Lateral Epicondyle | ECRB Origin | Open + Arthroscopic | Elbow
- ECRB is the pathological tendon — angiofibroblastic hyperplasia (NOT inflammation) at its origin on the anterior facet of the lateral epicondyle.
- Conservative treatment for 6-12 months first — physiotherapy, bracing, injections, PRP, ESWT — before surgical referral.
- Roughly 80-90% success with surgery — open, percutaneous and arthroscopic techniques all give broadly comparable success rates, with no high-level evidence that one is clearly superior.
- Cozen test and Mills test are the key clinical diagnostic tests for lateral epicondylitis.
- ECRB versus ECRL — only ECRB is pathological; ECRL is superficial, radial-nerve-innervated, and uninvolved.
- “The lesion is in ECRB — not ECU or ECRL. Precise identification is mandatory.
- “Angiofibroblastic hyperplasia was described by Nirschl and Pettrone, JBJS Am 1979 — the defining histopathological description (97.7% improvement in their 88-elbow series).
- “The Dunkow RCT (JBJS Br 2004) compared open versus percutaneous release and favoured percutaneous for earlier return to work and DASH improvement.
- “The lateral collateral ligament complex originates near the lateral epicondyle — do not detach or destabilise it.
When & Why
Indication. Surgery for lateral epicondylitis (tennis elbow) is reserved for the small minority whose symptoms have persisted despite a genuine trial of non-operative care. The diagnosis is clinical: lateral elbow pain of insidious onset, worse with gripping and lifting, with point tenderness maximal 1 cm distal and anterior to the lateral epicondyle (over the ECRB origin). Three provocation tests support it: - Cozen test — resisted wrist extension with the elbow extended and forearm pronated reproduces pain.
- Mills test — passive wrist flexion with the elbow extended and forearm pronated reproduces pain.
- Maudsley test — resisted middle-finger extension reproduces pain when ECRB is involved. Investigations are adjuncts, not requirements. X-ray is usually normal but may show calcification at the lateral epicondyle. MRI shows signal change at the ECRB origin on the anterior facet, with possible partial- or full-thickness tears — useful pre-operatively for planning and to exclude other pathology. Ultrasound shows a hypoechoic area, tendon thickening and neovascularisation at the origin. Exclude concurrent pathology before attributing pain to tennis elbow. Several conditions mimic or coexist with lateral epicondylitis and change management: - Radial tunnel syndrome (PIN compression) — point of maximal tenderness 4-5 cm distal to the lateral epicondyle over the radial head and neck, pain worse with resisted supination; distinct from tennis elbow.
- Medial epicondylitis — coexists in up to 10% of cases.
- Cervical radiculopathy (C6 dermatomal overlap).
- Osteochondritis dissecans of the capitellum — particularly in younger patients or racquet-sport athletes.
- Posterior interosseous nerve entrapment — may mimic or coexist with lateral epicondylitis. Surgery is a last resort. Most patients never need it. The conservative ladder should be exhausted first: | Step | Treatment | Evidence | |------|-----------|----------| | 1 | Activity modification, NSAIDs, physiotherapy (stretching, eccentric exercises) | First-line; 80-85% resolve without surgery | | 2 | Counterforce forearm orthosis (brace) | Reduces ECRB load; symptom relief in 60-70% | | 3 | Corticosteroid injection | Large short-term (4-week) pain reduction but inferior at 26 and 52 weeks — short-term gain, long-term harm (Coombes et al, Lancet 2010) | | 4 | PRP injection (leukocyte-rich) | No difference versus needling control at 12 weeks, but significantly better at 24 weeks (84% versus 68% success) — Mishra et al, AJSM 2014 | | 5 | Extracorporeal shockwave therapy (ESWT) | Reserved for chronic refractory cases; evidence inconsistent across trials | Surgical indications. Offer surgery when there is confirmed lateral epicondylitis (Nirschl tendinosis stage 2-3) with persistent functional impairment, after: - Failed conservative treatment for a minimum of 6-12 months.
