Definitive treatment for symptomatic TMT arthritis via dual dorsal longitudinal incisions with meticulous neurovascular protection and selective, anatomy-informed fusion
- Post-traumatic TMT arthritis following Lisfranc injury is the most common indication, occurring in 30-50% of high-energy Lisfranc injuries and presenting with chronic pain, deformity, and functional limitation.
- Medial and middle columns (1st-3rd TMT) have approximately 1-2 degrees of motion and can be fused with minimal functional loss; the lateral column (4th-5th TMT) has roughly 10-13 degrees of motion (cuboid-4th MT and cuboid-5th MT each about 10 degrees in the Ouzounian-Shereff cadaveric model) that is essential for gait adaptation on uneven surfaces.
- The dorsalis pedis artery runs 12-15mm deep between the 1st and 2nd metatarsal bases on the first dorsal interosseous, with the deep peroneal nerve immediately lateral - it MUST be identified early and protected throughout with vessel loops.
- The fish-scale cartilage-removal technique with curved osteotomes removes all cartilage to bleeding cancellous bone; fenestration of the subchondral bone with a 2mm drill promotes healing without weakening structural integrity.
- “Indications: post-traumatic arthritis (most common, 30-50% post-Lisfranc), primary OA, inflammatory arthropathy, failed ORIF, and adult flatfoot stage 3-4 with TMT collapse.
- “Tripod foot alignment on lateral fluoroscopy: the 1st MT plantarflexed 5-10 degrees relative to the lesser MTs, creating a stable base of calcaneus, 1st MT head and 5th MT head - this prevents transfer metatarsalgia.
- “Preserve lateral column (4th-5th TMT) motion whenever possible - it provides the roughly 10-13 degrees critical for gait mechanics; fuse ONLY if symptomatic arthritis is present (Ouzounian and Shereff, 1989).
- “Rigid compression constructs (combined plate-and-lag-screw, or robust crossed screws) give the highest reported union rates; dorsal plating is the standard approach, and reported midfoot fusion union rates cluster around 80-95% in contemporary series.
When & Why
Indication. Symptomatic tarsometatarsal (Lisfranc) arthritis - midfoot pain on weight-bearing with deformity and functional limitation - that has failed conservative management (stiff-soled or rocker-bottom shoes, custom orthotics, activity modification, NSAIDs and intra-articular corticosteroid injection). The decision to operate is always preceded by weight-bearing radiographs and a CT to map every arthritic joint, because the whole strategy turns on fusing the right rays and preserving the mobile ones. The five indications, in order of frequency. - Post-traumatic arthritis (most common). High-energy Lisfranc injuries damage articular cartilage and the stabilising ligaments, and arthritis develops in 30-50% of cases, typically presenting 12-24 months after injury with persistent medial midfoot pain, deformity and loss of function despite good initial reduction.
- Primary degenerative osteoarthritis. Idiopathic TMT arthritis most often affects the 1st-2nd TMT joints, producing medial column collapse, an acquired flatfoot, metatarsalgia and callus under the 2nd-3rd MT heads, and difficulty with shoe wear.
- Inflammatory arthropathy. Rheumatoid, psoriatic and seronegative spondyloarthropathies cause synovitis, erosions and progressive multi-ray deformity, often needing more extensive fusion because of panarticular involvement.
- Failed Lisfranc ORIF. Hardware failure, loss of reduction or symptomatic post-traumatic arthritis after fixation is converted to arthrodesis, usually with hardware removal at the same sitting.
- Adult-acquired flatfoot (stage 3-4). Advanced posterior tibial tendon dysfunction produces midfoot break, abduction and medial column instability; TMT arthrodesis corrects deformity and stabilises the column when isolated reconstruction is inadequate. Assess which rays to fuse before you cut. Map every symptomatic joint clinically (palpate each TMT joint, perform the drawer test for instability) and on CT. Then decide ray-by-ray - because the three TMT columns behave very differently (see Background). The single most important decision is the lateral column:
1st TMT (medial cuneiform-1st MT). Only about 1-2 degrees of sagittal motion - a rigid lever for push-off. Fusing it loses almost no function.
2nd TMT (the recessed keystone) and 3rd TMT. Minimal motion (0.6-1.6 degrees). Fuse when symptomatic; the 2nd MT base is the bony keystone of the midfoot.
4th-5th TMT (cuboid-4th/5th MT). Roughly 10-13 degrees of motion - essential for terrain adaptation and shock absorption. Fuse ONLY if definitively symptomatic.
Contraindications. Absolute: active infection at the surgical site (stage it - debridement and antibiotics first); and severe peripheral vascular disease (non-palpable pulses, ABI of 0.5 or lower, absent pedal perfusion on angiography). Relative: current smoking (raises non-union risk 3-4 fold, to 15-25% versus 5-15% - encourage cessation at least 6 weeks pre-operatively); poorly controlled diabetes with HbA1c above 8%; severe osteoporosis; and neuropathic (Charcot) arthropathy, which demands extended fusion, plantar plating and prolonged immobilisation. Consent specifically for non-union (5-15%), dorsiflexion malunion and transfer metatarsalgia, hardware prominence needing removal (5-10%), wound problems (higher in diabetics and smokers), deep infection (1-3%), adjacent-joint arthritis (10-20% at 5 years), and neurovascular injury including dorsalis pedis injury (2-3%). Setup. Supine on a radiolucent table with a bump under the ipsilateral buttock to externally rotate the leg for AP fluoroscopy, the knee flexed 30-45 degrees over a bolster, the C-arm brought from the contralateral side, and a well-padded thigh tourniquet inflated to 250-300mmHg. Keep tourniquet time under 90-120 minutes. Single-dose first-generation cephalosporin (e.g. cefazolin 2g IV) within 60 minutes of incision - glycopeptide where there is significant beta-lactam allergy or MRSA risk.
