Classification | Grading | Fusion Decisions
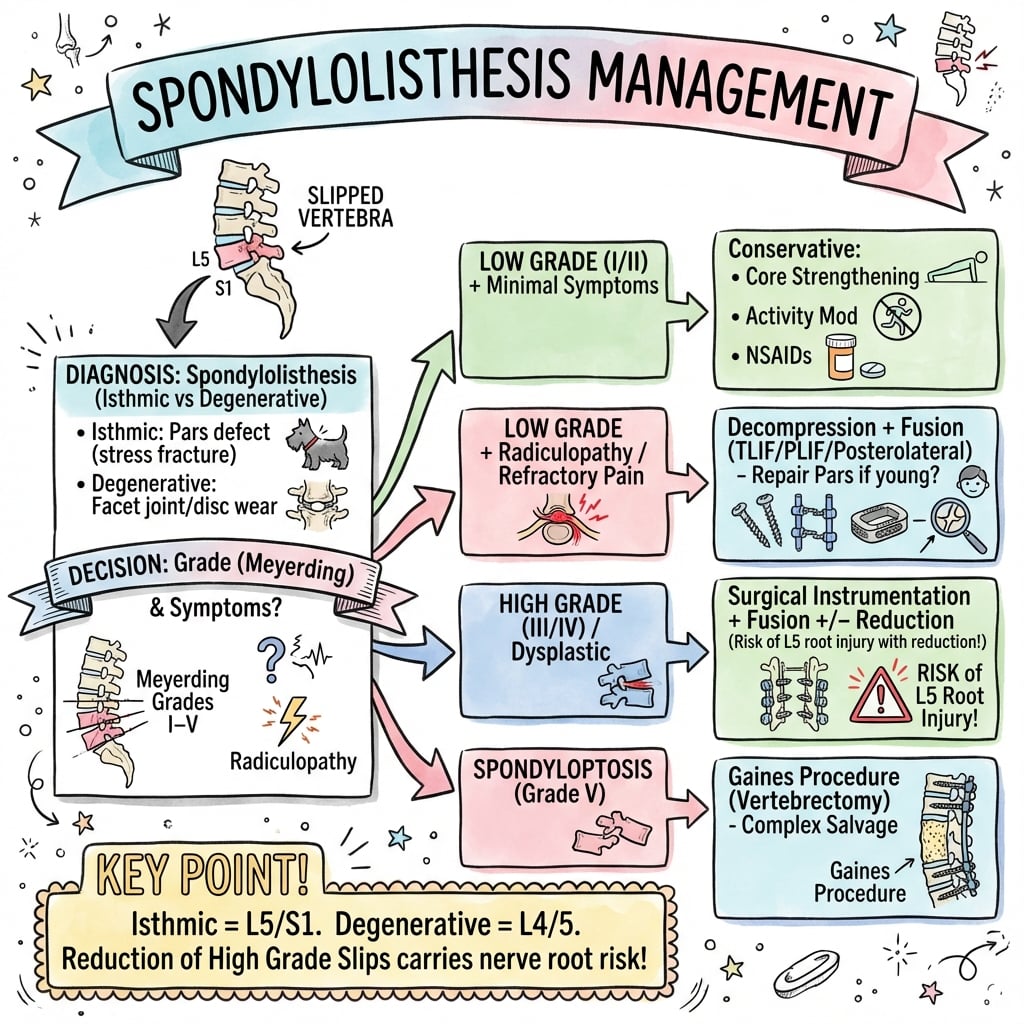
- Isthmic = pars defect, young, L5-S1
- Degenerative = facet arthropathy, older, L4-L5
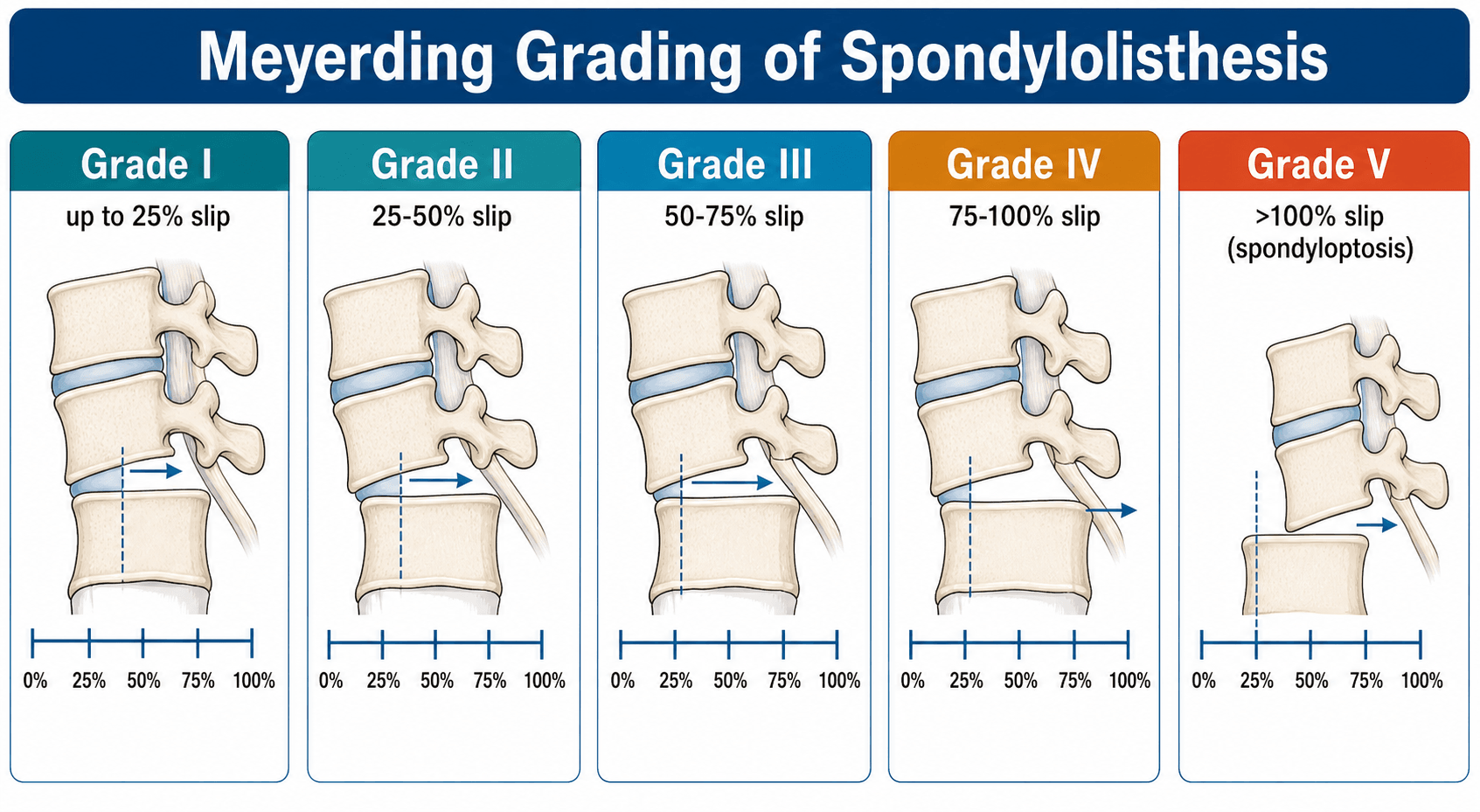
- Meyerding grades I-V based on slip percentage
- High-grade (greater than 50%) usually needs reduction consideration
- Fusion indicated for symptomatic with instability or progression
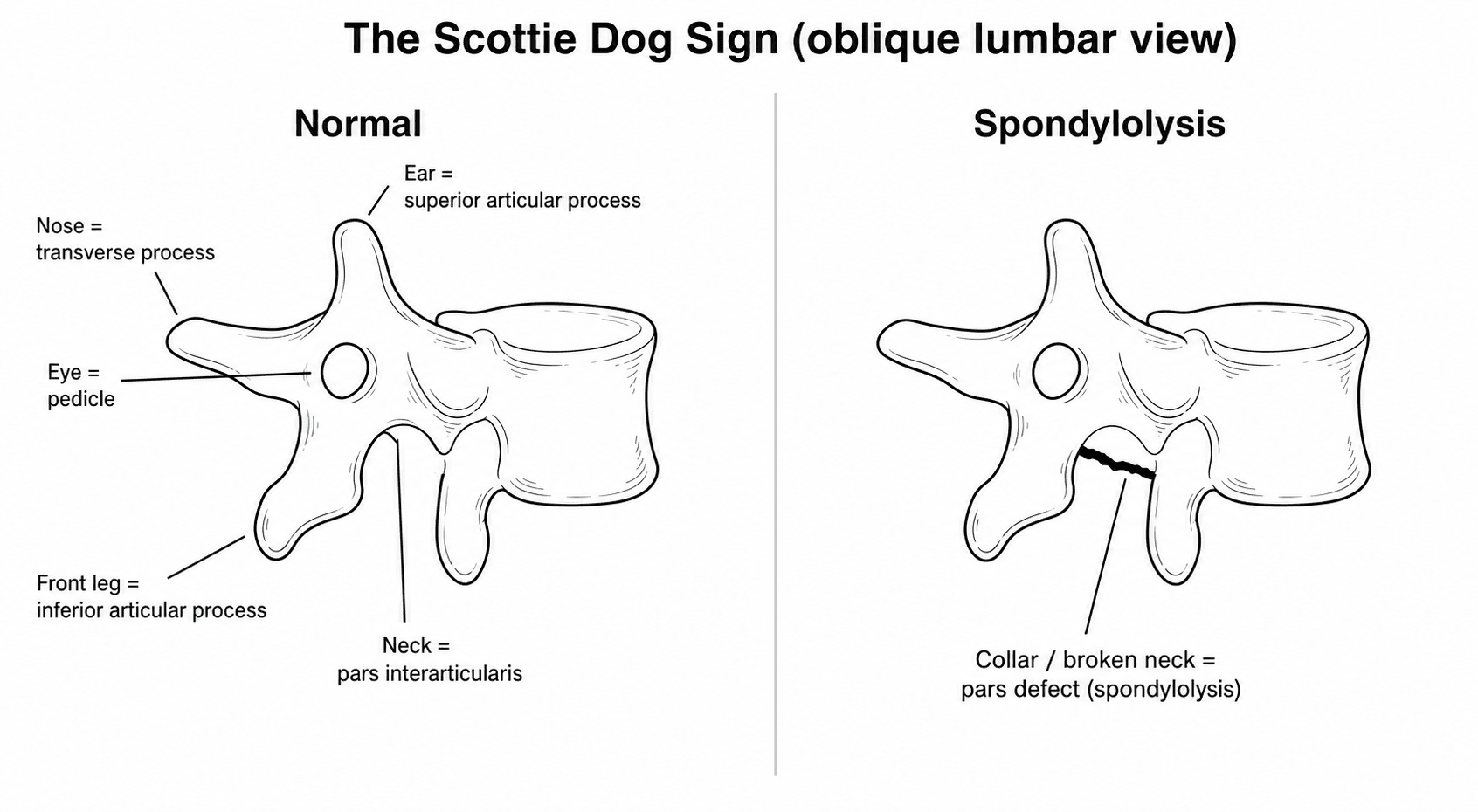
- “Scotty dog sign on oblique X-ray = pars defect
- “Degenerative rarely exceeds Grade II
