Arthroscopic reduction and fixation of ACL tibial avulsion · intermediate
- Meyers and McKeever classification drives management: Type I (nondisplaced) — extension cast; Type II (hinged anteriorly) — closed reduction then fixation if residual displacement greater than 2 mm; Type III (completely displaced) and Type IV (comminuted) — surgical fixation.
- Intermeniscal ligament and anterior horn of medial meniscus frequently interpose between the fragment and bed — arthroscopic clearing of this tissue is mandatory before reduction or the fracture will not reduce anatomically.
- In the skeletally immature knee all fixation must be physeal-sparing — sutures through the ACL footprint over a tibial tunnel bridge or all-epiphyseal screws avoid growth disturbance; transphyseal tunnels are contraindicated until physeal closure.
- Arthrofibrosis with loss of extension is the most common complication (up to 25 percent in some series) — aggressive early motion protocol and notchplasty if the fragment is prominent are essential to prevent this.
When & Why
Indication. A tibial spine (intercondylar eminence) avulsion is the bony equivalent of an ACL injury — the ligament stays intact and pulls off a fragment of bone. The Meyers and McKeever type drives management: a nondisplaced Type I fracture is managed in an extension cast; a Type II fracture (hinged anteriorly) is given a trial of closed reduction in extension and fixed if residual displacement exceeds 2 mm; and a completely displaced Type III or comminuted Type IV fracture needs arthroscopic reduction and fixation. Surgery is also indicated whenever interposed soft tissue prevents anatomic reduction, or when there is an associated meniscal or chondral injury that itself requires surgery. Absolute indications - Type III (completely displaced) and Type IV (comminuted) fractures
- Type II fractures with residual displacement greater than 2 mm after closed reduction in extension
- Any fracture with interposed soft tissue preventing anatomic reduction
- Associated meniscal tear or osteochondral injury requiring surgery Relative indications - Type II fracture in a high-demand athlete, or a patient unwilling to accept 6-8 weeks in a cast
- Skeletally immature patient with a Type II fracture where cast treatment risks compliance issues
- Delayed presentation with partial healing and displacement Contraindications. Absolute contraindications are active infection, soft-tissue swelling severe enough to preclude arthroscopy (consider a staged procedure), and medical comorbidity precluding anaesthesia. A nondisplaced Type I fracture, and a Type II fracture that reduces anatomically to less than 2 mm residual displacement, are managed non-operatively. The one decision that matters. Once you have decided to operate, the fixation method is chosen from the fragment morphology and the physis:
Preferred for comminuted or small fragments and for every skeletally immature patient. Two or three high-strength sutures through the ACL base, tied over a 2 cm bone bridge — no hardware to remove.
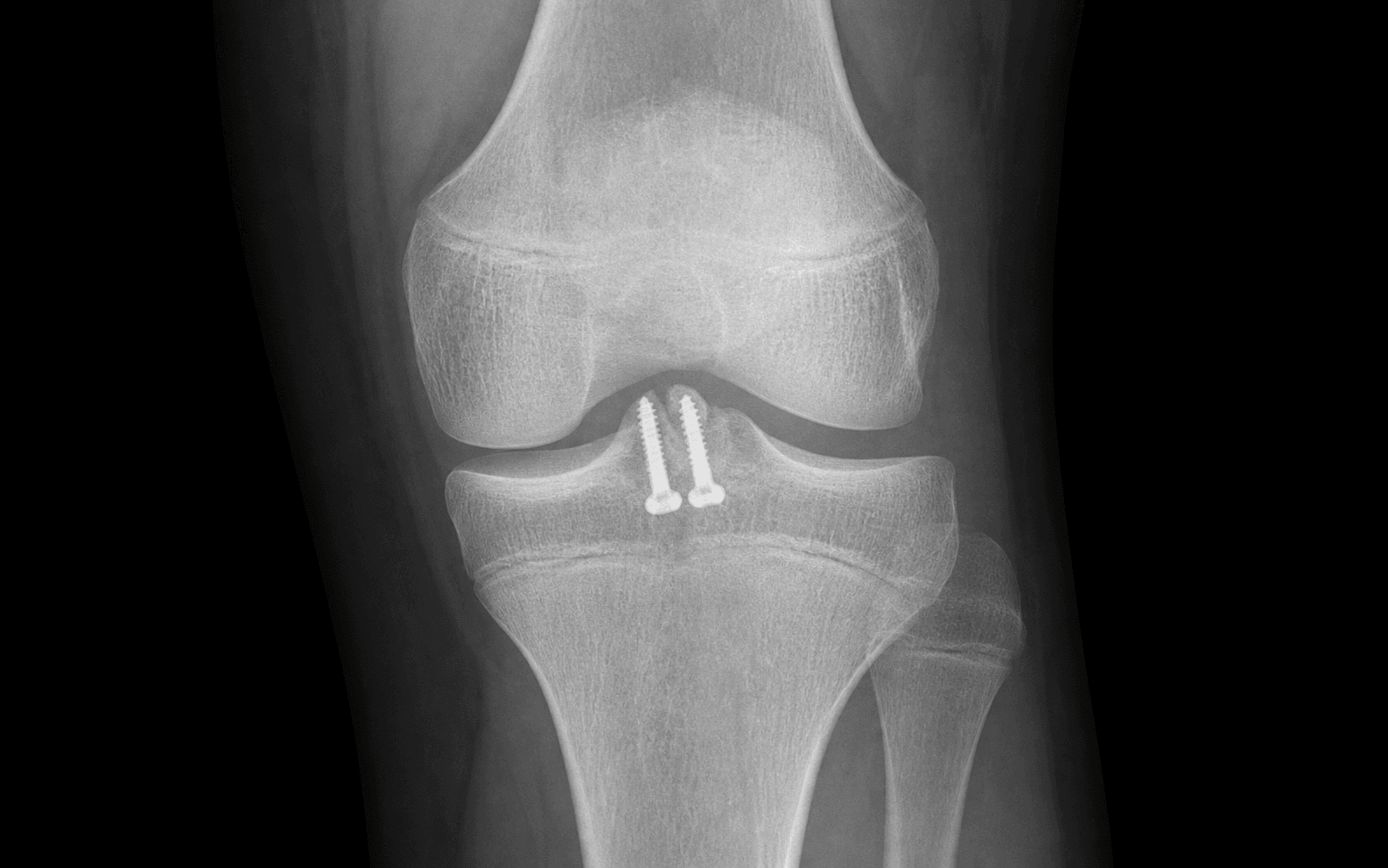
For a large single fragment (greater than 1 cm) in a patient with a closed physis. A 4.0-4.5 mm partially threaded screw with washer gives firm fixation but the hardware may need later removal.
Until skeletal maturity only suture-bridge or all-epiphyseal screw fixation is permitted — transphyseal tunnels cause recurvatum or leg-length discrepancy.
The Operation
The goal is to arthroscopically reduce the tibial spine fragment to an anatomic position, clear any interposed soft tissue, hold it with physeal-sparing fixation, and start early motion to prevent arthrofibrosis. The exposure is arthroscopic, through standard knee portals — the technique is laid out step by step below (portal anatomy is covered in depth on the knee arthroscopy approach page). Setup. Supine on a radiolucent table with a thigh tourniquet; a leg holder or post allows 90-degree flexion and full extension, with the contralateral leg in a well-leg holder. General anaesthesia with an optional adductor-canal or femoral-nerve catheter for post-operative analgesia (spinal is acceptable in adolescents). Equipment: 30-degree and 70-degree arthroscopes, standard knee instrumentation, an ACL guide, 2.4 mm and 4.5 mm cannulated drills, high-strength suture (FiberWire or equivalent), and 4.0 or 4.5 mm cannulated screws with washers if screw fixation is chosen, with C-arm fluoroscopy throughout. Consent for arthrofibrosis (10-25 percent), residual ACL laxity (5-10 percent), growth disturbance (less than 1 percent with a physeal-sparing technique), hardware prominence requiring removal, and infection (less than 1 percent).
Arthroscopic reduction and fixation — step by step
- Supine, radiolucent table, thigh tourniquet, leg holder/post for 90-degree flexion and full extension.
- Establish standard anterolateral and anteromedial portals. Perform a systematic diagnostic arthroscopy of the patellofemoral joint, both gutters and both compartments — inspect both menisci fully and address any meniscal or chondral injury before focusing on the spine.
- Inspect the tibial spine fracture. Identify the intermeniscal ligament and the anterior horn of the medial meniscus and use a probe to determine whether soft tissue is interposed within the fracture crater.
Always start with a full diagnostic sweep. In a displaced fracture expect to find the intermeniscal ligament sitting in the bed — pass a suture loop around it and retract it anteriorly, or resect the interposed portion with a shaver, before attempting reduction. If this step is skipped the fragment will not sit flush no matter how hard you push.