The Operation
The goal: expose the arthritic TMT joints through dual dorsal longitudinal incisions, identify and protect the dorsalis pedis artery and deep peroneal nerve before any bone work, prepare the joint surfaces to bleeding bone with the fish-scale technique, restore tripod alignment, and stabilise with rigid compression fixation - fusing the symptomatic medial and middle columns while preserving a mobile lateral column whenever possible. The exposure is laid out in full below (and in depth on the dorsal approach to the midfoot page).
Operative sequence
- Supine on a radiolucent table; 5-10cm bump under the ipsilateral buttock to externally rotate the leg for AP fluoroscopy; knee flexed 30-45 degrees over a bolster.
- C-arm from the contralateral side for AP, lateral and oblique views without repositioning the leg; surgeon ipsilateral, assistant opposite.
- Thigh tourniquet 250-300mmHg (about systolic BP plus 100mmHg); exsanguinate by elevation or Esmarch; keep tourniquet time under 90-120 minutes.
- Confirm implants: 2.7-3.5mm dorsal locking plates (various lengths), 3.5mm cortical screws (20-50mm), 0.062-inch and 1.6mm K-wires.
- Medial incision: 8-10cm longitudinal, centred over the 2nd MT, from mid-metatarsal shaft to the naviculocuneiform joint, slightly curved to follow the metatarsal contour and positioned just medial to the palpable dorsalis pedis pulse.
- Lateral incision: 6-8cm longitudinal over the 4th MT, only if lateral column fusion is needed.
- Maintain a minimum 4cm skin bridge between the two incisions - the critical measure that prevents dorsal skin necrosis.
- For an isolated 1st TMT fusion, a single 6-8cm dorsomedial incision centred over the 1st TMT joint suffices.
- Deepen through subcutaneous fat with sharp/scissor dissection; preserve dorsal subcutaneous veins where possible (venous congestion increases oedema and wound problems) and ligate small perforators with bipolar.
- In the lateral incision, identify and protect the superficial peroneal nerve branches - typically 2-3 branches crossing the field - and mark them with vessel loops.
- Find the EHL tendon medially and the EDL tendon to the 2nd toe laterally; the neurovascular bundle runs in the interval between them.
- Palpate the dorsalis pedis pulse in the 1st-2nd interspace and develop the interval with spreading dissection down to 12-15mm, where the artery lies on the first dorsal interosseous.
- The deep peroneal nerve lies immediately lateral to the artery, usually only 2-3mm away - it supplies EHB (motor) and the first webspace (sensation).
- The artery is absent or diminutive in about 12% (peroneal-dominant variant), demanding extra care.
- Mobilise the dorsalis pedis and deep peroneal nerve with gentle blunt dissection over a 3-4cm segment and pass each into a vessel loop for constant identification.
- Use nerve-safe retractors (Army-Navy, mini-Hohmann) and check the pulse frequently to avoid compression or stretch injury.
- With the bundle protected, expose the thickened arthritic joint capsules; elevate them from the dorsal metatarsal and cuneiform surfaces with a periosteal elevator.
- Incise each capsule to be fused (1st, 2nd, 3rd TMT) longitudinally; if the lateral column is being fused, divide the EDB muscle belly in line with its fibres.
- Remove dorsal and medial osteophytes with osteotome, rongeur or burr; perform a thorough synovectomy and debridement (dense scar in post-traumatic cases is excised sharply).
- Fish-scale cartilage removal: drive curved osteotomes (6mm and 10mm) along the cartilage-bone interface from the joint periphery to the centre, removing cartilage in strips down to bleeding cancellous bone.
- Curette residual cartilage, freshen the surfaces with a burr to punctate bleeding (the paprika sign), then fenestrate the subchondral bone with a 2.0mm drill - about 5-6 perforations per surface, short of the far cortex - to invite vascular in-growth without weakening the bone.
- Flatten the oval medial cuneiform to broaden the contact area; shape the metatarsal bases to match; preserve metatarsal length (excessive resection shortens the foot and weakens fixation).
- Perform frequent trial reductions to confirm bone-to-bone contact and identify gaps before grafting.
- Correct the pattern present: flatfoot - plantar-translate and plantarflex the 1st MT to restore the medial arch (release the plantar fascia or lengthen the Achilles if equinus); cavus - dorsiflex the 1st MT and elevate the medial column; restore rotation to neutral.
