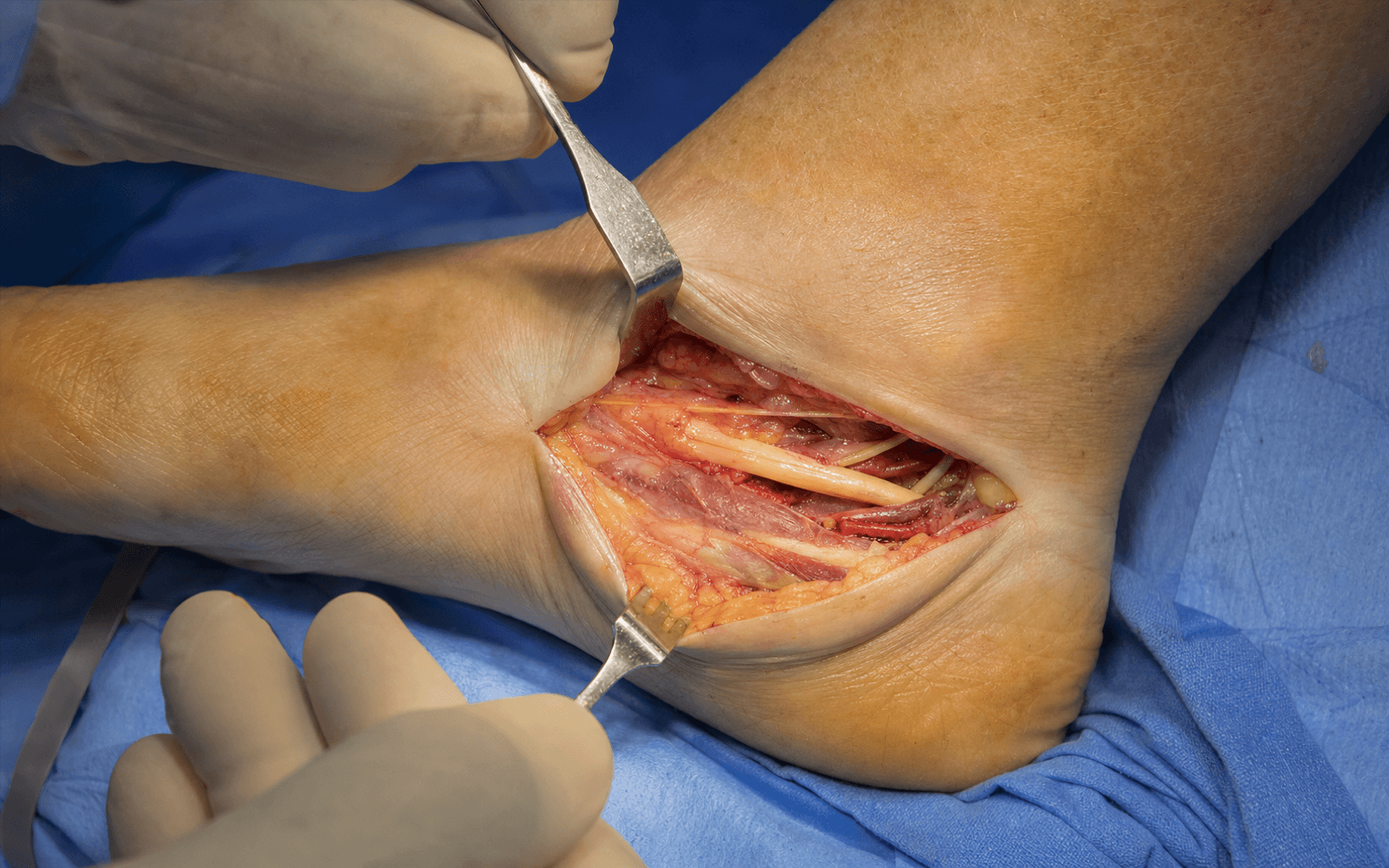
Medial curvilinear approach for complete decompression of the posterior tibial nerve, from 8 cm proximal to the medial malleolus to the navicular tuberosity distally
- Tarsal tunnel syndrome is compression of the posterior tibial nerve beneath the flexor retinaculum behind the medial malleolus. The clinical triad is burning plantar foot pain, a positive Tinel's sign, and symptoms worse with standing or walking and often nocturnal.
