Percutaneous retrograde medullary screw fixation of the superior pubic ramus for selected anterior pelvic ring injuries · advanced
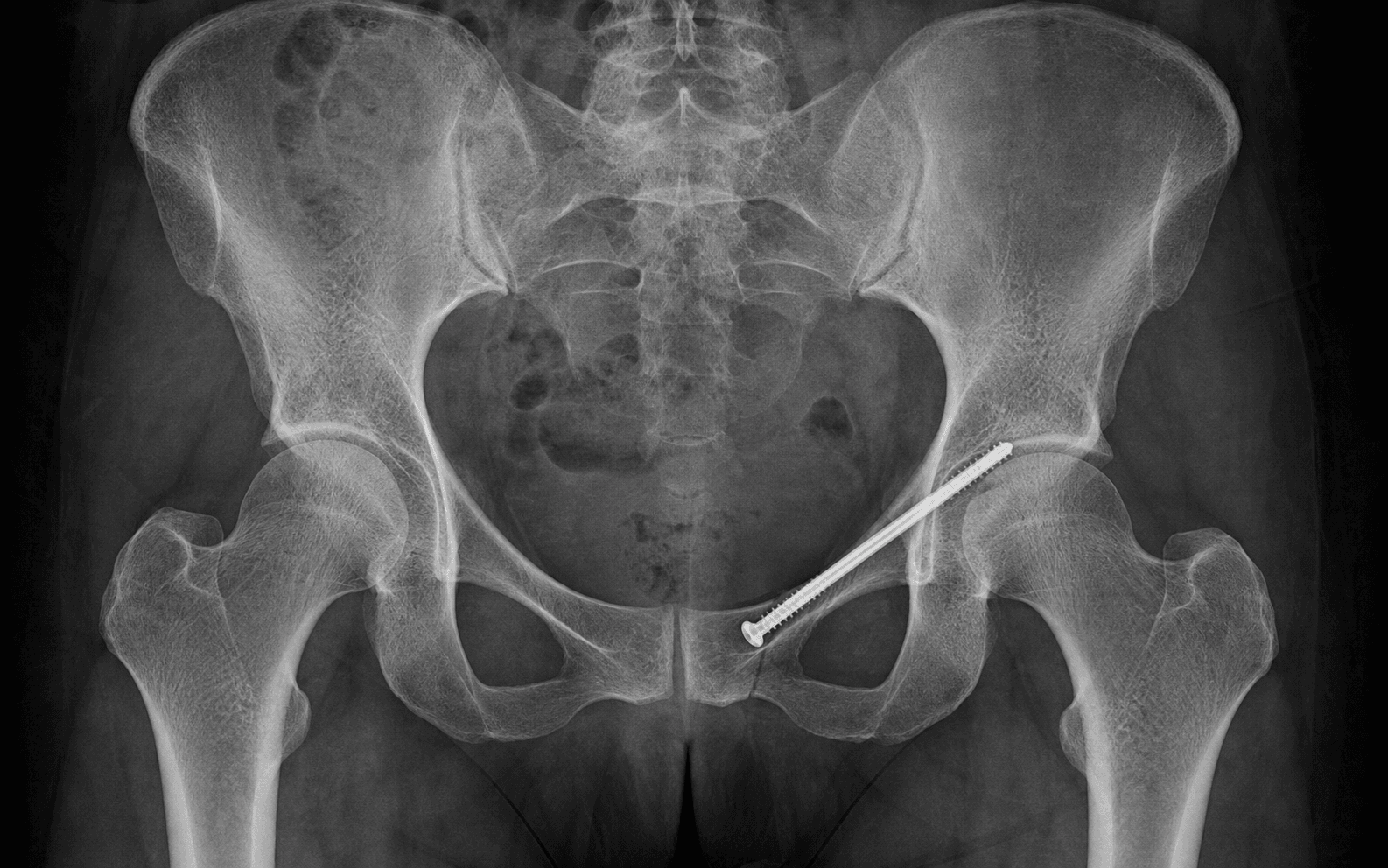
- A retrograde superior pubic ramus screw is an intramedullary cannulated screw inserted from an entry point on the pubic body near the pubic tubercle and advanced posterolaterally along the medullary canal of the superior ramus into the strong supra-acetabular ilium. It is a minimally invasive alternative to open anterior plating for an anatomically reducible ramus fracture with an intact corridor.
