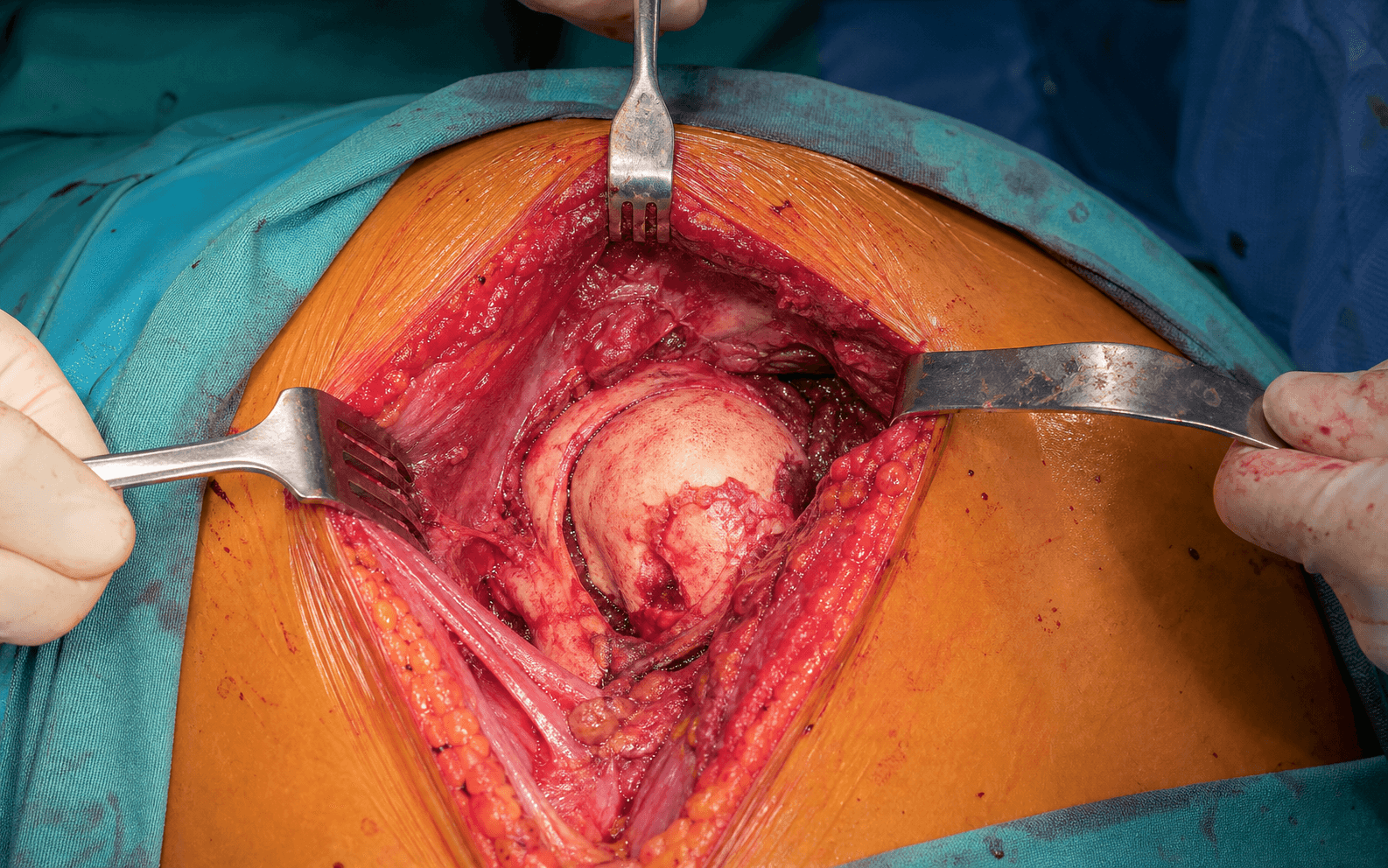
Proximal humerus fracture and glenohumeral arthritis · deltopectoral approach
- Indications: a 3-4 part proximal humerus fracture in the elderly (a declining indication versus reverse TSA), primary glenohumeral osteoarthritis with an intact cuff but glenoid bone loss unsuitable for an anatomic glenoid, and avascular necrosis of the humeral head with a preserved glenoid.
- The deltopectoral approach works the internervous plane between deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerves). The cephalic vein marks the interval and is retracted LATERAL with the deltoid to preserve the robust lateral tributaries and reduce thrombosis risk.
