Tarsal Tunnel | Tibial Nerve | Posterior Malleolus and Distal Tibia
- Tarsal tunnel contents in order — Tom, Dick And Very Nervous Harry: Tibialis posterior, Flexor digitorum longus, posterior tibial Artery with Venae comitantes, tibial Nerve, Flexor hallucis longus.
- Tibial nerve lies between FDL anteriorly and FHL posteriorly, with the posterior tibial artery anterior to the nerve — it must be identified and protected throughout.
- Internervous plane is between FDL (tibial nerve) and FHL (tibial nerve) — both are tibial-nerve supplied, but the interval is safe because the nerve branches enter the muscles proximally.
- Posterior malleolar fragment is fixed with a buttress plate or posterior-to-anterior screws; fix fragments greater than 25 percent of the articular surface or with greater than 2 mm step-off.
- Cannot access lateral structures — this approach exposes only the medial malleolus and posteromedial tibia.
When & Why
What it exposes. The posteromedial approach gives direct access to the posteromedial distal tibia, the medial malleolus and the posterior malleolar fragment by working through the tarsal tunnel behind the medial malleolus. It is the workhorse exposure for posterior malleolus fixation, posteromedial pilon fragment fixation, tarsal tunnel release, and procedures on the posterior tibial and FHL tendons. Why posteromedial (and its limit). It is the only approach that delivers the posterior malleolus and posteromedial tibial metaphysis for direct, buttress-style fixation. The trade-off is that it cannot access lateral structures — for complex pilon fractures it is therefore combined with an anterolateral or anteromedial approach rather than used alone. Position & landmarks. The approach can be performed prone (excellent for isolated posterior malleolus or bilateral posterior work — chest rolls, arms abducted less than 90 degrees, knee slightly flexed) or supine with the leg externally rotated (knee flexed over a bolster, allowing a combined anteromedial approach without repositioning — preferred for most pilon cases). Knee flexion relaxes the gastrocnemius and improves access. Mark the medial malleolus (tip and anterior/posterior borders), the posterior tibial artery pulse behind the malleolus, the FHL tendon (palpable with great-toe flexion) and the medial border of the Achilles tendon as the posterior boundary; the incision lies 1 cm posterior to the medial malleolus. When to fix the posterior malleolus. A posterior malleolar fragment carrying greater than 25 percent of the articular surface or with greater than 2 mm of articular step-off is fixed — the fragment restores the posterior tibial plafond and carries the posterior inferior tibiofibular ligament, so reducing it improves talar stability and lowers the risk of post-traumatic arthritis. The posteromedial approach allows this by direct buttress plating. Pilon context. In pilon fractures the posteromedial approach addresses the posteromedial fragment and medial malleolus, while an anterolateral or anteromedial approach handles the anterior and lateral columns. Staged soft-tissue management is critical — bridge-spanning external fixation first, then definitive fixation once the wrinkle test is positive.
The Exposure
Work down through the layers behind the medial malleolus, opening the tarsal tunnel to identify and protect the tibial nerve, then develop the FDL–FHL interval onto the posteromedial tibia and posterior malleolus.
Exposure sequence
- Make a longitudinal or slightly oblique incision 1 cm posterior to the medial malleolus, extending about 10 to 12 cm proximally along the medial border of the tibia and distally toward the navicular as the pathology requires.
- Confirm the surface landmarks first: medial malleolus tip and borders, posterior tibial artery pulse, FHL tendon and the medial border of the Achilles tendon.
- Incise skin and subcutaneous fat in line with the skin incision; identify and gently protect any saphenous nerve branches encountered.
- Expose the flexor retinaculum (laciniate ligament) that roofs the tarsal tunnel.
- Divide the flexor retinaculum longitudinally, starting proximally where the tibial nerve is larger and easier to identify — the nerve lies immediately deep to the retinaculum.