- Complete decompression has THREE components: proximal flexor retinaculum release (beginning 8 cm above the malleolus), distal release (to the navicular tuberosity), and release of the abductor hallucis origin. Incomplete release is the most common cause of failure (around 30 percent).
- The abductor hallucis release is the single most-missed step. Its origin from the calcaneus forms a fibrous arch that compresses the medial plantar nerve (distal tarsal tunnel syndrome).
- Tunnel contents anterior to posterior — Tom Dick ANd Very Nervous Harry: Tibialis posterior, flexor Digitorum longus, posterior tibial Artery, Vein, tibial Nerve, flexor Hallucis longus. The nerve lies between the vessels (anterior) and FHL (posterior).
- A space-occupying lesion is found in 20-30 percent of cases — ganglion is the most common (from the subtalar joint). Identify and excise it for the best outcome.
- Success is 70-90 percent with good patient selection. Favorable: young age, short symptom duration (under 1 year), an identifiable lesion, positive EMG. Poor: diabetes (about 50 percent success), bilateral symptoms, normal EMG, worker's compensation.
When & Why
Indication. Tarsal tunnel syndrome that has failed a 3-6 month trial of conservative care — burning, tingling or numbness in the plantar foot (medial plantar, lateral plantar or calcaneal distribution), worse with standing, walking and prolonged weight-bearing, frequently nocturnal (it wakes the patient), and relieved by rest, elevation and shoe modification. Make the diagnosis on clinical grounds first. The bedside signs are a Tinel's sign posterior to the medial malleolus with distal radiation (the Valleix phenomenon), a positive dorsiflexion-eversion test (maximal passive ankle dorsiflexion plus eversion reproduces symptoms — it stretches the nerve beneath the laciniate ligament), and in chronic disease diminished two-point discrimination on the plantar foot and intrinsic muscle atrophy. Confirm with electrodiagnosis, but treat the patient. Motor nerve conduction showing prolonged distal motor latencies of the medial and lateral plantar nerves (over 6.2 ms is abnormal), reduced or absent plantar sensory action potentials, and denervation potentials in abductor hallucis and flexor digitorum brevis support the diagnosis — but a normal study does not exclude it, and abnormal studies do not reliably predict outcome. Relative indications include acute (traumatic) tarsal tunnel syndrome, an identifiable space-occupying lesion (ganglion, varicosities, lipoma, accessory muscle) on imaging even before a full conservative trial, post-traumatic compression from a calcaneal or pilon malunion, and symptomatic post-surgical scarring. Who not to operate on. Avoid surgery when the true diagnosis is a systemic or proximal problem:
- Key distinguishing features
- Bilateral and symmetric, stocking-glove distribution; systemic disease (diabetes, alcohol, B12 deficiency, chemotherapy); reduced ankle reflexes; EMG shows diffuse demyelination with globally reduced amplitudes
- Key distinguishing features
- Back pain with radiating pain; dermatomal pattern (L5 — dorsal foot and great toe, S1 — lateral foot); positive straight leg raise; lumbar MRI shows disc herniation or foraminal stenosis
- Key distinguishing features
- Heel pain (not numbness); morning first-step pain and stiffness; tenderness at the plantar fascia origin; no Tinel's sign and no neurology
- Key distinguishing features
- Acute traumatic onset; deltoid ligament tenderness; no paresthesias and no Tinel's sign; MRI shows ligament injury without nerve compression
The patient factors that decide success. Surgery is most rewarding when a definable, mechanical cause is present and the patient is otherwise well; it is least rewarding when the symptom source is systemic.
Young age, short symptom duration (under 1 year), an identifiable compressing lesion, and positive EMG findings. Reported success 70-90 percent.