- Tripod alignment is the target - three weight-bearing points (calcaneus, 1st MT head, 5th MT head). On lateral fluoroscopy the 1st MT is plantarflexed 5-10 degrees relative to the lesser MTs; on AP the medial border of the 1st MT lines up with the medial cuneiform, the 2nd MT with the middle cuneiform, and the lateral border of the 4th MT with the cuboid, with no diastasis; on oblique there is no rotational malalignment.
- Hold the corrected position with 0.062-inch or 1.6mm K-wires - typically two divergent wires per joint - bent outside the skin to prevent migration.
- Confirm alignment on AP, lateral and oblique fluoroscopy before definitive fixation.
- Pack defects after provisional fixation: local morselised osteophytes (no donor morbidity), calcaneal trephine graft (minimal morbidity), or iliac crest for large defects (counsel about donor-site pain).
- Allograft cancellous chips, DBM and bone-marrow aspirate extend the graft; BMP is off-label for TMT fusion but is an option in high-risk non-union, weighed against ectopic bone, swelling and cost.
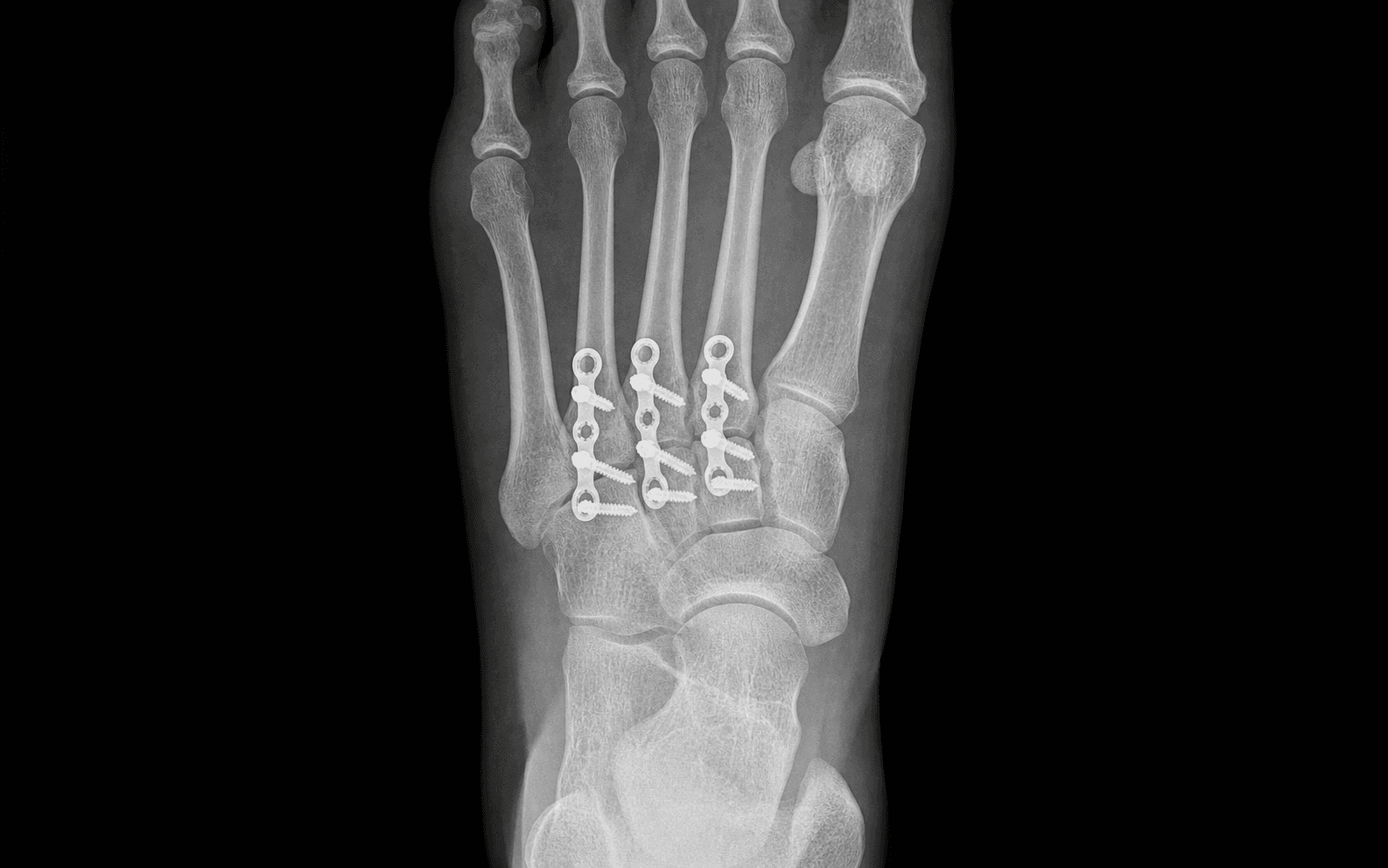
- Dorsal plates (standard): low-profile 2.7-3.5mm locking/non-locking plates contoured precisely across each joint - dorsomedial plate for the 1st TMT (medial cuneiform to 1st MT), a dorsal or bridge plate for the 2nd TMT, and an optional plate or screw-only fixation for the 3rd. Place proximal screws first, compress with a pointed clamp, then place distal screws.