- “L5 radiculopathy common in isthmic L5-S1
- “Slip angle more important than grade for high-grade
Know the types. Dysplastic (I), Isthmic (II - most common), Degenerative (III), Traumatic (IV), Pathologic (V).
Based on slip percentage. Grade I (less than 25%), II (25-50%), III (50-75%), IV (75-100%), V (spondyloptosis, greater than 100%).
Greater 50% controversial. Consider reduction to improve sagittal balance. Risk of L5 root stretch. In-situ fusion vs reduction.
Isthmic: often ALIF or circumferential. Degenerative: TLIF or posterolateral. Match technique to pathology.
- Isthmic (Type II)
- Young (teens to 30s)
- Degenerative (Type III)
- Older (greater 50)
- Isthmic (Type II)
- L5-S1 (90%)
- Degenerative (Type III)
- L4-L5 (most common)
- Isthmic (Type II)
- Defect (lysis)
- Degenerative (Type III)
- Intact
- Isthmic (Type II)
- Pars fracture
- Degenerative (Type III)
- Facet arthropathy
- Isthmic (Type II)
- Can progress to high-grade
- Degenerative (Type III)
- Rarely exceeds Grade II
25-50-75-100Meyerding Grading
Hook:Divide the vertebra into quarters to grade the slip!
