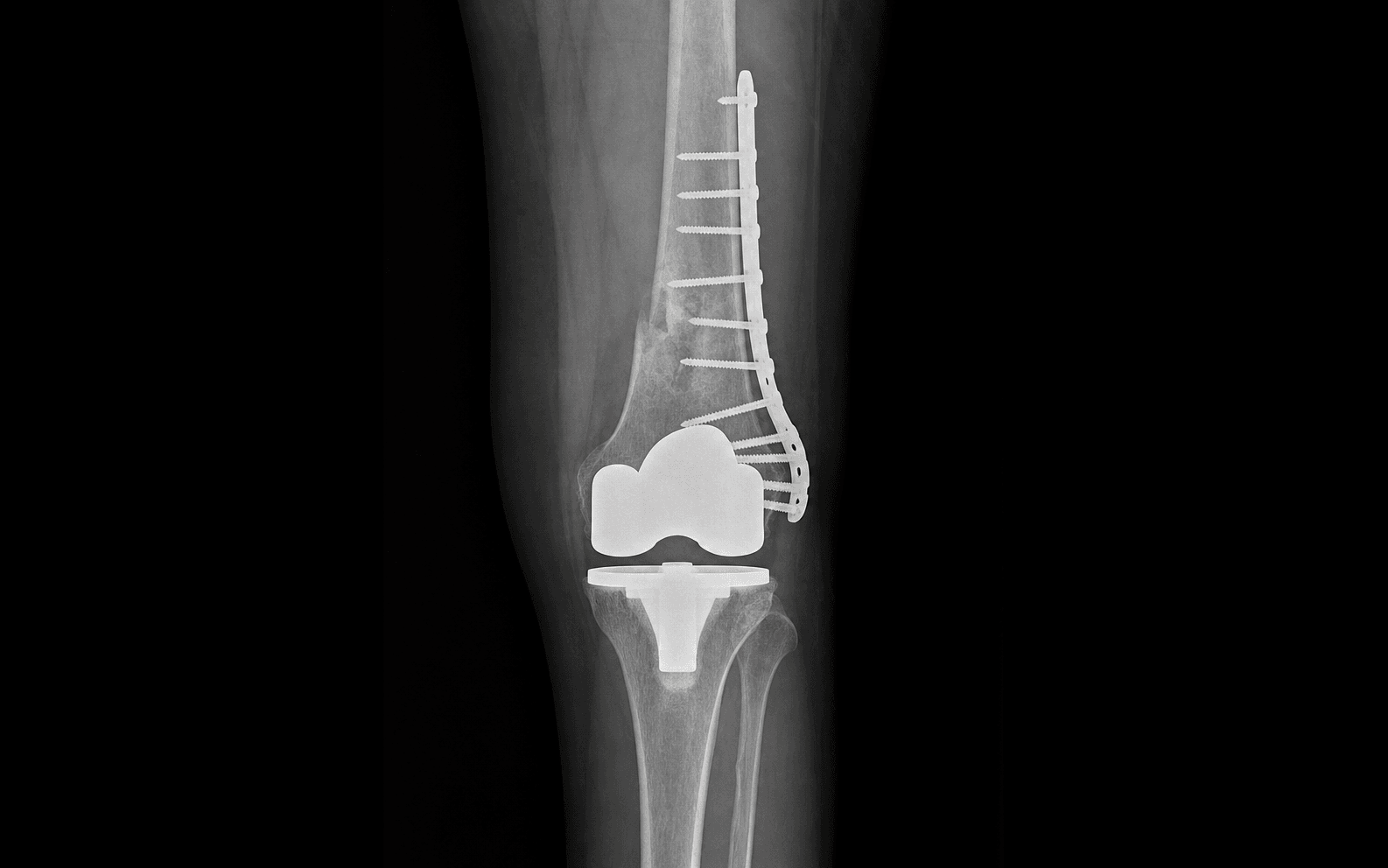
Lateral approach to the distal femur for a fracture above or around a TKR femoral component. Fixation of osteoporotic bone with limited distal screw options; component stability decides ORIF versus revision.
