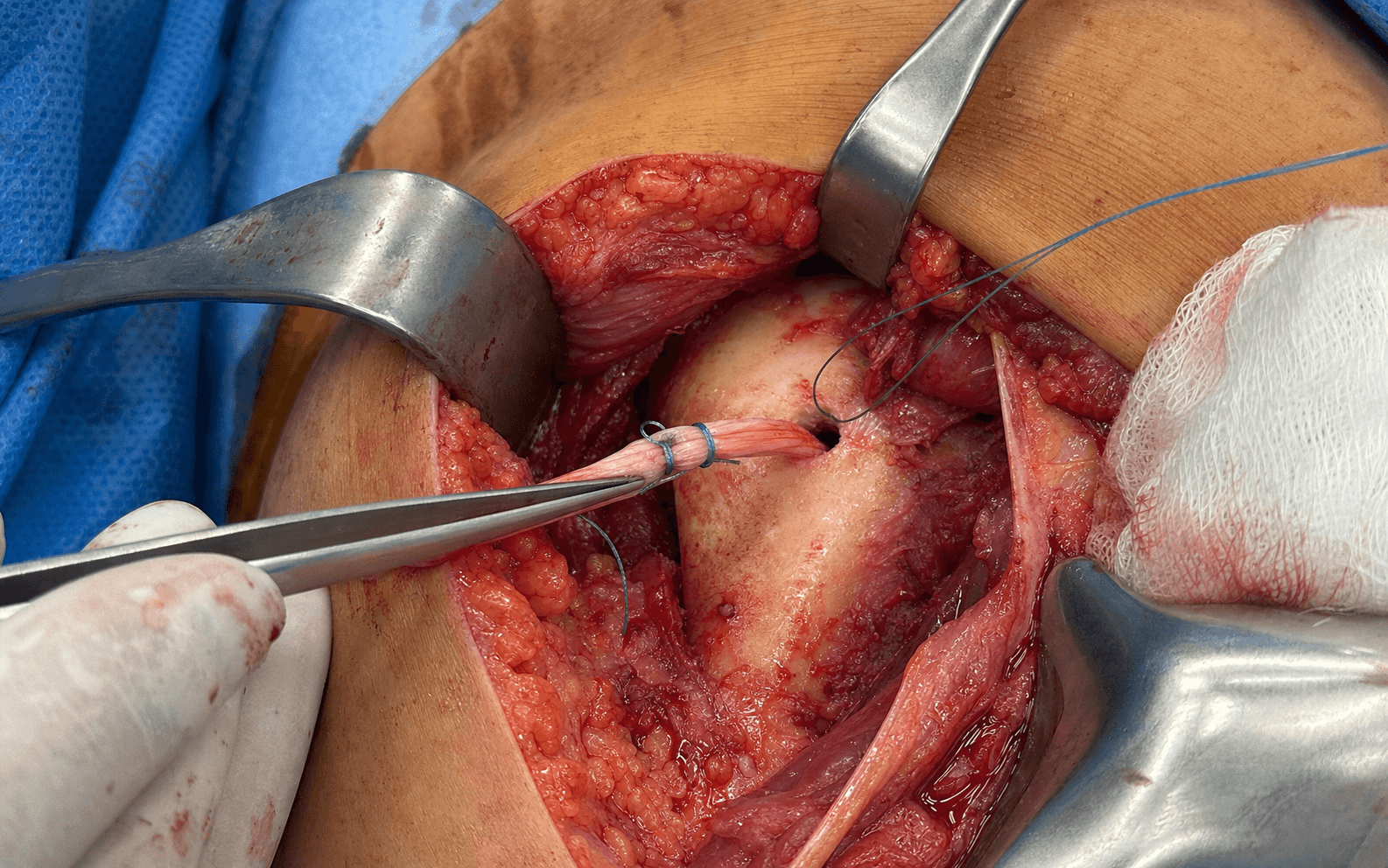
Open subpectoral tenodesis of the long head of biceps — the axillary-fold approach that removes the entire diseased intra-groove tendon and restores anatomic length-tension
- The subpectoral approach removes the entire intra-groove diseased tendon segment that suprapectoral techniques leave behind — this eliminates residual bicipital groove pain, the common cause of failed proximal tenodesis.