- Missing a bucket-handle meniscal tear in the medial or lateral compartment — always inspect both menisci fully before focusing on the spine.
- Attempting reduction with interposed tissue still present — the reduction will be non-anatomic and unstable.
- Portal placement too far medial or lateral — limits access to the spine footprint.
- Use a shaver and curette to remove haematoma and fibrous tissue from the fracture bed.
- Freshen the fragment edges and the crater walls to bleeding cancellous bone; confirm the intermeniscal ligament and meniscus are completely cleared from the interface — anatomic reduction is impossible until this is done.
- Measure the fragment size and assess comminution: a single large fragment (greater than 1 cm) favours a cannulated screw; a comminuted or small fragment favours a suture bridge.
- Flex the knee to 30-45 degrees. Use an ACL probe or elevator to reduce the fragment under direct vision, applying a posterior drawer force to the tibia while holding the fragment reduced.
- Confirm anatomic reduction — the fragment flush with the surrounding plateau on both anteroposterior and lateral fluoroscopic views.
- If reduction cannot be achieved, re-inspect for residual interposed tissue or an incarcerated meniscus.
Reduce the fragment with the knee at 30 degrees and apply a posterior drawer. Check the reduction on the lateral fluoroscopic view first — the anterior cortex must be perfectly aligned. If there is any gap, soft tissue is still interposed and you go back with the shaver.
- Over-reduction or buttonholing the fragment through the posterior cortex — risks popliteal vessel injury.
- Accepting a step-off greater than 1 mm — leads to notch impingement and extension loss.
- Forgetting to confirm reduction on a true lateral radiograph before fixation.
- Preferred for comminuted fragments and for all skeletally immature patients.
- Make a 2 cm longitudinal incision 3 cm distal to the tibial tuberosity, medial to midline. Drill two 2.4 mm tunnels from the anterior tibial cortex, exiting in the ACL footprint on either side of the reduced fragment.
- Pass a suture passer (or Hewson suture passer) through each tunnel. Using a suture lasso or bird-beak, pass two or three high-strength sutures through the base of the ACL just above the fragment, and retrieve them through the tibial tunnels.
- Tie the sutures over a 2 cm bone bridge on the anterior tibia with the knee in full extension. Confirm reduction and stability arthroscopically and fluoroscopically, and cycle the knee through a full range of motion to verify no loss of fixation.
- For a large single fragment in a patient with a closed physis.
- Reduce the fragment. Insert a guide wire from the anteromedial tibia through the fragment under fluoroscopic guidance, avoiding the physis; confirm wire position on anteroposterior and lateral views.
- Drill with a 4.0 mm cannulated drill over the wire, measure the length, and insert a 4.5 mm partially threaded cannulated screw with a washer — the screw should engage the posterior cortex but not protrude excessively.
- Perform a notchplasty if the reduced fragment remains proud greater than 2 mm.
- Confirm anatomic reduction, stable fixation and full extension under direct vision and fluoroscopy.
- Irrigate the joint. Close the portals with absorbable suture. Apply a sterile dressing and an extension brace.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | Day 0-14 | Brace locked in full extension for 2 weeks (suture) or 4 weeks (screw) | Passive extension to zero immediately; cryotherapy and elevation for 48-72 hours | | 2 | Weeks 2-6 | Removable functional brace from week 2-4 | Prone hangs and heel props; quadriceps sets and straight-leg raises; patellar mobilisation; active-assisted flexion from week 2 | | 3 | Weeks 6-12 | Brace for heavy tasks only | Progressive resistance; stationary cycling when range allows; proprioceptive training | | 4 | Months 3-9 | None | Return to running at 3-4 months if radiographic union and full painless range; return to sport at 6-9 months after isokinetic strength and hop testing | In children, compliance with the brace and non-weight-bearing is the challenge — involve the parents and consider a removable cast or a hinged brace with a lock. Obtain serial radiographs at 2, 6 and 12 weeks to confirm maintenance of reduction and physeal integrity, and follow with scanograms until skeletal maturity if there is any physeal concern. Post-operative extension loss greater than 5 degrees is unacceptable — pursue aggressive physiotherapy and consider a manipulation under anaesthesia at 6-8 weeks if motion is not progressing. Outcomes. Anatomic reduction with stable fixation yields greater than 90 percent good-to-excellent results (Lysholm greater than 90). Residual extension loss greater than 5 degrees occurs in 5-10 percent despite optimal care. Return to pre-injury sport level is 80-90 percent in adolescents with anatomic reduction. Long-term ACL laxity is present in 10-15 percent but symptomatic instability requiring reconstruction is uncommon (less than 5 percent) when the reduction is anatomic. Complications
