
- Proportion of humeral head diameter
- Less than 20 percent
- Note
- Rarely engages in isolation
- Proportion of humeral head diameter
- 20–40 percent
- Note
- May engage depending on track
- Proportion of humeral head diameter
- Greater than 40 percent
- Note
- Often engaging; assess track carefully
Infraspinatus and posterior capsule. The infraspinatus tendon inserts on the greater tuberosity immediately posterior and lateral to the Hill-Sachs lesion in most cases, and the posterior capsule lies deep to it — both are incorporated into the tenodesis. Tenodesing the infraspinatus into the defect fills it and shifts the posterior capsule medially, rendering the lesion extra-articular. The posterior humeral circumflex artery and axillary nerve lie inferior and medial to the typical remplissage portal sites and are at risk with inferior anchor placement. Glenoid bone loss considerations. Glenoid bone loss is quantified on 3D CT using the best-fit circle method or the Pico method. The critical threshold is greater than 15–20 percent of glenoid width, which significantly narrows the glenoid track and increases recurrence risk after soft-tissue stabilisation. An inverted-pear glenoid morphology indicates substantial bone loss and is a contraindication to isolated remplissage. Remplissage outcomes. Arthroscopic remplissage combined with Bankart repair achieves recurrence rates of 5–10 percent in appropriately selected patients with engaging Hill-Sachs lesions and glenoid bone loss less than 15 percent. Systematic reviews report a mean loss of external rotation of 5–10 degrees, usually well tolerated. Patient-reported outcomes (WOSI, Rowe, ASES) improve significantly and are comparable to Latarjet in low-glenoid-bone-loss cohorts. Because remplissage does not restore glenoid bone stock, failure rates rise sharply when glenoid bone loss exceeds 15–20 percent.
References
Arthroscopic remplissage with Bankart repair for engaging Hill-Sachs lesions
- Original description of the arthroscopic remplissage technique combining posterior capsulodesis and infraspinatus tenodesis
- Demonstrated conversion of an intra-articular engaging defect to an extra-articular non-engaging position
- Reported low recurrence and acceptable range-of-motion outcomes in the initial series
Glenoid bone loss and recurrence after Bankart repair with and without remplissage
- Prospective cohort demonstrating that off-track lesions have markedly higher recurrence after isolated Bankart repair
- Remplissage significantly reduced recurrence in off-track lesions with minimal glenoid bone loss
- Confirmed the 15–20 percent glenoid bone loss threshold as the point at which bony augmentation becomes necessary
Systematic review of remplissage outcomes in anterior shoulder instability
- Pooled analysis of 12 studies, 459 patients undergoing remplissage with Bankart repair
- Overall recurrence rate 7.5 percent; mean external rotation loss 6 degrees
- Higher failure rates when glenoid bone loss exceeded 15 percent or when bipolar bone loss was present
Long-term outcomes of remplissage for engaging Hill-Sachs lesions
- Minimum 5-year follow-up of 48 patients after arthroscopic remplissage and Bankart repair
- Recurrence rate 8.3 percent; mean Rowe score 92; external rotation loss averaged 8 degrees
- No significant progression of glenohumeral arthritis at final follow-up
The glenoid track concept and its clinical application
- Introduced the glenoid track formula defining the zone of humeral-glenoid contact during abduction-external rotation
- Off-track lesions engage because their medial margin lies medial to the glenoid track margin
- Provided the decision algorithm distinguishing remplissage from Latarjet indications