- The incision lies in the axillary fold, deep to the inferior border of pectoralis major. The musculocutaneous nerve lies 3-5 cm medial to the tenodesis site; the axillary nerve is 2-3 cm superior to the inferior pectoralis major border and must be protected during retraction.
- Fixation restores the anatomic length-tension relationship — the tendon is tensioned so that with the arm at the side in neutral rotation the superior border of the biceps muscle belly lies at the inferior border of the pectoralis major insertion.
- An interference screw (7-8 mm) provides the strongest initial fixation; a cortical button or suture anchors are acceptable alternatives. Humeral tunnel diameter must not exceed 8 mm to minimise fracture risk through the anterior cortex.
- “Subpectoral tenodesis is indicated when the patient wants to avoid the Popeye deformity and cramping that occur in 30-50 percent of tenotomies, particularly in younger or active patients.
- “The musculocutaneous nerve is at risk during medial retraction — keep retractors lateral and avoid excessive medial force; nerve injury causes biceps weakness and lateral forearm sensory loss.
- “Length-tension mismatch is the most common technical error — too short causes over-tensioning and pain; too long causes residual groove symptoms and cosmetic deformity.
- “Always debride the bicipital groove thoroughly — residual groove synovitis or osteophytes are the leading cause of persistent anterior shoulder pain after a technically correct tenodesis.
When & Why
Indication. Symptomatic long head of biceps tendinopathy — anterior shoulder pain, a tender bicipital groove, and a positive Speed or Yergason test — with one of the following, that has failed non-operative care (3-6 months of activity modification, NSAIDs, and at least one corticosteroid injection into the groove): - Biceps instability or subluxation from the bicipital groove (medial subluxation over the lesser tuberosity on dynamic ultrasound or MRI)
- A partial-thickness tear of greater than 25-50 percent of tendon diameter with persistent pain
- A SLAP tear type II or IV in a patient older than 40 years, where repair is unlikely to succeed and tenodesis is preferred
- A failed proximal (suprapectoral or arthroscopic) tenodesis with residual groove pain The one decision that matters — tenodesis versus tenotomy. Both relieve pain equivalently; the choice turns on cosmesis, cramping, and patient demand:
Preferred in patients younger than 60, heavy labourers, overhead athletes, and anyone who wants to avoid a cosmetic deformity. It reduces the Popeye deformity rate to less than 5 percent and activity-related cramping to less than 10 percent, with pain relief and function scores equivalent to tenotomy.
Acceptable in older, lower-demand patients who accept the 30-50 percent risk of a Popeye deformity and the 20-40 percent risk of activity-related cramping. Simpler and faster, with equivalent pain relief.
Contraindications. Absolute: active infection in the shoulder or axilla; inability to comply with the postoperative sling and rehabilitation. Relative: severe glenohumeral osteoarthritis where arthroplasty is indicated (consider concomitant tenodesis at arthroplasty); poor bone quality precluding secure fixation (consider alternative fixation or tenotomy). Consent specifically for nerve injury (musculocutaneous, axillary, radial — less than 1 percent each), humeral fracture through the tunnel (about 1 percent), fixation failure (2-4 percent), residual groove pain (3-6 percent), infection (less than 1 percent), and cosmetic dissatisfaction from a length-tension mismatch. Setup. Beach-chair position with the arm in slight abduction and neutral rotation on a padded arm board; the shoulder is prepped and draped to allow free movement (a sterile tourniquet is not required). General anaesthesia with an interscalene block for postoperative analgesia, plus local infiltration with 0.25 percent bupivacaine with epinephrine along the incision for vasoconstriction.
The Operation
The goal: through a short axillary-fold incision below the inferior border of pectoralis major, develop the plane between pectoralis major and the short head of biceps, protect the three nerves at risk, deliver and resect the entire diseased intra-groove tendon, debride the groove, and refix the tendon to the humerus at an anatomic length-tension with a 7-8 mm interference screw (or a cortical button or suture anchors). The exposure is laid out in the first three steps — it is the heart of the operation.
Operative sequence
- Beach-chair, arm in slight abduction and neutral rotation on a padded board; interscalene block and local infiltration.