Diabetes (success drops to around 50 percent), bilateral symptoms, a normal EMG (suggesting neuropathy rather than compression), worker's compensation, and chronic symptoms over 2 years (irreversible nerve damage).
Consent specifically for the incision behind the malleolus, possible saphenous or calcaneal nerve numbness or a painful neuroma, wound problems over the thin medial malleolar skin, haematoma, and the realistic expectation that nerve recovery is gradual over many months and that success is not guaranteed (a good or excellent result in roughly 44-85 percent depending on the series). Setup. Supine with a bump under the ipsilateral hip to internally rotate the leg and bring the medial ankle into view, the foot over the end of the table so the ankle can be manipulated, a thigh tourniquet (inflate to 250-300 mmHg), and loupe magnification (2.5x to 3.5x) — identifying and protecting the nerve and its branches is the whole game.
The Operation
The goal: expose and decompress the posterior tibial nerve along its entire course from 8 cm above the medial malleolus to the navicular tuberosity, through all three zones — the proximal and distal flexor retinaculum and the abductor hallucis origin — while protecting the artery, the vein and every nerve branch, excise any space-occupying lesion, and confirm with a dynamic check that the nerve glides freely before you close.
Operative sequence
- Supine, bump under the ipsilateral hip to internally rotate the leg, foot over the end of the table, thigh tourniquet, loupes on.
- Mark the landmarks: the medial malleolus, the posterior tibial artery pulse posterior to it, the course of the posterior tibial nerve, and distally the navicular tuberosity.
- Plan the incision to run from 8 cm proximal to the medial malleolus to the navicular tuberosity (12-15 cm total).
- A curvilinear incision starting 8 cm proximal to the medial malleolus, curving 1-2 cm posterior to the malleolar apex, and extending distally to the navicular tuberosity.
- Keep the curve gentle (sharp angles compromise the thin skin flaps) and stay posterior to the malleolus to protect the anterior saphenous structures.
- Incise the skin sharply to subcutaneous tissue and raise full-thickness flaps (skin and subcutaneous fat together) anteriorly and posteriorly — the thin skin over the medial malleolus will not survive thin flaps.
- Identify and preserve the great saphenous vein and the saphenous nerve, which run 1-2 cm anterior to the malleolus; injury causes medial ankle and foot numbness or a painful neuroma.
- Ligate small perforating veins with absorbable ties to prevent a haematoma.
- The flexor retinaculum (laciniate ligament) is the strong, taut, glistening white band running from the medial malleolus to the calcaneus that forms the roof of the tarsal tunnel.
- It has two layers — superficial and deep — and both must be divided; missing the deep layer is a classic cause of incomplete release.
- Palpate the underlying structures before cutting: the tendons (TP, FDL) anteriorly, the pulsatile neurovascular bundle in the middle, and FHL posteriorly.
- Begin the release proximally (8 cm above the malleolus), where the anatomy is less crowded and safer.
- Make a small longitudinal incision in the retinaculum and identify the posterior tibial nerve before any further cutting — a thick white cord with longitudinal striations, lying between the vessels (anterior) and FHL (posterior).
- Divide the retinaculum longitudinally with Metzenbaum scissors held parallel to the nerve, advancing distally and releasing both superficial and deep layers.
- Adequacy: the released nerve should bulge or "mushroom" out through a visible gap, with no constricting bands remaining.
- Continue the release past the medial malleolus and follow the nerve to its trifurcation (at or just distal to the malleolus), releasing the retinaculum over all three branches down to the navicular tuberosity.
- Identify the medial calcaneal nerve(s) branching proximal to the bifurcation (often multiple, 2-4 branches, to the heel) and preserve them.
- Identify the medial plantar nerve (the larger, anterior branch) as it passes deep to the abductor hallucis, and the lateral plantar nerve (the smaller, posterior branch) running toward the lateral plantar foot.