- Five critical danger structures: the axillary nerve (5-7 cm below the acromion), the musculocutaneous nerve (entering the conjoint tendon 5-8 cm from the coracoid), the cephalic vein, the anterior circumflex 'three sisters' at the inferior subscapularis border, and the posterior circumflex vessels travelling with the axillary nerve.
- Version is critical: 30-40 degrees of retroversion relative to the epicondylar axis. Excessive anteversion causes anterior instability, excessive retroversion causes posterior subluxation. Check before the cement sets - it cannot be revised after.
- In trauma, tuberosity healing is THE determinant of outcome - anatomic reduction with multiplanar fixation (GT-to-GT, cerclage to the shaft, sutures to the prosthesis). Long term, glenoid erosion develops in up to 50% by 5-10 years and may require conversion to an anatomic or reverse total shoulder arthroplasty.
When & Why
Indication. Shoulder hemiarthroplasty resurfaces the humeral side of the joint only, leaving the glenoid unresurfaced. It is chosen when the humeral head is irreparable but the glenoid either cannot or should not receive a component: - Trauma - an acute 3- or 4-part proximal humerus fracture in the elderly (older than 65-70 years) with a head-split pattern, severe comminution or a high AVN risk that makes ORIF unreliable; or a failed ORIF with humeral head collapse or AVN, articular incongruity, or a symptomatic malunion or nonunion. Note the modern trend toward reverse TSA for most elderly fracture cases.
- Elective - primary glenohumeral osteoarthritis with an intact rotator cuff but glenoid bone loss too severe for an anatomic glenoid component (or a patient who wishes to avoid one); avascular necrosis of the humeral head (Ficat stage 3-4) with a preserved glenoid; and selected rheumatoid arthritis with an intact cuff and severe humeral head destruction. Contraindications. Absolute: active infection (shoulder or systemic), neurologic dysfunction (axillary nerve palsy, complete brachial plexopathy), insufficient bone stock for component fixation, and medical comorbidities precluding surgery. Relative: rotator cuff deficiency (use reverse TSA), a young high-demand patient (anatomic or reverse TSA may be better long term), severe glenoid wear (which will progress), and likely non-compliance with rehabilitation. The one decision that matters - hemi versus reverse for fracture. Whatever the indication, the technique below is unchanged. The fracture decision is whether a hemi or a reverse is the better operation for an elderly 3- or 4-part fracture:
Elderly (older than 70-75), low demand, uncertain tuberosity healing. Better, more predictable function, tuberosity-independent, lower revision rate - at the cost of a higher dislocation and complication rate.
Younger patients (younger than 65-70) with good bone quality and a high likelihood of tuberosity healing, or concern that glenoid bone stock will not support a reverse baseplate.
Much younger patients with good bone and a simple fracture pattern only. In the elderly 4-part fracture the AVN, malunion and poor-function risk is high.
Pre-operative imaging and templating. Standard radiographs are a true AP (Grashey), a scapular Y and an axillary lateral. A CT is essential for fractures - to assess head-split, comminution, tuberosity displacement and glenoid involvement - and for elective cases to assess glenoid version and bone stock. MRI is added if AVN is suspected or to assess cuff integrity. Template the native humeral head (typically 42-50 mm), the canal diameter and the stem size, and note any varus or valgus deformity; avoid over-sizing in osteoporotic bone. Consent specifically for instability or dislocation, stiffness, tuberosity failure in trauma, axillary nerve injury, infection (1-2%), and the long-term glenoid erosion that drives revision (up to 50% by 5-10 years; revision rate 10-15% at 10 years, usually conversion to a reverse total shoulder). Setup. Beach-chair position with 70-80 degrees of head elevation, the entire shoulder, chest wall and arm to hand exposed, and the arm free-draped so it can be extended and rotated. General anaesthesia with an interscalene block, and IV cefazolin (or vancomycin if MRSA risk) within 60 minutes.
The Operation
The goal is to expose the glenohumeral joint through the deltopectoral approach, remove the destroyed humeral head while protecting the five danger structures, restore height, version and soft-tissue balance, and - in trauma - reconstitute the tuberosities anatomically around the stem. The exposure is the heart of the operation and is laid out in full as the first steps below.
Operative sequence
- Beach chair, 70-80 degrees of head elevation; arm free-draped to allow extension and rotation.
- Table break at the level of the scapula opens up the joint; head secured in a head holder.
- General anaesthesia with an interscalene block; IV cefazolin (or vancomycin if MRSA risk) within 60 minutes.