- The procedure is entirely fluoroscopy-dependent. Four views must be obtainable before the patient is prepped: inlet (anteroposterior depth of the wire), outlet (superoinferior containment within the ramus), obturator oblique outlet (profiles the ramus as a straight corridor) and iliac oblique (confirms the screw does not penetrate the acetabulum or hip joint). If these views cannot be seen, the case should not be done percutaneously.
- A screw does not reduce a ramus fracture. Anatomic reduction must be achieved first by closed manipulation, a pelvic clamp, an external fixator or a percutaneous Schanz pin joystick. The screw only maintains a reduction that has already been obtained.
- Six structures define the danger zone: the corona mortis crossing the ramus around 6 cm from the symphysis, the external iliac vessels along the pelvic brim, the obturator vessels and nerve beneath the ramus, the bladder behind the symphysis, the spermatic cord or round ligament at the superficial inguinal ring, and the acetabulum or hip joint laterally.
When & Why
The retrograde superior pubic ramus screw stabilises selected anterior pelvic ring injuries as part of an overall pelvic ring reconstruction. It is a fixation strategy, not a treatment in isolation — the decision to fix the anterior ring follows from the mechanical stability of the whole injury, because the pelvic ring is a ring and an anterior lesion is rarely the only break in an unstable pattern. Indications - Displaced superior pubic ramus fractures that are unstable or part of a rotationally or vertically unstable pelvic ring pattern (lateral compression type II or III, anteroposterior compression type II or III, vertical shear)
- Parasymphyseal fractures and ramus fractures extending into the pubic root, where an intramedullary screw can bridge and stabilise the anterior column
- Tilting fractures of the pubic root in osteoporotic bone, where a medullary screw gives better purchase than a plate
- Selected symphyseal and parasymphyseal disruptions where a medullary ramus screw supplements or substitutes for symphyseal plating
- Bilateral ramus fractures with an intact posterior ring but an unstable anterior segment, particularly in the elderly
- Fragility fractures of the anterior pelvic ring in geriatric patients fit for a short percutaneous procedure but not a large open exposure Relative indications include a ramus fracture with a displaced posterior ring injury that will be fixed posteriorly (fixing the anterior ring then restores the complete ring); a patient in whom an open anterior exposure is undesirable (contaminated or severely swollen anterior soft tissues, prior Pfannenstiel surgery, obesity); and a polytrauma patient who needs only minimal additional surgical insult once already positioned supine for another procedure. Contraindications
A destroyed or absent medullary ramus corridor (severe comminution, large bone defects) in which a screw cannot be contained; inability to obtain adequate multiplanar fluoroscopy; active infection at the intended entry site; and an unreduced ramus fracture that cannot be reduced closed or percutaneously and therefore requires an open reduction.
Severe osteoporosis where screw purchase in the supra-acetabular bone is expected to be poor; marked obesity or abundant bowel gas that degrades fluoroscopy; a very narrow ramus corridor on CT that will not accept even the smallest practical screw; and surgeon inexperience with percutaneous pelvic fixation without intraoperative navigation support.
The one decision that matters. Because every anterior fixation begins by asking the same question — can this ramus be fixed from the inside, through a percutaneous corridor, or must it be plated open? — the choice is between a retrograde intramedullary screw and open anterior plating, and the two are not mutually exclusive: a parasymphyseal fracture with symphyseal disruption may be plated at the symphysis while the ramus component is stabilised with a medullary screw.
