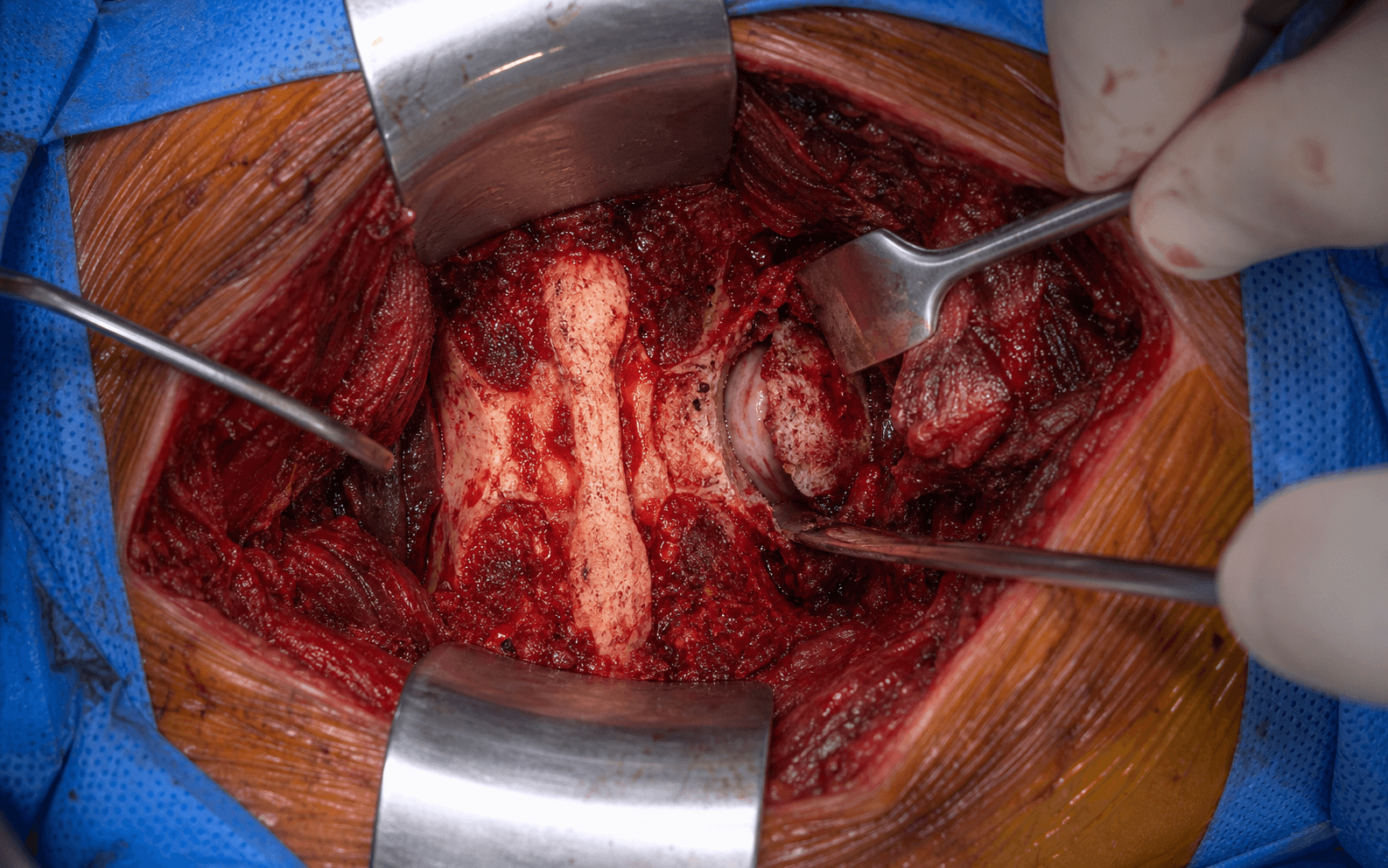
Unilateral facetectomy · Kambin's triangle · exiting nerve root at risk
- Kambin's triangle (safe zone): triangular working space in the lumbar foramen bounded by the exiting nerve root (superior/hypotenuse), the traversing nerve root (medial), and the superior endplate of the caudal vertebra (base). It provides a corridor for transforaminal disc access that avoids thecal-sac and traversing-root retraction (Kambin and Sampson 1986; cadaveric working-triangle area mean approximately 1.8 cm², Hardenbrook 2016).
- TLIF vs PLIF advantages: unilateral facetectomy preserves the contralateral facet and posterior tension band and mobilises only ONE nerve root (the exiting root) rather than retracting the thecal sac and traversing roots bilaterally. Comparative series show a TREND to fewer durotomies (TLIF approximately 9% vs PLIF approximately 17%) and less iatrogenic nerve-root dysfunction (TLIF approximately 2% vs PLIF approximately 8%), with EQUIVALENT fusion and pseudarthrosis rates (Mehta 2010).