- Palpate the landmarks: the coracoid (the starting point), the deltopectoral groove, the acromion (mark the danger zone 5-7 cm below its lateral edge) and the clavicle.
- Incision from the coracoid process, 12-15 cm distally along the deltopectoral groove, aimed at the lateral border of the deltoid insertion.
- The groove is a palpable depression between the deltoid and pectoralis major bellies.
- Develop the interval bluntly down to the clavipectoral fascia.
- Identify the cephalic vein in the deltopectoral groove; it marks the internervous plane between deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerves).
- Retract it LATERAL with the deltoid: the lateral tributaries from deltoid are more robust, and keeping them intact reduces the risk of thrombosis.
- Ligate only if torn - ligation risks an arm DVT.
- Incise the clavipectoral fascia lateral to the conjoint tendon (coracobrachialis plus the short head of biceps).
- Self-retaining retractors: deltoid lateral, conjoint tendon medial.
- Protect the musculocutaneous nerve - it enters the conjoint tendon 5-8 cm distal to the coracoid (range 3-10 cm); avoid aggressive medial retraction.
- Identify the subscapularis (the large anterior cuff tendon to the lesser tuberosity), the rotator interval superiorly, and the long head of biceps in its groove.
- Trauma: the subscapularis is usually torn off with the lesser tuberosity fragment - identify and tag both tuberosity fragments with strong sutures (#2 FiberWire), preserving every soft-tissue attachment.
- Elective: either a subscapularis tenotomy 1 cm from the insertion, or a lesser-tuberosity osteotomy with a thin 5 mm collar of bone (better healing potential); tag with #2 FiberWire.
- Before completing the release, identify and ligate or cauterise the 'three sisters' - the anterior circumflex humeral vessels running horizontally along the inferior border of subscapularis - to prevent bleeding that obscures the field. They are a landmark for the axillary nerve, which lies just inferior.
- Release the anterior capsule from the glenoid rim and place stay sutures for later repair; open the rotator interval superiorly.
- Release inferiorly GENTLY - the axillary nerve lies 5-7 cm below the acromion and winds around the surgical neck with the posterior circumflex artery.
- Deliver the head with gentle external rotation, extension and adduction.
- Trauma: identify all four fragments (head, shaft, greater and lesser tuberosity) and assess head viability (no soft-tissue attachment means AVN risk). Elective: assess the head and glenoid cartilage.
- Trauma: remove the comminuted head fragments, preserving the tuberosities. Elective: anatomic-neck osteotomy at 130-135 degrees to the shaft in 30-40 degrees of retroversion; measure the resected head for sizing.
- Clear the canal, then ream sequentially (start small, increase to cortical chatter) and broach to cortical contact - avoid over-sizing, which fractures osteoporotic bone.
- With the trial stem assess three parameters: HEIGHT (restore native offset), VERSION (30-40 degrees of retroversion to the epicondylar axis - palpate the epicondyles with the elbow flexed 90 degrees), and SIZE (cortical contact without over-sizing).
- Select a head matching the native diameter (typically 42-50 mm), with standard or offset eccentricity.
- Reduce and assess STABILITY (translation in all directions - no excessive laxity), ROM (passive forward elevation 90-120 degrees, external rotation 30-40 degrees) and TENSION (snug, not overstuffed).
- Adjust head size, eccentricity or stem height until balanced: overstuffing causes stiffness and glenoid erosion; understuffing causes instability and cuff dysfunction.
- Cement the stem for osteoporotic trauma bone (immediate fixation); press-fit is suitable for good elective bone.
- If cementing: restrictor 2 cm beyond the tip, clean and dry the canal, retrograde fill, pressurise, insert at the correct version and depth, and hold stable until set (8-10 minutes).
- Insert at 30-40 degrees of retroversion and re-check BEFORE the cement sets - version cannot be revised afterwards. Attach the modular head to the Morse taper and confirm seating.
- Reduce the greater and lesser tuberosities anatomically around the prosthesis, 5-10 mm below the head articular surface.
- Three planes of fixation: GT-to-GT horizontal mattress with #5 Ethibond (restores the rotator cable), vertical cerclage of GT and LT to the shaft proximal to the stem, and sutures from the tuberosities through the prosthesis fins/holes.
- Confirm the tuberosities do not displace on passive ROM.
- Repair subscapularis with transosseous sutures through drill holes in the lesser tuberosity (#2 FiberWire, mattress), tied with the arm in neutral to slight internal rotation - snug, allowing 30-40 degrees of external rotation.
