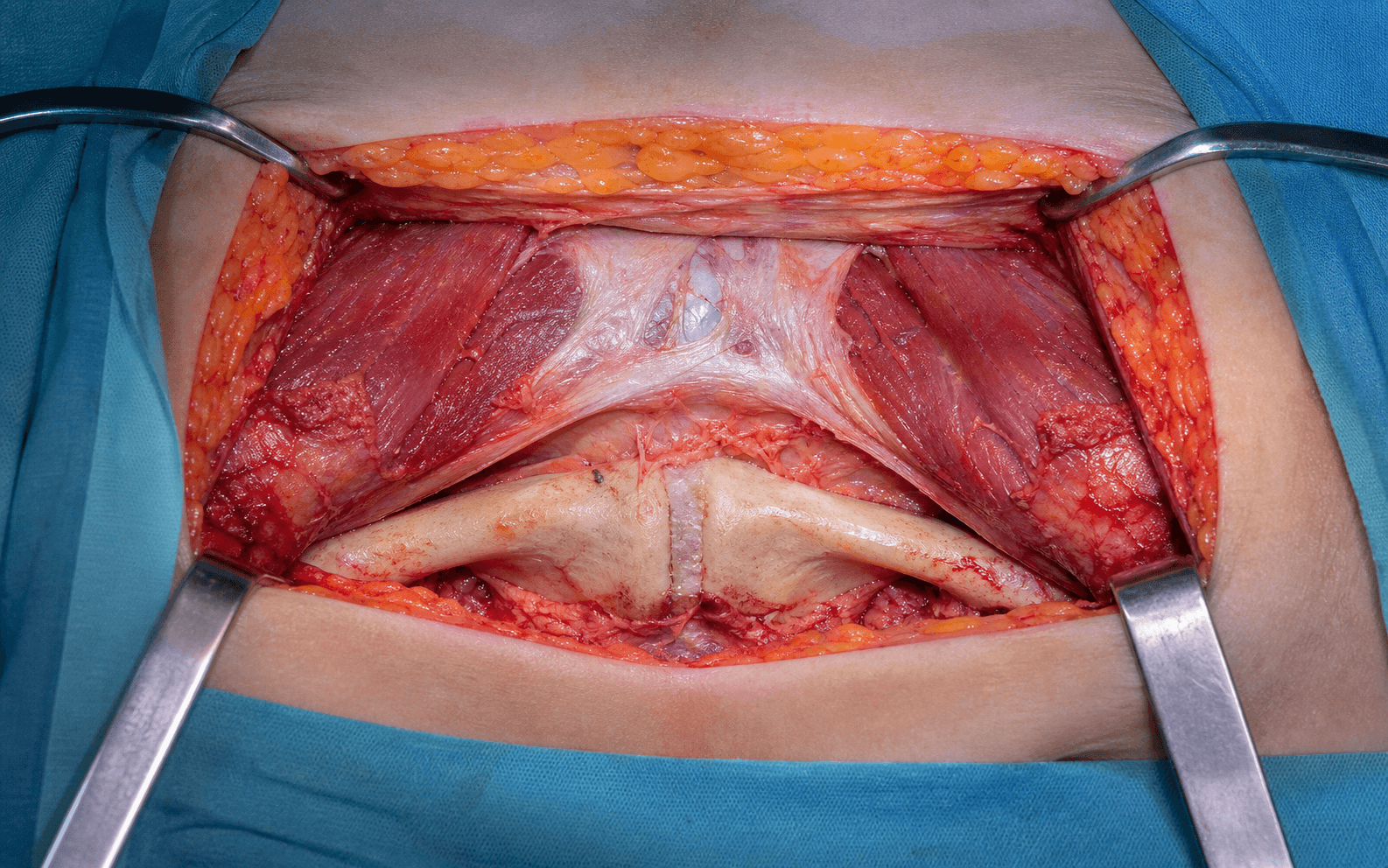
Transverse Suprapubic Incision | Rectus Split or Release | Corona Mortis at Risk
- Transverse suprapubic incision two fingerbreadths (about 2 cm) above the pubic crest, 8 to 12 cm long, following Langer's lines for an excellent cosmetic result.
- Decompress the bladder with a urinary catheter before any deep dissection — the bladder lies immediately deep to the linea alba at the symphysis.