- Failure of at least 2 non-operative modalities.
- A confirmed diagnosis (clinical, plus or minus MRI or ultrasound). Relative contraindications: active infection, anticoagulation, systemic inflammatory arthropathy (treat the underlying disease first), and bilateral medial and lateral epicondylitis (which may indicate a systemic cause). The one decision — which technique. Open, percutaneous and arthroscopic releases all begin from the same principle: identify the pathological ECRB and excise it. The choice rests on surgeon experience and whether the joint needs assessment:
The taught standard. Direct visualisation of the ECRB origin, complete excision of pathological tissue, decortication and repair. Nirschl and Pettrone (1979) reported 97.7% overall improvement; pooled success around 82.7% (Kholinne 2024).
Quickest. A percutaneous tenotomy through a small stab incision. The Dunkow RCT (2004) showed around 3 weeks earlier return to work and greater DASH improvement than open release.
Allows concurrent intra-articular assessment of the capitellum, synovium and loose bodies. Pooled success around 91.9% (Kholinne 2024), but it demands elbow arthroscopy skill and strict portal safety.
Consent specifically for lateral-sided numbness or a painful neuroma, scar tenderness, residual or recurrent pain (10-20%), infection, stiffness, and the rare but serious risks of posterolateral rotatory instability and posterior interosseous nerve injury. Setup. Supine with the arm on an arm board, upper-arm tourniquet, regional or general anaesthesia. Flex the elbow to 90 degrees and pronate the forearm so the lateral epicondyle faces upward.
The Operation
The goal is to expose the ECRB origin through a short lateral incision, excise the grey pathological angiofibroblastic tissue completely, decorticate the anterior facet of the lateral epicondyle to promote healing, and repair the extensor aponeurosis — all while protecting the lateral collateral ligament complex posteriorly, the posterior interosseous nerve distally, and leaving the healthy ECRL entirely untouched. The open modified Nirschl technique is laid out step by step below; the arthroscopic alternative follows.
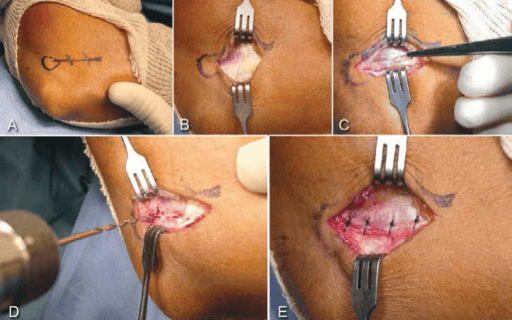
Open release — modified Nirschl technique
- Supine, arm on an arm board, upper-arm tourniquet inflated to 200-250 mmHg.
- Elbow flexed to 90 degrees, forearm pronated so the lateral epicondyle faces upward.
- Mark the lateral epicondyle and the ECRB origin — the point of maximal tenderness, 1 cm distal and anterior to the epicondyle.
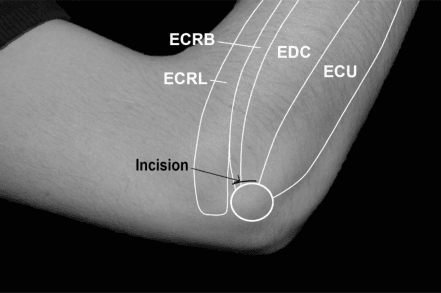
- A 4-5 cm curved or longitudinal incision centred over the lateral epicondyle, along its anterior border, from 1 cm proximal to the epicondyle to 1-2 cm distal.
- The anterior placement keeps you over the ECRB origin and away from the lateral collateral ligament complex posteriorly.
- Deepen through subcutaneous fat.
- Identify and protect the small posterior antebrachial cutaneous nerve branches crossing the field.
- Expose the common extensor aponeurosis.