- Exiting nerve root is MOST vulnerable: it lies in the SUPERIOR foramen, immediately deep to the superior articular process, and exits ABOVE the pedicle of the caudal vertebra (for example, the L4 nerve exits the L4–5 foramen above the L5 pedicle). It is injured chiefly during facetectomy/SAP resection, by a too-lateral or too-superior upper pedicle screw, or by aggressive lateral retraction during disc and cage work.
- Facetectomy technique is CRITICAL: perform a COMPLETE unilateral facetectomy (resect the inferior articular process of the cephalad vertebra, then the superior articular process of the caudal vertebra) to fully unroof the foramen and expose both traversing and exiting roots BEFORE disc access. Use a Kerrison rongeur or osteotome for the final bone over the nerve rather than an uncontrolled high-speed burr, and positively identify and protect the exiting root before instrumenting the disc.
- Cage insertion through Kambin's triangle: a single cage is inserted from one side, advanced obliquely and positioned to sit anteriorly across the midline of the disc on AP fluoroscopy (NOT left posterolaterally in the foramen where it would compress the exiting root). Cage height restores collapsed disc height without over-distraction (oversizing fractures the endplate and causes subsidence); a lordotic cage helps restore segmental lordosis.
- Global practice: TLIF is a first-line posterior interbody option for single- and two-level degenerative disease (spondylolisthesis, degenerative disc disease with instability, recurrent disc herniation) across contemporary practice. MIS-TLIF (tubular or expandable muscle-sparing retractor) reduces blood loss, surgical-site infection and length of stay versus open TLIF with equivalent fusion and patient-reported outcomes (Phan 2015).
When & Why
What it exposes. Transforaminal lumbar interbody fusion (TLIF) is a posterior lumbar fusion technique that accesses the disc space through a unilateral facetectomy and a transforaminal corridor (through the neural foramen), inserting a single interbody cage from ONE side while preserving the CONTRALATERAL facet and the posterior tension band. It was popularised by Harms and Rolinger as a modification of PLIF (posterior lumbar interbody fusion) to reduce neurological morbidity: the transforaminal approach mobilises only ONE nerve root (the exiting root) and avoids the BILATERAL thecal-sac and traversing-root retraction that PLIF demands. The critical anatomic concept — Kambin's triangle. This is the transforaminal "safe working zone", a triangular corridor in the posterolateral foramen bounded by: (1) the exiting nerve root (the superior, oblique hypotenuse — for example the L4 root crossing the upper L4–5 foramen), (2) the traversing nerve root and dural sac (the medial, vertical border — for example the L5 root descending to exit at L5–S1), and (3) the superior endplate of the caudal vertebra (the inferior border or base). A trapezoidal "safe zone" lies immediately superior to the caudal pedicle and is free of nerve roots; this is the target for disc access. Kambin's transforaminal access principle was first described clinically by Kambin and Sampson (1986), and the working-triangle dimensions have since been quantified in cadaveric studies (mean working-triangle area approximately 1.8 cm², largest at L5–S1 — Hardenbrook 2016). Why TLIF over PLIF. (1) Unilateral facetectomy preserves the contralateral facet and posterior tension band, theoretically reducing adjacent-segment stress compared with the bilateral facetectomy of PLIF. (2) Single-root mobilisation — only the exiting root is retracted, rather than the thecal sac and both traversing roots, with a comparative series showing a TREND to fewer durotomies (approximately 9% TLIF vs approximately 17% PLIF) and less iatrogenic nerve-root dysfunction (approximately 2% vs approximately 8%), all transient in that series (Mehta 2010). (3) Equivalent fusion — TLIF and PLIF achieve comparable interbody fusion rates, both higher than instrumented posterolateral fusion alone (Makanji 2018). Indications (consistent across advanced orthopaedic practice): - Degenerative spondylolisthesis (Grade I–II) — the MOST COMMON indication.
- Isthmic spondylolisthesis (Grade I–II) with instability.
- Degenerative disc disease with instability or failed conservative management (more than 6 months of physiotherapy, injections and medication).
- Recurrent disc herniation after prior discectomy (unstable segment).
- Adjacent segment disease after prior fusion.
- Post-laminectomy instability. Relative contraindications. High-grade spondylolisthesis (Grade III–IV), where TLIF access is difficult and ALIF may give better reduction and anterior load-sharing; severe central stenosis requiring extensive bilateral laminectomy (PLIF or decompression alone); severe osteoporosis with high subsidence risk (consider ALIF for better endplate contact or supplemental anterior support); and infection or tumour, which require a different approach. Position. Prone on a Jackson table or Wilson frame with hip flexion 30–45° to open the interlaminar space and reduce lumbar lordosis. Chest and iliac-crest support avoid abdominal compression (this reduces epidural venous pressure and bleeding). Arms on arm boards (shoulder 90°, elbow 90°); face on a horseshoe or mirror headrest with eye checks every 30–60 minutes. General anaesthesia is standard; intraoperative neuromonitoring (somatosensory and motor evoked potentials, and free-running/triggered EMG) is a common adjunct in many centres, though its routine use varies between units and remains an adjunct to — not a substitute for — sound technique. Position fluoroscopy for AP and lateral lumbar views and confirm the level before incision.