- Lag screws: 3.5mm cortical screws for interfragmentary compression - drill 2.5mm across, overdrill the near cortex to 3.5mm (gliding hole), tap the far cortex. Key trajectories: medial cuneiform-to-1st MT (plantar-medial to dorsal-lateral), and the Lisfranc screw from medial cuneiform to 2nd MT base replicating the native ligament.
- Length checks: typical 1st TMT screw 35-45mm; Lisfranc screw 40-50mm; lateral column screws limited to 25-30mm. Confirm on lateral fluoroscopy that plantar penetration is 3-5mm or less.
- Combined constructs (dorsal plate plus adjunctive lag screw) are the stiffest and underpin the 80-95% union rates of contemporary midfoot series. Reserve plantar (tension-side) plating for revision or high-demand cases - biomechanically superior but with higher neurovascular risk.
- Assess the 4th-5th TMT on pre-operative CT and intra-operatively (mobility, crepitus, cartilage).
- If asymptomatic with maintained cartilage, leave it mobile - the roughly 10-13 degrees of motion is critical for gait. Unnecessary fusion creates a rigid, painful foot with accelerated adjacent-joint arthritis.
- If genuinely symptomatic, choose: temporary K-wire fixation for 6 weeks; a bridge plate without compression (allows micromotion and a fibrous union); or a lag screw for rigid fusion - the choice follows the degree of arthritis and instability.
- AP: medial border of 1st MT aligned with medial cuneiform, 2nd MT with middle cuneiform, lateral border of 4th MT with cuboid; no diastasis; hardware centred.
- Lateral: 1st MT plantarflexed 5-10 degrees relative to the lesser MTs (tripod); no dorsal or plantar subluxation; screw lengths appropriate; medial arch restored.
- Oblique: no rotational malalignment; no intra-articular hardware. Save the images for the record.
- Release the tourniquet and achieve meticulous hemostasis with bipolar; consider a closed-suction drain for extensive dissection or high bleeding risk (remove at 24-48 hours).
- Close capsules (2-0 absorbable) if tissue allows, deep fascia/EDB (2-0 absorbable), subcutaneous layer (3-0 absorbable), and skin with subcuticular 3-0 monofilament or interrupted 3-0 nylon.
- Apply a well-moulded short-leg plaster splint with the ankle neutral and the 1st MT in slight plantarflexion; a three-sided splint is more stable than a single posterior slab.
Identify and vessel-loop the dorsalis pedis before any deep dissection. It runs 12-15mm deep between the 1st and 2nd metatarsal bases on the first dorsal interosseous, and is absent or diminutive in about 12% (peroneal-dominant), which forces you to dissect more carefully rather than more confidently. If it is injured: direct pressure, extend the exposure proximal and distal, control with vascular clamps or vessel loops, and repair primarily (6-0/7-0 Prolene) for a clean laceration or perform a vein-graft interposition for segment loss - call vascular surgery early. A missed injury presenting as a cool, pulseless forefoot on day 1 is a surgical emergency: the warm-ischaemia window for the forefoot is only about 6-8 hours.
The deep peroneal nerve travels immediately lateral to the dorsalis pedis (2-3mm) - protect it with the artery in the same vessel loop and avoid excessive traction. The medial plantar bundle lies 8-10mm plantar to the medial cuneiform-1st MT joint and the lateral plantar bundle plantar to the cuboid; limit plantar dissection and confirm every screw length on lateral fluoroscopy (plantar penetration 3-5mm or less) to spare them.
Between the two dorsal incisions, maintain a skin bridge of at least 4cm. A narrow bridge necroses, exposing tendon and hardware and converting a clean elective fusion into a reconstructive problem. Place the medial incision just medial to the palpable dorsalis pedis pulse and the lateral incision over the 4th MT.
The alignment that prevents transfer metatarsalgia is checked on the lateral fluoroscan: the 1st MT should sit 5-10 degrees plantarflexed relative to the lesser MTs, restoring the tripod of calcaneus, 1st MT head and 5th MT head. A dorsiflexed 1st MT unloads the first ray and overloads the 2nd-3rd MT heads - the classic avoidable malunion.