Overview and Epidemiology
Isthmic and degenerative are most common. Isthmic = young, pars defect, L5-S1. Degenerative = older, intact pars, L4-L5. Know the differences for exams!
- Extension sports (gymnastics, cricket fast bowling)
- Adolescent growth spurt
- Genetic predisposition
- Male more than female
- Repetitive hyperextension
- Age greater than 50
- Female more than male (3:1)
- Facet orientation (sagittal)
- Disc degeneration
- Hormonal factors (postmenopausal)
Pathophysiology and Mechanisms
Pars Defect (Spondylolysis)
Isthmus between superior and inferior articular processes.
On oblique X-ray, pars defect appears as "collar" on the Scotty dog (neck = pars).
Fatigue fracture from repetitive hyperextension and rotation.
Allow vertebra to slip forward (listhesis).
Unilateral pars defect = spondylolysis without listhesis.
On oblique lumbar X-ray: The Scotty dog represents the posterior elements. Eye = pedicle, nose = transverse process, ear = superior facet, front leg = inferior facet, neck = pars. A "collar" on the neck = pars defect.
Classification Systems
Wiltse-Newman Classification
- Name
- Dysplastic
- Mechanism
- Congenital facet abnormality
- Level
- L5-S1
- Name
- Isthmic
- Mechanism
- Pars defect (lytic, elongated, acute)
- Level
- L5-S1
- Name
- Degenerative
- Mechanism
- Facet arthropathy, intact pars
- Level
- L4-L5
- Name
- Traumatic
- Mechanism
- Acute fracture other than pars
- Level
- Any
- Name
- Pathologic
- Mechanism
- Tumor, infection, bone disease
- Level
- Any
Type II subtypes: IIa (lytic/fatigue fracture), IIb (elongated intact pars), IIc (acute pars fracture).
DITPPWiltse Classification
Hook:DITPP: the ways vertebrae slip!
Spinopelvic Balance and the SDSG Classification
The topic refers repeatedly to pelvic incidence, slip angle and sagittal balance; the modern framework that ties these together is the Spinal Deformity Study Group (SDSG) classification, which has largely superseded Marchetti-Bartolozzi for surgical planning. It works in two steps: first the slip grade (low-grade under 50% versus high-grade 50% or more), then the spinopelvic alignment.
- Slip grade
- Low-grade
- Spinopelvic alignment
- Low pelvic incidence (nutcracker type)
- Slip grade
- Low-grade
- Spinopelvic alignment
- Normal pelvic incidence
- Slip grade
- Low-grade
- Spinopelvic alignment
- High pelvic incidence (shear type)
- Slip grade
- High-grade
- Spinopelvic alignment
- Balanced pelvis (high sacral slope, low pelvic tilt)
- Slip grade
- High-grade
- Spinopelvic alignment
- Unbalanced (retroverted) pelvis, balanced spine
- Slip grade
- High-grade
- Spinopelvic alignment
- Unbalanced pelvis and unbalanced (forward) spine
The key high-grade distinction is the balanced versus unbalanced (retroverted) pelvis: a balanced pelvis has a high sacral slope and low pelvic tilt, while an unbalanced pelvis retroverts (low sacral slope, high pelvic tilt, a "vertical sacrum") to compensate for the slip. An unbalanced or retroverted pelvis (types 5 to 6) is the setting in which reduction to restore spinopelvic balance is most strongly considered, whereas a balanced high-grade slip may be managed with in-situ fusion.
In high-grade spondylolisthesis the SDSG asks whether the pelvis is balanced (high sacral slope, low pelvic tilt) or unbalanced and retroverted (low sacral slope, high pelvic tilt). The unbalanced, retroverted pelvis is the one most likely to benefit from reduction to restore sagittal balance.