- The abductor hallucis takes origin from the medial calcaneal tubercle and the medial plantar fascia, and this origin forms a fibrous arch over the medial plantar nerve — the site of distal tarsal tunnel syndrome.
- Identify the muscle belly, trace it to its calcaneal origin, and sharply release the origin (electrocautery or scalpel) along with its attachment to the medial plantar fascia.
- Elevate the muscle anteriorly to expose the medial plantar nerve beneath it and confirm the nerve is free and mobile along its entire course with no tethering fibrous bands.
- Inspect the nerve from proximal to distal: look for extrinsic compression (scar, a lesion) and for intrinsic pathology (a neuroma or hourglass constriction).
- Perform an external neurolysis — release scar and adhesions around the nerve with tenotomy scissors so it glides freely. Do not perform internal neurolysis (opening the epineurium) routinely; it causes more scarring and worse outcomes and is reserved only for a focal hourglass constriction.
- If a space-occupying lesion is present (20-30 percent of cases), excise it: a ganglion (most common, from the subtalar or talonavacular joint) — excise completely and ligate the stalk; varicosities — ligate proximal and distal and excise the segment; an accessory FDL or FHL muscle belly — excise the belly, preserving the tendon; a lipoma — excise and send for histology.
- Take the ankle through full range of motion — dorsiflexion and plantarflexion, inversion and eversion. Dorsiflexion-eversion places maximum tension on the nerve.
- The nerve must glide smoothly with no tethering, mushroom through the retinacular gap, and remain free of constricting bands through the full arc.
- If the nerve still tethers, do not close: re-check each zone (proximal retinaculum and its deep layer, distal extension to the navicular, the abductor release, all three branches, and any missed lesion) until it glides perfectly.
- Deflate the tourniquet and identify all bleeding; use bipolar cautery for small vessels (monopolar near the nerve is forbidden) and ligate larger ones with absorbable ties.
- Place a 10-French round drain deep to the skin and superficial to the nerve, exiting through a separate inferior stab incision, to prevent a haematoma — a haematoma scars and re-compresses the nerve and defeats the operation.
- Remove the drain at 24-48 hours when output is under 30 mL per 24 hours.
- Reapproximate the subcutaneous tissue with 3-0 absorbable interrupted sutures.
- The retinaculum: either leave open or loosely approximate to prevent bowstringing — never close it tightly, which would re-compress the nerve. (Z-lengthening is an option if approximating.)
- Skin with 4-0 nylon vertical mattress sutures or a 4-0 absorbable subcuticular running suture, then a sterile dressing with soft padding.
- Apply a below-knee backslab with the ankle neutral, non-weight-bearing, for 2 weeks of immobilisation, oedema control and wound protection.
Before dividing the retinaculum, identify the posterior tibial nerve proximally where the anatomy is safe — a thick white cord between the vessels (anterior) and FHL (posterior). Divide the retinaculum with scissors held parallel to the nerve, never perpendicular, through both layers. Nerve laceration is rare (less than 1 percent) but devastating: loupe magnification, identification first, and bipolar-only cautery near the nerve are how you prevent it.
Incomplete release causes around 30 percent of failures. Completely release the abductor origin from the calcaneus and the medial plantar fascia, elevate the muscle anteriorly, and visualise the medial plantar nerve beneath it along its whole course. If you do not do this, the distal compression remains and the operation will fail.
Keep the incision 1-2 cm posterior to the medial malleolus. Too anterior injures the saphenous vein and nerve (numbness or a painful neuroma); too posterior makes the nerve hard to reach. Ligate perforating veins as you go to prevent a haematoma.
Meticulous hemostasis after tourniquet deflation, a drain for 24-48 hours, immobilisation and elevation are not optional. A haematoma (5-10 percent without a drain, under 2 percent with one) scars around the nerve and re-creates exactly the compression you just released.