Three words carry the joint-preparation viva: fish-scale the cartilage off with curved osteotomes to bleeding cancellous bone, burr to the punctate paprika sign of bleeding, then fenestrate the subchondral plate with a 2mm drill (5-6 holes per surface) without penetrating the far cortex - vascular in-growth without structural weakening.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation / weight-bearing | Milestones and therapy | |-------|--------|--------------------------------|------------------------| | 1 | 0-2 weeks | Short-leg splint, strict NWB (crutches or knee scooter) | Elevation, multimodal analgesia, neurovascular checks; DVT prophylaxis (aspirin 325mg or enoxaparin 40mg daily for 2-3 weeks in higher-risk patients) | | 2 | 2-6 weeks | Cast or removable boot, still NWB; K-wires removed at about 6 weeks | Wound check and radiographs at 10-14 days; confirm maintained alignment | | 3 | 6-12 weeks | PWB progressing 25 to 50 to 75% if early callus; FWB by 10-12 weeks if union (bridging on 3 of 4 cortices, obliteration of the fusion line) | CT at 12 weeks if union is questionable - the gold standard for bony bridging | | 4 | 3-6 months | Stiff-soled or rocker-bottom shoe; custom orthotics in 70-80% | Physio from 12-14 weeks: ankle ROM, peroneal and tibialis-posterior strengthening, proprioception, gait re-training | Driving resumes at 10-12 weeks once FWB (right foot) and an emergency stop is safe. Return to activity: sedentary work 2-4 weeks, light duty 8-12 weeks, full/manual work 4-6 months; low-impact sport at 4-5 months, high-impact at 6-9 months, competitive sport at 6-12 months once fusion is solid. Radiographic surveillance at 4-6 months, 1 year, then yearly for 3-5 years; symptomatic hardware is removed in 5-10% at a minimum of 12 months once union is confirmed. Outcomes. Fusion 85-95% at 12-18 months with modern fixation; significant pain relief in 80-90%; AOFAS midfoot scores typically 75-85 at 2 years; return to pre-injury activity in 70-80%; satisfaction 80-90% for post-traumatic arthritis (lower, 60-70%, for primary OA and inflammatory arthropathy because of progressive disease). Complications
- Recognition
- Persistent pain at the fusion site, tenderness, visible motion; radiographic lucency at the fusion line at 4-6 months without bridging callus; CT shows less than 25% bony bridging
- Prevention
- Smoking cessation 6 weeks pre-op; complete cartilage removal to bleeding bone; subchondral fenestration; rigid compression fixation; bone graft in high-risk patients (smokers, diabetics, osteoporosis); strict NWB for the first 6-8 weeks
- Management
- Asymptomatic: observe, supportive footwear, orthotics. Symptomatic: revision fusion - excise fibrous tissue, re-prepare surfaces, iliac crest autograft, augment fixation (add plate/screws), consider off-label BMP, strict NWB 8-12 weeks. Revision union 70-85%
- Recognition
- Transfer metatarsalgia under 2nd-3rd MT heads, plantar calluses, pain walking; lateral radiograph shows the 1st MT dorsiflexed relative to the lesser MTs (loss of tripod alignment)
- Prevention
- Meticulous intra-operative fluoroscopic alignment; 1st MT plantarflexed 5-10 degrees on the lateral view; K-wire provisional fixation with all views checked before definitive fixation
- Management
- Mild (less than 5 degrees): orthotics with a metatarsal pad, rocker-bottom shoes, activity modification. Moderate-severe (greater than 5 degrees) or failed conservative: corrective dorsal closing-wedge osteotomy at the fusion site or MT shaft with bone graft and plate; NWB 6-8 weeks
- Recognition
- Palpable prominent dorsal hardware, pain with footwear, skin tenting over the plate, localised tenderness/erythema; radiographs confirm position; exclude infection (CRP, ESR, aspiration if concerned)
- Prevention
- Low-profile 2.7-3.5mm plates contoured precisely; countersink screw heads; position plates centrally off bony prominences; counsel the patient pre-operatively
- Management
- Conservative trial first 3-6 months (wider toe box, softer shoes, padding). Failed: removal at a minimum of 12 months once solid union is CT-confirmed; protected weight-bearing 2-4 weeks; risk of recurrent deformity if removed before solid fusion
- Recognition
- Wound-edge separation, drainage (serous or purulent), exposed subcutaneous tissue or hardware, surrounding erythema; systemic signs (fever, raised WBC) if infected; black eschar if necrotic
- Prevention
- Minimum 4cm skin bridge between dual incisions; gentle tissue handling; preserve dorsal veins; meticulous hemostasis; tension-free closure; smoking cessation; diabetic optimisation (HbA1c less than 8%); strict elevation for the first 48-72 hours
- Management
- Superficial without deep infection: local wound care, sterile dressing changes, negative-pressure therapy if needed, oral antibiotics for cellulitis; heals by secondary intention over 4-8 weeks. Deep with exposed hardware: urgent debridement, retain hardware if fusion progressing, IV antibiotics per cultures, VAC or flap cover; staged removal and revision if infected non-union
- Recognition
- Drainage beyond 2 weeks, purulent discharge, fever, severe local pain, erythema beyond the incision; raised markers (WBC greater than 12, CRP greater than 100, ESR greater than 40); positive deep cultures
- Prevention