- Repair the capsule (stay sutures), perform a final ROM and stability check, irrigate copiously (6-9 L) and achieve haemostasis.
- Close the deltopectoral interval loosely (drainage, prevents haematoma), then subcutaneous and skin.
- Immobilise in a sling with the arm in INTERNAL ROTATION to protect the subscapularis and tuberosity repairs for 4-6 weeks.
Protect the axillary nerve by staying within 5 cm of the acromion and releasing the inferior capsule bluntly (it runs 5-7 cm below the acromion, at risk in inferior release and humeral neck osteotomy). Protect the musculocutaneous nerve with gentle conjoint retraction (it enters the conjoint 5-8 cm from the coracoid). Retract the cephalic vein lateral with the deltoid. Ligate the anterior circumflex 'three sisters' before subscapularis release. If bleeding appears during humeral manipulation, the posterior circumflex vessels - and therefore the axillary nerve alongside them - are close: handle the humerus gently and avoid circumferential neck dissection.
"The cephalic vein marks the deltopectoral interval. I retract it LATERAL with the deltoid - the lateral tributaries from deltoid are more robust than the medial ones from pectoralis, so keeping them intact reduces bleeding and the risk of an arm DVT if the vein has to be sacrificed." This lateral-versus-medial detail is a perennial viva question.
Humeral version must be confirmed at 30-40 degrees of retroversion to the epicondylar axis before the cement polymerises. Once set, the stem cannot be re-rotated short of revision. Excessive anteversion causes anterior instability; excessive retroversion causes posterior subluxation. Palpate the epicondyles with the elbow flexed 90 degrees as the reference.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 - Protection | 0-6 weeks | Sling in internal rotation (tuberosity healing needs 6-12 weeks in trauma) | Pendulums from day 1; PASSIVE ROM only (forward elevation to 90 degrees then 120 degrees, external rotation 20-30 degrees); no active shoulder motion | | 2 - Early active | 6-12 weeks | Removable sling (once subscapularis healed and tuberosities uniting) | Active-assisted ROM (6-8 weeks), active ROM (8-12 weeks), isometric strengthening (10-12 weeks) | | 3 - Strengthening | 12-24 weeks | None for light tasks | Progressive resistive exercises (Theraband, light weights); rotator-cuff and scapular-stabiliser work | | 4 - Return to function | 6-12 months | None | Unrestricted ADLs and low-demand recreation; permanent restriction on heavy labour and high-impact sport | Expected outcomes. Pain relief is excellent (80-90% good or excellent). ROM depends on the indication: trauma cases achieve roughly 90-120 degrees of forward elevation and 20-40 degrees of external rotation (governed by tuberosity healing), while elective cases reach 120-150 degrees of elevation and 40-60 degrees of external rotation when the cuff is intact. Strength is generally weaker than after anatomic or reverse TSA, especially in trauma. Implant survival is 85-90% at 10 years, with a 10-15% revision rate at 10 years - higher in trauma (tuberosity failure, conversion to reverse) and driven in elective cases by glenoid erosion. Complications
- Recognition
- Pain, weakness, limited active elevation and rotation; radiographs show greater-tuberosity migration more than 5 mm, nonunion at the tuberosity-shaft interface or bone resorption with superior migration and impingement
- Prevention
- Anatomic reduction with multiplanar fixation (GT-to-GT, cerclage, to prosthesis); tuberosities 5-10 mm below the head; 4-6 weeks of protection; plate augmentation if osteoporotic
- Management
- Non-operative if low demand and minimal symptoms; revision GT ORIF if bone stock is adequate, or conversion to reverse TSA if the cuff is incompetent (the usual choice beyond 6-12 months, as it does not rely on tuberosity healing)
- Recognition
- Acute pain, inability to move the arm, visible deformity; AP and axillary radiographs confirm; assess for an associated greater-tuberosity or glenoid fracture
- Prevention
- Secure transosseous subscapularis repair; correct version (30-40 degrees retroversion - excessive anteversion risks anterior instability); correct height and size; immobilise in internal rotation for 4-6 weeks
- Management
- Closed reduction under sedation (longitudinal traction, gentle manipulation) with post-reduction imaging; if recurrent, operate on the cause (subscapularis repair, revise version) or convert to reverse TSA if irreparable
- Recognition
- Limited passive and active ROM, pain at end-range, capsular pattern (external rotation more than elevation more than internal rotation); distinguish true stiffness from cuff dysfunction