- The Kaplan interval lies between ECRL (superficial, originating from the lateral supracondylar ridge) and the common extensor origin (EDC anteriorly, ECU posteriorly).
- Split the common extensor aponeurosis longitudinally, in line with its fibres, over the anterior facet of the lateral epicondyle.
- This is the internervous plane that delivers the pathological tendon into the wound.
- Retract ECRL anteriorly.
- The ECRB origin is identified on the anterior facet as grey, glistening, avascular, friable tissue — starkly different from healthy tendon, which is white, fibrous and well-organised.
- Confirm identity by tracing ECRB distally toward the base of the third metacarpal. ECRL is never released.
- With a No. 15 blade, excise ALL visible grey, degenerate tendon from the ECRB origin.
- Excision is limited to abnormal tissue — do not extend posterior to the epicondylar equator (protects the LCL complex) and do not dissect more than 1 cm distal to the radiocapitellar joint (protects the PIN).
- If the capsule has been breached during excision, or if OCD of the capitellum or synovitis is suspected, inspect the joint with a small elevator or arthroscope and debride.
- Repair the capsule if it was deliberately opened.
- Using a small rongeur, dental pick or burr, abrade the anterior facet of the lateral epicondyle.
- Create multiple small cortical perforations to promote vascularisation and biological healing.
- Repair the extensor aponeurosis with absorbable sutures (2-0 Vicryl).
- If the extensor origin was released proximally, reattach it with non-absorbable suture anchors.
- Close subcutaneous tissue and skin in layers.
- Apply a short arm splint with the wrist in 20-30 degrees of extension for 7-10 days to protect the repair.
- Physiotherapy commences at 2 weeks.
The lateral collateral ligament complex (the radial collateral and lateral ulnar collateral ligaments) originates immediately posterior and deep to the ECRB, and the posterior interosseous nerve wraps the radial neck within the supinator 1-2 cm distal to the radial head. Keep the release strictly on the anterior facet of the lateral epicondyle: never cross the epicondylar equator posteriorly (detaching the LCL and causing posterolateral rotatory instability), and never dissect more than 1 cm distal to the radiocapitellar joint (injuring the PIN). Excise only grey, pathological ECRB tissue — ECRL is superficial, radial-nerve-innervated, and must never be released.
ECRL arises from the lateral supracondylar ridge (proximal, superficial, innervated by the radial nerve proper) and is never pathological. ECRB arises from the anterior facet (deeper, more distal, innervated by the PIN) and is the sole pathological structure. Releasing ECRL removes a functioning extensor and causes radial wrist-extension weakness without any benefit. Follow the supracondylar ridge to confirm the plane, and release only grey, avascular tissue at the ECRB origin.
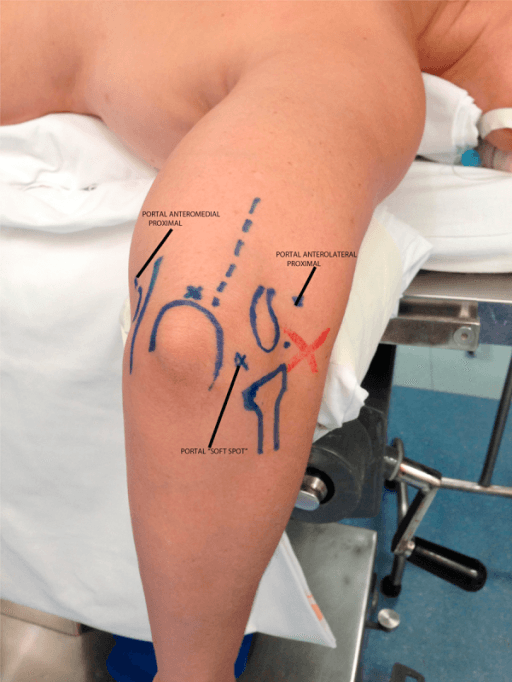
Arthroscopic release is the alternative when concurrent intra-articular assessment is wanted. Position supine (arm across the chest) or in lateral decubitus, with a tourniquet and the elbow flexed to 90 degrees. Establish three portals: a proximal medial portal (2 cm proximal and 1 cm anterior to the medial epicondyle) for inflow, an anterolateral viewing portal (1 cm distal and 1 cm anterior to the lateral epicondyle), and a proximal lateral working portal (1 cm proximal to the lateral epicondyle). Distend the joint with 20-30 mL of saline through the posterior soft spot, then survey the capitellum (OCD), synovium, coronoid and anterior capsule. The ECRB undersurface appears as grey, hypertrophic tissue at the anterolateral capsule adjacent to the radiocapitellar joint; debride it with a 4.0 mm shaver until normal extensor muscle fibres are visible.