- Incidence
- 10-25 percent
- Recognition
- Inability to achieve full extension by 6-8 weeks; painful end-range extension; quadriceps-avoidance gait
- Prevention and management
- Prevention: anatomic reduction, notchplasty if the fragment is prominent, immediate passive extension from day 1, night extension splint. Management: aggressive physiotherapy; manipulation under anaesthesia at 6-8 weeks if extension loss greater than 10 degrees; arthroscopic lysis of adhesions if manipulation fails
- Incidence
- 5-15 percent
- Recognition
- Positive Lachman or anterior drawer; pivot-shift glide; patient reports giving-way
- Prevention and management
- Prevention: anatomic reduction restoring ACL footprint tension; secure fixation allowing early motion. Management: functional bracing; consider ACL reconstruction if symptomatic instability persists beyond 6 months and the patient is skeletally mature
- Incidence
- less than 5 percent
- Recognition
- Persistent pain at 3 months; visible gap on radiograph; displacement on stress views
- Prevention and management
- Prevention: anatomic reduction, stable fixation, compliance with non-weight-bearing. Management: revision fixation with bone grafting if symptomatic; accept if asymptomatic with no instability
- Incidence
- less than 1 percent with physeal-sparing
- Recognition
- Leg-length discrepancy or recurvatum on scanogram; angular deformity on standing alignment radiograph
- Prevention and management
- Prevention: strict physeal-sparing fixation (suture bridge or all-epiphyseal screw); confirm physis location on pre-operative MRI. Management: epiphysiodesis of the contralateral limb or corrective osteotomy after skeletal maturity if clinically significant
- Incidence
- 5-10 percent with screw fixation
- Recognition
- Painful palpable screw head; bursitis over the anterior tibia
- Prevention and management
- Prevention: countersink the screw head; prefer suture fixation in thin patients or athletes. Management: screw removal after fracture union (usually 6-12 months)
- Incidence
- less than 1 percent
- Recognition
- Erythema, swelling, warmth, elevated CRP, fever
- Prevention and management
- Prevention: sterile technique, prophylactic antibiotics, meticulous haemostasis. Management: aspiration and culture-directed antibiotics; arthroscopic washout if deep infection is suspected
Viva & Exam Focus
SPINESPINE — Meyers and McKeever thresholds
FIXFIX — choosing the fixation
Four structures and pitfalls catch candidates in the viva — know each one cold.
The trap — attempting reduction without clearing the intermeniscal ligament or the anterior horn of the medial meniscus results in persistent displacement and malunion. The fix — use a probe or shaver to inspect the fracture bed; the ligament often lies within the crater. Resect the interposed portion or retract it with a suture loop before reducing the fragment. Anatomic reduction is impossible until this step is complete.
Location — the proximal tibial physis lies immediately posterior and distal to the tibial spine footprint. Risk — transphyseal tunnels or screws cause growth arrest or angular deformity. In the immature knee use only physeal-sparing techniques (a suture bridge over an epiphyseal tunnel, or all-epiphyseal screws). Verification — confirm skeletal age with a hand radiograph or the physeal appearance on knee MRI before choosing the fixation method.
Location — a Type II fracture that appears reduced in extension may still have greater than 2 mm displacement on the lateral radiograph. Risk — malunion leads to extension loss and ACL laxity. The threshold for surgery is residual displacement greater than 2 mm after attempted closed reduction. Action — obtain a true lateral radiograph in full extension; if the gap exceeds 2 mm proceed to arthroscopic fixation.
Deformity — a prominent reduced fragment or malunion can cause notch impingement and a fixed flexion contracture. Prevention — perform a notchplasty if the reduced spine remains prominent; ensure anatomic reduction so the fragment sits flush with the surrounding plateau. Examination — measure extension with the patient supine and the heel supported; any block greater than 5 degrees requires intervention.
Why it matters — the proximal tibial physis contributes about 60 percent of longitudinal growth; injury or iatrogenic damage produces leg-length discrepancy or recurvatum. Implication — all fixation in open-physis patients must avoid the physis. Follow patients with serial scanograms until skeletal maturity if any physeal concern exists.