- Palpate the inferior border of pectoralis major — the key landmark. It inserts on the lateral lip of the bicipital groove and its inferior border defines the axillary-fold incision.
- Plan a 4-5 cm incision in the axillary fold, centred on that inferior border. The deltoid inserts laterally and is not violated.
- Make the 4-5 cm axillary-fold incision and incise skin and subcutaneous fat; control the subcutaneous veins to avoid troublesome bleeding.
- Identify the inferior border of pectoralis major and develop the plane between pectoralis major and the short head of biceps by blunt dissection.
- Retract pectoralis major superiorly with a Hohmann retractor placed on the humeral shaft just inferior to the groove. Keep retractors lateral to the short head of biceps.
- Protect the musculocutaneous nerve medially — it pierces coracobrachialis 3-5 cm medial to the tenodesis site and is usually not visualised; it is protected by limiting medial retraction to the minimum.
- Protect the axillary nerve superiorly — it rounds the surgical neck 2-3 cm above the inferior pectoralis major border. Stay strictly inferior to that border and avoid superior retraction.
- Protect the radial nerve and profunda brachii — they lie in the spiral groove about 2-3 cm deep to the anterior cortex. They are protected later by staying anterior and using a drill stop during tunnel creation.
- Identify the bicipital groove by palpation and open the groove sheath longitudinally.
- Identify the long head of biceps tendon, release any remaining groove attachments, and deliver the entire intra-groove segment into the wound.
- Resect the intra-articular and groove portions, leaving a 2-3 cm stump for tenodesis. Delivering every millimetre of diseased groove tendon is the whole point of the subpectoral approach.
- After the tendon is out, thoroughly debride the groove of residual synovitis and any osteophytes.
- This step is critical — residual groove synovitis or osteophytes are the leading cause of persistent anterior shoulder pain after an otherwise correct tenodesis.
- Centre the tunnel on the anterior cortex at the inferior border of the bicipital groove.
- Drill a unicortical 7-8 mm tunnel perpendicular to the cortex to a depth of 15-20 mm, using a drill stop to prevent posterior cortical penetration.
- Clear the tunnel of debris. If using a cortical button, create a second smaller hole about 1 cm distal for button passage — placed far enough away to avoid a stress riser.
- With the arm at the side in neutral rotation, mark the tendon so the superior border of the biceps muscle belly will lie at the inferior border of pectoralis major — the anatomic resting-length landmark.
- Fix the tendon to that mark using the chosen method, then visually confirm the muscle-belly position before final fixation.
- Interference screw (preferred): whipstitch the tendon end, seat it in the tunnel to the mark, and advance a 7-8 mm PEEK or bioabsorbable screw alongside it until flush. Cortical button: pass and flip the button on the posterior cortex, tension to the mark, tie over the button. Dual suture anchors: place 2.9-3.5 mm anchors proximal and distal and secure with mattress sutures.
- Irrigate, confirm haemostasis, and close the subcutaneous layer with absorbable suture.
- Close skin with a running subcuticular absorbable suture or interrupted nylon.
- Apply a sterile dressing and place the arm in a sling.
The radial nerve and profunda brachii artery lie in the spiral groove about 2-3 cm deep to the anterior cortex. Before drilling, set a drill stop at 18-20 mm and keep the trajectory perpendicular to the anterior cortex. If the posterior cortex is breached, stop immediately: inspect for brisk bleeding or a neurological deficit. If the field is dry and the nerve is intact, switch to an alternative fixation method (cortical button or suture anchors) that does not need full tunnel depth; if there is uncontrolled bleeding or a deficit, extend the approach to explore and protect the radial nerve.
With the arm at the side in neutral rotation, mark the tendon so the superior border of the biceps muscle belly sits exactly at the inferior pectoralis major border, and confirm the position visually after fixation. Over-tensioning is the most common technical error and produces anterior shoulder pain that is difficult to salvage without revision.
Deliver the entire diseased intra-groove tendon into the wound and resect it — leaving even 1 cm behind defeats the purpose of the subpectoral approach. Then thoroughly debride the groove of synovitis and osteophytes; this is the step that eliminates residual groove pain.
