A muscle-sparing arthrotomy for primary TKA that passes under vastus medialis obliquus, preserving the extensor mechanism and its nerve supply for the fastest quadriceps recovery of any TKA approach — at the cost of limited exposure in selected cases.
- Definition: The subvastus (Southern) approach is a muscle-sparing TKA arthrotomy that passes UNDER the vastus medialis obliquus (VMO), elevating it subperiosteally from the medial tibia WITHOUT cutting through muscle fibres or the quadriceps tendon.
- Why it is muscle-sparing: The VMO is swept up and laterally off the medial tibial periosteum in a loose areolar plane, so its fibres and its nerve supply are both preserved — preserving extensor-mechanism integrity.
- Fastest quadriceps recovery of all TKA approaches: earlier straight-leg raise than medial parapatellar (controlled data about 3 vs 4 days; older series quote 2-3 days vs up to a week or more) and earlier early flexion.
- Key limitation — limited exposure: a 10-20 percent learning-curve conversion rate to medial parapatellar when exposure is inadequate; difficult in obese patients (BMI greater than 35), stiff knees (flexion less than 70 degrees), muscular patients and severe deformity (greater than 20 degrees).
- Best indications: straightforward primary TKA in thin patients (BMI under 30), good preoperative ROM (flexion at least 90 degrees), minimal deformity (less than 15 degrees), younger active patients prioritising rapid recovery.
- Contraindications: revision TKA, obesity (BMI greater than 35), knee stiffness (flexion less than 70 degrees), severe deformity (greater than 20 degrees), prior open surgery with scarring, and any need for extensive soft-tissue releases.
When & Why
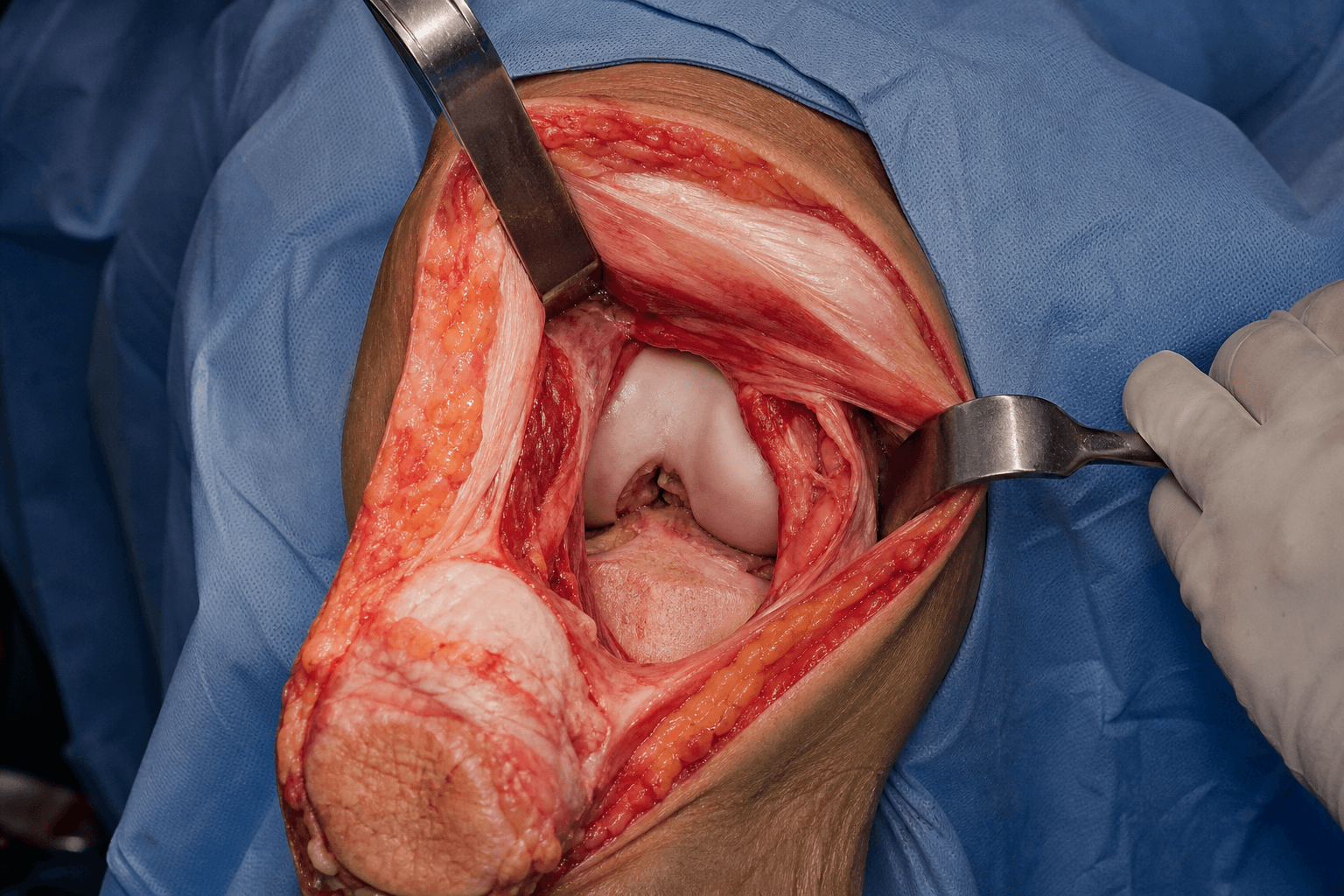
What it exposes. The subvastus approach delivers the knee joint for primary total knee arthroplasty — the distal femur, proximal tibia, both femoral condyles and the patellofemoral joint — through an arthrotomy that runs deep to the vastus medialis obliquus rather than through it. Why subvastus (and not medial parapatellar). The medial parapatellar arthrotomy remains the worldwide default because of its versatility and excellent exposure. The subvastus approach trades a degree of exposure for an intact extensor mechanism: because the VMO is elevated and not cut, patients recover quadriceps control faster, reach straight-leg raise earlier, track the patella better, and have less early postoperative pain. The functional gains are real but concentrated in the first weeks and largely attenuate by 3 to 6 months, so subvastus is best framed as a tool for selected fast-track patients, not a routine replacement.