- Retrograde ramus screw
- Minimal, percutaneous
- Open anterior plating
- Large anterior exposure, higher wound morbidity
- Retrograde ramus screw
- Low
- Open anterior plating
- Higher (corona mortis and iliac vessels at risk)
- Retrograde ramus screw
- Intramedullary cannulated screw, commonly 7.3 mm
- Open anterior plating
- Reconstruction plate (3.5 mm or 4.5 mm) and screws
- Retrograde ramus screw
- Intramedullary, load-sharing, resists ramus bending
- Open anterior plating
- Extramedullary plate, load-bearing beam across comminution
- Retrograde ramus screw
- Must be reducible closed or percutaneously first
- Open anterior plating
- Allows direct open reduction of comminution
- Retrograde ramus screw
- Destroyed corridor, poor fluoroscopy, severe osteoporosis
- Open anterior plating
- Contaminated or severely compromised anterior soft tissues
- Retrograde ramus screw
- Very low
- Open anterior plating
- Moderate
- Retrograde ramus screw
- High, multiplanar, learning curve
- Open anterior plating
- Lower
- Retrograde ramus screw
- Displaced but reconstructable ramus fracture with intact corridor
- Open anterior plating
- Comminuted parasymphyseal injury, symphyseal disruption, multiple ramus fractures
The corridor is everything. The single most important determinant of whether a percutaneous screw can be used is whether the ramus corridor exists and will accept a screw. Preoperative CT with three-dimensional reconstruction confirms the corridor, measures its narrowest diameter and plans the trajectory. A corridor that tapers below the diameter of the smallest practical screw is a contraindication, and in osteoporotic or severely comminuted rami the medullary channel may be destroyed entirely. Consent specifically for the percutaneous anterior procedure combined with posterior ring fixation when indicated; the small but serious risk of vascular injury (external iliac, obturator, corona mortis) requiring conversion to open vascular control; screw malposition including hip joint penetration requiring revision; loss of reduction; infection; and the need for limited weight bearing and deep vein thrombosis prophylaxis after surgery.
The Operation
The goal is to drive a single intramedullary cannulated screw down the medullary canal of the superior pubic ramus, from a pubic entry to the supra-acetabular ilium, entirely within bone and extra-articular to the hip, maintaining a reduction that has already been achieved. The operation is fluoroscopy-defined: the "exposure" is the multiplanar image, not a surgical incision, so confirming the four views on the awake patient and confirming the corridor on CT come first.
Operative sequence
- Full pelvic radiographs and a CT with multiplanar and three-dimensional reconstruction are mandatory.
- The CT characterises the pelvic ring pattern, confirms the ramus corridor exists, measures its narrowest diameter and plans the screw trajectory and length.
- The trajectory is rehearsed so the intended path keeps the screw entirely within bone, extra-articular to the hip and clear of the pelvic viscera. If the corridor is destroyed or too narrow, plan an open or alternative strategy now.
- Supine on a flat, fully radiolucent table. No bumps or breaks that would distort the pelvic ring are used unless required for reduction.
- Insert a Foley catheter before prepping to decompress the bladder, move it off the posterior aspect of the symphysis and superior rami, and improve the radiographic appearance of the anterior ring.
- Prepare and drape the entire pelvis and both groins to allow the pubic entry and, if needed, conversion to an open anterior approach or a counter-incision for reduction.
- Bring the C-arm in from the contralateral side.
- Obtain inlet, outlet, obturator oblique and iliac oblique views on the awake, unprepped patient, and confirm all four are obtainable before the patient is prepped and draped.
- Difficulty seeing the inlet or outlet because of obesity or bowel gas is a relative contraindication to the percutaneous route — discover it now, not after draping.
- A retrograde ramus screw maintains a reduction; it does not achieve one. Reduce the ramus anatomically before any wire is advanced.
- Reduction tools: closed manipulation by adjusting the leg with traction or internal/external rotation; a percutaneous Schanz pin into the pubic body or iliac crest as a joystick; a Jungbluth or pointed pelvic reduction forceps through stab incisions gripping the pubic body and lateral ramus; or an anterior external fixator to close an externally rotated or diastased anterior ring.
- Confirm the reduction on both inlet and outlet views (posterior displacement is best seen on the inlet) before touching a wire.
- The entry is on the pubic body, just lateral to the symphysis, at the level of the pubic tubercle, chosen so the wire aligns with the long axis of the ramus.
- Rehearse the intended trajectory under fluoroscopy on the obturator oblique outlet view first, so a line from the entry through the centre of the corridor lands in the supra-acetabular ilium.
- Make a small stab incision kept below and medial to the superficial inguinal ring to protect the spermatic cord or round ligament, and bluntly dissect to the pubic body.
- Introduce a smooth guide wire onto the pubic body and advance it under live fluoroscopy along the medullary corridor toward the supra-acetabular ilium, stopping short of the sacroiliac joint.
- The obturator oblique outlet is the primary guide — it projects the ramus as a straight corridor and shows the full length of the intended screw path.
- Switch repeatedly to the inlet to confirm anteroposterior depth and the outlet to confirm superoinferior containment.
- Before accepting the final position, look at the iliac oblique to be certain the wire has not drifted into the hip joint.