Incidence — up to 40 percent of tibial spine fractures have associated meniscal tears or osteochondral lesions. Implication — thorough diagnostic arthroscopy of the medial and lateral compartments is mandatory before focusing on the spine. Missed bucket-handle tears lead to chronic instability and early arthritis.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 12-year-old gymnast sustains a hyperextension injury to her right knee during a vault. A lateral radiograph shows a displaced tibial spine fracture with the fragment elevated 5 mm anteriorly. MRI confirms a Type III fracture with intermeniscal ligament interposition and an open physis. How do you manage her?”
“You have reduced a comminuted Type IV tibial spine fracture in a 16-year-old soccer player with a closed physis. The fragment is too small and fragmented for screw fixation. Describe your fixation technique and post-operative plan.”
“A 9-year-old boy underwent suture fixation of a Type III tibial spine fracture 7 days ago. At his first post-operative visit he has a 15-degree extension lag and only 40 degrees of flexion. MRI shows no mechanical block but diffuse synovitis. What is your management?”
Classification and thresholds
- Meyers and McKeever: Type I nondisplaced — cast; Type II hinged — fix if residual greater than 2 mm after extension; Type III displaced and Type IV comminuted — surgery
- Intermeniscal ligament interposition in greater than 50 percent of displaced fractures — clear before reduction
- Anatomic reduction (less than 1 mm step-off) is mandatory to prevent extension loss and ACL laxity
- Skeletally immature: all fixation must be physeal-sparing (suture bridge or all-epiphyseal screw)
Surgical anatomy
- ACL footprint on the medial tubercle of the intercondylar eminence; the physis lies 3-5 mm posterior and distal
- The intermeniscal ligament crosses anterior to the spine — the most common cause of an irreducible fracture
- The popliteal artery lies 1-2 cm posterior to the plateau — avoid posterior perforation
- Notch width 18-22 mm — a prominent fragment causes impingement and an extension block
Indications for surgery
- Type III and IV fractures — absolute indication
- Type II with residual displacement greater than 2 mm after closed reduction
- Any fracture with interposed soft tissue preventing anatomic reduction
- Associated meniscal or chondral injury requiring surgery
Fixation options
- Suture bridge over a tibial bone bridge: preferred for comminuted fragments and open physis; two or three high-strength sutures through the ACL base
- Cannulated screw (4.0-4.5 mm with washer): large single fragment in a closed physis; avoid in children
- Physeal-sparing is mandatory until skeletal maturity — confirm the physis on pre-operative MRI
- Notchplasty if the reduced fragment remains proud greater than 2 mm
Danger zones
- Interposed intermeniscal ligament or meniscus — prevents anatomic reduction
- Proximal tibial physis — transphyseal fixation causes recurvatum or leg-length discrepancy
- Popliteal vessels — posterior perforation with a drill or guide wire
- Prominent reduced fragment — notch impingement and a fixed flexion contracture
Complications
- Arthrofibrosis / extension loss: 10-25 percent — the most common; prevent with immediate motion and notchplasty
- Residual ACL laxity: 5-15 percent — anatomic reduction reduces the incidence
- Growth disturbance: less than 1 percent with physeal-sparing technique
- Nonunion: less than 5 percent — revision with bone graft if symptomatic
Post-operative protocol
- Extension brace for 2-4 weeks; toe-touch weight-bearing for 4-6 weeks
- Immediate passive extension exercises; active flexion from week 2
- Full range-of-motion goal by 6-8 weeks; return to sport at 6-9 months after strength testing
- Serial radiographs and scanograms until skeletal maturity in children
Background & Evidence
Surgical anatomy ACL footprint and tibial spine. The ACL tibial footprint occupies the anteromedial aspect of the intercondylar eminence. The intercondylar eminence bears two tubercles — medial and lateral — and the ACL attaches to the medial tubercle and its anterior slope. In adults the footprint measures approximately 10-12 mm anteroposteriorly and 8-10 mm mediolaterally; in children it is proportionally larger relative to the plateau and lies closer to the physis. Proximal tibial physis. The physis lies 3-5 mm posterior and distal to the posterior margin of the ACL footprint. It is undulating and slopes proximally in the midline, so any tunnel or screw directed posteriorly risks physeal penetration. In the skeletally immature knee the physis must be visualised on a pre-operative MRI or intra-operative fluoroscopy so that all fixation remains epiphyseal. Intermeniscal ligament and meniscus. The intermeniscal (transverse geniculate) ligament crosses the anterior intercondylar area immediately