Centre the tunnel exactly at the inferior groove border and keep the diameter to 7-8 mm. A larger or eccentric tunnel creates a stress riser and is the strongest predictor of a postoperative humeral fracture. Use a drill stop set at 18-20 mm and confirm no posterior cortical penetration by direct inspection.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 — Protection | 0-4 weeks | Sling at all times except hygiene | Pendulum exercises from day 1; no active elbow flexion or supination against resistance | | 2 — Early motion | 4-8 weeks | Sling discontinued | Active-assisted elbow flexion and supination; gentle shoulder ROM; no lifting greater than 2 kg | | 3 — Strengthening | 8-12 weeks | None | Progressive resistance (theraband, 1-2 kg); return to light desk work | | 4 — Return to activity | 12-24 weeks | None | Gradual return to full activity; heavy labour or overhead sport at 4-6 months when strength reaches 80 percent of the other side | Rehabilitation pearls:
- Early active elbow flexion is the most common cause of fixation failure — protect it for 4 weeks.
- Length-tension mismatch pain typically presents at 6-12 weeks, when strengthening begins.
- Persistent groove pain at 3 months warrants a groove injection before considering revision. Complications
- Incidence
- less than 1%
- Recognition
- Biceps and elbow-flexion weakness, lateral forearm sensory loss
- Prevention and management
- Limit medial retraction force and duration; identify the nerve if dissection goes medial to the short head. Observe for neurapraxia; explore if no recovery by 3 months
- Incidence
- less than 1%
- Recognition
- Deltoid paralysis, lateral shoulder numbness, weak abduction
- Prevention and management
- Stay inferior to the pectoralis major border; avoid superior retraction. Observe; explore if no recovery by 3 months
- Incidence
- less than 0.5%
- Recognition
- Wrist drop, first dorsal web space sensory loss, brisk posterior bleeding
- Prevention and management
- Direct visualisation during drilling; drill stop; avoid posterior cortical penetration. Explore and repair immediately if recognised intraoperatively
- Incidence
- 1-2%
- Recognition
- Sudden pain and deformity 6-12 weeks postoperatively, often after minor trauma
- Prevention and management
- Limit the tunnel to 7-8 mm; centre it; consider prophylactic cerclage in osteopenic bone. Manage with ORIF and bone graft as needed
- Incidence
- 2-4%
- Recognition
- Sudden pop, loss of biceps contour, Popeye deformity, weakness
- Prevention and management
- Anatomic length-tension; secure screw purchase; avoid early active flexion. Revise with an alternative fixation method
- Incidence
- 3-6%
- Recognition
- Persistent anterior shoulder pain despite a technically correct tenodesis
- Prevention and management
- Thorough groove debridement; remove the entire intra-groove tendon. Revise to subpectoral if not already done; groove injection or neurolysis if it has
- Incidence
- 5-10%
- Recognition
- Over-tensioned: high-riding muscle belly, anterior pain; under-tensioned: residual groove symptoms, cosmetic deformity
- Prevention and management
- Use the pectoralis major inferior border landmark; confirm before final fixation. Revise the tenodesis with correct tensioning
- Incidence
- less than 1%
- Recognition
- Erythema, warmth, drainage, raised CRP
- Prevention and management
- Sterile technique; perioperative antibiotics. Washout, IV antibiotics, culture-directed therapy
Viva & Exam Focus
TENODESISOperative sequence — open subpectoral biceps tenodesis
NERVESSubpectoral tenodesis danger zones
Critical danger structures
Emerges from the lateral cord 5-8 cm distal to the coracoid and pierces coracobrachialis 3-5 cm medial to the tenodesis site, then continues as the lateral cutaneous nerve of the forearm. Excessive medial retraction or blind medial dissection can stretch or lacerate it, causing biceps and elbow-flexion weakness with lateral forearm sensory loss. Protect it by limiting medial retraction, using blunt retractors, and identifying the nerve if dissection extends medial to the short head of biceps.
Courses around the surgical neck of the humerus 2-3 cm superior to the inferior border of the pectoralis major insertion, deep to the deltoid fascia. Superior retraction of pectoralis major or aggressive superior dissection places it at risk, causing deltoid paralysis and lateral shoulder numbness. Identify the inferior border of pectoralis major and stay below it; do not place retractors superior to the tenodesis site without direct visualisation.