- Prevention
- Avoid overstuffing (correct head size and height); early pendulums and passive ROM; adequate pain control; avoid over-tightening the subscapularis
- Management
- Aggressive physical therapy; manipulation under anaesthesia if within 6 months of surgery; arthroscopic or open capsular release if beyond 6 months and conservative care has failed; address overstuffing by revision if needed
- Recognition
- Progressive anterior and superior glenoid pain; radiographs show glenoid wear, subchondral sclerosis and cysts; CT quantifies bone loss; MRI assesses cuff integrity for revision planning
- Prevention
- Appropriate patient selection; anatomic component positioning (avoid overstuffing, correct version); balanced soft tissues; counsel on realistic expectations
- Management
- Non-operative (activity modification, NSAIDs, injections) if mild; operative conversion to anatomic TSA if the cuff is intact with adequate glenoid bone, or to reverse TSA if the cuff is deficient or bone is inadequate (more common); bone grafting may be needed
- Recognition
- Intra-operative: sudden loss of stability, a visible crack or palpable step-off; post-operative: pain after a fall, inability to use the arm; radiographs confirm the site and pattern
- Prevention
- Avoid over-sizing the stem (gentle sequential broaching); gentle technique in osteoporotic bone; cement if bone is poor; avoid excessive torque on insertion; fall-prevention advice
- Management
- Intra-operative: cerclage wires or cables proximal to the stem, consider a long stem and cement for immediate stability; post-operative: if the stem is stable, ORIF with plates or cables; if loose, revision to a longer stem with fixation; allograft or reverse TSA if bone loss is chronic
- Recognition
- Acute: fever, wound drainage, erythema, raised WCC, CRP and ESR; chronic: persistent pain, stiffness, wound issues, raised ESR or CRP; aspiration shows a positive culture, WCC more than 3000, PMN more than 80%
- Prevention
- Prophylactic IV cefazolin within 60 minutes; sterile technique; limit theatre traffic; meticulous haemostasis; optimise diabetes, nutrition and smoking
- Management
- Acute (within 4 weeks): irrigation and debridement with component retention if stable and long-term suppressive antibiotics; chronic: two-stage revision with an antibiotic spacer, 6-12 weeks of IV antibiotics, then reimplantation (often reverse TSA, which is more forgiving of soft tissues)
- Recognition
- Axillary: deltoid paralysis (cannot abduct) and lateral-arm sensory loss (regimental badge); musculocutaneous: weak elbow flexion and lateral-forearm sensory loss; EMG or NCS at 3-4 weeks confirms grade and severity
- Prevention
- Protect the axillary nerve (no dissection more than 5 cm below the acromion, gentle inferior retractor); protect the musculocutaneous nerve (no aggressive medial conjoint retraction); atraumatic technique
- Management
- Most are neurapraxias - observe for 3-6 months (up to 12-18 months for recovery) with therapy to prevent contractures; tendon transfers (e.g. trapezius for abduction) if no recovery by 12-18 months; neurolysis if the nerve is found compressed at surgery
- Recognition
- Restriction of motion; radiographs show new bone around the joint
- Prevention
- Indomethacin 25 mg three times daily for 6 weeks (if not contraindicated), or a single 700 cGy dose within 72 hours in high-risk patients (trauma, male, DISH, prior HO)
- Management
- Observation if mild; excision if severe and mature (beyond 12-18 months), with peri-operative prophylaxis
- Recognition
- Pain with activity; progressive radiographic lucency more than 2 mm
- Prevention
- Sound cement or press-fit technique; correct version and size
- Management
- Revision arthroplasty (anatomic or reverse TSA depending on cuff status)
- Recognition
- Weakness, limited active ROM with preserved passive ROM, positive lag signs
- Prevention
- Avoid overstuffing (which over-tensions the cuff); atraumatic handling
- Management
- Physical therapy for compensation; revision to reverse TSA if symptomatic and the cuff is irreparable
Viva & Exam Focus
SISTERSSISTERS - the three sisters at the inferior subscapularis border
VERSIONVERSION - humeral version determines stability
The five critical danger structures
Exits the quadrangular space with the posterior circumflex humeral artery, winds around the surgical neck, and runs 5-7 cm (range 3-9 cm) below the lateral acromion edge. At risk during inferior capsular release, humeral neck osteotomy, inferior retractor placement and circumferential neck dissection. Injury causes deltoid paralysis and regimental-badge sensory loss. Protect by staying within 5 cm of the acromion and a blunt, gentle inferior release.