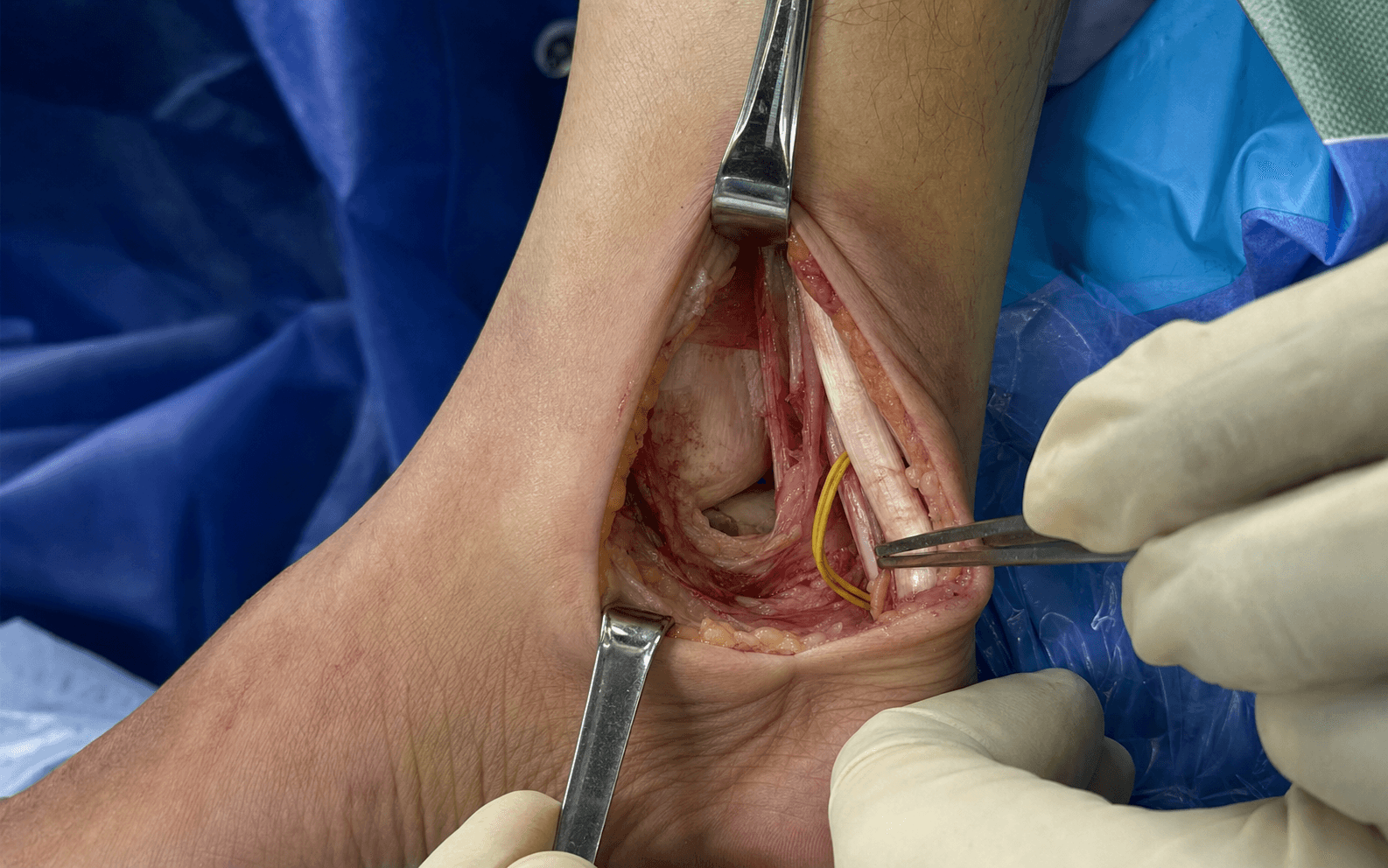
- The tibial nerve sits between FDL anteriorly and FHL posteriorly, with the posterior tibial artery and venae comitantes anterior to the nerve. Pass a vessel loop around the nerve for gentle control.
- Mobilise the tibialis posterior and FDL tendons (Tom and Dick) anteriorly.
- Develop the interval between FDL and FHL (Harry) — both muscles are supplied by the tibial nerve, but the interval is safe because the nerve branches enter the muscles proximally.
- Retract the FHL posteriorly and medially, keeping the tendon between the dissection and the tibial nerve to protect the nerve.
- Perform subperiosteal elevation of the FHL origin from the posterior distal tibia and medial malleolus.
- The posteromedial distal tibial metaphysis, medial malleolus and posterior malleolar fragment are now exposed.
- For posterior malleolus visualisation, incise the posterior capsule carefully while protecting the FHL tendon; reduce the fragment under direct vision and apply a buttress plate or posterior-to-anterior screws.
The tibial nerve is the critical structure of this approach — it supplies the posterior compartment muscles and sensation to the sole of the foot, so injury causes plantarflexion weakness, loss of toe flexion and sole numbness. Identify the nerve early in the tarsal tunnel, control it with a vessel loop, never place a metal retractor directly on the nerve, and avoid prolonged or aggressive retraction.