The Exposure
Work down through the posterior lumbar layers in the midline, place the pedicle screws first, then perform the defining step of TLIF — a complete unilateral facetectomy that unroofs the foramen and exposes both roots — before entering the disc through Kambin's triangle.
Exposure sequence
- Obtain a lateral fluoroscopy image and identify the target level by counting from L5 (the most caudal lumbar vertebra with a disc space) upward.
- Mark a midline incision over the spinous processes, centred on the target level and extending one to two levels above and below (for an L4–5 TLIF, from the L3 to the L5 spinous process — about 6–8 cm). A paramedian incision 2–3 cm lateral to the midline is used for MIS-TLIF.
- Incise skin and subcutaneous tissue in the midline down to the thoracolumbar fascia; divide the fascia in the midline over the spinous processes (a bloodless plane) for the full length of the incision.
- Elevate the paraspinal muscles (multifidus, longissimus) subperiosteally off the lamina and facets with electrocautery or a Cobb elevator — stay on bone to reduce bleeding.
- Expose the lamina, spinous process, facet joints and transverse processes (the lateral limit, where pedicle screws are placed). Place a self-retaining retractor (for example McCullough or Caspar) and confirm the level with a lateral fluoroscopy marker.
- Identify the bilateral pedicle entry points at the target level (and the adjacent level for a multi-level construct). Landmarks are the mamillo-accessory notch on the transverse process, or the junction of the lateral pars and superior facet (the "eye of the Scotty dog" on lateral fluoroscopy), typically 3–5 mm lateral to the facet and 2–3 mm inferior to the superior endplate of the pedicle.
- Decorticate the entry point with a burr, then probe the pedicle (Lenke or Magerl probe) directed 10–15° convergent in the transverse plane and parallel to the endplates in the sagittal plane, advancing 40–45 mm and palpating all four walls.
- Critical: if a wall is breached, remove the probe and redirect — do not advance through a medial (canal) or lateral (foraminal/exiting root) breach. Tap the pedicle and confirm trajectory on AP and lateral fluoroscopy.
- Insert the screws (typically 5.5–6.5 mm diameter, 40–50 mm length). Perform triggered EMG on each screw — a threshold greater than 8–10 mA is safe; a threshold less than 8 mA raises concern for a medial/foraminal breach and warrants re-inspection or repositioning. Leave the screw heads tall (do not fully seat) so the rod can be connected later without compressing the decompression site.
- TLIF is performed unilaterally. Choose the pathology side if lateral-recess or foraminal stenosis predominates there (combining decompression with fusion); otherwise choose by surgeon preference (right-handed surgeons often prefer the right side), preserving the contralateral facet.
- On the working side, use a Kerrison rongeur to remove the inferior portion of the lamina of the cephalad vertebra (for example the L4 lamina for an L4–5 TLIF), medial to the facet, exposing the ligamentum flavum and the superior edge of the facet joint. This creates the space for the facetectomy and access to the foramen.
- This is what opens the transforaminal corridor. Resect the inferior articular process of the cephalad vertebra first, then the superior articular process of the caudal vertebra down to the level of the pedicle, fully unroofing the foramen. Save and morselise the resected facet — it is excellent local autograft.
- Technique: incise the facet capsule; take the IAP with an osteotome, Kerrison or burr to expose the underlying SAP; thin and resect the SAP until the foramen is unroofed, switching to a Kerrison rongeur or osteotome (tactile feedback) for the final bone over the nerve rather than plunging with a burr. Keep irrigation on — bone dust obscures the root and heat damages nerve.
- With the foramen unroofed, positively identify both roots: the exiting root in the superior foramen (a soft, pale structure crossing above the caudal pedicle) and the traversing root and dural sac medially. Palpate the exiting root gently with a blunt nerve hook or ball-tip probe to confirm it is mobile and out of the working corridor before any disc access.
- After the facetectomy, remove the ligamentum flavum from the interlaminar space with Kerrison rongeurs, starting laterally at the facet and working medially. The ligamentum is thick (3–5 mm) and yellow.
- This exposes the epidural space, the thecal sac medially and the exiting root laterally, completing the central and lateral-recess decompression.
- Confirm the triangle's borders: the exiting root (superior/oblique hypotenuse, already exposed), the traversing root and dural sac (medial, covered by epidural fat), and the superior endplate and pedicle margin of the caudal vertebra (base).
- Using a number 15 blade on a long handle, make an annulotomy (about 10–12 mm) over the lateral disc space within the triangle, between the exiting and traversing roots, using the nerve-free supra-pedicular safe zone.
- Remove the nucleus with pituitary rongeurs and angled curettes, then extend the discectomy circumferentially — anterior, contralateral and posterior — aiming for a 360° clearance down to both endplates.
- Reach the contralateral side through the unilateral annulotomy using angled curettes and reverse-angle rongeurs, working around the thecal sac anteriorly.
- Preserve the posterior longitudinal ligament (PLL) — it is the posterior boundary separating the disc from the thecal sac; violating it risks a CSF leak. Complete discectomy is essential for fusion: residual disc blocks graft incorporation and causes pseudarthrosis.
- Remove the thin cartilaginous endplate (0.5–1 mm) from both endplates with curettes or scrapers to expose bleeding cancellous bone.