- Before any drilling, confirm the wire lies entirely within bone, extra-articular to the hip, with no cortical breach superiorly, inferiorly, anteriorly or posteriorly on inlet, outlet, obturator oblique outlet and iliac oblique views.
- If any view shows a breach, withdraw the wire and reposition it.
- Measure the screw length over the wire; drill over the wire only if the chosen screw requires it.
- Choose the screw to fit the corridor measured on CT — a 7.3 mm cannulated screw is most common; a smaller calibre (6.5 mm) for a narrow corridor; an 8.0 mm screw only if the corridor comfortably accepts it.
- Use a partially threaded lag screw when compression across the fracture is desired and the pattern permits; use a fully threaded position screw when the ramus is comminuted and lag compression would shorten or displace the anterior ring.
- Advance the screw over the wire, seating the head flush at the pubic body so it is not palpable and painful later.
- Close the small entry wound with skin sutures.
- Save final inlet, outlet, obturator oblique and iliac oblique images to document screw position, extra-articular placement and maintained reduction.
- Obtain a postoperative CT in complex cases or whenever joint position is uncertain to confirm containment.
- What it shows
- Anteroposterior or depth position of structures on the pelvic brim
- Role for the ramus screw
- Confirms the wire advances within the ramus in the sagittal plane (no anterior groin or posterior pelvic perforation); the key view for monitoring reduction, as posterior displacement is best seen here
- What it shows
- The pubic rami and symphysis in the superoinferior plane
- Role for the ramus screw
- Primary containment view: a superior exit threatens the external iliac vessels, an inferior exit threatens the obturator bundle — keep the wire centred in the ramus
- What it shows
- Aligns the beam along the long axis of the superior ramus
- Role for the ramus screw
- Primary guiding view: projects the ramus as a straight corridor and is used to drive the wire down its centre
- What it shows
- The posterior column, posterior wall and iliac wing
- Role for the ramus screw
- Confirms the lateral end of the screw stays extra-articular — excludes acetabular and hip joint penetration
- Superior exit at the lateral ramus strikes the external iliac artery and vein along the pelvic brim (artery lateral to the vein), and possibly the corona mortis medially — the most dangerous direction, monitored on the outlet view.
- Inferior exit into the obturator canal strikes the obturator artery, vein and nerve (adductor weakness, medial thigh numbness) — monitored on the outlet view.
- Lateral or posterior drift strikes the acetabulum and hip joint — a silent chondral injury excluded on the iliac oblique view.
- Posterior or superior perforation from the pubic body strikes the bladder — prevented by the preoperative Foley catheter.
A medullary screw is a maintainer of reduction, not a reducer. Reduce the ramus anatomically first with closed manipulation, a percutaneous clamp, a joystick or an external fixator, confirm it on inlet and outlet views, and only then advance the wire. A screw driven across a malreduced ramus simply fixes it in a displaced position.
Plan the entry point so that a line from the entry through the centre of the ramus corridor lands in the supra-acetabular ilium, then make the incision. Keep it below the superficial inguinal ring and bluntly dissect to the pubic body to keep the spermatic cord or round ligament out of harm's way.
Use a fully threaded position screw when the ramus is comminuted and lag compression would shorten the anterior ring, and seat the head flush at the pubic body so it is not palpable and painful later.
When the pubic region is inaccessible from scarring, a prior Pfannenstiel incision, a urinary diversion, a contaminated anterior wound or local soft-tissue injury, place the screw antegrade from a supra-acetabular entry just above the anterior inferior iliac spine, directing the wire anteromedially along the ramus toward the pubis. The same fluoroscopic principles apply: obturator oblique outlet profiles the corridor, inlet and outlet control depth and containment, and the iliac oblique excludes the hip joint.
Obesity, abundant bowel gas and contrast from prior imaging all degrade pelvic fluoroscopy. When adequate multiplanar images cannot be obtained, intraoperative navigation (fluoroscopic or CT-based) reconstructs the pelvis and tracks the wire in three dimensions, extending the percutaneous route to these patients. If neither adequate fluoroscopy nor navigation is available and the anterior ring must be fixed, convert to an open anterior approach with plating — a percutaneous screw driven through an uncontrolled corridor is never acceptable.
In a vertically or rotationally unstable injury, reduce and fix the posterior ring first (iliosacral or sacroiliac screws, lumbopelvic fixation, plating) to restore the overall template, then reduce and stabilise the anterior ring. Fixing the anterior ring in isolation, without addressing the posterior injury, risks late loss of reduction.
