Seronegative Spondyloarthropathy | HLA-B27 | Axial Skeleton Involvement
- HLA-B27 positive in 90-95% of patients - but not diagnostic alone
- Sacroiliitis is the hallmark - bilateral symmetric involvement
- Inflammatory back pain: Morning stiffness greater than 30 min, improves with exercise, worse with rest
- Bamboo spine - complete fusion creates high fracture risk from minor trauma
- Spinal fractures - all 3 columns at risk, treat as unstable, high neurological risk
- “Schober test measures lumbar flexion - less than 5cm increase is abnormal
- “Romanus lesion (shiny corner sign) = vertebral body corner erosion
- “Fractures: Assume unstable, image entire spine, CT is gold standard
- “Cervical osteotomy: C7-T1 preferred level for kyphosis correction
ALL spinal fractures in AS are UNSTABLE - fused spine fractures through all 3 columns. Assume unstable even with minor trauma. Image ENTIRE spine (high rate of non-contiguous fractures). CT is the imaging of choice - X-rays often miss fractures.
HLA-B27 is NOT diagnostic - present in 8% of general population. 90-95% of AS patients are positive. A negative HLA-B27 does not exclude AS. Diagnosis is clinical + imaging (sacroiliitis on MRI or X-ray).
Airway management critical - fixed cervical kyphosis limits intubation options. Fibreoptic intubation often required. Position carefully - avoid neck extension. Consider awake positioning before induction.
THA commonly required - hip involvement in 30-50% of patients. Outcomes good but higher heterotopic ossification risk. Consider prophylaxis. Stiff spine increases mechanical demands on hip.
- Ankylosing Spondylitis
- 90-95%
- Reactive Arthritis
- 60-80%
- Psoriatic Arthritis
- 40-50%
- Ankylosing Spondylitis
- Always (defining feature)
- Reactive Arthritis
- Common
- Psoriatic Arthritis
- 40% have spondylitis
- Ankylosing Spondylitis
- Uncommon
- Reactive Arthritis
- Predominant
- Psoriatic Arthritis
- Common - DIP, dactylitis
- Ankylosing Spondylitis
- Bilateral symmetric
- Reactive Arthritis
- Asymmetric
- Psoriatic Arthritis
- Asymmetric
- Ankylosing Spondylitis
- Uveitis, aortitis
- Reactive Arthritis
- Conjunctivitis, urethritis
- Psoriatic Arthritis
- Skin, nail changes
- Ankylosing Spondylitis
- Chronic progressive
- Reactive Arthritis
- Often self-limiting
- Psoriatic Arthritis
- Variable
NIGHTInflammatory Back Pain Features
Hook:NIGHT pain keeps AS patients awake but MOVEMENT makes it better!
APICALExtra-Articular Manifestations
Hook:APICAL manifestations affect areas beyond the spine!
Overview and Epidemiology
Ankylosing spondylitis (AS) is a chronic inflammatory disease primarily affecting the axial skeleton, leading to progressive spinal fusion. It is the prototypical seronegative spondyloarthropathy, characterized by sacroiliitis and enthesitis.
- Prevalence: 0.1-0.5% in Caucasian populations
- Male to female ratio: 2-3:1 (historically higher ratios due to underdiagnosis in women)
- Peak age of onset: 20-30 years (rarely presents after age 45)
- Strong HLA-B27 association: 90-95% of patients positive
- Family history: 10-20 times increased risk in first-degree relatives
- HLA-B27 positivity: Major genetic risk factor
- Family history: Strong familial aggregation
- Male sex: Higher prevalence and more severe disease
- Smoking: Associated with worse outcomes and progression
HLA-B27 is present in approximately 8% of the general Caucasian population but only 5-10% of HLA-B27 positive individuals develop AS. It is a risk factor, not a diagnostic test. Approximately 5-10% of AS patients are HLA-B27 negative.
Pathophysiology
Understanding the pathophysiology of AS is essential for both diagnosis and management. The disease involves aberrant immune responses at entheses leading to inflammation and subsequent new bone formation.
Genetic Basis
- MHC Class I molecule expressed on cell surfaces
- Mechanism of disease association not fully understood
- Theories include: arthritogenic peptide presentation, protein misfolding, cell surface homodimer formation
- Over 100 HLA-B27 subtypes - B27:05 and B27:02 most associated with AS
- ERAP1 (aminopeptidase) - involved in peptide processing
- IL-23R - IL-23/IL-17 axis important in pathogenesis
- Multiple other loci identified by GWAS
Inflammation and New Bone Formation
- Primary site of inflammation - where tendons/ligaments attach to bone
- Entheses at sacroiliac joints and spine particularly affected
- Inflammatory infiltrate with TNF-alpha, IL-17, IL-23
- Initial erosive inflammation at entheses
- Bone marrow edema visible on MRI
- TNF and IL-17 drive inflammation
- Repair response involves new bone formation (syndesmophytes)
- Eventually leads to complete fusion
Anti-TNF therapy effectively controls inflammation but may not prevent radiographic progression (new bone formation). This disconnect between inflammation and ossification is important for patient counseling and is a common exam discussion point.