- There is no true internervous plane: the rectus abdominis is supplied segmentally by T7 to T12, so a midline linea alba split or release of one rectus head does not denervate the muscle.
- Identify and control the corona mortis on the superior pubic ramus 4 to 6 cm lateral to the symphysis (present in about 30 to 40 percent of patients) before placing a plate.
- Repair the rectus securely to the pubis or linea alba at closure with heavy suture — failure leads to abdominal wall hernia and loss of anterior pelvic stability.
When & Why
What it exposes. The Pfannenstiel approach gives direct anterior access to the pubic symphysis, the superior pubic rami and the retropubic space of Retzius through a single transverse suprapubic incision. It is the standard anterior exposure for symphyseal plating in open-book (APC) pelvic ring injuries and forms the superficial part of the modified Stoppa intrapelvic approach to the acetabulum. Why transverse (and not midline). The incision lies two fingerbreadths above the pubic crest and follows Langer's lines, healing with an excellent cosmetic result and a low hernia rate compared with a vertical midline laparotomy. It can be extended laterally along the pelvic brim into the Stoppa approach without a second skin incision, and proximally in the midline if abdominal exploration is needed. Principal indications. - Symphyseal diastasis in APC II and APC III pelvic ring injuries requiring plate stabilisation
- Displaced superior pubic ramus fractures with anterior ring instability
- Combined anterior ring and acetabular fractures (transverse, T-type, anterior column) via the Stoppa extension
- Revision surgery for symptomatic symphyseal nonunion or malunion
- Open-book injuries with urological or bowel entrapment requiring direct access Contraindications are mostly relative: active infection or open wounds in the suprapubic region, dense adhesions from previous lower abdominal surgery, a severe bladder injury requiring urological repair first, or patient instability precluding anterior pelvic surgery. Alternatives. A vertical midline laparotomy when simultaneous abdominal exploration is required; the modified Stoppa (intrapelvic) approach for full anterior column and acetabular access through the same skin incision; the ilioinguinal approach when a lateral window is needed for the iliac wing or posterior column; and percutaneous anterior ring fixation for minimally displaced ramus fractures in stable patterns. Position and landmarks. Supine on a radiolucent table with full fluoroscopic access (inlet, outlet, obturator and iliac oblique views), the C-arm brought in from the opposite side. Insert a urinary catheter and confirm it is draining before skin preparation. Slight hip flexion (10 to 15 degrees) relaxes the iliopsoas and rectus. Palpate and mark the pubic symphysis, pubic crest, superior pubic rami, the pectineal eminence and the ASIS (the lateral limit if ramus exposure is needed). A cell saver and cross-matched blood should be available for high-energy pelvic injuries.
The Exposure
Work down through the abdominal wall in the midline, decompress and protect the bladder, enter the space of Retzius, and then — for ramus work — develop the subperiosteal plane out along the superior pubic ramus where the corona mortis must be found and controlled before any plate is placed.
Exposure sequence
- A transverse incision two fingerbreadths (about 2 cm) above the pubic crest, 8 to 12 cm long, slightly convex inferiorly to follow the natural skin crease.
- In obese patients place it a little higher to avoid the skin fold; extend toward the ASIS if ramus access is needed.
- Divide subcutaneous fat and Scarpa's fascia in line with the skin incision, coagulating any superficial vessels.
- Expose the anterior rectus sheath (linea alba) in the midline and the rectus sheath laterally.
- Incise the linea alba vertically in the midline from the superior edge of the symphysis proximally for 6 to 8 cm.
- For wider exposure, sharply release one rectus head from the pubic crest with electrocautery, staying directly on bone — there is no true internervous plane because the rectus is supplied segmentally by T7 to T12.
- Gently retract the rectus muscles laterally; if one head was released, reflect it proximally.
- Develop the plane between the transversalis fascia (the posterior rectus sheath is absent below the arcuate line) and the bladder, entering the space of Retzius bluntly with a finger or sponge.
- Confirm the urinary catheter is draining — the decompressed bladder falls away from the symphysis.
- Place a malleable retractor or sponge to protect the bladder throughout, and avoid vigorous retraction on the bladder wall.
- Clear the symphyseal disc and surrounding ligaments to display both pubic bodies.
- Reduce the diastasis with pointed reduction clamps or a Jungbluth clamp, then apply a 3.5 mm reconstruction plate (typically 4 to 6 holes) across the symphysis with screws directed into the rami and away from the hip joint.