- Preserve the subchondral bony endplate — it gives structural support and resists subsidence. Over-aggressive preparation (removing the subchondral plate) is a leading cause of cage subsidence (8–15%).
- Measure disc height and depth with trials or calipers. Typical sizing: height 10–12 mm at L4–5 (8–10 mm at L5–S1), depth 25–30 mm (within the anterior 60–70% of the disc space — avoid oversizing anteriorly, risk of retroperitoneal/vascular injury), width 10–12 mm, with 6–10° of built-in lordosis. PEEK cages (radiolucent) are most common; titanium and expandable cages are alternatives.
- Pack the cage with local morselised autograft (the gold standard; allograft, DBM, BMP or synthetic graft if inadequate). Compress graft into the cavity and pack additional graft around the cage edges.
- Advance the cage through the annulotomy under continuous lateral fluoroscopy, angled slightly toward the contralateral side to centre it. Confirm: lateral view — cage at midline, parallel to the endplates, within the anterior 60–70% (not too anterior); AP view — centred mediolaterally, not in the posterolateral foramen. Avoid oversizing the height (subsidence/endplate fracture) or anterior over-placement (vascular injury, less than 0.5% but catastrophic).
- Pack additional graft posterolaterally in the gutter between the transverse processes and over the pedicle screws — this supplements the interbody fusion with a posterolateral fusion (a 360° construct).
- Bend the rods (5.5 mm cobalt-chromium or titanium) to match lumbar lordosis, seat them into the screw heads from caudal to cephalad, and provisionally tighten the set screws.
- Apply compression across the disc space with a rod persuader — this restores disc height without over-distraction, loads the graft under compression (not crushing it), and maintains lordosis.
- Confirm on AP and lateral fluoroscopy that all screws are within the pedicles (no breach, appropriate depth), the cage is centred and parallel to the endplates, and the rods are secure with a lordotic contour.
- Irrigate with antibiotic solution (for example bacitracin 50,000 units in 1 L saline), place a deep drain if desired, and close the fascia with number 1 absorbable suture, subcutaneous tissue with 2-0 absorbable, and skin with 3-0 non-absorbable or staples. An LSO brace for 6–12 weeks supports a single-level TLIF during early healing if bone quality is questionable.
The exiting nerve root is the SINGLE MOST VULNERABLE structure in TLIF (1–8% injury risk — the commonest neurological complication). It lies in the superior foramen, deep to the superior articular process, crossing ABOVE the pedicle of the caudal vertebra (the L4 root exits the L4–5 foramen above the L5 pedicle), passing beneath the pars before descending out of the foramen. The four injury patterns, and how to avoid each: - Facetectomy / SAP resection — the root lies immediately deep to the facet; an uncontrolled burr or a Kerrison passed without seeing the root can lacerate it, and an INADEQUATE facetectomy (root not exposed before disc work) forces the surgeon to instrument the disc blind.
- Upper pedicle screw — a screw placed too laterally or too superiorly breaches the foramen and injures the root.
- Lateral retraction — aggressive lateral retraction during disc and cage access stretches or compresses the root against the pedicle.
- Cage insertion — an oversized cage, or one left too far posterolaterally in the foramen, compresses the root. Protection: (1) perform a COMPLETE unilateral facetectomy that unroofs the foramen and POSITIVELY IDENTIFIES both roots before any disc access — do not work blind through a partial facetectomy; (2) take the final bone over the nerve with a Kerrison or osteotome (not an uncontrolled burr), keeping irrigation on; (3) palpate the root with a blunt hook to confirm it is mobile and out of the corridor; (4) use free-running EMG during facetectomy and triggered EMG on the screws (a low threshold, commonly under 8–10 mA, flags a breach — stop and reassess); (5) retract gently and protect the root superolaterally rather than dragging it medially over the pedicle, releasing retraction periodically; and (6) confirm the cage sits anteriorly across the disc on the AP view, never in the posterolateral foramen.
An INADEQUATE facetectomy — the foramen not unroofed and the roots not seen before disc work — is the key cause of exiting-root injury: the surgeon then instruments the disc blind. A complete facetectomy that exposes both roots is both the safest path to the disc and the source of the local autograft.