- Subvastus
- None — VMO elevated, not cut
- Medial parapatellar
- Through vastus medialis and medial retinaculum
- Subvastus
- Limited (adequate for straightforward cases)
- Medial parapatellar
- Excellent (gold standard)
- Subvastus
- Narrow (thin, good ROM, minimal deformity)
- Medial parapatellar
- Broad (all primary TKAs)
- Subvastus
- About 2-3 days
- Medial parapatellar
- About 7-10 days
- Subvastus
- Faster, 6-8 weeks to baseline
- Medial parapatellar
- Slower, 12-16 weeks to baseline
- Subvastus
- Better (VMO preserved)
- Medial parapatellar
- Good but VMO disrupted
- Subvastus
- 2-5 percent
- Medial parapatellar
- 5-10 percent
- Subvastus
- Steep (limited exposure)
- Medial parapatellar
- Standard (taught in residency)
- Subvastus
- 10-20 percent convert to medial parapatellar
- Medial parapatellar
- Not applicable (standard approach)
- Subvastus
- Contraindicated (inadequate exposure)
- Medial parapatellar
- Standard approach
Ideal candidate. BMI under 30, preoperative flexion at least 90 degrees, minimal deformity (varus or valgus under 15 degrees), no significant flexion contracture (under 10 degrees), primary osteoarthritis, and a patient who wants the fastest possible recovery. Poor candidate. Obese (BMI greater than 30), stiff knee (flexion under 90 degrees), severe deformity requiring releases, inflammatory arthritis with fragile bone, or a muscular/athletic build with a thick VMO that makes the dissection difficult. Absolute contraindications. Revision TKA (inadequate exposure), previous open knee surgery with scarring, and any need for extensive ligament releases or balancing. Patella baja, short stature and a thick muscular build are relative contraindications because they make patellar eversion difficult. Position & landmarks. Supine on a standard table with a small ipsilateral hip bump (optional) and a side post at thigh level that lets the knee flex to 90 degrees — flexion aids VMO visualisation and is essential to this approach. Pad the post carefully to avoid peroneal nerve compression. A proximal-thigh tourniquet gives a bloodless field for identifying the VMO fibres and the areolar plane; deflate before closure for haemostasis. Palpate and mark the patella, the medial femoral epicondyle, the adductor tubercle (superior to the epicondyle), the tibial tubercle (the distal/anterior reference), and the medial joint line about 1 cm distal to the medial epicondyle.