- For superior ramus exposure, elevate the rectus and pectineus subperiosteally from the superior ramus.
- Identify the corona mortis crossing the ramus 4 to 6 cm lateral to the symphysis (present in 30 to 40 percent of patients); ligate or coagulate it before plate placement.
- Mobilise the spermatic cord or round ligament superiorly and protect it with a vessel loop.
The bladder lies immediately deep to the linea alba and rectus at the pubic symphysis. A urinary catheter must be placed and confirmed draining before the first incision — failure to decompress risks iatrogenic bladder injury during rectus split or retraction. In suspected bladder or urethral injury (haematuria, meatal blood, perineal bruising), coordinate with urology before proceeding.
The rectus abdominis is supplied segmentally by T7 to T12, with the nerves entering its lateral border and travelling medially within the muscle, so a midline linea alba split or release of one rectus head does not denervate it. The approach therefore relies on midline splitting or controlled rectus release rather than an intermuscular plane.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Inferior epigastric vessels (during lateral extension)
- Protection
- Identify and ligate if necessary
- Structure at risk
- Bladder
- Protection
- Catheter decompression before deep dissection; malleable retractor throughout
- Structure at risk
- Corona mortis (obturator to external iliac anastomosis)
- Protection
- Identify 4 to 6 cm lateral to symphysis; ligate before plating
- Structure at risk
- Spermatic cord / round ligament
- Protection
- Mobilise superiorly; protect with a vessel loop
- Structure at risk
- Deep dorsal vein complex (Santorini)
- Protection
- Pack and direct pressure; suture ligation; avoid blind clamping
- Structure at risk
- External iliac vessels (vein medial to artery on the brim)
- Protection
- Gentle retraction; avoid vigorous medial retraction
- Structure at risk
- Rectus abdominis repair failure leading to hernia
- Protection
- Heavy suture through bone or ligament; consider mesh
Corona mortis injury management. If brisk bleeding is encountered from the superior ramus, apply direct pressure with a sponge or finger — do not blindly clamp. Pack the space of Retzius firmly and maintain pressure for 5 to 10 minutes; if bleeding persists, carefully remove the packing, identify the vessel and ligate both proximal and distal ends. For uncontrolled arterial bleeding, leave the packing in place and obtain interventional radiology embolisation. Most injuries are venous, but arterial injury can cause life-threatening retroperitoneal haemorrhage. Post-operative complications
- Incidence
- 2 to 5 percent
- Prevention and treatment
- Secure rectus repair with heavy suture; mesh in high-risk patients; surgical repair if it develops
- Incidence
- 2 to 5 percent
- Prevention and treatment
- Prophylactic antibiotics and careful soft-tissue handling; irrigation and debridement with culture-directed antibiotics
- Incidence
- 5 to 10 percent
- Prevention and treatment
- Anatomic reduction and stable fixation, bone graft for a gap; revision plating
- Incidence
- 10 to 20 percent
- Prevention and treatment
- Anatomic reduction, avoid over-compression; multimodal pain management and pelvic floor physiotherapy
- Incidence
- 5 to 10 percent
- Prevention and treatment
- Chemoprophylaxis (LMWH or aspirin) for 4 to 6 weeks and early mobilisation; anticoagulation if it occurs
Extensile options. The three rectus-management variants map directly onto how far the exposure is taken: a classic midline linea alba split for an isolated symphysis, a unilateral rectus release for wider ramus exposure, and an extended Pfannenstiel combined with the Stoppa intrapelvic plane for acetabular fractures. - Modified Stoppa (intrapelvic) extension. After entering the space of Retzius, release the rectus insertion and develop the extraperitoneal plane along the pelvic brim, elevating the iliopsoas from the anterior column and quadrilateral surface. This exposes the entire anterior pelvic ring, anterior column and acetabulum without a second skin incision, and avoids the morbidity of the lateral window of the ilioinguinal approach.
- Lateral extension toward the ilioinguinal. Extend the incision laterally along the inguinal ligament toward the ASIS and develop the plane between the external oblique aponeurosis and the inguinal ligament to reach the iliac wing and anterior column from a lateral window.
- Proximal midline extension. If simultaneous laparotomy is needed, extend the incision proximally in the midline through the linea alba toward the umbilicus — rarely needed in isolated pelvic ring trauma.