- Rorabeck Type II — a displaced fracture with a STABLE femoral component — is the classic indication for ORIF with a long lateral locking plate.
- Component stability is the single critical assessment: a loose component (Rorabeck Type III) treated with ORIF alone fails in more than 80 percent of cases and needs revision arthroplasty.
- The TKR femoral component blocks posterior screw paths. Use an anterior-to-posterior trajectory for distal screws, and accept unicortical or short bicortical purchase.
- Use a LONG plate — at least 10 to 12 cortices (5 to 6 screws) proximal to the fracture — to distribute load across osteoporotic bone. A short construct is a common, avoidable cause of failure.
- Protect the fixation with touch-down or partial (20 to 30 kg) weight-bearing for around 12 weeks; these fractures heal slowly (4 to 6 months) in elderly osteoporotic bone.
When & Why
Indication. A displaced supracondylar or distal femoral fracture above or around a stable total knee replacement femoral component — Lewis and Rorabeck Type II — that has no prospect of conservative management. Most are low-energy falls in an elderly patient (typically 70 to 85 years) with osteoporotic bone. The decision rests on one variable — is the femoral component stable? Everything flows from this single assessment:
A conservative trial is reasonable: a hinged knee brace and touch-down weight-bearing with weekly X-rays. Convert to ORIF at the first sign of displacement. Realistic only in a low-demand, compliant patient.
ORIF with a long lateral locking plate is the standard operation and the commonest indication — good outcomes if adequate fixation is achieved.
Revision arthroplasty is mandatory (long-stem revision TKR or a distal femoral replacement). ORIF alone fails in more than 80 percent of cases.
ORIF or distal femoral replacement (DFR)? Even with a stable component, a DFR is a strong alternative in the very elderly, severely osteoporotic, low-demand patient with comminuted metaphyseal bone where plate fixation is likely to fail. DFR allows early weight-bearing and removes the fixation-failure risk, at the cost of higher medical morbidity. Pre-operatively, counsel for both possibilities so you can convert intra-operatively if the bone is worse than expected. Retrograde nail as an alternative. When the distal fragment is adequate (about 5 to 6 cm), the canal is not blocked by a long cement stem, and comminution is minimal, a retrograde nail is equivalent to a locking plate. It is rarely possible in the periprosthetic setting because the component box and cement stem usually obstruct the entry point. Assess the whole patient, not just the film. Three domains: patient (age, comorbidities, pre-fracture mobility, bone quality, cognition, social support), fracture (displacement, comminution, bone stock, location relative to the component), and prosthesis (type, stability, cement mantle, age of implant, reason for the original TKR). Consent specifically for fixation failure (10 to 20 percent), non-union (10 to 15 percent), deep infection near the TKR (2 to 5 percent, potentially catastrophic), malrotation, restricted weight-bearing for about three months, slow healing, and a small chance of needing conversion to a DFR if fixation is inadequate. One-year mortality is 5 to 10 percent — these are fragile patients.
The Operation
The goal: expose the distal femur laterally, confirm the component is stable, reduce the fracture gently onto a long bridging lateral locking plate, and fix it with robust proximal purchase and carefully aimed distal screws that avoid the component and the popliteal vessels. The lateral exposure is laid out in full below.
Operative sequence
- Supine on a radiolucent table; small folded-towel bump under the ipsilateral hip to control external rotation; sandbag lateral to the thigh for stability.
- Contralateral leg in a leg holder so you can compare length and rotation.
- Free-drape from iliac crest to toes.
- C-arm from the contralateral side; confirm AP, lateral, hip and knee views of the WHOLE femur and the TKR BEFORE draping.
- Thigh tourniquet available but used cautiously in the elderly (PVD common); if used, keep it under 90 minutes, or rely on meticulous haemostasis.
- Consider tranexamic acid (1 g IV at induction, 1 g at 3 hours) — elderly patients on anticoagulation bleed significantly.
- Assess the previous TKR scar (usually midline or medial parapatellar) and the skin quality — elderly skin is thin and atrophic.
- Option 1 (common): extend the existing midline/medial scar proximally, curving laterally over the distal femur — single incision, familiar anatomy.