The tibial nerve lies between FDL anteriorly and FHL posteriorly, with the posterior tibial artery (and its venae comitantes) anterior to the nerve. Always identify and loop the nerve before retracting any structure in the tunnel.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Saphenous nerve branches
- Protection
- Identify in the subcutaneous fat and retract gently if encountered
- Structure at risk
- Tibial nerve (immediately deep to the retinaculum)
- Protection
- Open the retinaculum proximally first; vessel-loop the nerve before any retraction
- Structure at risk
- Posterior tibial artery with venae comitantes
- Protection
- Mobilise together with the nerve; avoid ligation unless exposure demands
- Structure at risk
- Tibial nerve
- Protection
- Never place a metal retractor directly on the nerve; release retraction periodically
- Structure at risk
- FHL tendon
- Protection
- Retract medially to keep it between the dissection and the nerve
- Structure at risk
- Posterior capsule
- Protection
- Incise carefully to avoid injury to the underlying FHL tendon
Extensile options. Extend proximally along the medial border of the tibia to reach the distal tibial metaphysis for pilon fracture fixation — this may require partial release of the soleus origin from the medial tibia. Extend distally toward the navicular tuberosity to reach the posterior tibial tendon insertion for repair or reconstruction, which is useful in posterior tibial tendon dysfunction surgery. Closure. Irrigate thoroughly and achieve haemostasis; a deep drain is not usually required. Close the flexor retinaculum loosely to avoid compressing the tibial nerve, approximate the subcutaneous tissue, and close skin with interrupted sutures or staples. Apply a well-padded posterior splint or cast with the ankle in neutral, and document tibial nerve function (sensation and toe flexion) postoperatively.
Procedures Through This Approach
- Posterior malleolus fixation — buttress plate or posterior-to-anterior screws for fragments greater than 25 percent of the surface or with greater than 2 mm step-off; the principal indication.
- Posteromedial pilon fragment fixation, usually combined with an anterolateral or anteromedial approach for the anterior column.
- ORIF of medial malleolus fractures as an alternative to the anteromedial approach.
- Tarsal tunnel release and posterior tibial nerve decompression — performed through the same interval.
- Posterior tibial tendon debridement, repair or transfer via the distal extension.
- FHL tendon procedures including tenolysis or transfer.
- Posteromedial ankle arthrodesis (limited).
- Herbert screw fixation of a Cedell fracture (posteromedial talar process) through this exposure.
Viva & Exam Focus
TDAVNHTARSAL TUNNEL — Tom Dick And Very Nervous Harry
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old presents after a fall with a trimalleolar ankle fracture. CT shows a large posterior malleolar fragment involving 30 percent of the articular surface with 3 mm step-off. Describe your surgical approach.”
“During a posteromedial approach for a pilon fracture, you notice the patient has new numbness on the sole of the foot and weak toe flexion postoperatively. What is your assessment?”
“A 55-year-old with a complex pilon fracture has both anterolateral and posteromedial fragments. How do you plan your surgical approaches and positioning?”
Positioning
- Prone or supine with the leg externally rotated
- Knee flexed 20 to 30 degrees relaxes gastrocnemius
- Radiolucent table for fluoroscopy
- Tourniquet optional but useful for visualisation
Tarsal tunnel contents (anterior to posterior)
- Tom: Tibialis posterior tendon (most anterior)
- Dick: Flexor digitorum longus tendon
- And Very: Posterior tibial artery with venae comitantes
- Nervous: Tibial nerve
- Harry: Flexor hallucis longus tendon (most posterior)
- Tibial nerve lies between FDL and FHL
Internervous plane
- Deep plane between FDL and FHL (both tibial nerve)
- Open the flexor retinaculum to enter the tunnel
- Tibial nerve mobilised with a vessel loop
- FHL retracted medially to protect the nerve
Danger structures
- Tibial nerve — motor and sensory deficit if injured
- Posterior tibial artery — mobilise with the nerve
- FHL tendon — protect during deep dissection
- Saphenous nerve branches — superficial risk
Key indications
- Posterior malleolus fixation (greater than 25 percent or greater than 2 mm step-off)
- Posteromedial pilon fragment fixation
- Tarsal tunnel release and nerve decompression
- Posterior tibial and FHL tendon procedures
Closure principles
- Close the retinaculum loosely to avoid nerve compression
- No deep drain routinely required
- Posterior splint with the ankle in neutral
- Document tibial nerve function postoperatively
References
Surgical approaches for the treatment of posterior malleolar fracture: which one to choose?
- The posteromedial approach provides direct access for reduction and fixation of posterior malleolar fractures
Comparison of applied tension to the postero-medial structures in the traditional and modified postero-medial ankle approaches
- Modified posteromedial ankle approaches show differences in tension applied to neurovascular structures compared to traditional
Cedell's Fracture of the Talus Managed with Herbert Screw Fixation through Posteromedial Approach
- The posteromedial approach allows safe Herbert screw fixation for Cedell fractures of the talus
Surgical Treatment of a Posterior Malleolus Fracture: Literature Review
- Direct posteromedial approaches improve reduction quality for posterior malleolus fractures in pilon and ankle injuries