A triggered-EMG threshold greater than 8–10 mA is reassuring; a threshold less than 8 mA raises concern for a medial or foraminal pedicle breach and warrants screw re-inspection or repositioning. Combine it with free-running EMG during the facetectomy so an offending manoeuvre can be stopped in real time.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Exiting nerve root (1–8% — commonest neurological complication)
- Protection
- Complete facetectomy unroofing the foramen; Kerrison/osteotome for bone over the nerve; identify and protect superolaterally; free-running EMG
- Structure at risk
- Dural sac and traversing root (durotomy 3–9%)
- Protection
- Stay lateral within Kambin's triangle; gentle thecal retraction; preserve the PLL during discectomy; smooth bone edges before dural work
- Structure at risk
- Aorta, IVC, iliac vessels (rare, less than 0.5%, but catastrophic)
- Protection
- Avoid anterior over-instrumentation; keep the cage within the anterior 60–70%; preserve the ALL and anterior cortex; beware the anteriorly breaching screw
- Structure at risk
- Vertebral artery
- Protection
- Not at risk in lumbar TLIF — it is a cervical/upper-thoracic structure; anterior great vessels are the lumbar vascular concern
Choosing between posterior interbody techniques
- TLIF
- Posterior, unilateral facetectomy, transforaminal disc access
- PLIF
- Posterior, bilateral laminectomy, bilateral disc access
- ALIF
- Anterior retroperitoneal, direct anterior disc access
- TLIF
- Unilateral (exiting root only) — safer
- PLIF
- Bilateral (both traversing roots) — higher risk
- ALIF
- None (anterior to the neural structures) — safest
- TLIF
- Lower (durotomy approx 9%, nerve dysfunction approx 2% — Mehta 2010)
- PLIF
- Higher (durotomy approx 17%, nerve dysfunction approx 8%)
- ALIF
- No direct root mobilisation; risks are vascular and (in males) retrograde ejaculation
- TLIF
- High; comparable to PLIF, both beat posterolateral fusion alone (Makanji 2018)
- PLIF
- High; largest graft surface (bilateral cages), comparable to TLIF
- ALIF
- High — large anterior disc space and load-sharing
- TLIF
- Contralateral facet and posterior tension band preserved
- PLIF
- Both facets typically removed
- ALIF
- All posterior structures preserved
- TLIF
- Lower with MIS than open (median 177 vs 461 mL; SSI 1.2% vs 4.6% — Phan 2015)
- PLIF
- Higher (bilateral dissection, more muscle trauma)
- ALIF
- Moderate (no posterior stripping; retroperitoneal approach)
- TLIF
- First-line for single-level posterior fusion (lower nerve risk than PLIF)
- PLIF
- Second-line — when bilateral decompression is mandatory or TLIF access inadequate
- ALIF
- First-line if no posterior pathology (best fusion), accepting vascular risk
Durotomy occurs in roughly 3–9% of TLIF (a trend lower than PLIF — Mehta 2010), most often during ligamentum-flavum removal at the lateral recess, medial thecal-sac retraction, or discectomy. - Recognition. Clear fluid (CSF) pooling in the wound; a Valsalva manoeuvre (anaesthesia raises airway pressure to 30–40 cmH2O) increases flow; post-operatively, a positional headache (worse upright, better supine) with nausea, photophobia or neck stiffness.
- Intraoperative management. Identify the tear's location and size (small less than 5 mm vs large greater than 5 mm; medial, lateral or anterior). Expose it adequately (extend the laminotomy; use microscope or loupes). Primary repair when possible with 6-0 or 7-0 non-absorbable suture (Prolene or nylon) on a tapered needle, in a running or interrupted watertight closure, confirmed by a dry Valsalva test. If primary repair is not possible (large tear, friable tissue, inaccessible — for example an anterior tear during discectomy), apply a dural sealant (fibrin glue or DuraSeal) with a muscle or fat patch, and consider a lumbar drain (10–20 mL/hour for 3–5 days) for large tears.
- Closure modifications. Do NOT place a deep suction drain (negative pressure disrupts the repair) — use either no drain or a closed drain on low/gravity drainage only; perform a watertight fascial closure.
- Post-operative positioning. Keep the patient FLAT (avoid head elevation greater than 30°) for 24–48 hours; avoid Valsalva (stool softeners, antiemetics); manage a lumbar drain if placed. Prognosis: 80–90% of primarily repaired tears heal without complication; large tears or patch repairs carry a 10–20% persistent-leak rate.
- Unrecognised/persistent leak. Conservative first (flat bed rest, IV fluids, caffeine/NSAIDs for headache, stool softeners — 60–80% settle); then an epidural blood patch (60–80% success) or a lumbar drain; revision surgery if all conservative measures fail.
- Prevention. Adequate bone removal and thinning of the ligamentum before using a Kerrison (thick lateral-recess ligamentum is adherent to dura — pulling it tears dura); blunt dissection to develop the plane between ligamentum and dura; smooth sharp bone edges before manipulating the dura; gentle thecal retraction; and careful PLL preservation during discectomy.
Complications. The principal complications cluster around the exiting root, the dura and the endplate. - Exiting nerve-root injury (1–8%, commonest neurological complication). Presents as intraoperative EMG activity or a post-operative deficit in the exiting-root distribution (for example an L4 injury gives anterior-thigh pain and quadriceps weakness). Mechanism: overzealous facetectomy drilling, a too-lateral/superior upper screw, or aggressive lateral retraction. If the EMG fires, STOP drilling, irrigate, switch to a Kerrison/osteotome, inspect the root (intact vs lacerated), and proceed only if it is intact — most deficits are a recoverable neuropraxia; axonotmesis recovers slowly and incompletely; neurotmesis (transection) does not recover and needs exploration/repair. Prevention is a complete facetectomy exposing the root, controlled bone removal, triggered EMG, and gentle retraction.
- Dural tear / durotomy (3–9%). Managed as above.