- Option 2 (if skin is fragile): a separate lateral incision parallel to the femur, keeping a skin bridge greater than 7 to 10 cm from the old scar to protect perfusion.
- Typical lateral incision: from about 10 to 15 cm above the fracture down to the lateral epicondyle or joint line (around 20 to 30 cm), centred over the lateral femur with the iliotibial band (ITB) as the palpable landmark.
- Sharp single-pass skin incision — elderly skin tears easily, handle it gently.
- Meticulous haemostasis of superficial vessels; expect scar tissue from the previous TKR.
- Palpate the ITB (a thick fascial band on the lateral thigh) and split it longitudinally in line with its fibres for the length needed for plate application.
- Ligate the lateral superior genicular vessels if encountered distally.
- Elevate vastus lateralis ANTERIORLY off the lateral intermuscular septum to create the submuscular plane the plate will sit in.
- In the elderly with a prior TKR, expect the muscle to be atrophic, thin and scarred to the femur — use sharp dissection through scar and preserve what muscle is present.
- Blunt dissection along the periosteum proximally and distally; minimise stripping to preserve fracture biology.
- Exposure goals: 10 to 15 cm proximal to the fracture for plate length, a clear fracture zone for reduction, and distal access to the femoral component level to test stability and plan distal screws.
- Evacuate the haematoma (save it if using a biological MIPO technique).
- Minimal periosteal stripping — preserve the blood supply.
- Identify the major fragments (usually two, with variable metaphyseal comminution) and assess bone quality.
- The critical bone-stock decision: if cortices are genuinely "eggshell" so that screw purchase is futile, plate fixation will fail — convert to a DFR (discussed with the patient pre-op).
- Inspect the cement-bone interface directly if the component is exposed; look for lucency or gross motion.
- Apply varus and valgus stress to the knee while palpating the component and fracture site; any component motion means loosening.
- Image during stress testing and compare with pre-operative films.
- If the component is LOOSE (Rorabeck Type III): STOP. ORIF alone will fail. Convert to revision arthroplasty (preferred), ORIF plus simultaneous component revision (experienced surgeon only), or — if the patient cannot tolerate revision — accept a high failure risk and counsel the family.
- If STABLE: proceed to ORIF. Note the component position, because it blocks posterior screw paths distally.
- Osteoporotic bone fragments with force: the "do not crush the egg" principle. Accept metaphyseal comminution if the major fragments are aligned — this is bridging, not anatomic, fixation.
- Restore length (to the contralateral limb; 1 to 2 cm shortening is acceptable in a low-demand elder), coronal alignment (5 to 7 degrees valgus), sagittal alignment (neutral), and rotation (compare with the contralateral limb — malrotation is the common error).
- Techniques: sustained manual traction, padded reduction clamps (pad them — bone crushes), provisional K-wires away from planned screws, and the plate itself as a reduction tool in the comminuted zone.
- Acceptable reduction: length within 1 cm, alignment within 5 degrees, rotation under 10 degrees. Varus is never acceptable (high failure risk).
- Anatomically contoured lateral distal femur locking plate (a periprosthetic-specific plate if available); fixed-angle locking screws are essential in osteoporotic bone.
- LONG plate: minimum 10 to 12 cortices (5 to 6 screws) proximal to the fracture — MORE than a native fracture — to distribute stress and avoid a proximal stress riser (the commonest failure site).
- Seat the plate on the TRUE lateral cortex (not anterior or posterior, which causes sagittal malreduction); confirm on fluoroscopy — AP shows it on the lateral edge, lateral shows it superimposed on the cortex.
- Distal end at or just proximal to the component (no bone for screws beyond it); proximal end well above the fracture.
- Minimal contouring of pre-contoured plates; avoid notching. In osteoporotic bone the plate sits ON the cortex rather than being compressed down.
- Provisional K-wires or temporary cortical screws hold it for assessment before definitive screws.
- Fill MORE holes than in a young patient: 5 to 6 screws (10 to 12 cortices) proximal, staggered to reduce stress concentration.