- Pre-operative cefazolin 2g IV within 60 minutes; sterile technique; minimise operative time and tissue trauma; meticulous hemostasis; tension-free closure; post-op glucose control; smoking cessation; early treatment of superficial infection
- Management
- Urgent debridement; deep bone and tissue cultures (minimum 3-5 samples); retain hardware if stable and fusion progressing, remove if loose. Empiric IV flucloxacillin 2g q6h plus ciprofloxacin 400mg q12h, de-escalate on cultures, minimum 6 weeks IV then oral suppression 3-6 months. Staged reconstruction (antibiotic spacer, revision fusion once CRP normalised); below-knee amputation for recalcitrant infection
- Recognition
- Plantar forefoot pain under 2nd-3rd-4th MT heads 3-6 months post-op, plantar calluses, worse walking; lateral radiograph may show dorsiflexion malunion or lesser MT overload
- Prevention
- Achieve tripod alignment (1st MT plantarflexed 5-10 degrees on the lateral view); avoid excessive 1st MT dorsiflexion or shortening; consider prophylactic lesser MT (Weil) osteotomies if 1st MT shortening is unavoidable; supportive footwear and orthotics early
- Management
- Conservative first-line: orthotics with a metatarsal pad proximal to the MT heads, rocker-bottom shoes, activity modification, NSAIDs, cortisone injection. Failed after 6-12 months: lesser MT shortening (Weil) osteotomies, or corrective osteotomy of a 1st MT malunion
- Recognition
- New pain proximal to the fusion (naviculocuneiform, intercuneiform) worsening despite a successful fusion; progressive radiographic joint-space narrowing, sclerosis, osteophytes and cysts; CT/MRI confirms if radiographs are equivocal
- Prevention
- Restore anatomic alignment to minimise abnormal stress; fuse only symptomatic joints (avoid over-fusion); maintain lateral column motion; patient education; annual radiographic surveillance
- Management
- Early: footwear modification, orthotics, NSAIDs, corticosteroid injections (maximum 3 per joint per year), AFO if severe. Advanced failing conservative: extend the fusion to the arthritic adjacent joint (most often the naviculocuneiform); 80-85% satisfaction, slightly lower than primary fusion
- Recognition
- Dorsalis pedis: absent pulse, cool forefoot, capillary refill greater than 3 seconds, ischaemic pain. Deep peroneal nerve: first-webspace numbness, weak or absent EHB. Plantar nerve: medial or lateral plantar numbness, painful neuroma with a Tinel sign
- Prevention
- Early identification and vessel-loop protection of the dorsalis pedis and deep peroneal nerve; nerve-safe retractors; avoid excessive traction; check the pulse frequently; limit plantar dissection; verify screw lengths on fluoroscopy (plantar penetration 3-5mm or less)
- Management
- Dorsalis pedis: intra-operative primary repair or vein-graft interposition; a missed injury presenting post-operatively is an emergency - urgent vascular consult, CT angiography, re-exploration within the 6-8 hour warm-ischaemia window. Nerve injury: primary repair if clean transection; observe incomplete or stretch injuries (most recover 3-6 months); neuroma excision with burial if refractory
Viva & Exam Focus
MEDIALMEDIAL - indications for medial/middle column fusion
TRIPODTRIPOD - the alignment that prevents transfer metatarsalgia
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old professional dancer presents 18 months after a high-energy Lisfranc injury treated with ORIF. She has failed conservative management with ongoing medial midfoot pain preventing return to dance. Examination shows tenderness over the 1st and 2nd TMT joints with drawer instability. Weight-bearing radiographs demonstrate 1st and 2nd TMT joint-space narrowing and sclerosis but preserved 3rd-5th TMT joints. How would you manage this patient and what are the critical surgical decision points?”
“Describe the functional anatomy of the TMT joints and why it is critical to preserve lateral column motion. How does this influence your surgical decision-making?”
“During exposure for a medial column TMT arthrodesis you accidentally lacerate the dorsalis pedis artery. How would you recognise this and what are your immediate steps? What if you do not recognise it intra-operatively and the patient presents on day 1 with a cool, painful, pulseless forefoot?”
Indications (MEDICAL)
- Post-traumatic arthritis after Lisfranc injury - most common, 30-50% of high-energy injuries, presenting at 12-24 months
- Primary degenerative OA with medial column collapse and flatfoot, failed conservative care
- Inflammatory arthropathy (RA, psoriatic, seronegative) with erosions and synovitis
- Failed Lisfranc ORIF with hardware failure, loss of reduction or symptomatic hardware
- Adult-acquired flatfoot stage 3-4 with TMT collapse and midfoot break
Danger zones - must protect
- Dorsalis pedis: 12-15mm deep between 1st-2nd MT on the first dorsal interosseous; vessel-loop before any deep dissection; injury risks forefoot ischaemia (absent in ~12%, peroneal-dominant)
- Deep peroneal nerve: immediately lateral to dorsalis pedis (2-3mm); motor to EHB, sensory to the first webspace
- Medial plantar nerve: 8-10mm plantar to the medial cuneiform-1st MT joint; at risk from plantar screw penetration over 3-5mm
- Superficial peroneal branches: subcutaneous over the dorsum; identify and vessel-loop in the lateral incision
Functional anatomy