- Cage malposition (2–5%). Too posterior (canal/root compression), too anterior (vascular/retroperitoneal risk) or too lateral (foraminal/exiting-root compression). Symptomatic neural compression needs urgent revision; asymptomatic malposition is observed. Prevent with continuous biplanar fluoroscopy and confirming position before closure.
- Epidural haematoma with deficit (2–5%). New or progressive deficit 6–24 hours post-op (foot drop, cauda equina) with wound swelling — obtain URGENT MRI/CT myelogram and re-explore and evacuate; delay greater than 24 hours reduces the chance of recovery. Prevent with meticulous haemostasis, a deep drain, and close neuro checks for the first 24 hours.
- Wound infection (2–5%). Superficial (1–2%) within 2–4 weeks — empirical oral antibiotics covering skin flora (a first-generation cephalosporin, or clindamycin if penicillin-allergic) per local guidance. Deep infection (1–3%) — empirical IV broad-spectrum cover including MRSA (for example vancomycin) plus Gram-negative cover, surgical debridement with hardware retention if fixation is stable, NPWT where appropriate, and a prolonged course guided by infectious diseases. Prevent with pre-operative cefazolin (2 g IV within 1 hour; re-dose every 4 hours if the case exceeds 4 hours), sterile technique, glycaemic control (perioperative glucose less than 180 mg/dL) and minimised operative time.
- DVT/PE (8–12%). Posterior lumbar surgery carries a higher VTE risk than anterior (prolonged immobility, prone positioning, epidural-venous manipulation). Mechanical prophylaxis for all, with chemical prophylaxis (for example LMWH) added per institutional protocol once the bleeding/epidural-haematoma risk is acceptable, and early mobilisation. Timing of chemical prophylaxis after spinal surgery is individualised, and named-society guidance differs.
- Pseudarthrosis (8–15%). Persistent back pain beyond 6 months with no bridging bone on CT at 12 months. Risk factors: smoking (a strong modifiable inhibitor), diabetes, chronic NSAID use, inadequate graft volume, excessive motion. Revision options: revision TLIF with a larger cage and BMP, anterior supplementation (ALIF), or extension of the fusion. Prevent with smoking cessation (delay elective surgery until smoke-free more than 4 weeks), avoiding NSAIDs for more than 3 months post-op, complete graft packing, and bracing.
- Cage subsidence (8–15%). Recurrent back/radicular pain 2–6 months post-op with loss of disc height (cage migration greater than 2 mm into the endplate). Osteoporosis is the strongest risk factor; others are over-aggressive endplate preparation and an oversized cage/over-distraction. Most subsidence is asymptomatic and observed; symptomatic/progressive cases may need revision, preferably anterior supplementation (ALIF) for a larger endplate contact area. Prevent by optimising bone quality pre-operatively, preserving the subchondral endplate, and using the largest cage footprint without over-distraction.
- Adjacent segment disease. New back/radicular pain 2–5 years after fusion as load transfers to adjacent segments. Preserve the contralateral facet and posterior tension band and restore sagittal lordosis at the index fusion; manage conservatively first, reserving revision (extension of fusion) for structural adjacent-level pathology that fails conservative care. Post-operative protocol (general guidance). - Phase 1 (days 0–2): multimodal analgesia (NSAIDs used cautiously given fusion concerns); out of bed to chair on day 1 and walking with assistance days 1–2; continue EMG/SSEP monitoring for the first 2–4 hours; remove the drain when output is less than 50 mL per 8-hour shift; remove the urinary catheter on day 1. Discharge is typically day 3–5 (open) or day 2–3 (MIS).
- Phase 2 (weeks 0–6): LSO brace during upright activities for 6–12 weeks if a single-level TLIF; no bending, lifting greater than 10 lb, or twisting; unlimited walking; driving at 4–6 weeks off opioids; return to sedentary work at 6–8 weeks; AP and lateral X-rays at 2, 6 and 12 weeks.
- Phase 3 (months 3–6): wean the brace if fusion is progressing; CT at 6 months if fusion is questionable on X-ray (CT is the gold standard); core-strengthening physiotherapy once the fusion is solid; return to manual labour at 6–9 months and high-impact activity at 9–12 months after confirmed solid fusion.
- Phase 4 (12+ months): annual X-rays to monitor for adjacent-segment disease; track ODI and VAS; address hardware failure (rare, less than 2% if fusion is solid) and pseudarthrosis. Extensile options. Extend to a second level through the same midline incision for two-level disease. The MIS-TLIF variant (tubular or expandable muscle-sparing retractor via a paramedian incision) reduces blood loss, SSI and length of stay with equivalent fusion, at the cost of greater intraoperative radiation and a learning curve (Phan 2015). For high-grade spondylolisthesis or a failed/osteoporotic TLIF, supplement anteriorly with ALIF for a larger endplate contact area and better anterior load-sharing. Closure: watertight fascia (number 1 absorbable), subcutaneous 2-0 absorbable, skin 3-0 non-absorbable or staples; LSO brace for 6–12 weeks for a single-level TLIF if bone quality is questionable.
Procedures Through This Approach
- Single- and two-level lumbar fusion for degenerative or isthmic spondylolisthesis (Grade I–II) — the principal use of TLIF.