Clinical Assessment
- Back pain: Worse with extension
- Leg pain: Radicular pattern
- Claudication: If associated stenosis
- Activity: Sports history (isthmic)
- Age of onset: Young = isthmic, old = degenerative
- Posture: May see hyperlordosis or flexed stance
- Step-off: Palpable in high-grade
- Hamstrings: Tight (especially high-grade)
- Gait: Waddling if severe (pelvic waddle gait)
- Neuro: L5 and S1 root testing
- Exiting Root
- L4
- Traversing Root
- L5
- Clinical
- L5 radiculopathy common (degenerative)
- Exiting Root
- L5
- Traversing Root
- S1
- Clinical
- L5 radiculopathy (foraminal narrowing in isthmic)
High-grade spondylolisthesis findings: Palpable step-off, flattened buttocks (vertical sacrum), tight hamstrings, waddling gait, trunk shortened. May have severe sagittal imbalance.
Differential Diagnosis
Mechanical and radicular back pain in this age range has a broad differential. The key discriminators are the presence of a slip on standing lateral radiograph, dynamic motion on flexion-extension, and the pattern of neural compression.
- Distinguishing Features
- Pars defect without forward translation; extension-related pain
- Key Investigation
- Oblique X-ray, CT, SPECT/MRI for activity
- Distinguishing Features
- Neurogenic claudication, no vertebral translation
- Key Investigation
- Standing lateral X-ray (no slip), MRI
- Distinguishing Features
- Acute dermatomal radiculopathy, positive SLR, no slip
- Key Investigation
- MRI
- Distinguishing Features
- Extension/rotation pain, no instability, no neural deficit
- Key Investigation
- MRI/CT, diagnostic facet block
- Distinguishing Features
- Night pain, weight loss, destructive lesion (Wiltse V)
- Key Investigation
- MRI with contrast, CT, biopsy
- Distinguishing Features
- Acute injury, fracture other than pars (Wiltse IV)
- Key Investigation
- CT, MRI for ligamentous injury
Investigations
Plain Radiographs
- AP, lateral (standing preferred)
- Oblique (Scotty dog for pars)
- Flexion-extension (dynamic instability)
- Meyerding grade (lateral view)
- Slip angle
- Pars defect (oblique)
- Dynamic motion
Standing laterals better demonstrate true slip.
Slip angle (angle between L5 and S1) is more important than grade for high-grade slips. High slip angle indicates worse sagittal imbalance and higher risk of progression.
Measuring the Slip: Grade and Slip Angle
Two measurements from the standing lateral radiograph drive grading and prognosis: the amount of forward slip and the kyphotic angulation across the slip.
- How it is taken
- Divide the S1 superior endplate into quarters and grade by which quarter the posteroinferior corner of L5 overlies
- What it means
- Grade I to IV by quarter; Grade V is spondyloptosis (L5 below the S1 endplate)
- How it is taken
- Anterior displacement of L5 divided by the AP width of the S1 endplate, times 100
- What it means
- A precise continuous slip percentage, useful for tracking progression
- How it is taken
- Angle between the inferior endplate of L5 and the posterior cortex of S1
- What it means
- Measures lumbosacral kyphosis; a higher (more kyphotic) angle means worse deformity and higher progression risk
The Meyerding grade and Taillard percentage measure how far L5 has translated; the slip angle measures how kyphotically it has rotated on the sacrum. Because the slip angle reflects lumbosacral kyphosis and sagittal balance, it predicts progression better than grade in high-grade slips.
Management Algorithm
Non-Operative Management
- Bracing (Boston overlap brace) 6-12 weeks
- Activity modification
- Physical therapy (flexion-based, core)
- May heal if caught early (bone scan or MRI edema positive)
- PT, core strengthening
- Activity modification
- Weight management
- Monitor for progression
Many patients with low-grade slips remain asymptomatic.
Direct pars repair (Buck fusion, Scott wiring, pedicle screw-hook construct) is an option in young patients with single-level isthmic spondylolysis, no significant disc degeneration, and no or minimal slip. Preserves motion.
Surgical Technique
Posterolateral Fusion with Instrumentation
Most low-grade listhesis.
- Prone positioning
- Midline approach, exposure of transverse processes
- Pedicle screw placement
- Decompression if needed (laminectomy, foraminotomy)
- Decortication and bone grafting to transverse processes
Adequate decompression of affected roots while achieving solid fusion.
L5 nerve root at significant risk with reduction of high-grade slips. The root is draped over the sacral dome and tethered. Aggressive reduction can stretch and injure it. Consider partial reduction and neuromonitoring.
PAINSSurgical Indications
Hook:When listhesis causes PAINS, consider surgery!