The shaver must stay on the anterolateral capsule. Extending more than 1 cm distal to the radiocapitellar joint risks the PIN at the arcade of Frohse; extending posterior to the midline risks the LCL complex. Visualise the capsule before activating the shaver, and stop the release when healthy extensor muscle fibres come into view.
Aftercare & Complications
Immediate post-operative period (0-2 weeks). Immobilise in a short arm volar splint with the wrist in 20-30 degrees of extension for 7-10 days to protect the repair. Check the wound at 7-10 days and remove sutures or clips at 12-14 days. Simple analgesia (paracetamol, an NSAID if not contraindicated); avoid opioids beyond 48 hours. Elevate for 48 hours and ice for 20 minutes every 2-3 hours to reduce swelling. Physiotherapy programme (2-12 weeks). - Weeks 2-4 — gentle active range of motion: wrist flexion and extension, forearm pronation and supination, elbow flexion and extension. No resistance.
- Weeks 4-6 — begin isometric wrist and forearm strengthening, scar massage, and progress to light functional tasks.
- Weeks 6-12 — progressive-resistance wrist-extensor exercises (concentric and eccentric) and grip strengthening. Return to light work is permitted at 6 weeks. Return to activity. | Activity | Timeframe | |----------|-----------| | Light activities of daily living | 2-4 weeks | | Light manual work / office work | 4-6 weeks | | Moderate physical work | 8-12 weeks | | Racquet sports / heavy manual labour | 3-6 months | | Competitive sport (full intensity) | 4-6 months | Prognosis. Roughly 80-90% of patients achieve good-to-excellent outcomes (Nirschl and Pettrone 1979 reported 97.7% improved; the Kholinne 2024 meta-analysis pooled success at about 82.7% open, 91.0% percutaneous and 91.9% arthroscopic). Around 10-20% have residual symptoms or recurrence at 1-2 years. Return to work is faster after less-invasive techniques — about 3 weeks earlier with percutaneous than open in the Dunkow 2004 RCT, and around 2.2 weeks in Baker's arthroscopic series. Predictors of a poorer outcome include workers' compensation claims, bilateral disease, symptoms lasting more than 12 months, and concurrent shoulder or cervical pathology. Complications.