Aftercare & Complications
Rehabilitation | Phase | Timing | Weight bearing and activity | Monitoring | |-------|--------|-----------------------------|------------| | Acute | 0 to 2 weeks | Weight bearing dictated by the overall pelvic ring injury. For an isolated stable ramus with an intact posterior ring, touch-down or partial weight bearing for the first six weeks; for an unstable pattern, restrict to the posterior injury | Chemical deep vein thrombosis prophylaxis (low-molecular-weight heparin once haemostasis secure, mechanical on the contralateral limb); paracetamol and a short opioid course, NSAIDs cautiously; early upright mobilisation with physiotherapy and a frame as needed; wound check at 10 to 14 days | | Early follow-up | 2 to 6 weeks | Progressive as pain allows | Inlet and outlet radiographs at 2 and 6 weeks to confirm maintenance of reduction | | Maturing | 6 to 12 weeks | Advance toward full weight bearing as the ring stabilises | Inlet and outlet radiographs at 12 weeks; CT only for concern about reduction, screw position or union | | Return to function | around 3 months | Manual work and sport once the ring is stable and union is progressing | Union typically by 3 months, later in osteoporotic or comminuted injuries | Return to seated desk work is usually within 2 to 3 weeks. The deep vein thrombosis prophylaxis choice and duration are individualised to the bleeding risk, because pelvic trauma carries a high venous thromboembolism risk. Special situations. In the geriatric fragility-fracture patient the goal of surgery is pain relief and mobilisation as much as radiographic union, so early mobilisation with physiotherapy and aggressive osteoporosis treatment are central to the post-operative plan, with protected weight bearing initially and a low threshold for thromboprophylaxis in the immobilised elderly. Complications
- Incidence
- Rare but potentially catastrophic
- Recognition
- Brisk intraoperative bleeding, haemodynamic instability, expanding pelvic or groin haematoma
- Prevention and management
- Prevention: keep the wire contained on the outlet view, plan the corridor on CT, recognise the corona mortis zone. Management: immediate direct pressure, call vascular surgery, convert to open vascular control, resuscitate and transfuse
- Incidence
- Rare
- Recognition
- Adductor weakness and medial thigh or groin numbness, bleeding from an inferior wire exit
- Prevention and management
- Prevention: avoid inferior wire exit, confirmed on the outlet view. Management: observe an obturator neuropraxia; explore and control if there is active bleeding from an obturator vessel injury
- Incidence
- Small percentage, dependent on fluoroscopic quality
- Recognition
- New hip or groin pain after surgery, restricted or painful rotation; may be silent initially, chondral injury or sepsis if missed
- Prevention and management
- Prevention: iliac oblique view to exclude joint entry throughout; reposition any wire drifting toward the acetabulum. Management: remove or reposition the screw; refer for hip preservation if a chondral injury is present
- Incidence
- Variable, higher when fluoroscopy is inadequate
- Recognition
- Postoperative CT shows cortical breach; loss of fixation or pain
- Prevention and management
- Prevention: multiplanar fluoroscopy, confirm the corridor and trajectory on preoperative CT. Management: revise the screw if it is symptomatic, intra-articular or unstable
- Incidence
- Higher with comminution, osteoporosis and an unfixed posterior ring
- Recognition
- Drift or displacement on serial radiographs, leg-length or rotational asymmetry
- Prevention and management
- Prevention: reduce anatomically first, fix the posterior ring when indicated, choose the appropriate implant and length. Management: revision fixation once the cause is addressed
- Incidence
- Very rare
- Recognition
- Haematuria, lower abdominal pain, ileus, low urine output
- Prevention and management
- Prevention: Foley catheter before prepping, avoid posterior or superior wire exit. Management: leave the catheter, involve urology, repair if intraperitoneal
- Incidence
- Very low, less than 2 percent (percutaneous)
- Recognition
- Erythema, warmth, discharge, systemic inflammatory signs
- Prevention and management
- Prevention: sterile percutaneous technique, prophylactic antibiotics. Management: wound swab and oral antibiotics; debride and give intravenous antibiotics if deep
- Incidence
- Occasional
- Recognition
- Tender, palpable screw head over the pubis, pain with activities pressing on the groin
- Prevention and management
- Prevention: seat the screw head flush, countersink where the cortex allows. Management: remove the screw after union if it remains symptomatic
- Incidence
- Higher with poor fixation, comminution and osteoporosis
- Recognition
- Persistent groin or pelvic pain, persistent radiolucency at 3 to 6 months
- Prevention and management
- Prevention: stable fixation of the reduced ramus; bone graft for comminuted or deficient fractures. Management: revision fixation with graft if symptomatic and unstable
Viva & Exam Focus
CORRIDORCORRIDOR — the retrograde ramus screw technique
DANGERDANGER — the six structures of the ramus
The six danger structures at a glance
An aberrant arterial and venous anastomosis between the inferior epigastric or external iliac system and the obturator system, crossing the superior pubic ramus around 6 cm lateral to the symphysis. It lies directly in the field of the pubic entry and any anterior exposure, and division or avulsion causes brisk bleeding that is difficult to control because the vessel retracts above and below the ramus.