Subvastus is a specialised technique for straightforward primary TKA in favourable anatomy. Examiners test your understanding of the specific contraindications and of when to convert to medial parapatellar — not the incision itself.
The Exposure
The exposure works down to the VMO, then develops the subvastus plane — the interval UNDER (deep to) the VMO muscle belly and the medial tibial periosteum — and sweeps the intact muscle proximally and laterally to reveal the medial capsule. The whole point is that no quadriceps fibres are cut.
Exposure sequence
- A midline or slightly medial incision, 5-6 cm proximal to the superior pole of the patella, running to the tibial tubercle (or 2 cm distal), 10-15 cm long — similar in length to a medial parapatellar incision.
- Sharp through skin and subcutaneous tissue with electrocautery haemostasis; identify and protect the saphenous nerve and vein if encountered on the medial side.
- Develop a medial flap to expose the medial border of the patella and the VMO muscle belly medially, tracing the oblique fibres to their distal insertion.
- Palpate the VMO belly on the medial thigh and follow its oblique fibres (about 50-55 degrees to the femoral long axis) distally toward the patella.
- The key step: identify the interval UNDER (deep to) the VMO — the plane between the VMO muscle belly and the medial tibial periosteum, palpated through the muscle.
- Make a small fascial incision at the distal VMO and develop the plane with blunt dissection. If the elevator slides easily through loose areolar tissue, you are in the correct plane.
- Begin at the medial aspect of the tibial tubercle and elevate periosteum from the medial tibial metaphysis, working proximally and posteriorly under the VMO.
- Bluntly sweep the VMO muscle belly laterally and proximally, off the tibial periosteum, without cutting any fibres.
- Proximal limit: superior pole of the patella. Posterior limit: the posteromedial capsule (superficial MCL fibres). Distal limit: the tibial tubercle.
- Place a narrow retractor deep to the VMO and retract it laterally, creating the VMO "dome" above the joint.
- Incise the medial capsule and retinaculum, starting proximally and extending distally to the tibial tubercle. Stay medial — do not compromise the VMO insertion on the patella.
- Flex the knee to 90 degrees and gently evert the patella laterally. This is harder than in a medial parapatellar because the VMO is intact; never force it (VMO avulsion risk).
- If exposure is inadequate: extend the capsular incision more proximally, use lamina spreaders, or remove obstructing osteophytes — and convert early rather than force (see Dangers & Extensions).
- With the joint open, visualise the femoral condyles, access the tibial plateau, and remove bone spurs to improve exposure.
- Standard TKA cuts follow: proximal tibial resection (extramedullary or intramedullary guide), intramedullary femoral referencing with distal, anterior, posterior and chamfer cuts, sizing/rotation assessment, then flexion-extension gap balancing, trial reduction, patellar resurfacing as planned, and cementing of final components.
- Re-approximate the medial capsule and retinaculum with a number-1 absorbable suture to a watertight closure.
- Let the VMO fall back into its anatomic position — no sutures are placed through VMO muscle, because it was elevated, not cut.
- Close the fascia over the VMO with 2-0 absorbable suture to eliminate dead space, then 2-0 Vicryl in subcutaneous tissue and 3-0 Monocryl or staples for skin. Consider an intra-articular drain, removed when output is less than 30 mL per shift.
The subvastus plane is UNDER the VMO muscle belly. If you find yourself cutting muscle fibres with bleeding and resistance, you are in the wrong (intramuscular) plane — the correct plane has loose areolar tissue and minimal resistance. Limited exposure is the Achilles heel of this approach (a 10-20 percent learning-curve conversion rate). Have a low threshold to convert to a medial parapatellar arthrotomy if you cannot evert the patella, cannot see the posterior femoral condyles or lateral compartment, or feel you are forcing the exposure. Convert EARLY, before bone cuts — better to switch approaches than avulse the VMO or compromise component positioning.
Because the VMO was elevated and never divided, closure needs no muscle repair — the VMO simply falls back into position and the fascia is closed over it. If you are suturing VMO fibres at closure, the approach was no longer truly subvastus.