- Modified working length: leave only 1 to 2 holes empty near the fracture (weak bone needs more stability, less reliance on biology alone) — the opposite of the young-patient strategy.
- Mix non-locking cortical screws (to compress plate to bone if a gap remains) then locking screws (fixed-angle stability).
- Bicortical purchase for maximum grip in weak bone; torque-limiting screwdriver for locking screws.
- The TKR femoral component sits posteriorly on the distal femur and BLOCKS posterior screw trajectories; the cement mantle is very hard and breaks drills. Hitting it dulls or breaks the drill, may crack the component, and the screw will not advance.
- FIRST CHOICE: anterior-to-posterior screws — drill from the anterior cortex toward the posterior, AWAY from the component and AWAY from the popliteal vessels; unicortical or short bicortical.
- Alternatives if the plate design allows: medial-to-lateral or lateral-to-medial screws perpendicular to the joint line; screws through the femoral component pegs if modular; or accept unicortical locking screws (which still grip well) when bicortical would endanger the component or vessels.
- Technique: targeting guide attached to the plate, 3.2 mm drill, FREQUENT AP and lateral fluoroscopy before and during each screw; STOP if you meet hard resistance (cement); verify each screw does not penetrate the joint.
- Realistic yield: 2 to 4 distal screws. Even 2 to 3 well-placed screws suffice IF proximal fixation is long and robust.
- Bone graft (autograft, allograft chips, or a substitute such as calcium phosphate / DBM) for a significant metaphyseal void or gap after reduction.
- Cement augmentation of proximal screws is off-label and not evidence-based for this indication — a longer plate with more screws, or a DFR, is preferable.
- In high non-union-risk patients (active smoking, diabetes, severe osteoporosis), BMP or DBM may be considered; most cases need no biological augmentation beyond MIPO biology and void-filling.
- Fluoroscopy: AP (5 to 7 degrees valgus maintained, no translation, screws clear of the component), lateral (no sagittal angulation, no posterior screw penetration), plus hip and knee views for proximal and distal hardware.
- Clinical: palpate the fracture site for stability; gently flex the knee to 45 to 60 degrees and confirm the construct holds; recheck length and rotation against the other leg.
- If fixation is inadequate (fewer than 2 distal screws, poor purchase, questionable reduction) — reconsider additional fixation, bone grafting, or conversion to a DFR before closure.
- Copious (at least 3 L) saline irrigation.
- Layered closure: re-approximate vastus lateralis to the septum (often atrophic — do not over-tension), close the ITB split (0 or 1 absorbable), close subcutaneous tissue to obliterate dead space, then skin (staples, interrupted or subcuticular) without tension.
- Drain (12 to 14 Fr) if dissection is large or anticoagulation expected; remove at 24 to 48 hours when output is under 30 mL per 8 hours.
- Dressing, then a hinged knee brace locked in extension for comfort and to protect the distal fixation from flexion stress.
Two structures are endangered by every distal screw: the TKR femoral component and the popliteal vessels. The component sits posteriorly and blocks the posterior path; the vessels lie directly posterior to the distal femur. Use an anterior-to-posterior trajectory, accept unicortical or short bicortical purchase, and image (AP and lateral) before and during EVERY distal screw. If the drill meets hard resistance it is cement — stop and redirect. A posterior bicortical screw can cause fatal vascular injury. Check distal pulses after tourniquet release.
Elderly skin necroses easily — handle it gently, keep skin bridges over 7 to 10 cm, and close without tension. The patellar tendon (compromised by the prior TKR) must not be violated distally. Strip the minimum soft tissue to preserve fracture biology (submuscular, periosteum-sparing). Stay proximal to the fibular neck to avoid a common peroneal nerve palsy.
Stable component (Rorabeck I or II) means ORIF is appropriate. Loose component (Type III) means ORIF alone fails — more than 80 percent failure rate — and revision arthroplasty is mandatory. Pre-operative films hint at loosening (lucency greater than 2 mm, subsidence, alignment change), but confirm it intra-operatively with stress testing before committing to fixation.