- Fusion for degenerative disc disease with instability and for recurrent disc herniation with an unstable segment.
- Revision for pseudarthrosis after posterolateral fusion, and for adjacent segment disease or post-laminectomy instability.
- The MIS-TLIF variant for the same indications where a muscle-sparing approach is preferred.
Viva & Exam Focus
KAMBINKAMBIN — Kambin's triangle anatomy for safe TLIF
FACETFACET — safe facetectomy to protect the exiting nerve
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“During a right-sided L4–5 TLIF for degenerative spondylolisthesis you are resecting the right L5 superior articular process with a high-speed burr when the EMG suddenly fires with high-frequency spontaneous activity. How do you manage this?”
“A 65-year-old woman with osteoporosis (T-score minus 2.6) had an L4–5 TLIF for degenerative spondylolisthesis 4 months ago. She initially improved but now has recurrent back pain; radiographs show about 4 mm of cage subsidence into the L5 superior endplate. How do you manage this?”
“During an L5–S1 TLIF, while removing the ligamentum flavum with a Kerrison rongeur, you notice clear fluid pooling in the wound; anaesthesia performs a Valsalva and the flow increases. How do you manage this dural tear?”
Exam-day power phrase
- TLIF is a posterior lumbar fusion that accesses the disc through a unilateral facetectomy and the transforaminal corridor (Kambin's triangle), inserting a single cage from one side while preserving the contralateral facet and posterior tension band. Because only the exiting root is mobilised — rather than retracting the thecal sac and both traversing roots as in PLIF — comparative series show a trend to fewer durotomies (approx 9% vs 17%) and less nerve-root dysfunction (approx 2% vs 8%) with equivalent fusion (Mehta 2010). Interbody support increases the odds of solid fusion over posterolateral fusion alone (Makanji 2018). The most vulnerable structure is the exiting root in the superior foramen; protection is a COMPLETE facetectomy exposing both roots, controlled bone removal over the nerve, and neuromonitoring. MIS-TLIF reduces blood loss and SSI with equivalent fusion (Phan 2015).
Critical anatomy — memorise cold
- Kambin's triangle: superior/oblique (hypotenuse) = exiting root (L4 at L4–5); medial (vertical) = traversing root and dural sac (L5 at L4–5); base (inferior) = superior endplate and pedicle margin of the caudal vertebra
- Nerve-free trapezoidal safe zone just superior to the pedicle; cadaveric mean working-triangle area approx 1.8 cm², largest at L5–S1 (Hardenbrook 2016)
- Exiting root: superior foramen, deep to the SAP, crossing ABOVE the caudal pedicle (L4 exits above the L5 pedicle)
- Traversing root: descends medial to the exiting root and exits at the next level down (L5 traverses L4–5, exits L5–S1)
- Facet joint: SAP of the caudal vertebra plus IAP of the cephalad vertebra; lumbar facets are relatively sagittally oriented
- Neural foramen: anterior = posterior body/disc; posterior = pars/facet; superior = cephalad pedicle; inferior = caudal pedicle
- Vertebral artery is NOT a lumbar structure and is not at risk in TLIF — the anterior great vessels are
Evidence to cite
- Mehta 2010 (Neurol Res, PMID 20546682): TLIF (n=43) vs PLIF (n=76) — PLIF trended to more nerve-root dysfunction (7.8% vs 2%) and durotomy (17% vs 9%); all nerve injuries transient; pseudarthrosis comparable (PLIF 2.6% vs TLIF 4.6%)
- Makanji 2018 (Eur Spine J, PMID 29546538): systematic review (160 studies, 8,599 patients) — interbody techniques beat posterolateral fusion (PLIF OR 3.20, TLIF OR 2.46); MIS higher clinical success (OR 2.44) despite equivalent fusion
- Hardenbrook 2016 (Neurosurg Focus, PMID 26828881): cadaveric Kambin's-triangle anatomy — working-triangle area mean 1.83 cm² (largest L5–S1, 2.19 cm²); supra-pedicular safe zone is nerve-free
- Kambin and Sampson 1986 (Clin Orthop, PMID 3720102): original posterolateral transforaminal access — foundation of the Kambin's-triangle concept
- Phan 2015 (Eur Spine J, PMID 25813010): MIS vs open TLIF meta-analysis — lower blood loss (median 177 vs 461 mL) and SSI (1.2% vs 4.6%), modestly better early VAS/ODI, no operative-time penalty
Global practice and guidelines
- Indications: low-grade spondylolisthesis, DDD with instability, recurrent disc herniation with instability, pseudarthrosis after posterolateral fusion
- Choice of interbody approach turns on the decompression needed and the neurological risk profile, not on fusion rate (TLIF and PLIF are comparable)
- Reserve interbody fusion for cases decompression and posterolateral fusion alone cannot address (Mehta 2010)
- MIS-TLIF reduces blood loss, SSI and stay with equivalent fusion, at the cost of radiation and a learning curve (Phan 2015)
- Neuromonitoring (EMG/SSEPs/MEPs) is a common adjunct, not a substitute for technique; routine use varies between units
- VTE prophylaxis: mechanical for all; timing of chemical prophylaxis after spinal surgery is individualised given epidural-haematoma risk