- Medial/middle columns (1st-3rd TMT): 1-2 degrees motion; rigid lever for propulsion; fuse without functional loss
- Lateral column (4th-5th TMT): roughly 10-13 degrees sagittal motion (Ouzounian and Shereff 1989); preserve unless symptomatic
- 2nd MT base is the recessed keystone - the most rigid, least mobile joint
- Plantar Lisfranc ligament (medial cuneiform to 2nd MT base, 3-5mm thick) is the strongest stabiliser; no intermetatarsal ligament between 1st and 2nd MT
Technique highlights
- Dual dorsal incisions: medial 8-10cm over 2nd MT, lateral 6-8cm over 4th MT; minimum 4cm skin bridge
- Identify dorsalis pedis in the EHL-EDL interval at 12-15mm; vessel-loop the artery and nerve for the whole case
- Fish-scale to bleeding bone, burr to the paprika sign, fenestrate with a 2mm drill (5-6 holes per surface)
- Tripod alignment: 1st MT plantarflexed 5-10 degrees on lateral view; borders aligned on AP; no rotation on oblique
- Combined plate-and-lag-screw fixation (dorsal 2.7-3.5mm locking plates plus Lisfranc/adjunctive lag screws) - the stiffest construct, 80-95% union
Post-operative protocol
- Strict NWB 6 weeks; K-wires out at 6 weeks; radiographs at 2, 6 and 10-12 weeks
- PWB 6-10 weeks (25-50-75%) if early callus; FWB at 10-12 weeks if solid (bridging on 3 of 4 cortices)
- CT at 12 weeks if union is questionable - the gold standard for bony bridging
- Orthotics in 70-80%; physio at 12-14 weeks; driving at 10-12 weeks, low-impact sport 4-5 months, high-impact 6-9 months
Complications
- Non-union 5-15% primary (15-25% smokers); CT at 4-6 months; symptomatic needs revision with iliac crest graft and augmented fixation (70-85% revision union)
- Dorsiflexion malunion causes transfer metatarsalgia; mild treated with orthotics, moderate-severe with corrective osteotomy
- Hardware irritation 5-10%; remove at minimum 12 months once union is confirmed
- Adjacent-joint arthritis 10-20% at 5 years (often naviculocuneiform); extend fusion if refractory (80-85% satisfaction)
- Neurovascular injury 2-3%; dorsalis pedis injury is an emergency within the 6-8 hour warm-ischaemia window
Evidence to cite
- Ouzounian and Shereff 1989: medial/middle ~1-2 degrees vs lateral ~10-13 degrees - the basis for selective fusion
- Ly and Coetzee 2006 and Henning 2009 (Level I RCTs): primary arthrodesis beats ORIF for ligamentous/severe Lisfranc (AOFAS 88 vs 68.6; far fewer secondary surgeries, 16.7% vs 78.6%)
- Komenda et al 1996: 32 post-traumatic fusions, AOFAS 44 to 78; extent of fusion did not affect outcome
- Sangeorzan et al 1990: salvage arthrodesis, 69% good-to-excellent; alignment quality is the key determinant
- Dang/Coughlin 2020: 81.5% union; non-union linked to more joints spanned (3.6 vs 2.5)
- Shibuya et al 2013: in diabetics, neuropathy, longer surgery and HbA1c over 7% predict bone-healing complications
Background & Evidence
Pathoanatomy and epidemiology. The TMT (Lisfranc) articulation is a three-column complex. The 2nd MT base is recessed into the cuneiforms as a bony keystone, and stability rests on the ligamentous complex - the plantar Lisfranc ligament from the medial cuneiform to the 2nd MT base (3-5mm thick) is the strongest; dorsal ligaments are weak, and there is no intermetatarsal ligament between the 1st and 2nd MT, a key vulnerability in Lisfranc injury. Post-traumatic arthritis follows high-energy Lisfranc disruption in 30-50% of cases, typically declaring itself 12-24 months after injury; primary OA and inflammatory arthropathy make up the remainder, the latter often multi-ray. Functional anatomy - the basis for selective fusion. The motion data that govern the whole operation come from the cadaveric study of Ouzounian and Shereff (1989). The medial and middle columns are near-rigid; the lateral column is mobile:
- Joints
- 1st TMT (medial cuneiform-1st MT)
- Sagittal motion
- About 1-2 degrees (3.5 deg reported)
- Fusion principle
- Fuse freely - rigid lever for push-off
- Joints
- 2nd TMT (middle cuneiform-2nd MT keystone) and 3rd TMT (lateral cuneiform-3rd MT)
- Sagittal motion
- Minimal (0.6-1.6 deg)
- Fusion principle
- Fuse freely when symptomatic
- Joints
- 4th TMT and 5th TMT (cuboid-4th/5th MT)
- Sagittal motion
- About 10-13 degrees (9.6-10.2 deg)
- Fusion principle
- Preserve unless independently symptomatic
Neurovascular anatomy at risk. The dorsalis pedis - the terminal anterior tibial artery - passes under the inferior extensor retinaculum, runs between EHL and EDL to the 2nd toe, and at the TMT level lies 12-15mm deep between the 1st and 2nd MT bases on the first dorsal interosseous; it gives off the first dorsal metatarsal artery then continues as the deep plantar artery through the first interspace, and is absent or diminutive in about 12% (peroneal-dominant). The deep peroneal nerve travels immediately lateral to it (motor to EDB/EHB, sensory to the first webspace). The medial plantar bundle lies 8-10mm plantar to the medial cuneiform-1st MT joint and the lateral plantar bundle plantar to the cuboid; the superficial peroneal nerve emerges 10-12cm proximal to the ankle and branches across the dorsum between the incisions. Key evidence. Two Level I RCTs establish primary arthrodesis as superior to ORIF for purely ligamentous and severe Lisfranc injuries: Ly and Coetzee (2006) reported AOFAS 88 versus 68.6 and activity 92% versus 65% of pre-injury at a mean 42.5 months, and Henning et