Dangers & Extensions
Critical anatomy: the VMO neurovascular pedicle. The nerve to VMO is a distal branch of the femoral nerve that descends within the adductor (subsartorial / Hunter's) canal and enters the muscle on its deep, proximal surface. It runs with the descending genicular artery (a branch of the superficial femoral artery arising in the canal) as a proximal neurovascular pedicle. Because the pedicle enters the muscle proximally, distal subperiosteal elevation of the VMO off the medial femur and tibia leaves its supply intact — injury comes from excessive PROXIMAL dissection into the muscle substance or aggressive proximal extension of the arthrotomy, not from distal elevation. Structures at risk, by layer
- Structure at risk
- Saphenous nerve and vein (medial side)
- Protection
- Develop the medial flap in the correct plane; identify and protect if encountered
- Structure at risk
- VMO fibres — tearing or avulsion from forced eversion or poor subperiosteal technique
- Protection
- Stay in the loose-areolar subperiosteal plane; gentle retraction; never force patellar eversion
- Structure at risk
- Nerve to VMO and descending genicular artery (enter proximally from the adductor canal)
- Protection
- Elevate distally and subperiosteally; limit proximal dissection to the superior pole of the patella
- Structure at risk
- Popliteal vessels (posterior to the joint)
- Protection
- Standard anterior work keeps them at safe distance; not at risk in routine subvastus
When to convert to medial parapatellar. Limited exposure is the most common problem (10-20 percent in the early learning curve). Convert early — during the exposure phase, before bone cuts — if any of these apply:
Low threshold to convert when exposure is inadequate:
- Cannot evert the patella despite proper VMO elevation
- Cannot visualise the posterior femoral condyles or access the lateral compartment
- Patient anatomy (obese, muscular, stiff) limits instrument placement
- Severe deformity requiring extensive soft-tissue releases Damage risks if you force exposure instead: VMO avulsion (losing the muscle-sparing benefit), descending genicular artery injury (compromising VMO blood and nerve supply), and inadequate bone resection (component malposition, instability, early failure). Make the conversion decision EARLY — converting after bone cuts is difficult.
Complications.
- Inadequate exposure — 10-20 percent (learning-curve dependent); managed by extending the capsular incision, lamina spreaders, or conversion.
- VMO muscle damage — fibre tearing or tibial avulsion from forced eversion or poor technique; repair if torn, or complete as medial parapatellar if extensive.
- VMO nerve injury — under 1 percent, from excessive dissection into the VMO substance; results in denervation and loss of terminal extension strength.
- Quadriceps dysfunction (paradoxical) — despite muscle-sparing, from nerve injury, muscle trauma or pain inhibition; managed with aggressive physiotherapy.
- Wound complications — similar to medial parapatellar (haematoma 2-5 percent, superficial infection under 1 percent, deep infection under 1 percent).
- Extensor lag — 2-5 percent (vs 5-10 percent medial parapatellar); preserved VMO lowers the risk.
- Knee stiffness — 3-5 percent; manipulation under anaesthesia at 6-12 weeks if severe.
- Component malposition — no different from medial parapatellar, but harder to assess landmarks with limited exposure; surgeon experience is critical. Extensile options. Exposure can be improved within the approach by extending the capsular incision proximally and using lamina spreaders. If still inadequate, the approach converts to a medial parapatellar by formally incising through the VMO/medial retinaculum — the standard rescue. Subvastus does not extend usefully for revision work.
Procedures Through This Approach
- Primary total knee arthroplasty — the principal operation, in selected straightforward cases (CR or PS components based on PCL integrity; standard instrumentation, with thicker polyethylene options available).
- Mini-subvastus TKA — the same subperiosteal VMO elevation performed through a shorter incision and without patellar eversion, for fast-track recovery.
- Bilateral staged TKA — subvastus on the first knee to speed rehab and improve function before the second side. Subvastus is not used for revision TKA, complex deformity correction, or cases needing extensive soft-tissue releases — those go through a medial parapatellar or extensile approach.
Pair a subvastus approach with a motor-sparing adductor canal block, not a femoral nerve block — a femoral block blunts the very quadriceps recovery the approach is meant to deliver. Standard antibiotic prophylaxis (a weight-adjusted first-generation cephalosporin, e.g. cefazolin 2 g IV, 3 g if over 120 kg, within 60 minutes of incision) is independent of the arthrotomy chosen. Early recovery milestones (the practical payoff of an intact extensor mechanism): straight-leg raise by day 1-2 (achievable in 2-3 days vs 7-10 with medial parapatellar), weight-bearing as tolerated from day 1, passive ROM to 90 degrees by week 1 and 0-110 degrees by 6 weeks, driving at 4-6 weeks, light labour at 8-12 weeks, and full activities at 12-16 weeks.