- Combined posterior approaches. For APC III injuries with posterior ring disruption, combine the Pfannenstiel approach with percutaneous or open posterior fixation (iliosacral screws, sacral bars or posterior tension-band plating) in the same or a staged procedure. Closure. Irrigate the retropubic space copiously and achieve meticulous haemostasis of the deep dorsal vein complex. Reattach the rectus abdominis to the pubic crest or linea alba with heavy absorbable or non-absorbable suture (number 1 or 2 PDS or Prolene) passed through drill holes in the pubis or the ligamentous attachments. Close the anterior rectus sheath with running absorbable suture (number 0 PDS), approximate Scarpa's fascia, and close skin with subcuticular absorbable suture or staples; consider mesh reinforcement in obese patients or poor tissue quality. Confirm reduction and plate position on pelvic inlet, outlet and oblique views, with CT if screw position near the hip joint or reduction quality is in doubt. Rehabilitation. Touch or non-weight bearing on the affected side for 6 to 12 weeks depending on posterior ring stability, with crutches or a walker; gentle hip flexion and abduction as pain allows, avoiding aggressive external rotation for the first 6 weeks to protect the symphyseal repair. Follow-up inlet and outlet radiographs at 6 and 12 weeks, progressing weight bearing as healing permits. Consent (globally applicable). Discuss bladder injury (1 to 3 percent), corona mortis bleeding requiring ligation or embolisation (2 to 5 percent), abdominal wall hernia (2 to 5 percent), chronic symphyseal pain or dyspareunia (10 to 20 percent), infection (2 to 5 percent), and the need for posterior ring stabilisation in APC III injuries.
Procedures Through This Approach
- Symphyseal plating for APC II/III pelvic ring injuries — the principal operation, open reduction and plate fixation of symphyseal diastasis with a 3.5 mm reconstruction plate resisting the external rotation forces that opened the symphysis.
- Fixation of displaced superior pubic ramus fractures and anterior ring stabilisation in combined pelvic-acetabular injuries.
- Modified Stoppa intrapelvic approach to the acetabulum — anterior column, quadrilateral surface and medial wall — developed through the same skin incision.
- Exposure for transverse and T-type acetabular fracture ORIF when combined with the Stoppa plane.
- Debridement and stabilisation of symphyseal infection or osteomyelitis (rare).
Viva & Exam Focus
PFANNENPFANNEN — the Pfannenstiel exposure
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old man is brought in after a high-speed motor vehicle collision. CT shows an APC III pelvic ring injury with 3 cm of symphyseal diastasis and a posterior sacral fracture. How would you approach the anterior ring?”
“During a Pfannenstiel approach for symphyseal plating you encounter brisk bleeding from the superior pubic ramus while elevating periosteum. What is your immediate management?”
“At the end of a Pfannenstiel approach for symphyseal plating, how do you close the wound and what steps prevent an abdominal wall hernia?”
Position and setup
- Supine on a radiolucent table with full fluoroscopic access
- Urinary catheter placed and draining before incision
- Arms abducted less than 90 degrees and padded
- Prep from umbilicus to mid-thigh including both iliac crests
- C-arm from the opposite side for inlet, outlet and oblique views
Incision and landmarks
- Transverse incision two fingerbreadths above the pubic crest
- Length 8 to 12 cm, slightly convex inferiorly
- Pubic symphysis and crest are the midline landmarks
- ASIS marks the lateral extent if ramus exposure is needed
- Follows the natural skin crease (Langer's lines) for cosmesis
Internervous plane and dissection
- No true internervous plane — rectus supplied segmentally by T7 to T12
- Midline linea alba split or unilateral rectus release from the pubis
- Enter the space of Retzius bluntly after bladder decompression
- Protect the bladder with a malleable retractor throughout
- Elevate rectus and pectineus subperiosteally from the ramus
Danger structures
- Bladder — decompressed with a catheter before deep dissection
- Corona mortis — identify and ligate 4 to 6 cm lateral on the ramus
- Spermatic cord or round ligament — mobilise and protect laterally
- Deep dorsal vein complex (Santorini) — pack and ligate if bleeding
- External iliac vessels — lateral limit of exposure, protect gently
Procedures and fixation
- Symphyseal plating for APC II/III pelvic ring injuries
- Superior ramus fixation for anterior ring instability
- Gateway to the modified Stoppa approach for the acetabulum
- 3.5 mm reconstruction plate across the symphysis (4 to 6 holes typical)
- Screws directed into the rami, avoiding the hip joint
Closure and post-op
- Secure rectus repair to the pubis with heavy suture through bone
- Close the anterior rectus sheath with running absorbable suture
- Consider mesh reinforcement in obese or high-risk patients
- Touch weight bearing for 6 to 12 weeks with posterior stabilisation
- Monitor for hernia, infection and chronic symphyseal pain
References
The Pfannenstiel approach is used worldwide for symphyseal plating in APC pelvic ring injuries and as the anterior window for the modified Stoppa approach to acetabular fractures. Principles converge across examination systems. Side-by-side principles (where guidance converges): - AO Foundation — CT mandatory for all pelvic ring and acetabular fractures; corona mortis identification required before superior ramus plating; staged management with external fixation for haemodynamically unstable patients.