Complications
- Notes
- 5-15% depending on technique
- Prevention/Management
- Adequate graft, rigid fixation, smoking cessation
- Notes
- With reduction
- Prevention/Management
- Partial reduction, neuromonitoring
- Notes
- Long-term
- Prevention/Management
- Consider minimizing fusion length
- Notes
- Especially in young
- Prevention/Management
- Monitor, early fusion if progressing
- Notes
- 5-10%
- Prevention/Management
- Careful technique, primary repair
Fusion rates affected by: Number of levels, smoking, biology, technique, bone graft quality. Interbody fusion has higher rates than posterolateral alone.
Postoperative Care
Spondylolisthesis Fusion Recovery
Pain control. DVT prophylaxis. Early mobilization. Brace if used. Neurological checks (especially after high-grade reduction).
Activity restrictions (no BLT: bending, lifting, twisting). Wound care. Gradual walking increase. Brace compliance if prescribed.
Radiographs to assess. Begin PT for core strengthening. Gradual activity increase. Wean brace.
Fusion consolidation. Return to activities. Final radiographs for fusion assessment. CT if fusion in doubt.
Solid fusion signs: No motion on flexion-extension, bridging bone, no lucencies around hardware. CT scan gold standard for fusion assessment.
Outcomes and Prognosis
Prognostic Factors
- Low-grade slip
- Predominant leg pain
- Good bone quality
- Non-smoker
- Single level
- High-grade slip
- Predominant back pain
- Osteoporosis
- Smoker
- Multi-level disease
Guidelines, Registries & Global Practice
Global Epidemiology
- Isthmic spondylolysis/spondylolisthesis: affects roughly 4-6% of the general adult population; the classic Fredrickson cohort found pars defects in about 4.4% of children by age 6 and 6% by adulthood, most at L5.
- Marked ethnic variation: prevalence is far higher in some Inuit/Alaska Native populations (reported up to 30-50%) and lower in some Black African populations - evidence for a strong genetic and biomechanical contribution.
- Sport exposure: rates rise sharply with repetitive lumbar hyperextension - cricket fast bowlers, gymnasts, divers, weightlifters and rowers.
- Degenerative spondylolisthesis: predominantly over age 50, female-to-male around 3:1, classically L4-L5, associated with sagittally-oriented facets and disc degeneration.
Side-by-Side Guideline Positions
- Core Position
- Decompression indicated for symptomatic stenosis with listhesis; fusion considered where instability present
- Emphasis
- Evidence-graded; supports surgery over medical/interventional care
- Core Position
- Decompression for stenosis; fusion not routine and reserved for demonstrable instability or deformity
- Emphasis
- Conservative-first; cautious about adding fusion
- Core Position
- Decision driven by instability, deformity and sagittal/spinopelvic parameters rather than slip grade alone
- Emphasis
- Classification- and alignment-led planning
- Core Position
- Individualised; SLIP vs Swedish trial discordance means no universal fusion mandate
- Emphasis
- Shared decision-making, registry-informed
Registry & Practice Variation
- Registry signal: large spine registries (e.g. Swespine, the UK British Spine Registry) consistently show good patient-reported gains after decompression for degenerative listhesis, with wide centre-to-centre variation in fusion rates that is not fully explained by case mix - underscoring practice-pattern (rather than evidence) driven fusion.
- High-resource settings: ready access to MRI, intraoperative neuromonitoring, navigation/robotics and interbody implants; greater use of circumferential reconstruction for high-grade slips.
- Limited-resource settings: reliance on plain radiographs and clinical assessment; in-situ posterolateral fusion (without expensive interbody cages or neuromonitoring) remains a safe, durable default, particularly for high-grade slips where reduction risk is highest.
Across FRCS, FRACS, EBOT, ABOS and DNB exams the same core is tested: Wiltse and Meyerding classifications, isthmic vs degenerative differences, surgical indications (PAINS), the SLIP vs Swedish trial fusion controversy, and the L5 root risk in high-grade reduction.
Controversies and Areas of Uncertainty
The defining modern debate. SLIP (Ghogawala, 2016) favoured adding fusion in grade I degenerative listhesis; the Swedish Spinal Stenosis Study (Forsth, 2016) found no benefit even in the listhesis subgroup. The reconciling view: fuse when there is demonstrable instability (dynamic motion, mobile slip, facet effusion), decompress alone when the segment is stable.