Viva & Exam Focus
SUBVASTUSSUBVASTUS — patient selection
VMOVMO — the critical anatomy
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 65-year-old woman (BMI 27) with primary knee OA needs a TKA. She has 95 degrees of flexion, minimal varus (5 degrees), and wants the fastest possible recovery, asking about a 'muscle-sparing' approach. Is she a candidate for subvastus, and how would you perform it?”
“During VMO elevation for a subvastus TKA you dissect INTO the muscle belly instead of staying subperiosteal, with fibre tearing and bleeding. What went wrong technically, and what are your options?”
Decision points
- Reserve subvastus for straightforward primary TKA in thin patients with good ROM and minimal deformity
- Ideal candidate: BMI under 30, flexion at least 90 degrees, minimal deformity, primary OA
- Contraindications: revision TKA, obesity (BMI greater than 35), stiff knee (flexion less than 70), severe deformity, prior scarring, extensive releases needed
- Convert to medial parapatellar if exposure is inadequate (10-20 percent conversion rate)
Technique
- Subvastus plane is UNDER the VMO — elevate the muscle off the tibial periosteum, do not cut through it
- Blunt dissection in loose areolar tissue between VMO and tibia (minimal resistance = correct plane)
- Protect the VMO pedicle (nerve to VMO plus descending genicular vessels) entering proximally from the adductor canal — elevate distally and stay subperiosteal
- Limited exposure — use lamina spreaders, extend the capsular incision, or convert; never force patellar eversion
- Closure: the VMO is not sutured (it was elevated, not cut) — it falls back naturally; close the fascia over it
Critical anatomy
- Nerve to VMO: a femoral branch descending in the adductor (subsartorial) canal, entering the muscle on its deep proximal surface
- Descending genicular artery: from the superficial femoral artery in the canal, running with the nerve as a proximal pedicle
- VMO fibres run obliquely (about 50-55 degrees to the femoral long axis) to the medial patella and retinaculum
- VMO origin: medial lip of the linea aspera and adductor magnus tendon; function: terminal 15 degrees of extension and patellar stabilisation
- Saphenous nerve and vein run subcutaneously on the medial side
Complications
- Inadequate exposure (10-20 percent) — the most common problem
- VMO fibre tearing or avulsion from forced eversion or poor technique
- VMO nerve injury (under 1 percent) from excessive proximal dissection
- Extensor lag 2-5 percent (vs 5-10 percent medial parapatellar); knee stiffness 3-5 percent
- Wound: haematoma 2-5 percent, superficial and deep infection each under 1 percent
Must-know numbers
- Straight-leg raise: about 2-3 days (subvastus) vs 7-10 days (medial parapatellar)
- Quadriceps recovery: 6-8 weeks vs 12-16 weeks to baseline
- Extensor lag: 2-5 percent (subvastus) vs 5-10 percent (medial parapatellar)
- Conversion to medial parapatellar: 10-20 percent (learning-curve dependent)
- Analgesia: adductor canal block (motor-sparing), NOT a femoral nerve block
References
Guidelines, Registries & Global Practice Global practice pattern. The medial parapatellar arthrotomy remains the default approach for primary TKA worldwide because of its versatility and excellent exposure. The subvastus (and mini-subvastus) approach is used selectively by arthroplasty surgeons internationally as an extensor-mechanism-sparing option within enhanced-recovery (fast-track) pathways, reserved for thin patients with good preoperative range of motion and minimal deformity. Its uptake is limited chiefly by a steep learning curve and restricted exposure in obese, muscular, stiff or severely deformed knees. Major joint registries. National arthroplasty registries do not generally stratify revision risk by surgical arthrotomy (parapatellar vs subvastus vs midvastus), so there is no registry-level signal that the subvastus approach changes implant survivorship. The key registry-level message for vivas: the choice of arthrotomy is an early-recovery decision, not an implant-survival decision.