- Assess and optimise osteoporosis before elective fusion (DEXA, anti-resorptive/anabolic therapy) to reduce subsidence
Viva traps — don't get caught
- Trap: 'Why not PLIF for better bilateral decompression?' — PLIF needs bilateral thecal/traversing-root retraction with a trend to more durotomies and nerve dysfunction and equivalent fusion (Mehta 2010); reserve it for mandatory bilateral decompression
- Trap: 'Where is the exiting root?' — superior foramen, deep to the SAP, crossing above the caudal pedicle (L4 above L5); a complete facetectomy exposing it before disc access is protective
- Trap: 'What is the subsidence risk and how do you prevent it?' — roughly 8–15%, higher in osteoporosis; prevent by optimising bone quality, preserving the subchondral endplate, largest cage footprint, no over-distraction
- Trap: 'Is the vertebral artery at risk with lumbar pedicle screws?' — no; it is cervical/upper-thoracic; the lumbar vascular risk is the anterior great vessels from an anteriorly breaching screw or instrument
References
TLIF vs PLIF — comparative surgical morbidity
- Single-institution retrospective comparison of 119 consecutive interbody fusions for degenerative disc disease or spondylolisthesis (PLIF n=76, TLIF n=43) with matched baseline characteristics. PLIF was associated with a higher incidence of postoperative iatrogenic nerve-root dysfunction (6/76, 7.8% vs 1/43, 2%) and durotomy (13/76, 17% vs 4/43, 9%); these differences favoured TLIF but did NOT reach statistical significance in this sample. All nerve-root injuries were transient and resolved by 3 months. Estimated blood loss, length of stay and other perioperative indices were similar. At 12 months, pseudarthrosis rates were comparable (PLIF 2/76, 2.6% vs TLIF 2/43, 4.6%), as were improvements in radicular pain (88% vs 79%) and back pain (74% vs 80%).
Kambin's triangle — cadaveric anatomy of the transforaminal corridor
- Cadaveric analysis of 8 human spines (L1–sacrum) defining the dimensions and trajectory for transforaminal interbody access. Two areas were measured: the working triangle (between the exiting and traversing nerve roots, above the superior margin of the inferior pedicle) and the safe zone (the trapezoid bounded by the superior and inferior pedicle widths between the two roots). Mean working-triangle surface area was 1.83 cm² (largest at L5–S1, 2.19 cm²); mean safe-zone area was 1.19 cm² (largest at L5–S1, 1.26 cm²). Superior to the MEDIAL pedicle border, no neural structures lay within 1.19 cm at any level; on the LATERAL pedicle border the exiting root was closest superiorly (as near as 0.3 cm). The safe zone just superior to the pedicle was free of nerve structures.
Perioperative complications of TLIF — consecutive series
- Consecutive series of 204 TLIF procedures (with rhBMP-2) reviewing complications within a 3-month perioperative window. Complications occurred in 47/204 patients (21.6%): major in 13 (6.4%) and minor in 34 (16.7%). NEW or more severe postoperative neurological complaints occurred in 13 patients (6.4%), of whom 6 required further surgery; identifiable causes included a malpositioned pedicle screw and an epidural haematoma. In 4 patients (2.0%) a foraminal seroma/haematoma caused neural compression requiring revision, and 1 had vertebral osteolysis causing transient radiculopathy. Persistent radiculopathy without a clear imaging cause was seen in 6 patients. Wound-related problems occurred in 6 patients (2.9%): infection (3), haematoma/seroma (1), drainage/dehiscence (2).
Fusion rate by technique — interbody vs posterolateral fusion
- Systematic review of 160 studies (8,599 patients) of adult lumbar fusion for degenerative disorders (2000–2015), analysing fusion, complications and clinical success by technique. Both interbody techniques achieved significantly higher fusion rates than instrumented posterolateral fusion (PLF): PLIF OR 3.20 and TLIF OR 2.46 for fusion versus PLF. There was a trend over time toward more interbody and MIS fusions. Clinical success was statistically higher with MIS versus non-MIS fusion (OR 2.44), despite equivalent fusion and complication rates between MIS and open approaches. The authors emphasise substantial study heterogeneity and call for higher-quality comparative trials.
Minimally invasive (MIS) TLIF vs open TLIF — meta-analysis
- Systematic review and meta-analysis comparing MIS-TLIF and open TLIF for degenerative lumbar disease. There was no significant difference in operative time. Median intraoperative blood loss was significantly lower with MIS-TLIF (177 vs 461 mL; weighted mean difference minus 256 mL, p less than 0.00001). Surgical-site infection was significantly lower in the MIS cohort (1.2% vs 4.6%; relative risk 0.27, p=0.0001). Postoperative VAS back pain (WMD minus 0.41, p less than 0.00001) and ODI (WMD minus 2.21, p=0.04) were modestly better with MIS-TLIF. The authors note higher radiation exposure to the surgical team with MIS and call for prospective randomised confirmation.