Penetrates the conjoint tendon (coracobrachialis) 5-8 cm distal to the coracoid tip but is highly variable (3-10 cm). At risk with aggressive medial retraction of the conjoint tendon or dissection medial to it. Injury causes weak elbow flexion and lateral-forearm sensory loss. Protect with gentle conjoint retraction and no medial dissection.
A branch from the third part of the axillary artery, running horizontally along the inferior border of subscapularis, typically three small arteries. Ligate or cauterise BEFORE subscapularis release to prevent bleeding that obscures the field. They are a landmark for the axillary nerve, which lies just inferior.
Runs in the deltopectoral groove and marks the interval; lateral tributaries drain the deltoid, medial tributaries the pectoralis. Retract it LATERAL with the deltoid to preserve the robust lateral tributaries and reduce thrombosis risk. Avoid ligation, which risks an arm DVT.
Travel with the axillary nerve through the quadrangular space and wind around the surgical neck posteriorly. Bleeding during humeral manipulation indicates the axillary nerve is near - handle the humerus gently and avoid circumferential neck dissection.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old woman presents 3 days after a fall with a 4-part proximal humerus fracture. She lives alone and was previously independent. Walk me through your decision-making between hemiarthroplasty and reverse total shoulder replacement.”
“You are performing a hemiarthroplasty via the deltopectoral approach. Describe the critical neurovascular structures at risk and how you protect each one.”
“What are the key technical factors that determine the outcome of hemiarthroplasty, and what are the long-term problems you counsel patients about?”
Indications
- Trauma: 3-4 part proximal humerus fracture in the elderly (reverse TSA increasingly preferred); hemi reserved for younger patients (younger than 65-70) with good bone
- Elective: primary glenohumeral OA with intact cuff but glenoid bone loss unsuitable for an anatomic glenoid, AVN with a preserved glenoid, selected rheumatoid arthritis
- Contraindications: active infection, cuff deficiency (use reverse TSA), severe glenoid wear, neurologic dysfunction, insufficient bone stock
Key anatomy and danger zones
- Axillary nerve: 5-7 cm below the lateral acromion, winds around the surgical neck with the posterior circumflex artery - protect during inferior release and humeral neck osteotomy
- Musculocutaneous nerve: enters the conjoint 5-8 cm from the coracoid (variable 3-10 cm) - avoid aggressive medial conjoint retraction
- Cephalic vein: in the deltopectoral groove - retract LATERAL with the deltoid (preserves lateral tributaries, reduces DVT risk)
- Anterior circumflex 'three sisters': at the inferior subscapularis border - ligate BEFORE subscapularis release; landmark for the axillary nerve
- Posterior circumflex vessels: travel with the axillary nerve - bleeding during humeral manipulation signals the nerve is near
Critical steps
- Approach: deltopectoral incision from the coracoid 12-15 cm distally; cephalic vein retracted LATERAL; incise clavipectoral fascia; deltoid lateral, conjoint medial
- Subscapularis: trauma - tag torn fragments; elective - tenotomy versus lesser-tuberosity osteotomy, tag with #2 FiberWire; ligate the three sisters FIRST
- Exposure: release the anterior capsule with stay sutures; deliver the head with external rotation, extension and adduction
- Humeral preparation: ream and broach sequentially; trial stem - assess HEIGHT, VERSION (30-40 degrees retroversion), SIZE
- Trialing: head 42-50 mm typically; check STABILITY, ROM and TENSION (snug, not overstuffed)
- Implantation: cement for osteoporotic trauma, press-fit for good bone; version 30-40 degrees retroversion - check before cement sets
- Tuberosity repair (trauma): anatomic GT and LT reduction; GT-to-GT (#5 Ethibond, restores the rotator cable), vertical cerclage to the shaft, sutures to the prosthesis; tuberosities 5-10 mm below the head
- Subscapularis repair: transosseous #2 FiberWire through the lesser tuberosity, arm in neutral to slight internal rotation; allow 30-40 degrees of external rotation
- Closure: repair the capsule; final ROM and stability check; copious irrigation; close the deltopectoral interval loosely; sling in INTERNAL ROTATION for 4-6 weeks
Technical pearls
- Version is critical: 30-40 degrees of retroversion to the epicondyles; check before the cement hardens
- Height: overstuffing causes stiffness and glenoid erosion; understuffing causes instability and cuff dysfunction
- Size: avoid over-sizing the stem (iatrogenic fracture in osteoporotic bone); sequential broaching to cortical contact
- Tuberosity healing (trauma): THE determinant of outcome - multiplanar fixation is essential
- Subscapularis repair: critical for anterior stability; failure causes dislocation
Complications and management