- Region
- United Kingdom
- Relevant signal
- Arthrotomy not routinely coded; primary TKA tracked by implant, fixation and constraint
- Region
- United States
- Relevant signal
- Approach is not a standard reported field; outcomes reported by implant and patient factors
- Region
- Australia and New Zealand
- Relevant signal
- Tracks implant survivorship; arthrotomy type is not a registry variable
- Region
- Sweden
- Relevant signal
- Long-running TKA data; revision driven by implant, infection and instability, not arthrotomy
Society guidance and consensus. AAOS (US), NICE and BOA (UK), AO Foundation and EFORT (Europe) do not mandate a specific arthrotomy for primary TKA; approach selection is left to surgeon judgement and patient anatomy. Enhanced-recovery (ERAS) consensus statements endorse quadriceps-sparing approaches and motor-sparing analgesia as components of fast-track care where they suit the patient. Antibiotic prophylaxis — a single weight-adjusted dose of a first-generation cephalosporin (e.g. cefazolin 2 g IV, 3 g if over 120 kg) within 60 minutes of incision, with a glycopeptide where MRSA-colonised or beta-lactam-allergic — is independent of the arthrotomy chosen. Across all settings, when a subvastus approach is used to accelerate quadriceps recovery, a motor-sparing adductor canal block is preferred over a femoral nerve block, which would blunt the very quadriceps recovery the approach is intended to deliver. Practical global take. The functional advantages of the subvastus approach (earlier straight-leg raise, earlier flexion, less lateral release, lower early pain) are real but concentrated in the first weeks and attenuate by 3 to 6 months. It is best framed globally as a tool for selected fast-track patients rather than a routine replacement for the medial parapatellar approach.
Subvastus (Southern) Approach for Primary Total Knee Arthroplasty
- Modern re-introduction and detailed anatomical description of the subvastus (Southern) approach for primary TKA (originally described in 1929)
- Preserves the integrity of the extensor mechanism and maintains the vascular supply to the patella
- Emphasises that a complete understanding of the medial neurovascular anatomy is essential to perform the approach safely
- Positioned the subvastus approach as a valuable extensor-mechanism-sparing alternative to the standard medial parapatellar arthrotomy
Mini-subvastus Versus Medial Parapatellar Approach in Total Knee Arthroplasty
- Prospective observer-blinded study, 120 matched patients (mini-subvastus without patellar eversion vs standard medial parapatellar with eversion)
- Mini-subvastus reached active straight-leg raise earlier (3.2 vs 4.1 days) and 90 degrees flexion earlier (2.8 vs 4.5 days)
- Mini-subvastus lost on average 100 mL less blood and had lower day-one pain (VAS 2.4 vs 3.89)
- Trade-offs: technically more demanding, tourniquet time longer by about 15 minutes, with two intraoperative complications; component geometry and limb alignment were good in both groups
Systematic Review of Medial Parapatellar and Subvastus Approaches in Total Knee Arthroplasty
- Systematic review of five comparative studies (published 1993-2001) meeting quality inclusion standards
- Methodological quality of included studies was generally poor and too heterogeneous for meta-analysis
- Insufficient evidence to demonstrate a clinically or statistically significant difference between subvastus and medial parapatellar approaches across outcomes
- Called for higher-quality trials with objective functional outcomes and follow-up beyond 6 to 12 months
A Meta-analysis of the Subvastus Approach and Medial Parapatellar Approach in Total Knee Arthroplasty
- Meta-analysis of 10 randomized/quasi-randomized trials, 976 knees
- Subvastus required significantly less lateral retinacular release (RR 0.37; 95 percent CI 0.17-0.81)
- Subvastus offered earlier straight-leg raise and superior knee flexion within the first postoperative week
- No increase in operative duration with the subvastus approach in the pooled analysis
Subvastus Approach Supporting Fast-Track TKA Over the Medial Parapatellar Approach: A Systematic Review and Network Meta-analysis
- Network meta-analysis of 33 randomized controlled trials comparing TKA surgical approaches
- Subvastus and mini-subvastus ranked best for early range-of-motion improvement (days 1, 3, 4 and 6) versus medial parapatellar
- Mini-subvastus gave significantly lower early pain scores (days 1, 3 and 7) and the best early Knee Society Scores
- All between-approach differences attenuated with time — benefits are concentrated in the early postoperative period