The external iliac artery and vein run along the pelvic brim on the medial border of psoas, just superior and posterior to the lateral superior ramus (artery lateral to the vein). A wire or screw that exits the superior cortex of the lateral ramus injures these vessels — the outlet view is the safeguard that keeps the wire contained.
The obturator artery, vein and nerve run in the obturator canal beneath the superior ramus; an inferior exit threatens them. The bladder lies immediately behind the symphysis and superior ramus in the retropubic space; a posterior or superior perforation from the pubis can injure it, prevented by a preoperative Foley catheter.
The spermatic cord in males and the round ligament in females pass through the superficial inguinal ring, just superior and lateral to the pubic tubercle. The retrograde entry incision sits directly beneath them; a blind stab incision can transect them, so use a small incision and blunt dissection to the pubic body, protecting the contents of the ring superiorly.
The acetabulum forms the lateral boundary of the corridor. A wire that drifts too lateral or posterior enters the hip joint or penetrates the acetabular cartilage — the iliac oblique view is the safeguard. Joint penetration may be clinically silent initially but causes early hip pain, chondral injury or sepsis if missed.
Surgeons assume the intramedullary screw will reduce the fracture as it crosses it. It will not. A screw driven across a malreduced ramus simply fixes it in a displaced position. Reduce the ramus anatomically first, then advance the wire to maintain the reduction obtained.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 34-year-old man is involved in a high-speed motor vehicle collision. Pelvic CT shows a displaced right superior pubic ramus fracture with a right sacral fracture and anterior widening of the right sacroiliac joint — a rotationally and vertically unstable pelvic ring injury. He is now haemodynamically stable. Describe your management, with particular reference to the anterior ring.”
“You are placing a retrograde right superior pubic ramus screw. The wire is advancing well on the obturator oblique outlet view, but on the outlet view you notice the wire has begun to drift toward the superior cortex of the lateral ramus. What is the significance, what structures are at risk, and what do you do next?”
“An 82-year-old woman sustained a low-energy fall three weeks ago and has a displaced left superior pubic ramus fracture. She remains in severe pain and is unable to mobilise despite analgesia and protected weight bearing. CT shows the ramus is displaced but the medullary corridor is preserved. How do you decide whether to fix this, and if so how?”