al. (2009) showed secondary surgery fell from 78.6% (ORIF) to 16.7% (primary arthrodesis) with no functional-score difference. Series data (Komenda 1996; Sangeorzan 1990) confirm reliable pain relief with rigid fixation and grafting, and that alignment quality and timing - not age or number of joints fused - dominate outcome. Dang and Coughlin (2020) linked non-union to the number of joints spanned (3.6 vs 2.5), and Shibuya et al. (2013) identified neuropathy, longer surgery and HbA1c above 7% as independent bone-healing risk factors in diabetics. Reported union with contemporary fixation clusters around 80-95%. Guidelines, registries and global practice. TMT arthrodesis is supported by Level I evidence and consistent series data across the AO Foundation, AOFAS and BOFAS literature, with broad international consensus that primary arthrodesis is favoured for purely ligamentous and severely comminuted Lisfranc injuries and that selective (not routine) lateral-column fusion best preserves function. National registries (NJR, AJRR, AOANJRR) track arthroplasty rather than midfoot fusion, so outcome benchmarks derive from published series. Construct choice varies by region and resource: dorsal locked plating predominates in higher-resource practice, while crossed and lag-screw fixation remains effective where plating systems are less available; compression staples and intramedullary devices are emerging adjuncts. The unifying principle across settings is meticulous joint preparation, anatomic tripod alignment and rigid compression. Perioperative prophylaxis follows WHO/AAOS principles: single-dose first-generation cephalosporin within 60 minutes (glycopeptide for beta-lactam allergy or MRSA risk); mechanical thromboprophylaxis with selective chemical prophylaxis in higher-risk patients; early NSAID use remains debated on theoretical non-union grounds.
References
In vitro determination of midfoot motion
- Cadaveric model of 10 fresh-frozen below-knee specimens measuring intertarsal motion in three dimensions
- Medial/middle column near-rigid: medial cuneiform-1st MT 3.5/1.5 deg, middle cuneiform-2nd MT 0.6/1.2 deg, lateral cuneiform-3rd MT 1.6/2.6 deg
- Lateral column mobile: cuboid-4th MT 9.6/11.1 deg, cuboid-5th MT 10.2/9.0 deg (dorsiflexion-plantarflexion / supination-pronation)
Results of arthrodesis of the tarsometatarsal joints after traumatic injury
- 32 patients fused for intractable post-traumatic midfoot pain with rigid internal fixation; autograft in 24 with a debridement defect
- Mean AOFAS midfoot score improved from 44 to 78 points (p = 0.02)
- Extent of fusion and mechanism of injury did not significantly affect outcome; one asymptomatic non-union
Locked dorsal compression plate arthrodesis for degenerative arthritis of the midfoot
- 62 patients, 173 joints fused with locked dorsal compression plates for midfoot arthritis
- Radiographic union 81.5% (141/173 joints); 14 patients with non-union
- Mean joints spanned higher in non-unions (3.6) than unions (2.5), p = 0.02
Primary arthrodesis vs ORIF for primarily ligamentous Lisfranc injuries (RCT)
- 41 patients randomized; primary arthrodesis of the medial two or three rays versus ORIF
- Mean AOFAS midfoot score 88 (arthrodesis) versus 68.6 (ORIF) at about 42.5 months, p less than 0.005
- Estimated activity level 92% versus 65% of pre-injury, p less than 0.005
ORIF versus primary arthrodesis for Lisfranc injuries: a prospective randomized study
- 40 patients (32 analysed) with acute TMT fracture-dislocations randomized to ORIF versus primary arthrodesis
- Secondary surgery (including hardware removal and salvage fusion) 78.6% after ORIF versus 16.7% after primary arthrodesis
- No significant difference in SF-36 or SMFA functional scores between groups
Salvage of Lisfranc's tarsometatarsal joint by arthrodesis
- 16 patients, 49 joints salvaged by TMT arthrodesis with rigid lag-screw fixation after failed initial treatment
- Good-to-excellent results in 11 patients (69%); symptomatic non-union at four sites in three patients
- Accurate reduction and early treatment correlated significantly with better outcome; work-related injury and long delay correlated with worse outcome
First tarsometatarsal arthrodesis: dorsomedial versus plantar plating (anatomic study)
- Cadaveric comparison of dorsomedial versus plantar plating for first TMT (Lapidus) arthrodesis in six paired specimens
- Both approaches were feasible and safe
- The dorsomedial approach more often endangered subcutaneous veins and the saphenous and superficial fibular nerves; the plantar approach more often involved smaller terminal branches of the medial plantar artery
Severe Lisfranc injuries: primary arthrodesis or ORIF?
- Comparative series of 28 patients using the Baltimore Painful Foot Score
- Complete primary arthrodesis showed more forefoot stiffness and arch loss
- Led the authors to favour ORIF or partial arthrodesis and to reserve complete arthrodesis for salvage
Factors associated with nonunion, delayed union, and malunion in foot and ankle surgery in diabetic patients
- Cohort of 165 diabetic patients undergoing foot/ankle arthrodesis, osteotomy or fracture reduction
- After multivariable adjustment, peripheral neuropathy (the strongest factor), longer surgical duration and HbA1c greater than 7% were independently associated with bone-healing complications