- Location
- Between the vessels (anterior) and FHL (posterior) in the tunnel
- How to protect it
- Identify early, loupe magnification, scissors parallel to the nerve, bipolar-only cautery
- Consequence of injury
- Laceration is devastating — permanent plantar sensory and motor deficit
- Location
- Immediately anterior to the nerve, between FDL and the nerve
- How to protect it
- Careful retinacular division, bipolar cautery only, meticulous hemostasis
- Consequence of injury
- Haematoma causes scarring and nerve compression, defeating the operation
- Location
- Anterior to the incision, 1-2 cm anterior to the malleolus
- How to protect it
- Incision 1-2 cm posterior to the malleolus; identify and preserve vein and nerve
- Consequence of injury
- Numbness of the medial ankle and foot, or a painful neuroma
- Location
- The larger, anterior branch at the trifurcation, deep to abductor hallucis
- How to protect it
- Complete abductor hallucis release; identify the nerve before releasing the muscle origin
- Consequence of injury
- Sensory loss over the medial 3.5 toes and intrinsic weakness
- Location
- Branch proximal to the bifurcation, often multiple (2-4), to the heel
- How to protect it
- Identify all branches during proximal release and preserve them
- Consequence of injury
- Painful heel and medial heel numbness — difficult to treat
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | 0-2 weeks | Below-knee backslab, non-weight-bearing; drain out at 24-48 hours when under 30 mL/day | Elevation, ice, neurovascular checks; finger and toe active motion only | | 2 | 2-6 weeks | Remove backslab and sutures at week 2; CAM boot or ankle brace | Touch-down to partial then full weight-bearing; gentle active ankle and toe ROM. No passive stretching (nerve irritation) | | 3 | 6-12 weeks | Wean to a supportive shoe; full weight-bearing | Proprioception (balance board), theraband resistance, intrinsic foot strengthening (towel curls, marble pickup) | | 4 | 3-6 months | Supportive footwear with arch support | Walking program, gradual return to activity; avoid high-impact work until the nerve has recovered | Nerve recovery is slow and reassuring. Symptoms may worsen briefly after surgery (manipulation), then improve gradually over 3-6 months. Sensory recovery precedes motor recovery, and a positive Tinel's that migrates distally as the nerve regrows is a good sign. Full recovery can take 12 months. Review at 2 weeks (wound), 6 weeks (progress), 3 months (symptoms), 6 months (repeat EMG/NCS if no improvement) and 1 year (final outcome).
- Recognition
- Persistent symptoms identical to preoperative; positive Tinel's unchanged; no improvement by 3-6 months; repeat EMG shows persistent prolonged latencies; MRI shows incomplete release
- Prevention
- Complete proximal-to-distal release through both layers; mandatory abductor release; dynamic assessment of nerve glide
- Management
- Confirm with EMG and MRI; revision at 6-12 months with wide release, external neurolysis and scar excision — 50-60 percent success versus 70-90 percent primary
- Recognition
- No improvement despite a complete release; bilateral symptoms; EMG shows diffuse demyelination rather than isolated compression; systemic disease present
- Prevention
- Thorough preoperative workup; EMG confirmation; exclude peripheral neuropathy and radiculopathy before operating
- Management
- Neurology consultation; treat the underlying condition (diabetic control, B12); revision is unlikely to help
- Recognition
- Nerve transected intra-operatively; complete plantar sensory loss and intrinsic weakness postoperatively
- Prevention
- Loupe magnification; identify the nerve before cutting; scissors parallel; no monopolar cautery near the nerve
- Management
- Immediate tension-free neurorrhaphy with 8-0 or 9-0 nylon; sural nerve graft if a gap; immobilise 4 weeks; refer to a nerve specialist if delayed
- Recognition
- Increasing pain at 24-48 hours; tense swelling over the incision; bloody drainage; expanding mass
- Prevention
- Meticulous hemostasis after tourniquet deflation; 10-French drain for 24-48 hours; immobilisation and elevation
- Management