Reduction improves sagittal/spinopelvic alignment but carries a real risk of L5 nerve root injury (highest during the final stage of reduction). No RCT settles this; many surgeons favour partial reduction with neuromonitoring over both full reduction and pure in-situ fusion.
Interbody (TLIF/ALIF) raises radiographic fusion rates but the clinical advantage over posterolateral fusion is small and of debated significance, while adding cost and potential morbidity.
Optimal brace type, duration and timing of return to sport in adolescent athletes remain poorly standardised; the value of bracing over activity restriction alone is contested.
Examiners reward candidates who acknowledge the conflicting trial evidence (SLIP vs Swedish study) and then give a principled, instability-based decision rather than a dogmatic "always fuse" or "never fuse" answer.
MCQ Practice Points
Q: What is the most common type of spondylolisthesis? A: Type II (Isthmic) - pars defect from fatigue fracture. Most common level is L5-S1.
Q: What is the most common level for degenerative spondylolisthesis? A: L4-L5. Degenerative rarely exceeds Grade II. Isthmic is most common at L5-S1.
Q: What defines high-grade spondylolisthesis? A: Grade III or higher (greater than 50% slip). Grade III = 50-75%, Grade IV = 75-100%, Grade V = spondyloptosis.
Q: What does the collar on the Scotty dog sign represent? A: Pars interarticularis defect (spondylolysis). Seen on oblique lumbar X-ray.
Q: What nerve root is most at risk during reduction of high-grade L5-S1 spondylolisthesis? A: L5 nerve root. Draped over sacral dome and tethered; stretched with reduction.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 17-year-old fast bowler presents with back pain worse with extension and bowling. X-rays show bilateral pars defects at L5 with Grade I spondylolisthesis. How do you manage?”
“A 68-year-old woman has failed conservative treatment for neurogenic claudication. MRI shows L4-L5 stenosis and Grade I degenerative spondylolisthesis with 4mm dynamic instability. What is your surgical plan?”
“A 15-year-old girl presents with worsening back pain and hamstring tightness. X-rays show L5-S1 isthmic spondylolisthesis Grade III (55% slip) with high slip angle. What are the management considerations?”
Wiltse Classification (DITPP)
- I Dysplastic: congenital facet
- II Isthmic: pars defect (most common)
- III Degenerative: facet arthropathy
- IV Traumatic: acute fracture
- V Pathologic: tumor/infection
Meyerding Grades
- I: 0-25% (low-grade)
- II: 25-50% (low-grade)
- III: 50-75% (high-grade)
- IV: 75-100% (high-grade)
- V: greater 100% (spondyloptosis)
Isthmic vs Degenerative
- Isthmic: young, L5-S1, pars defect
- Degenerative: old, L4-L5, intact pars
- Degenerative rarely exceeds Grade II
- Isthmic can progress to high-grade
Surgical Indications (PAINS)
- Progressive slip
- Associated neurological deficit
- Intractable pain (failed conservative)
- Nerve compression
- Sagittal imbalance
High-Grade Considerations
- In-situ vs reduction controversy
- L5 root at risk with reduction
- Slip angle more important than grade
- Often needs circumferential fusion
Key Imaging Signs
- Scotty dog collar = pars defect
- Standing laterals best for grading
- Flexion-extension for instability
- MRI for neural compression assessment
Evidence Base and Key Studies
The three NEJM randomised trials below are the most-quoted evidence in any spine viva: SPORT established that surgery beats non-operative care for symptomatic degenerative spondylolisthesis, while SLIP and the Swedish Spinal Stenosis Study reached opposite conclusions on whether to add fusion to decompression - the central modern controversy.
SPORT - Surgical vs Nonsurgical Treatment for Degenerative Spondylolisthesis
- Randomised plus observational cohorts, 607 patients, 13 US centres, degenerative listhesis with stenosis
- Randomised arm had ~40% crossover in each direction, limiting intention-to-treat
- As-treated analysis: surgery superior at 2 years - bodily pain effect 18.1, physical function 18.3, Oswestry -16.7
- Treatment standardised as decompressive laminectomy with or without fusion