- Tuberosity malunion or nonunion (trauma): most common cause of a poor result; revision ORIF if early, conversion to reverse TSA if late and cuff-incompetent
- Instability (anterior dislocation): subscapularis failure, malversion; closed reduction, address the cause, consider reverse TSA if recurrent
- Stiffness: especially in trauma; physical therapy, MUA if within 6 months, capsular release if beyond 6 months
- Glenoid erosion (long-term): up to 50% by 5-10 years; convert to anatomic TSA (cuff intact) or reverse TSA (cuff deficient)
- Periprosthetic fracture: over-sizing in osteoporotic bone; ORIF if stem stable, revision to a long stem if loose
- Nerve injury (axillary most common, 5-8%): most are neurapraxia - observe 3-6 months; tendon transfers if no recovery by 12-18 months
Post-operative protocol
- Phase 1 (0-6 weeks): sling in internal rotation; pendulums from day 1; PASSIVE ROM only
- Phase 2 (6-12 weeks): active-assisted ROM 6-8 weeks, active ROM 8-12 weeks, isometrics 10-12 weeks
- Phase 3 (12-24 weeks): progressive resistive exercises; cuff and scapular strengthening
- Phase 4 (6-12 months): return to ADLs and low-demand recreation; permanent restriction on heavy labour
- Fracture cases progress more slowly; tuberosity healing (6-12 weeks) governs advancement
Outcomes and exam tips
- Pain relief: excellent (80-90%)
- ROM: trauma 90-120 degrees elevation and 20-40 degrees external rotation; elective 120-150 degrees elevation and 40-60 degrees external rotation
- Survivorship: 85-90% at 10 years; revision 10-15% at 10 years
- Reverse TSA is now preferred over hemi for elderly fractures - candidates who advocate hemi as first-line will fail
- Know the danger-zone distances: axillary nerve 5-7 cm below the acromion, musculocutaneous nerve 5-8 cm from the coracoid
Background & Evidence
Epidemiology. Proximal humerus fractures are among the most common osteoporotic fragility fractures, typically sustained as a low-energy fall in the elderly, and they are the basis for most fracture hemiarthroplasties. For elective glenohumeral osteoarthritis, hemiarthroplasty has been progressively displaced by anatomic and reverse total shoulder arthroplasty and is now reserved for the specific situations where a glenoid component is not feasible - inadequate glenoid bone stock, or a very young patient in whom glenoid loosening is a concern. Why hemiarthroplasty fails long term. Hemiarthroplasty resurfaces only the humerus, leaving the glenoid cartilage to articulate against a metal or ceramic head. Because the prosthetic head is far harder than native glenoid cartilage, eccentric and imbalanced loading progressively erodes the glenoid - the central long-term problem, evident radiographically in up to 50% of patients by 5-10 years. In trauma the separate problem is biological: the outcome hinges not on the implant but on whether the reattached tuberosities heal, which is unreliable in elderly osteoporotic bone.
- Hemiarthroplasty
- OA with glenoid bone loss and intact cuff; selected 3-4 part fracture in younger patients
- Anatomic TSA
- Elective OA with intact cuff and adequate glenoid
- Reverse TSA
- Elderly 3-4 part fracture; cuff-deficient arthropathy; revision
- Hemiarthroplasty
- Not resurfaced (erosion risk)
- Anatomic TSA
- Resurfaced (glenoid component)
- Reverse TSA
- Resurfaced (glenosphere)
- Hemiarthroplasty
- Requires an intact cuff
- Anatomic TSA
- Requires an intact cuff
- Reverse TSA
- Not required
- Hemiarthroplasty
- Critical - determines outcome
- Anatomic TSA
- Not applicable (elective)
- Reverse TSA
- Not dependent
- Hemiarthroplasty
- Glenoid erosion (up to 50% by 5-10 years)
- Anatomic TSA
- Glenoid loosening
- Reverse TSA
- Scapular notching; instability
- Hemiarthroplasty
- 93% stemmed (Nordic registry, OA)
- Anatomic TSA
- 96% (Nordic registry, OA)
- Reverse TSA
- Lowest revision of the three for fracture
Key evidence. Boileau's multicentre series of fracture-sequelae arthroplasties (2001) showed that greater-tuberosity osteotomy was the single factor most strongly associated with a poor outcome - establishing the central principle that anatomic tuberosity healing, not the implant, governs function. The same group's later fracture-stem study (Boileau, 2013) found anatomic tuberosity healing in 87% with a fracture-specific stem versus 45% with a conventional stem, with age 75 or older, female sex and a bulky stem predicting failure - a key argument for reverse arthroplasty in elderly women. Namdari's systematic review (2013) showed reverse arthroplasty gave function independent of tuberosity healing but at roughly four times the odds of a complication. For elective OA, Rispoli's 11-year follow-up (2006) documented progressive glenoid erosion driving a high revision rate, and the Nordic registry study (Rasmussen, 2018) confirmed lower survivorship for hemiarthroplasty than anatomic TSA (93% versus 96% at 10 years). Together this evidence explains why hemiarthroplasty has been displaced by anatomic TSA for elective OA and by reverse TSA for elderly fractures.