- Small — observe, elevate, ice; large or expanding — return to theatre for evacuation, hemostasis and re-drain
- Recognition
- Initial improvement then symptom recurrence at 3-12 months; MRI shows scar tethering the nerve
- Prevention
- Atraumatic technique; avoid excessive internal neurolysis; drain placement; gentle tissue handling
- Management
- Conservative trial for 3-6 months; revision with external neurolysis, scar excision and nerve wrapping (vein, fat or synthetic)
- Recognition
- Infection — erythema, warmth, purulent drainage, fever; dehiscence — wound edges separated; necrosis — black eschar
- Prevention
- Prophylactic cefazolin 2 g IV; sterile technique; full-thickness flaps; careful skin handling over the thin malleolar skin
- Management
- Superficial infection — cephalexin 500 mg QID; deep infection — IV antibiotics and debridement; necrosis — wound VAC and possible skin graft
- Recognition
- Numbness of the medial ankle and foot; dysesthesia; a tender neuroma if transected
- Prevention
- Incision 1-2 cm posterior to the malleolus; identify and preserve the saphenous nerve with the vein
- Management
- Observe if neuropraxia (often recovers 3-6 months); desensitisation; painful neuroma — excision and burial in muscle, plus gabapentin
- Recognition
- Painful heel and numbness of the medial heel
- Prevention
- Identify and preserve the multiple calcaneal branches during proximal release
- Management
- Observe (often improves over 6-12 months); desensitisation; neuroma excision if persistent
- Recognition
- Severe pain out of proportion; allodynia; temperature and colour change; oedema; Budapest criteria
- Prevention
- Gentle surgical technique; adequate pain control; early mobilisation from week 2
- Management
- Early recognition; therapy (desensitisation, ROM, stress loading); gabapentin 300-900 mg TID or pregabalin; sympathetic blocks
Viva & Exam Focus
Tom Dick ANd Very Nervous Harry
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old woman has 18 months of burning pain in her left plantar foot, worse at night and with standing, a positive Tinel's sign behind the medial malleolus, and failure of 6 months of conservative care. EMG shows prolonged distal motor latencies to the medial plantar nerve (7.8 ms; normal less than 6.2 ms). Describe your surgical approach for tarsal tunnel release.”
“Describe the anatomy of the tarsal tunnel in detail — its boundaries, contents, and the course and branching of the posterior tibial nerve.”
“You have completed a tarsal tunnel release. Intra-operatively the nerve still feels tethered with the ankle in dorsiflexion and eversion. What are the possible causes and how do you address them?”
Indication
- Tarsal tunnel syndrome failing 3-6 months of conservative care
- Clinical: burning plantar pain, positive Tinel's, nocturnal, worse with standing
- EMG: prolonged distal latencies (over 6.2 ms), reduced SNAP, denervation if chronic
- A space-occupying lesion even before a full conservative trial
Anatomy
- Tom Dick ANd Very Nervous Harry — TP, FDL, Artery, Vein, Nerve, FHL
- Flexor retinaculum has TWO layers — both must be released
- Three branches: medial plantar (larger, anterior), lateral plantar (smaller, posterior), calcaneal (proximal, often multiple)
- Abductor hallucis origin compresses the medial plantar nerve (distal tarsal tunnel syndrome)
The operation
- Incision 8 cm proximal to the malleolus, 1-2 cm posterior, to the navicular (12-15 cm)
- Release retinaculum proximal-to-distal, scissors parallel, BOTH layers
- Release the abductor hallucis origin — the critical, most-missed step
- External neurolysis; excise any lesion; dynamic check — nerve glides freely
Danger zones
- Posterior tibial nerve — between vessels and FHL
- Posterior tibial artery and vein — immediately anterior to the nerve
- Saphenous nerve and vein — anterior, stay posterior to the malleolus
- Medial plantar nerve — under abductor hallucis
- Calcaneal branches — proximal, multiple, to the heel
Aftercare
- Below-knee backslab, non-weight-bearing 2 weeks; drain out under 30 mL/day
- Week 2-6: CAM boot, progressive weight-bearing, gentle active ROM