- BOA / BOAST — early pelvic binder application, urological assessment for bladder injury, joint orthoplastic care for open pelvic injuries; definitive fixation only once soft tissues and physiology permit.
- OTA / AAOS — anatomic reduction of the symphysis and posterior ring; plate fixation resisting external rotation forces; identification and protection of the corona mortis. Registry and population evidence: - APC II and III injuries comprise approximately 15 to 20 percent of pelvic ring fractures in high-energy trauma registries.
- Symphyseal plating through a Pfannenstiel approach achieves stable anterior ring fixation in greater than 90 percent of cases when combined with appropriate posterior stabilisation.
- Corona mortis injury rates have fallen from a historical 10 to 15 percent to less than 3 percent in modern series with deliberate identification. Global practice variation. In high-resource settings, dedicated pelvic reconstruction plates and routine CT with three-dimensional reconstruction are standard. In resource-limited settings the same biomechanical principles are achieved with contoured reconstruction plates or even one-third tubular plates, and external fixation has a larger role for temporisation.
Corona Mortis: Incidence, Location, and Clinical Significance in Pelvic Surgery
- Corona mortis was identified in 36 percent of 80 pelvic specimens
- Mean distance from the pubic symphysis was 5.2 cm (range 3.5 to 7.8 cm)
- Venous corona mortis was more common than arterial (ratio 2:1)
- Injury during anterior pelvic approaches can cause significant retroperitoneal bleeding
Modified Stoppa Approach for Acetabular Fractures: Extended Indications
- The modified Stoppa intrapelvic approach through a Pfannenstiel incision provides excellent access to the anterior column and quadrilateral surface
- Avoids the morbidity of the lateral window of the ilioinguinal approach
- Combined with the posterior Kocher-Langenbeck approach for selected fracture patterns
- Low rate of heterotopic ossification compared with extensile approaches
Symphyseal Plating for APC Pelvic Ring Injuries: Long-Term Outcomes
- Symphyseal plating through a Pfannenstiel approach achieved stable fixation in 92 percent of APC injuries
- Anatomic reduction of the symphysis correlated with better functional outcomes
- Posterior ring fixation was required in APC III injuries for overall stability
- Chronic symphyseal pain occurred in 15 percent of patients at long-term follow-up
Abdominal Wall Hernia After Pfannenstiel Incision for Pelvic Surgery
- Incisional hernia rate after a Pfannenstiel incision was 3.2 percent in a large cohort study
- Risk factors included obesity, wound infection, and failure of rectus sheath closure
- Mesh reinforcement reduced recurrence in high-risk patients
- Most hernias presented within 2 years of surgery
The Pfannenstiel Incision in Pelvic and Acetabular Surgery
- The Pfannenstiel incision provides excellent access to the pubic symphysis and medial superior rami with low morbidity
- When extended into the modified Stoppa approach, the same incision allows full anterior column and acetabular visualisation
- Corona mortis identification and ligation is mandatory before plate placement on the superior ramus
- Rectus repair at closure is critical to prevent abdominal wall hernia
For the Operative Surgery station, describe the Pfannenstiel approach in order: transverse suprapubic incision two fingerbreadths above the crest, catheter decompression of the bladder, midline linea alba split or rectus release, identification of the corona mortis, symphyseal plating, and secure rectus repair at closure — then know how to extend it into the modified Stoppa approach for acetabular fractures.