- Rate
- Less than 1%
- Prevention
- Restrict dissection to the ECRB origin; never extend more than 1 cm distal to the radiocapitellar joint; keep open dissection proximal to the arcade of Frohse
- Management
- Most are neurapraxias from traction — observe with a wrist and finger extension splint; EMG and NCS at 6 weeks if no recovery; explore at 3-4 months if none; tendon transfers (PT to ECRB, FCR to EDC, PL to EPL) for permanent palsy
- Rate
- Less than 1%
- Prevention
- Identify and preserve the LCL complex before dividing any tissue; restrict the release to the anterior facet only; never release posterior to the equator of the lateral epicondyle
- Management
- Posterolateral rotatory instability — brace initially; if symptomatic, LUCL reconstruction with a palmaris longus or gracilis graft via a Kocher lateral approach
- Rate
- 10-20%
- Prevention
- Complete excision of all grey tissue; adequate decortication; correct patient selection with 6-12 months of conservative treatment; address concurrent pathology
- Management
- Physiotherapy and activity modification first; MRI to confirm residual or recurrent ECRB pathology; revision open or arthroscopic release; reconsider radial tunnel syndrome or medial epicondylitis as an alternative diagnosis
- Rate
- Less than 2%
- Prevention
- Standard aseptic technique; perioperative antibiotics (cefazolin 2 g IV at induction); minimise dead space
- Management
- Superficial: oral antibiotics and wound care. Deep: surgical washout with culture-directed IV antibiotics
- Rate
- 2-5%
- Prevention
- Careful haemostasis; gentle tissue handling; layered closure; avoid perioperative NSAIDs where possible
- Management
- Haematoma: aspiration or surgical evacuation if large. Seroma: aspiration. Dehiscence: wound care, with secondary closure if deep
- Rate
- 10-15%
- Prevention
- Systematic identification of all grey degenerate ECRB tissue; decortication; intra-operative confirmation of complete excision; confirm ECRB and not ECRL was released
- Management
- Re-evaluate the diagnosis (radial tunnel syndrome, cervical radiculopathy, medial epicondylitis); MRI to confirm residual pathology; revision release of residual ECRB tissue
Viva & Exam Focus
ECRBECRB — the pathological tendon
COPECOPE — the conservative ladder
Location: wraps the radial neck within the supinator at the arcade of Frohse, 1-2 cm distal to the radial head. Risk: excessive distal dissection (open) or shaving beyond the radial neck (arthroscopic) injures a pure motor nerve, causing finger and wrist extensor paralysis with no sensory loss. Protection: keep dissection at the ECRB origin and never go more than 1 cm distal to the radiocapitellar joint.
Location: the radial collateral and lateral ulnar collateral ligaments originate from the lateral epicondyle immediately deep to the ECRB. Risk: release extending posterior to the equator detaches the complex and causes posterolateral rotatory instability. Protection: restrict the release to the anterior facet only and preserve the LCL before dividing any tissue.
Location: the capsule lies immediately deep to the ECRB origin. Risk: unintentional entry during open release, or iatrogenic cartilage damage with the shaver. Protection: excise only abnormal tissue and decorticate without entering the joint unless OCD is suspected; arthroscopically, visualise the capsule before activating the shaver.
Location: ECRL arises from the lateral supracondylar ridge (proximal, superficial, radial-nerve-innervated); ECRB arises from the anterior facet (deeper, distal, PIN-innervated). Risk: releasing ECRL removes a functioning extensor and causes radial wrist-extension weakness without benefit. Protection: follow the supracondylar ridge to confirm the plane and release only grey, avascular tissue at the ECRB origin.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old recreational tennis player presents with a 4-month history of lateral elbow pain. She is tender 1 cm distal to the lateral epicondyle, and pain is reproduced with resisted wrist extension and with passive wrist flexion with the elbow straight. How do you diagnose and manage her?”
“The patient has now failed 12 months of conservative management. You plan an open ECRB release. Walk me through the operative technique, the structures at risk, and the key intra-operative decisions.”
“Four months after open tennis elbow release, your patient returns with persistent weakness of finger and wrist extension. How do you assess, investigate and manage this?”