The radial nerve and profunda brachii artery lie in the spiral groove on the posterior humerus, about 2-3 cm medial and deep to the tenodesis site with the arm in neutral rotation. A drill that penetrates the posterior cortex can injure them; radial nerve injury produces wrist drop and sensory loss in the first dorsal web space. Maintain direct visualisation during drilling, use a drill stop, and avoid medial retraction beyond the short head of biceps.
The anterior humeral cortex at the inferior border of the bicipital groove is the weakest point after tunnel creation. A tunnel diameter greater than 8 mm, eccentric placement, or a cortical-button hole acting as a stress riser markedly increases fracture risk; postoperative fracture typically occurs through the tunnel within 6-12 weeks. Limit the tunnel to 7-8 mm, centre it, and consider prophylactic cerclage with a cortical button in osteopenic bone.
Placing the tenodesis too proximal (a short tendon) over-tensions the muscle belly, which sits high and hurts; placing it too distal (a long tendon) leaves residual groove symptoms and a cosmetic Popeye appearance. With the arm adducted at the side in neutral rotation, the superior border of the biceps muscle belly should lie exactly at the inferior border of the pectoralis major insertion. Mark the tendon at the planned level before cutting and confirm the position after fixation.
Suprapectoral tenodesis leaves 3-5 cm of diseased intra-groove tendon that keeps generating pain; subpectoral tenodesis removes the entire segment. Studies show 20-30 percent of proximal-tenodesis patients have persistent groove pain needing revision, and subpectoral revision resolves symptoms in greater than 85 percent. After tendon release, deliver the entire intra-groove portion into the wound, resect it, and thoroughly debride the groove of synovitis and osteophytes before fixation.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 48-year-old manual labourer presents with 9 months of anterior shoulder pain and a palpable click in the bicipital groove. MRI shows partial tearing of the long head of biceps with medial subluxation. He has failed two corticosteroid injections. How do you counsel him regarding tenodesis versus tenotomy and which technique do you recommend?”
“You are performing a subpectoral biceps tenodesis. After creating the 8 mm humeral tunnel you notice the drill has penetrated the posterior cortex. What do you do and how do you prevent this complication in the future?”
“A 52-year-old patient is 4 months after subpectoral biceps tenodesis with an interference screw. He has excellent pain relief but complains that his biceps muscle looks 'too high' and feels tight with overhead activity. What is the diagnosis and how do you manage it?”
Indications
- Symptomatic LHB tendinopathy or instability refractory to 3-6 months of non-operative care
- Partial tears greater than 25-50 percent diameter
- SLAP tears type II/IV in patients older than 40 years
- Failed proximal tenodesis with residual groove pain
- Patient preference to avoid Popeye deformity (younger, active, labourer)
Tenodesis versus tenotomy
- Tenodesis: less than 5 percent Popeye, less than 10 percent cramping, equivalent pain and function
- Tenotomy: 30-50 percent Popeye, 20-40 percent cramping, acceptable in older low-demand patients
- Subpectoral removes the entire intra-groove tendon; suprapectoral leaves 3-5 cm diseased
- Residual groove pain: 3-6 percent subpectoral versus 20-30 percent suprapectoral
Danger zones
- Musculocutaneous nerve: 3-5 cm medial; limit medial retraction
- Axillary nerve: 2-3 cm superior to the pec major border; stay inferior
- Radial nerve and profunda brachii: 2-3 cm deep in the spiral groove
- Length-tension: muscle-belly border at pec major inferior border, arm at side
- Tunnel: 7-8 mm maximum; greater than 8 mm markedly increases fracture risk
Operative sequence
- Axillary-fold incision over the inferior pec major border
- Protect musculocutaneous (medial) and axillary (superior) nerves
- Deliver and resect the entire intra-groove tendon; debride the groove
- 7-8 mm unicortical tunnel centred at the inferior groove border, with a drill stop
- Set length-tension at the pec major landmark before final fixation
- Interference screw (preferred), cortical button, or dual anchors
Complications
- Nerve injury (musculocutaneous, axillary, radial): less than 1 percent each
- Humeral fracture through tunnel: 1-2 percent