Indications and decision points
- Displaced ramus fractures that are part of an unstable ring pattern (LC II or III, APC II or III, vertical shear)
- Selected parasymphyseal and symphyseal disruptions where a medullary screw supplements or substitutes for plating
- Tilting pubic root fractures and geriatric fragility fractures with a preserved corridor and failed non-operative care
- Contraindicated by a destroyed corridor, inadequate fluoroscopy, or an unreduced ramus that cannot be reduced closed
Anatomy and danger structures
- Corona mortis: anastomosis between the external iliac or inferior epigastric and obturator systems, crossing the ramus around 6 cm from the symphysis
- External iliac artery and vein: along the pelvic brim, superior and posterior to the lateral ramus (artery lateral to vein)
- Obturator artery, vein and nerve: in the obturator canal beneath the ramus
- Bladder: behind the symphysis and superior rami (Foley catheter decompresses and retracts it)
- Spermatic cord or round ligament: at the superficial inguinal ring, just above the pubic entry
- Acetabulum and hip joint: the lateral boundary of the corridor (iliac oblique view excludes penetration)
The corridor and fluoroscopy
- Confirm the ramus corridor exists and measure its narrowest diameter on preoperative CT with three-dimensional reconstruction
- Inlet view (beam cephalad): anteroposterior or depth position of the wire; monitors reduction
- Outlet view (beam caudad): superoinferior containment within the ramus
- Obturator oblique outlet view: profiles the ramus as a straight corridor, the primary guiding view
- Iliac oblique view: confirms the screw stays extra-articular, clear of the acetabulum and hip joint
- All four views must be obtainable on the awake patient before prepping
Operative technique
- Supine on a radiolucent table, Foley catheter, C-arm contralateral; confirm all four views before prepping
- Reduce the ramus first by closed manipulation, a percutaneous clamp, a joystick or an external fixator
- Entry on the pubic body just lateral to the symphysis, below the superficial inguinal ring
- Drive the wire under live fluoroscopy down the corridor on the obturator oblique outlet view
- Confirm containment on the outlet and depth on the inlet throughout; exclude the hip joint on the iliac oblique
- Measure, drill if needed, and place a cannulated screw that fits the corridor, seating the head flush; save all four final images
Implants
- Cannulated screw, most commonly 7.3 mm; 6.5 mm for a narrow corridor, 8.0 mm only if the corridor comfortably accepts it
- Partially threaded for lag compression across a suitable fracture; fully threaded position screw for comminution to avoid shortening
- Guide wire advanced under live fluoroscopy; washer and countersinking used selectively at the pubic head
- Calibre and length chosen to fit the corridor measured on preoperative CT
Complications
- Vessel injury (external iliac, corona mortis, obturator): rare but catastrophic — prevention is containment on the outlet view and CT corridor planning
- Acetabular or hip joint penetration: small percentage — prevent with the iliac oblique view; revise if intra-articular
- Loss of reduction: higher with comminution, osteoporosis and an unfixed posterior ring
- Screw malposition or cut-out: prevented by multiplanar fluoroscopy and preoperative CT planning
- Bladder injury, infection and hardware prominence are uncommon; non-union is higher with poor fixation
Post-operative and rehabilitation
- Weight bearing dictated by the overall pelvic ring injury, not the anterior screw in isolation
- Chemical deep vein thrombosis prophylaxis — pelvic trauma carries a high thromboembolism risk
- Inlet and outlet radiographs at 2, 6 and 12 weeks; CT for concern about reduction or union
- Union typically by 3 months; return to manual work and sport once the ring is stable and union is progressing
Special cases
- Geriatric fragility fractures: a retrograde screw relieves pain and enables mobilisation when the corridor is preserved and non-operative care has failed
- Combined injuries: the retrograde ramus screw is usually paired with posterior ring fixation; fix the posterior ring first to restore the template
- Obesity or poor fluoroscopy: consider intraoperative navigation, or convert to an open anterior approach with plating
- Antegrade variant: supra-acetabular entry toward the pubis when the pubic region is inaccessible
Background & Evidence
Epidemiology. Low-energy fragility fractures of the anterior pelvic ring are increasingly common in the elderly, often sustained in a simple fall. A superior pubic ramus fracture may be isolated or accompanied by a contralateral ramus fracture, an ischial ramus fracture or a sacral insufficiency fracture. Persistent pain and an inability to mobilise are the typical problems that bring these patients to surgical consideration, and a displaced ramus fracture with a preserved corridor that has failed non-operative care is the setting in which a retrograde medullary screw is most useful. The superior pubic ramus corridor. The superior pubic ramus is a curved osseous strut connecting the pubic body to the acetabulum. It contains a medullary canal that runs from the pubic body, through the ramus superomedial to the acetabulum, into the dense supra-acetabular ilium — and this medullary channel is the corridor for the retrograde screw. The corridor is narrow, curved in two planes and individually variable: some patients have a generous channel that readily accepts a screw, while others have a thin, sharply curved ramus in which safe screw placement is impossible. Because it varies, preoperative CT with multiplanar and three-dimensional reconstruction