The distal screws are the hardest part of the case and the most dangerous. Anterior-to-posterior trajectory first; medial-lateral or through-peg options only if the plate allows; accept unicortical. Image every screw in two planes. Hitting the component dulls drills, breaks screws and may crack the cement — and a posterior overshoot hits the popliteal vessels.
Posterior to the distal femur — at risk from posterior or long bicortical screws. Protect with an anterior trajectory, unicortical or short bicortical screws, and constant fluoroscopy.
At the fibular neck — at risk if lateral dissection runs too distal or retraction is excessive. Identify the ITB, stay proximal to the neck, and warn the patient of the small palsy risk.
Posterior and distal on the femur — blocks posterior screw paths. Map it pre-operatively, image before each distal screw, use anterior trajectory, and test for loosening before fixation.
Vastus lateralis is often atrophic and scarred; the patellar tendon is the critical distal structure. Sharp dissection through scar, preserve muscle, protect the tendon, layered tension-free closure.
"Eggshell" cortices give poor screw purchase and propagate fractures. Reduce gently, use a long plate with multiple bicortical screws, consider a DFR if fixation is futile, and protect weight-bearing.
Thin elderly skin, prior incisions and diabetes risk necrosis and dehiscence. Gentle handling, adequate skin bridges, tension-free layered closure, and a drain when needed.
Aftercare & Complications
Rehabilitation. Recovery is slower and more protected than for a native distal femur fracture — osteoporotic bone, limited distal fixation and an elderly patient. | Phase | Timing | Weight-bearing | Range of motion | |-------|--------|----------------|-----------------| | 1 | 0 to 6 weeks | TTWB or PWB 20 to 30 kg, walker or crutches | 0 to 45 degrees, passive and active-assisted | | 2 | 6 to 12 weeks | Advance to PWB 50 percent if early callus | 0 to 90 degrees, begin gentle active ROM | | 3 | 3 to 6 months | WBAT if bridging callus on 3 of 4 cortices | Goal 0 to 120 degrees | | 4 | 6 to 12 months | Full, unrestricted | Maintain motion; quadriceps and gait work | Advance earlier only with excellent bone quality, robust fixation (6 or more screws each side) and a simple pattern; restrict longer with severe osteoporosis, fewer than 3 distal screws, comminution or questionable stability. Follow-up. Wound check and suture/staple removal at 2 weeks; AP and lateral X-rays at 6, 12 weeks and 4 to 6 months. Periprosthetic fractures heal SLOWER than native — bridging callus on 3 of 4 cortices is union; 4 to 6 months is typical, up to 12 months acceptable. VTE prophylaxis is a high priority — elderly, TKR, fracture, surgery and immobility make a very high-risk combination. Mechanical prophylaxis from induction; chemical prophylaxis (LMWH, a DOAC, or aspirin in selected lower-risk patients) once haemostasis is secure, continued for an extended course given prolonged protected weight-bearing. Balance against bleeding risk.
- Recognition
- Increasing pain, loss of reduction, screw loosening or varus on X-ray, usually within 3 months
- Prevention
- Long plate (10 to 12 cortices proximal), 5 to 6 proximal screws, 2 to 4 distal screws, protected weight-bearing
- Management
- Revision ORIF if early with good bone stock; otherwise conversion to a distal femoral replacement
- Recognition
- No callus progression by 6 months; persistent pain, unable to bear weight
- Prevention
- MIPO biology, long stable construct, nutrition and vitamin D, smoking cessation
- Management
- Revision ORIF with bone grafting and compression; DFR if poor bone stock
- Recognition
- Wound drainage, erythema, fever; raised WBC and CRP; sinus tract if chronic
- Prevention
- Prophylactic cefazolin, sterile technique, tension-free closure, glycaemic control
- Management
- Acute: debride, irrigate, retain stable hardware. Chronic: staged removal, spacer, IV antibiotics, revision