anterior to the tibial spine. In greater than 50 percent of displaced fractures the ligament or the anterior horn of the medial meniscus becomes interposed between the fragment and its bed, and the anterior horn may flip into the crater — failure to clear these structures prevents anatomic reduction. Neurovascular structures at risk. The popliteal artery lies 1-2 cm posterior to the tibial plateau at the level of the spine, so posterior perforation with a drill or guide wire risks vascular injury. The common peroneal nerve is protected laterally but can be injured with aggressive lateral-compartment retraction, and the infrapatellar branch of the saphenous nerve is at risk with anteromedial portal placement. Notch anatomy. The intercondylar notch width averages 18-22 mm; a prominent reduced fragment can cause notch impingement and an extension block. A limited notchplasty (resection of the anterior notch roof) is indicated when the reduced fragment remains proud greater than 2 mm. ### Meyers and McKeever classification
- Description
- Nondisplaced or minimally displaced
- Management
- Extension cast or brace for 4-6 weeks
- Description
- Anteriorly hinged, posterior cortex intact
- Management
- Closed reduction in extension; fix if residual greater than 2 mm
- Description
- Completely displaced, no cortical continuity
- Management
- Arthroscopic reduction and fixation
- Description
- Comminuted or rotated
- Management
- Arthroscopic or open reduction with suture or screw fixation
Evidence for the fixation threshold - Residual displacement greater than 2 mm after closed reduction correlates with extension loss and ACL laxity across multiple series.
- Anatomic reduction (less than 1 mm step-off) restores ACL footprint tension and reduces the risk of arthrofibrosis.
- In skeletally immature patients, physeal-sparing fixation yields excellent outcomes with minimal growth disturbance when performed correctly.
References
Tibial spine fractures in children and adolescents: a multicenter study
- Retrospective review of 83 children with tibial spine fractures
- Type II and III fractures treated with arthroscopic or open reduction showed superior outcomes to cast alone when displacement exceeded 2 mm
- Arthrofibrosis occurred in 25 percent of patients; an early motion protocol reduced the incidence
Arthroscopic suture fixation of tibial spine avulsion fractures
- Case series of 12 patients using a suture bridge technique over a tibial tunnel
- All fractures achieved anatomic reduction; no growth disturbance in open-physis patients
- Mean Lysholm score 94 at 2-year follow-up
Comparison of screw versus suture fixation for tibial eminence fractures
- Biomechanical study comparing cannulated screw and suture fixation in cadaveric knees
- Suture fixation demonstrated equivalent load to failure and less fragment comminution during insertion
- Suture technique preferred when fragment size is less than 1 cm or comminuted
Physeal-sparing fixation of tibial spine fractures in skeletally immature patients
- Series of 18 skeletally immature patients treated with all-epiphyseal screw or suture fixation
- No cases of growth arrest or angular deformity at mean 3.2-year follow-up
- All patients achieved full extension and returned to sport
Incidence and risk factors for arthrofibrosis after tibial spine fixation
- Retrospective review of 32 patients undergoing tibial spine fixation
- Arthrofibrosis requiring intervention occurred in 25 percent; risk factors included delayed surgery greater than 7 days and prolonged immobilisation
- An early motion protocol reduced the arthrofibrosis rate to less than 10 percent
Laxity and functional outcome after arthroscopic reduction and internal fixation of displaced tibial spine fractures in children
- Arthroscopic reduction and internal fixation of displaced tibial spine fractures in children yields good functional outcomes with low residual laxity
- Early motion after fixation reduces arthrofibrosis risk
Suture Versus Screw Fixation of Tibial Spine Fractures in Children and Adolescents: A Comparative Study
- Comparative study of suture versus screw fixation for tibial spine fractures in children and adolescents
- Both techniques effective with high healing rates; suture fixation avoids hardware complications in skeletally immature patients
Range of Motion Improvement Following Surgical Management of Knee Arthrofibrosis in Children and Adolescents
- Surgical management of knee arthrofibrosis after tibial spine fixation improves range of motion in children and adolescents
- Early intervention for arthrofibrosis yields better outcomes
Tibial Spine Avulsion Fractures: A Focus on Arthroscopic Treatment and Rehabilitation
- Arthroscopic treatment of tibial spine avulsion fractures with a structured rehabilitation protocol
- Emphasis on anatomic reduction and early motion to optimise outcomes