- Week 6-12: wean boot, proprioception and strengthening
- Nerve recovery gradual, sensory before motor; full recovery up to 12 months
Outcomes & failures
- Success 70-90 percent with selection; 50 percent in diabetes
- Incomplete decompression (10-30 percent) is the most common failure
- Wrong diagnosis (10-30 percent) — bilateral symptoms, systemic neuropathy
- Revision success 50-60 percent versus 70-90 percent primary
Background & Evidence
Epidemiology. Tarsal tunnel syndrome is uncommon relative to carpal tunnel syndrome. It is most frequent in adults in the fourth to sixth decades and shows a slight female predominance. A structural or space-occupying cause — ganglion, talocalcaneal coalition, varicosities, accessory muscle, tumour or post-traumatic deformity — is found in a large proportion of surgical cases; truly idiopathic compression carries a more guarded prognosis. Outcomes. Reported complete symptom relief ranges from about 44 percent (Pfeiffer and Cracchiolo, a sobering benchmark) to 85 percent objective relief (Gondring), the variability reflecting patient selection. Across series, outcomes are best when a definite compressing lesion is identified and addressed early, and worst in idiopathic disease, diabetes, bilateral symptoms and worker's compensation cases. Revision surgery succeeds in roughly 50-60 percent — materially lower than primary release. Surgical anatomy — boundaries and contents. The tarsal tunnel is a fibro-osseous canal posterior to the medial malleolus. Its deep floor is the medial malleolus, the posterior talus, the sustentaculum tali and the medial calcaneus; its superficial roof is the flexor retinaculum (laciniate ligament) running from the medial malleolus to the calcaneus, with superficial and deep layers. From anterior to posterior it contains the tendons of tibialis posterior and flexor digitorum longus, the posterior tibial artery and its venae comitantes, the tibial nerve, and the flexor hallucis longus tendon — Tom Dick ANd Very Nervous Harry. Surgical anatomy — the nerve and its branches. The posterior tibial nerve enters the tunnel about 8 cm proximal to the malleolus, running between FDL and FHL, posterior to the vessels and anterior to FHL. It trifurcates at or just distal to the malleolus into three branches, each of which must be individually decompressed:
- Position and course
- Branches proximal to the bifurcation; often multiple (2-4 branches)
- Sensory distribution
- Medial heel
- Motor supply
- Sensory only — no motor
- Position and course
- Larger, anterior branch; runs deep to abductor hallucis (site of distal compression)
- Sensory distribution
- Medial 3.5 toes (hallux to medial side of the 4th)
- Motor supply
- Abductor hallucis, flexor hallucis brevis, flexor digitorum brevis, first lumbrical
- Position and course
- Smaller, posterior branch; runs deep toward the lateral plantar foot
- Sensory distribution
- Lateral 1.5 toes (lateral side of the 4th and the 5th)
- Motor supply
- Remaining intrinsics — interossei, adductor hallucis, lateral lumbricals
The abductor hallucis. Taking origin from the medial calcaneal tubercle and the medial plantar fascia, it forms a fibrous arch over the medial plantar nerve — the anatomical basis of distal tarsal tunnel syndrome and the reason its release is the single most important and most-missed step. Key evidence. The clinical diagnostic framework and the recommendation to operate after failed conservative care come from Cimino's foundational review. Kinoshita's dorsiflexion-eversion provocation test — positive in affected feet and negative in every normal foot — underpins both bedside diagnosis and the intra-operative dynamic check. Daniels' cadaveric work showed the tibial nerve is most tensioned by combined dorsiflexion-eversion, the biomechanical rationale for that test. Outcomes data (Takakura; Pfeiffer and Cracchiolo; Gondring) consistently show that an identifiable lesion treated early does best. For failed primary surgery, Barker, Rosson and Dellon demonstrated that systematic neurolysis of every branch in its own tunnel offers meaningful relief, but coexisting radiculopathy or neuropathy predicts a poor result.