is essential to measure the narrowest diameter, the curvature and the relationship to the acetabulum and hip joint, and to plan a trajectory that keeps the screw entirely within bone, extra-articular and clear of the pelvic viscera. The acetabular boundary. Laterally the corridor is bounded by the acetabulum. The screw must stay superior and medial to the acetabular dome, in the true ramus corridor, to avoid entering the hip joint. An intra-articular screw damages hyaline cartilage and may present late with hip pain or post-traumatic arthritis — the most feared silent error of the procedure, excluded on the iliac oblique view. Danger structures in detail. The corona mortis is an aberrant vascular connection between the inferior epigastric or external iliac system above and the obturator system below, crossing the superior pubic ramus around 6 cm lateral to the symphysis; it is present in a majority of hemipelves in cadaveric studies and varies from a small venous connection to a substantial arterial anastomosis, so division produces brisk bleeding from both ends of a vessel that retracts above and below the ramus. The external iliac artery and vein run along the pelvic brim on the medial border of psoas, superior and posterior to the lateral superior ramus, with the artery lateral to the vein, before passing under the inguinal ligament to become the femoral vessels. The obturator artery, vein and nerve leave the pelvis through the obturator canal inferior to the ramus; an inferior exit threatens the nerve (adductor weakness and medial thigh numbness) and the vessels. The bladder lies immediately behind the pubic symphysis and superior rami in the retropubic space, decompressed and retracted by a preoperative Foley. The spermatic cord in males and the round ligament in females pass through the superficial inguinal ring just superior and lateral to the pubic tubercle, directly above the retrograde entry. Rationale and biomechanics. Open plating of the anterior pelvic ring through a Pfannenstiel or extended ilioinguinal exposure provides strong fixation and allows direct reduction but carries the morbidity of a large anterior wound: blood loss from the corona mortis and iliac vessels, infection, hernia and wound complications. The retrograde medullary ramus screw provides stable intramedullary fixation through a percutaneous route because it lies on the neutral axis of the ramus and resists bending in the plane of greatest deformation, behaving as a load-sharing implant. Key evidence. Routt and colleagues introduced the fluoroscopically guided percutaneous retrograde medullary superior pubic ramus screw in 1995, showing that multiplanar fluoroscopy and a reducible fracture corridor are prerequisites for safe placement. Starr and colleagues (2008) found that fracture comminution, poor bone quality and residual displacement after reduction predict fixation failure, confirming that percutaneous ramus screws are effective when the corridor is intact and the reduction anatomic. The Young-Burgess classification (Burgess, 1990) provides the framework that determines which anterior ring injuries require stabilisation, Tile (1988) set out the principle that mechanically unstable pelvic ring injuries should be fixed, and Matta and Tornetta (1996) supported combined anterior and posterior internal fixation for vertically and rotationally unstable patterns.
References
The retrograde medullary superior pubic ramus screw for the treatment of anterior pelvic ring disruptions: a new technique
- Introduced the fluoroscopically guided percutaneous retrograde medullary superior pubic ramus screw for unstable anterior pelvic ring injuries.
- Showed that the technique avoids the morbidity of an open anterior exposure while providing stable intramedullary fixation of the ramus.
- Emphasised that multiplanar fluoroscopy and a reducible fracture corridor are prerequisites for safe screw placement.
Superior pubic ramus fractures fixed with percutaneous screws: what predicts fixation failure?
- Reviewed superior pubic ramus fractures treated with percutaneous screws to identify factors associated with fixation failure.
- Found that fracture comminution, poor bone quality and residual displacement after reduction predicted loss of fixation.
- Concluded that percutaneous ramus screws are effective when the ramus corridor is intact and an anatomic reduction is achieved.
Pelvic ring disruptions: effective classification system and treatment protocols
- Established the Young-Burgess biomechanical classification of pelvic ring disruptions into anteroposterior compression, lateral compression and vertical shear patterns.
- Linked a protocolised resuscitation approach matched to the injury pattern with a marked reduction in pelvic fracture mortality.
- Provided the framework that determines which anterior ring injuries require surgical stabilisation.
Pelvic ring fractures: should they be fixed?
- Set out the principle that mechanically unstable pelvic ring injuries should be surgically stabilised rather than managed non-operatively.
- Defined the stability-based classification that guides which patients benefit from fixation of the anterior and posterior ring.
- Argued that restoring pelvic anatomy and stability permits early mobilisation and reduces late deformity and pain.
Internal fixation of unstable pelvic ring injuries
- Reported outcomes of open internal fixation of unstable pelvic ring injuries across both the anterior and posterior columns.
- Showed that anatomic reduction and stable fixation permitted early mobilisation and good functional results.
- Supported combined anterior and posterior internal fixation for vertically and rotationally unstable pelvic patterns.