Pathology
- Angiofibroblastic hyperplasia (NOT inflammation)
- ECRB origin — anterior facet of the lateral epicondyle
- Nirschl and Pettrone, JBJS Am 1979
- Fibroblasts, immature collagen, NO inflammatory cells
- ECRB is the ONLY pathological tendon
Diagnosis
- Tenderness 1 cm distal-anterior to the lateral epicondyle
- Cozen test — resisted wrist extension (elbow extended)
- Mills test — passive wrist flexion (elbow extended)
- Maudsley test — resisted middle-finger extension
- MRI or ultrasound confirms ECRB signal change if needed
Conservative ladder
- Activity modification plus NSAIDs
- Eccentric physiotherapy programme
- Counterforce forearm orthosis
- Corticosteroid injection (short-term benefit only)
- PRP injection or ESWT for refractory cases
- Minimum 6-12 months before surgery
Surgical indications
- Failed 6-12 months of conservative management
- Failed at least 2 non-operative modalities
- Persistent functional impairment
- Nirschl tendinosis stage 2-3
Open release steps
- 1. Curved incision over the lateral epicondyle
- 2. Expose the extensor aponeurosis
- 3. Identify the Kaplan interval (ECRL versus common extensor)
- 4. Retract ECRL — expose the grey ECRB tissue
- 5. Excise all pathological grey tissue sharply
- 6. Decorticate the anterior facet of the lateral epicondyle
- 7. Repair the extensor aponeurosis with absorbable sutures
- 8. Layered skin closure; splint for 7-10 days
Arthroscopic technique
- Anterolateral viewing portal (1 cm distal, 1 cm anterior to the epicondyle)
- Proximal lateral working portal
- Identify the grey ECRB undersurface at the radiocapitellar margin
- Shave and debride with a 4.0 mm shaver
- Limit to the anterolateral capsule — stop within 1 cm distal to the joint line
- Allows concurrent intra-articular inspection
Danger zones
- PIN — 1-2 cm distal to the radial head (arcade of Frohse)
- LCL complex — posterior to the lateral epicondyle equator
- Radiocapitellar joint — deep to the ECRB origin
- ECRL — superficial, must NOT be released
Complications
- PIN injury less than 1% — observe, splint, EMG at 6 weeks
- LCL damage — posterolateral rotatory instability; reconstruct if unstable
- Recurrence 10-20% — revision release
- Inadequate release 10-15% — revise if residual grey tissue confirmed
- Overall success around 80-90% (Nirschl 1979; Kholinne 2024 meta-analysis)
Key references
- Nirschl and Pettrone — JBJS Am 1979 — angiofibroblastic hyperplasia, open release
- Dunkow et al — JBJS Br 2004 — RCT, open versus percutaneous (percutaneous faster recovery)
- Kholinne et al — OJSM 2024 — meta-analysis of open, percutaneous and arthroscopic success rates
- Coombes et al — Lancet 2010 — corticosteroid inferior at 6-12 months
- Buchbinder et al — Cochrane 2002 — no controlled surgical trials at the time of review
Background & Evidence
The lesion is degeneration, not inflammation. Nirschl and Pettrone (1979) established that the pathological process in tennis elbow is angiofibroblastic hyperplasia of the ECRB origin — proliferation of disorganised fibroblasts, immature type III collagen and vascular ingrowth, with an absence of true inflammatory cells. The affected tissue is grey, glistening, avascular and friable, quite unlike healthy white, fibrous, organised tendon. This is why the term 'tendinopathy' is preferred to 'tendinitis'. ECRB, not ECRL. ECRB arises from the anterior facet of the lateral epicondyle (deep to ECRL), inserts on the base of the third metacarpal, extends the wrist, and is innervated by the posterior interosseous nerve. ECRL arises more proximally from the lateral supracondylar ridge, is innervated by the radial nerve proper, and is superficial and uninvolved — it is never released. Nirschl pathological staging of tendinosis. This is a conceptual staging of progressive angiofibroblastic tendinosis attributed to Nirschl; the original 1979 Nirschl and Pettrone paper described the angiofibroblastic ECRB lesion itself.