- Recognition
- Gait abnormality, leg-length difference, patellar maltracking; CT for rotation
- Prevention
- Meticulate reduction to 5 to 7 degrees valgus and neutral rotation; compare with the other side
- Management
- Mild and asymptomatic: observe. Symptomatic varus over 10 degrees: corrective osteotomy
- Recognition
- Drainage, skin blanching or necrosis, separation at the week-2 review
- Prevention
- Gentle handling, skin bridge over 7 to 10 cm, layered tension-free closure, drain
- Management
- Local care for superficial dehiscence; return to theatre for full-thickness breakdown
- Recognition
- Pulsatile bleeding or expanding haematoma intra-op; absent pulses, cool foot, compartment syndrome post-op
- Prevention
- Anterior trajectory, unicortical or short bicortical distal screws, constant fluoroscopy
- Management
- Immediate vascular consult, exploration and repair, fasciotomy if needed
- Recognition
- Calf swelling and pain (DVT); dyspnoea, tachycardia, hypoxia (PE)
- Prevention
- Mechanical prophylaxis immediately; LMWH, DOAC or aspirin once haemostasis secure
- Management
- Therapeutic anticoagulation for 3 to 6 months; thrombolysis or embolectomy for massive PE
- Recognition
- Progressive loss of motion, pain at end range, usually by 3 to 6 months
- Prevention
- Early protected ROM from day 1 to 2, balanced with fixation protection
- Management
- Intensive physiotherapy, static-progressive splinting; MUA only with caution
Viva & Exam Focus
STABLESTABLE — assessing the femoral component
DISTALDISTAL — screw strategy around the component
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 78-year-old woman presents with a displaced periprosthetic supracondylar femur fracture 6 years after a TKR. What is your critical assessment and management approach?”
“You are performing periprosthetic ORIF and attempting distal screw fixation. What are your strategies, and why is this the most challenging aspect?”
“How does your plate selection and proximal fixation strategy differ in a periprosthetic fracture compared with a native distal femur fracture in a young patient?”
Classification
- Rorabeck: I non-displaced stable (conservative), II displaced stable (ORIF), III loose (revision)
- Su: I above, II at component (IIA stable = ORIF, IIB loose = revision), III below (rare)
- Component stability is the critical variable — if loose, ORIF fails
- Loosening signs: lucency greater than 2 mm, subsidence, alignment change — confirm intra-op
Indication & setup
- Rorabeck II — displaced fracture, stable component — is the ORIF indication
- Assess patient, fracture and prosthesis domains
- Supine, radiolucent table, hip bump, whole-femur fluoroscopy before draping
- Counsel for ORIF and possible DFR conversion
Exposure
- Lateral approach to the distal femur
- Use the existing scar or a separate lateral incision (skin bridge over 7 to 10 cm)
- ITB split, vastus lateralis elevated anteriorly (expect atrophic scarred muscle)
- Submuscular plane for the plate; expose to the component level
Reduction & plate
- Gentle biological reduction — do not crush osteoporotic bone
- Goals: length, 5 to 7 degrees valgus, neutral rotation (compare the other side)
- LONG lateral locking plate — 10 to 12 cortices (5 to 6 screws) proximal
- Fill most holes (leave 1 to 2 empty), bicortical preferred
Distal fixation — critical
- Component blocks posterior paths — use ANTERIOR-to-posterior trajectory (first choice)
- Alternatives: medial-lateral, through pegs if modular, accept unicortical
- Constant AP and lateral fluoroscopy for each distal screw
- Realistic yield 2 to 4 screws; compensate with long proximal fixation
Aftercare
- TTWB or PWB 20 to 30 kg for 12 weeks (more restricted than native)
- ROM 0 to 45 degrees for 6 weeks, then progress to 0 to 90 degrees
- Extended VTE prophylaxis — very high risk group
- Heals slowly — 4 to 6 months typical, up to 12 acceptable