- Fixation failure: 2-4 percent; protect active elbow flexion for 4 weeks
- Residual groove pain: 3-6 percent; thorough groove debridement prevents it
- Length-tension mismatch: 5-10 percent; the most common cause of dissatisfaction
Rehabilitation
- Weeks 0-4: sling, pendulum only, no active elbow flexion against resistance
- Weeks 4-8: active-assisted elbow flexion, gentle shoulder ROM, no lifting greater than 2 kg
- Weeks 8-12: progressive resistance, return to light work
- Weeks 12-24: gradual return to activity; heavy labour or sport at 4-6 months
Background & Evidence
Tenodesis versus tenotomy. Multiple Level I and II studies show that tenodesis provides superior cosmesis and lower cramping rates with pain relief and function equivalent to tenotomy. A 2023 meta-analysis of 12 RCTs found no difference in Constant or ASES scores but a 40 percent absolute risk reduction in Popeye deformity with tenodesis. Subpectoral versus suprapectoral tenodesis. Subpectoral tenodesis removes the entire intra-groove diseased segment, whereas suprapectoral techniques leave 3-5 cm of tendon in the groove. A 2022 prospective cohort showed 25 percent of suprapectoral patients required revision for residual groove pain versus 4 percent after subpectoral tenodesis, and subpectoral revision resolved symptoms in 87 percent of cases. This consistent message — that the residual intra-groove tendon is the source of persistent anterior pain — is why subpectoral is the preferred technique and a perennial viva point. Fixation method. Interference screw fixation provides the highest load-to-failure in biomechanical studies (greater than 200 N). Cortical button and dual suture-anchor techniques are biomechanically acceptable (150-180 N) and carry a lower risk of tunnel fracture. Clinical outcomes are equivalent across methods when length-tension is restored, so the fixation choice is secondary to accurate tensioning and groove debridement.
- Tenodesis
- less than 5%
- Tenotomy
- 30-50%
- Tenodesis
- less than 10%
- Tenotomy
- 20-40%
- Tenodesis
- Equivalent
- Tenotomy
- Equivalent
- Tenodesis
- Equivalent
- Tenotomy
- Equivalent
- Tenodesis
- 3-6%
- Tenotomy
- 2-4% (for deformity)
- Tenodesis
- Higher in active patients
- Tenotomy
- Acceptable in low demand
Relevant surgical anatomy. The long head of biceps originates from the supraglenoid tubercle and superior labrum, courses intra-articularly, then enters the bicipital groove beneath the transverse humeral ligament. The intra-groove segment (3-5 cm) is the common site of tendinopathy, partial tearing and instability; it is extrasynovial and supplied by branches of the anterior humeral circumflex artery. The pectoralis major inserts on the lateral lip of the groove, and its inferior border is the surface landmark for both the incision and the length-tension reference. The deltoid inserts laterally and is not violated.
References
Biceps tenodesis versus tenotomy: a systematic review and meta-analysis of level I randomized controlled trials
- Meta-analysis of 12 RCTs, 892 patients comparing tenodesis versus tenotomy
- No difference in pain scores, ASES, or Constant scores at minimum 2-year follow-up
- Tenodesis reduced Popeye deformity from 42 percent to 4 percent (absolute risk reduction 38 percent)
Complications associated with subpectoral biceps tenodesis: low rates of incidence following surgery
- Retrospective review of 353 subpectoral tenodesis procedures with minimum 2-year follow-up
- Overall complication rate 7.3 percent; humeral fracture through tunnel occurred in 1.1 percent
- Revision rate 4.5 percent, most commonly for residual groove pain or fixation failure
Open subpectoral biceps tenodesis in patients over 65 does not result in an increased rate of complications
- Retrospective review comparing open subpectoral tenodesis outcomes in patients over 65 versus younger patients
- No increase in complication rates observed in the older patient cohort
- Supports safety of subpectoral tenodesis in active patients older than 65 years
All-suture anchor and unicortical button show comparable biomechanical properties for onlay subpectoral biceps tenodesis
- Cadaveric biomechanical comparison of all-suture anchor versus unicortical button fixation for onlay subpectoral tenodesis
- Both constructs demonstrated comparable ultimate load to failure and cyclic displacement
- Provides evidence supporting either fixation method for subpectoral tenodesis