References
The dorsiflexion-eversion test for diagnosis of tarsal tunnel syndrome
Prospective study in 50 normal volunteers (100 feet) and 37 operatively treated patients (44 feet). Maximal passive ankle dorsiflexion plus eversion plus toe dorsiflexion, held 5-10 seconds, intensified or induced symptoms in the large majority of affected feet and produced no symptoms in any normal foot. Intra-operative observation confirmed the manoeuvre stretches and compresses the tibial nerve beneath the laciniate ligament; symptoms resolved a mean of 2.9 months after release. The basis of both the bedside provocation test and the intra-operative dynamic excursion check.
Tarsal tunnel syndrome: review of the literature
The foundational literature review defining tarsal tunnel syndrome as entrapment of the posterior tibial nerve at the ankle, with diagnosis resting on plantar dysaesthesia, a positive Tinel's sign, provocation on compression, the Valleix phenomenon and sensorimotor change. Synthesises traumatic, space-occupying and idiopathic aetiologies and concludes most authors recommend surgical decompression after failed conservative care; electrodiagnosis supports but does not by itself establish the diagnosis.
Clinical results after tarsal tunnel decompression
Retrospective review of 30 patients (32 feet), mean follow-up 31 months. Only 14 of 32 feet (44 percent) achieved a good or excellent result — materially lower than earlier optimistic series. Of five completely satisfied patients, three had a discrete coexisting lesion (ganglion, accessory navicular, talocalcaneal coalition) treated at the same sitting. There was no correlation between abnormal pre-operative electrodiagnostic studies and clinical outcome. A sobering benchmark reinforcing rigorous patient selection.
Tarsal tunnel syndrome: causes and results of operative treatment
Operative treatment of 50 feet in 45 patients. A space-occupying or structural lesion was present in most: ganglia in 18 feet, a bony prominence from talocalcaneal coalition in 15, tumour in 3, trauma in 5, and no obvious cause in only 9. Outcome stratified by cause — feet with coalition or tumour fared best, whereas idiopathic and post-traumatic cases did worse. An excellent result is expected when a definite lesion is addressed early.
Outcome of neurolysis for failed tarsal tunnel surgery
Revision surgery in 44 patients (2 bilateral) with neurolysis of the tibial nerve and of the medial plantar, lateral plantar and calcaneal nerves in their respective tunnels, plus intertunnel septum excision and resection of painful neuromas; mean follow-up 2.2 years. Patient-rated outcomes were 54 percent excellent, 24 percent good, 13 percent fair and 9 percent poor; mean numerical pain score improved from 6.0 to 2.7 (P less than 0.001). Coexisting lumbosacral disc disease or neuropathy predicted a poor result.
An outcomes analysis of surgical treatment of tarsal tunnel syndrome
Outcomes study of 60 patients (68 feet), all with a positive Tinel's sign and abnormal motor nerve conduction velocity. Objective complete symptom relief was 85 percent versus subjective relief of 51 percent, highlighting the dichotomy between objective and patient-perceived outcomes, with significant improvement in work quality, productivity and interpersonal function.
The effects of foot position and load on tibial nerve tension
Cadaveric study of 9 feet showing tibial nerve tension is significantly increased by eversion, dorsiflexion and combined dorsiflexion-eversion, and is greater in an unstable (pes planus) foot and with increasing internal rotation under load. Provides the biomechanical rationale for the dorsiflexion-eversion provocation test and the intra-operative dynamic assessment.
Variations in the origin of the medial calcaneal nerve
Live-dissection study of 85 feet: a single medial calcaneal nerve in 37 percent, two in 41 percent, three in 19 percent and four in 3 percent; origin from the medial plantar nerve in 46 percent. Demonstrates the variability and multiplicity of calcaneal branches that must be identified and preserved during proximal release.
Conservative management of a case of tarsal tunnel syndrome
Discussion of conservative management for tarsal tunnel syndrome (NSAIDs, orthotics, corticosteroid injection, manual therapy). Surgical referral is generally reserved for failure of a 3-6 month conservative trial, particularly with motor involvement or a space-occupying lesion.