References
Shoulder arthroplasty for the sequelae of fractures of the proximal humerus
- Multicentre series of 71 fracture-sequelae shoulder arthroplasties; proposed a 4-type classification (cephalic collapse or necrosis, locked dislocation, surgical-neck nonunion, severe tuberosity malunion)
- Greater-tuberosity osteotomy was the single most significant factor associated with poor outcome (P less than.005)
- ALL excellent or good Constant scores occurred in types 1 and 2 (no GT osteotomy); ALL type 3 and 4 patients (who needed GT osteotomy) had fair or poor results and failed to regain active elevation above 90 degrees
Can surgeons predict what makes a good hemiarthroplasty for fracture?
- 61 shoulders with 3- and 4-part fractures; anatomic greater-tuberosity healing was achieved in 87% with a fracture-specific stem versus 45% with a conventional stem (P =.0001)
- Fracture stems gave significantly better active forward elevation (136 vs 113 degrees), external rotation (34 vs 23 degrees) and Constant score (68 vs 58; P less than.0001)
- Independent risk factors for tuberosity failure and poor function were age 75 years or older, female sex, and use of a bulky conventional stem
Comparison of hemiarthroplasty and reverse arthroplasty for proximal humeral fractures: a systematic review
- Systematic review of 14 studies comparing reverse arthroplasty with fracture-specific hemiarthroplasty for proximal humeral fractures
- Frequency-weighted Constant, ASES and range-of-motion outcomes were similar between groups when tuberosities healed
- Reverse arthroplasty carried roughly 4.0 times higher odds of a postoperative complication than hemiarthroplasty
Humeral head replacement for the treatment of osteoarthritis
- 51 humeral head replacements for primary OA followed a mean of 11.3 years; significant long-term pain relief and ROM gains overall (P less than.0001)
- Progressive glenoid erosion developed by a mean of 10.7 years (P less than.0001); 9 of 10 revisions were for painful glenoid arthrosis
- By the modified Neer rating, 21 of 51 results were unsatisfactory, with a high revision rate
Anatomical total shoulder arthroplasty has higher survival than hemiarthroplasty for glenohumeral OA: a Nordic registry study
- Pooled Danish, Norwegian and Swedish registry data (n greater than 5800 arthroplasties for OA)
- 10-year cumulative survival was 0.96 for anatomic TSA, 0.93 for stemmed hemiarthroplasty and 0.85 for resurfacing hemiarthroplasty (P less than 0.001)
- Resurfacing hemiarthroplasty had 2.5 times and stemmed hemiarthroplasty 1.4 times the revision risk of TSA; survival was lower for all implants in patients under 55
Reverse shoulder arthroplasty for the treatment of proximal humeral fractures in older adults: a systematic review
- Systematic review demonstrating superior outcomes of reverse TSA compared with hemiarthroplasty for proximal humeral fractures in older adults
Revision of failed shoulder arthroplasty for glenohumeral arthritis
- Comprehensive review of revision shoulder arthroplasty, including the management of glenoid erosion after hemiarthroplasty
Late prosthetic shoulder arthroplasty for displaced proximal humerus fractures
- Classic paper on tuberosity management in fracture hemiarthroplasty, establishing the principles of anatomic reduction and secure fixation
Outcome after primary hemiarthroplasty for fracture of the head of the humerus
- Long-term outcomes showing inferior results of hemiarthroplasty for fractures compared with elective indications
Reverse shoulder prosthesis for acute four-part fracture: tuberosity fixation using a horseshoe graft
- Technical article on reverse TSA for acute fractures with a tuberosity fixation technique, representing the modern approach to complex fractures