- Description
- Inflammatory or irritative changes — reversible with conservative management
- Description
- Angiofibroblastic hyperplasia — pathological tendon, partial (less than 50%) involvement
- Description
- Angiofibroblastic hyperplasia with structural failure — complete ECRB involvement, grey avascular tendinosis tissue
- Description
- Stage 2 or 3 plus fibrosis, calcification, or frank tendon rupture — advanced end-stage disease
Key evidence. The high-level evidence does not show one surgical technique to be clearly superior. The Kholinne 2024 meta-analysis (43 studies, 1,941 elbows) pooled success at 91.9% arthroscopic, 91.0% percutaneous and 82.7% open, but the evidence base is predominantly low level. The Dunkow RCT (2004) compared open with percutaneous tenotomy and favoured percutaneous for earlier return to work and greater DASH improvement. For non-operative care, the Coombes Lancet systematic review (2010) showed corticosteroid injection gives a large short-term benefit but worse outcomes at 26 and 52 weeks than no intervention, while the Mishra RCT (2014, 230 patients) found leukocyte-rich PRP no better than needling at 12 weeks but significantly better at 24 weeks (84% versus 68% success).
References
Tennis elbow. The surgical treatment of lateral epicondylitis
- Series of 88 elbows (82 patients) operated from a cohort of 1,213 lateral tennis-elbow cases.
- Consistent lesion identified: immature fibroblastic and vascular infiltration of the ECRB origin (angiofibroblastic hyperplasia) — NOT inflammation.
- Technique: expose ECRB, excise the identified pathological tissue, then repair.
- Excellent in 66, good in 9, fair in 11, failed in 2 — 97.7% overall improvement and 85.2% returned to full activity including rigorous sport.
A comparison of open and percutaneous techniques in the surgical treatment of tennis elbow
- Prospective RCT of 45 patients (47 elbows): formal OPEN release versus PERCUTANEOUS tenotomy.
- Minimum 12-month follow-up with DASH scoring.
- Percutaneous group: significantly greater DASH improvement (p=0.001), better satisfaction (p=0.012) and around 3 weeks earlier return to work (p=0.0001).
- Conclusion: percutaneous tenotomy was quicker, simpler and produced faster recovery.
Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: a systematic review of randomised controlled trials
- Systematic review and meta-analysis of 41 RCTs (2,672 participants).
- For lateral epicondylalgia, corticosteroid injection gave a LARGE short-term pain benefit (SMD 1.44) versus no intervention.
- Effect reversed at intermediate (26-week) and long term (52-week) — no intervention was favoured.
- Serious adverse events from corticosteroid were rare (1 in 991, tendon rupture).
Efficacy of platelet-rich plasma for chronic tennis elbow: a double-blind, prospective, multicenter, randomized controlled trial of 230 patients
- 230 patients with chronic tennis elbow across 12 centres; leukocyte-rich PRP needling versus needling-only active control.
- No significant difference at 12 weeks (75.2% versus 65.9% success, p=0.104).
- By 24 weeks PRP was significantly better: 83.9% versus 68.3% success (p=0.037) and less residual tenderness (p=0.009).
- No significant complications in either group.
Comparison of clinical outcomes after different surgical approaches for lateral epicondylitis: a systematic review and meta-analysis
- 43 studies, 1,941 elbows, minimum 12-month follow-up.
- Pooled success: arthroscopic 91.9%, percutaneous 91.0%, open 82.7%.
- Largest VAS pain reduction with arthroscopic (5.54) and the best DASH and MEPS functional gains.
- Evidence base is predominantly low level (Level IV) — differences should be interpreted cautiously.
Surgery for lateral elbow pain
- Cochrane systematic review of surgery for lateral elbow pain.
- At the time of the review, NO controlled trials of surgery existed.
- The effectiveness of surgery versus placebo or no intervention could not be concluded.
Tennis elbow: its course, natural history, conservative and surgical management
- Classic description of the course, natural history and conservative and surgical management of tennis elbow.
Arthroscopic classification and treatment of lateral epicondylitis: two-year clinical results
- Cohort of 42 arthroscopic releases with an arthroscopic capsular classification (types I to III).
- 37 of 39 patients rated themselves better or much better at 2.8 years.
- Return to work averaged around 2.2 weeks.
Tendinosis of the extensor carpi radialis brevis: an evaluation of three methods of operative treatment
- Evaluation of three methods of operative treatment for ECRB tendinosis.