Complications
- Fixation failure 10 to 20 percent; non-union 10 to 15 percent
- Deep infection 2 to 5 percent — catastrophic near a TKR
- Varus malunion and malrotation the deformities to avoid
- Union 80 to 90 percent; only 70 to 80 percent return to pre-fracture mobility; 1-year mortality 5 to 10 percent
Background & Evidence
Background. Periprosthetic fractures around a total knee replacement are fragility injuries of the elderly osteoporotic femur, and their incidence is rising as the number of primary knee arthroplasties grows and patients live longer with their implants. Most are low-energy falls in women in their eighth decade, frequently on anticoagulation, with medical comorbidity and limited physiological reserve — they belong on a formal fragility-fracture pathway with orthogeriatric co-management, bone-health optimisation and VTE prophylaxis. Classification drives management. Two complementary systems are used together:
- Component
- Stable
- Fracture
- Non-displaced
- Management
- Conservative trial — hinged brace, TTWB, weekly X-rays; low threshold to convert to ORIF
- Component
- Stable
- Fracture
- Displaced
- Management
- ORIF with a long lateral locking plate — the standard operation
- Component
- Loose or failing
- Fracture
- Displaced
- Management
- Revision arthroplasty — long-stem revision TKR or distal femoral replacement
- Location
- Above the component
- Component
- Usually stable
- Management
- Treat as a native supracondylar fracture; lateral locking plate
- Location
- At the proximal aspect of the component
- Component
- Stable
- Management
- ORIF — the most challenging distal fixation
- Location
- At the component
- Component
- Loose
- Management
- Revision arthroplasty
- Location
- Below the component (less than 5 percent)
- Component
- Often with tibial loosening
- Management
- Complex; usually revision arthroplasty
ORIF or distal femoral replacement? The choice is individualised. Pooled meta-analysis (Bundschuh, 2023; 1,258 fractures) found NO significant difference in surgical complication or reoperation rates between ORIF and DFR, but a significantly higher MEDICAL complication rate with DFR (about 23 percent versus 9 percent). A separate meta-analysis (Ponugoti, 2022; 406 patients) found no significant difference in length of stay, mortality, revision or complication rates. DFR therefore allows early weight-bearing and removes fixation-failure risk — attractive in the very elderly, severely osteoporotic, low-demand patient — but at greater medical morbidity; failed ORIF can be salvaged with a DFR.
- ORIF (lateral locking plate)
- Stable component, adequate bone stock, higher-demand patient
- Distal femoral replacement
- Very elderly, severe osteoporosis, low-demand, unreconstructable bone
- ORIF (lateral locking plate)
- Protected TTWB or PWB 20 to 30 kg for about 12 weeks
- Distal femoral replacement
- Early — immediate to 6 weeks
- ORIF (lateral locking plate)
- Preserved
- Distal femoral replacement
- Removed (limits future options)
- ORIF (lateral locking plate)
- 10 to 20 percent
- Distal femoral replacement
- Lower
- ORIF (lateral locking plate)
- About 9 percent
- Distal femoral replacement
- About 23 percent
- ORIF (lateral locking plate)
- Comparable (about 13 percent)
- Distal femoral replacement
- Comparable (about 13 percent)
Outcomes. Union is achieved in 80 to 90 percent with appropriate modern fixation (locked plate or retrograde nail), but the overall major-complication rate is high — fixation failure 10 to 20 percent, non-union 10 to 15 percent, deep infection 2 to 5 percent, malunion or malrotation 10 to 15 percent. Time to union is 4 to 6 months (up to 12 acceptable). Even when the fracture heals, only 70 to 80 percent of patients return to their pre-fracture mobility, 20 to 30 percent require nursing-home placement, and one-year mortality is 5 to 10 percent — a reminder that these are challenging fractures in fragile patients.
References
Classification of periprosthetic fractures complicating total knee arthroplasty
- Defined the Lewis and Rorabeck classification: Type I non-displaced with stable prosthesis, Type II displaced with stable prosthesis, Type III displaced with loose or failing prosthesis
- Component stability, not fracture displacement alone, is the pivotal variable directing treatment selection
- Provides the framework distinguishing fractures amenable to internal fixation from those requiring revision arthroplasty
Treatment of acute distal femur fractures above a total knee arthroplasty: systematic review of 415 cases (1981-2006)
- Pooled 415 fractures from 29 series: nonunion 9 percent, fixation failure 4 percent, infection 3 percent, revision surgery 13 percent
- Retrograde nailing and locked plating were superior to traditional non-locking plating and to non-operative treatment for nonunion and revision risk
- Retrograde nail showed an 87 percent relative risk reduction for nonunion and 70 percent for revision versus conventional plating
Risk factors for failure of locked plate fixation of distal femur fractures: an analysis of 335 cases
- 335 distal femur fractures across three trauma centres; 19 percent required reoperation to promote union
- Shorter plate length was an independent risk factor for proximal implant failure, alongside open fracture, smoking and higher BMI
- Plate length is the principal modifiable, surgeon-controlled technical factor reducing fixation failure
Distal femoral replacement versus operative fixation for periprosthetic distal femur fractures: a systematic review and meta-analysis
- Pooled 1,258 periprosthetic distal femur fractures (977 ORIF, 281 DFR) from 32 studies
- Surgical complication rate (20.5 percent ORIF versus 14.9 percent DFR) and reoperation rate (12.9 percent versus 12.5 percent) were not significantly different
- DFR carried a significantly higher medical complication rate (23.1 percent versus 8.5 percent, p equals 0.0006)
Comparable outcomes between native and periprosthetic fractures of the distal femur
- 54 native versus 54 periprosthetic AO/OTA type 33 fractures, matched 1 to 1 by age and sex (mean age 73 to 74 years)
- No significant differences in operative time, blood loss, length of stay, discharge disposition or mortality
- The large majority in both groups (51 of 54) were managed with lateral locked-plate ORIF
Further reading 1. Su ET, DeWal H, Di Cesare PE. Periprosthetic femoral fractures above total knee replacements. J Am Acad Orthop Surg. 2004;12(1):12-20. doi:10.5435/00124635-200401000-00003 — the Su classification system (Types I, IIA, IIB, III) and treatment algorithms. 2. Ehlinger M, Ducrot G, Adam P, Bonnomet F. Distal femur fractures. Surgical techniques and a review of the literature. Orthop Traumatol Surg Res. 2013;99(3):353-360. doi:10.1016/j.otsr.2012.10.014 — lateral locked plating technique including periprosthetic cases. 3. Aldrian S, Schuster R, Haas N, et al. Fixation of supracondylar femoral fractures following total knee arthroplasty: angular stable plate fixation versus rigid interlocking nail fixation. Arch Orthop Trauma Surg. 2013;133(7):921-927. doi:10.1007/s00402-013-1736-8 — locked plating versus retrograde nailing; equivalent union, plating preferred when the distal fragment is limited or the canal is blocked. 4. Fulkerson E, Tejwani N, Stuchin S, Egol K. Management of periprosthetic femur fractures with a first generation locking plate. Injury. 2007;38(8):965-972. doi:10.1016/j.injury.2007.02.026 — distal screw placement around TKR components; unicortical and anterior trajectory screws. 5. Horneff JG, Scolaro JA, Jafari SM, et al. Intraoperative fluoroscopy to evaluate screw placement in distal femur fracture fixation. Orthopedics. 2013;36(5):e625-e629. doi:10.3928/01477447-20130426-25 — multi-plane fluoroscopy to avoid the component and the popliteal vessels. 6. Frosch KH, Balcarek P, Walde T, et al. A modified Palmer approach for internal fixation of distal femur fractures. J Orthop Trauma. 2010;24(11):731-737. doi:10.1097/BOT.0b013e3181d04c5f — minimally invasive lateral submuscular approach preserving fracture biology. 7. Ebraheim NA, Liu J, Hashmi SZ, et al. High complication rate in locking plate fixation of lower periprosthetic distal femur fractures in patients with total knee arthroplasties. J Arthroplasty. 2012;27(5):809-813. doi:10.1016/j.arth.2011.08.007 — 30 to 40 percent complication rate (fixation failure 15 percent, non-union 12 percent, infection 5 percent). 8. Ponugoti N, Raghu A, Kosy JD, Magill H. Distal femoral replacement versus fixation in treating periprosthetic supracondylar femur fractures: a systematic review and meta-analysis. Arch Orthop Trauma Surg. 2023;143(6):3335-3345. doi:10.1007/s00402-022-04603-1 — 406 patients; no significant difference in length of stay, mortality, revision or complication rates.