Pathological Features
- Earliest site of involvement
- Subchondral bone erosions
- Sclerosis and widening initially, then fusion
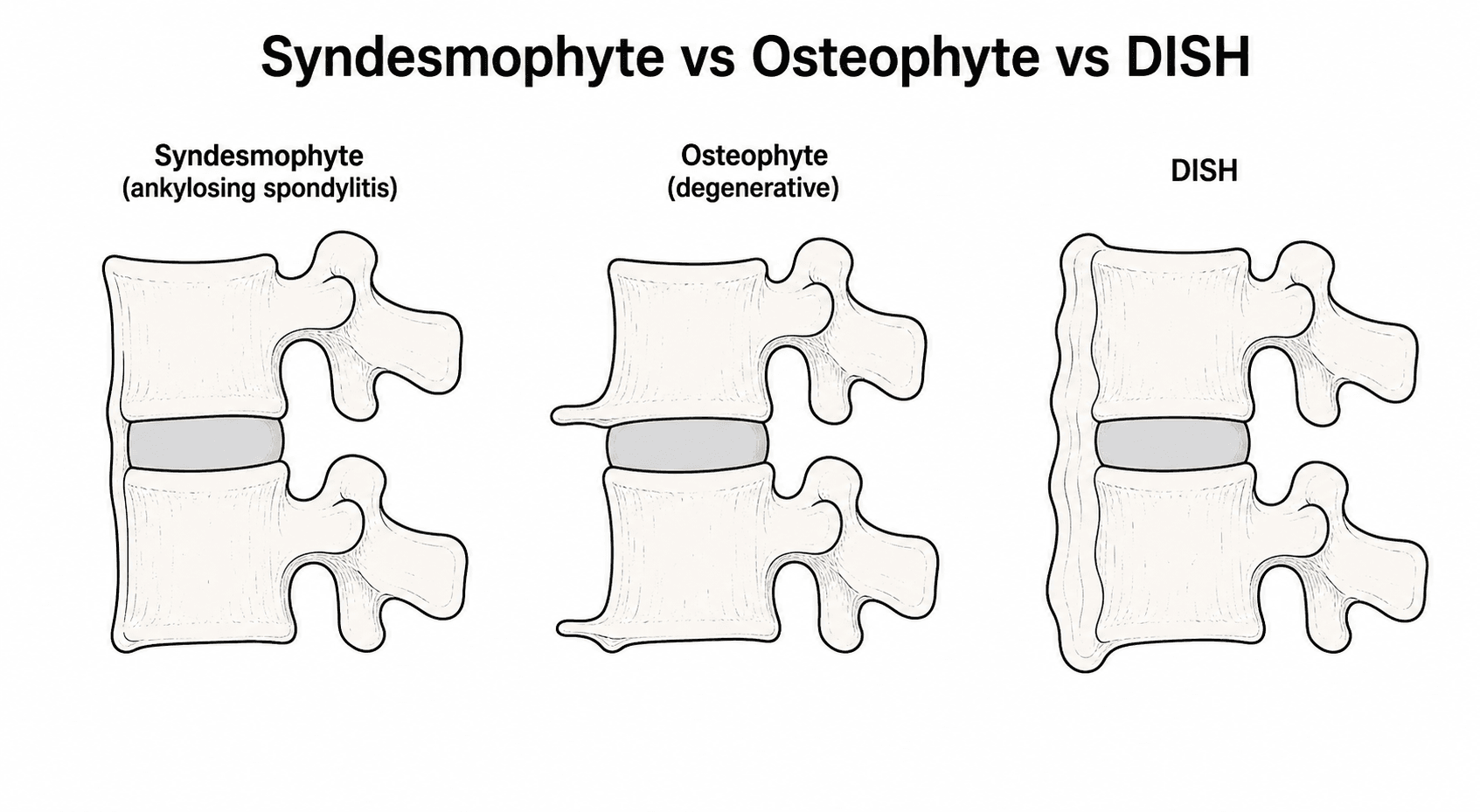
- Romanus lesion: Corner erosion at vertebral body margins
- Syndesmophytes: Vertical bony bridges between vertebrae
- Squaring of vertebral bodies
- Complete fusion: Bamboo spine appearance
Clinical Presentation
Axial Symptoms
- Insidious onset over months
- Age of onset typically less than 40 years
- Morning stiffness greater than 30 minutes
- Improves with exercise, worse with rest
- Night pain - wakes in second half of night
- Alternating buttock pain (sacroiliitis)
- Loss of lumbar lordosis
- Thoracic kyphosis increases
- Reduced chest expansion (less than 2.5cm abnormal)
- Cervical involvement leads to fixed forward gaze
Peripheral Manifestations
- Present in 30-50% of patients
- Often bilateral
- Major cause of disability
- Early onset (less than 10 years disease duration) = worse prognosis
- Shoulder involvement common
- Knee, ankle less frequent
- Asymmetric oligoarthritis pattern
Extra-Articular Manifestations
- Most common extra-articular feature (25-40%)
- Unilateral, recurrent
- Presents with painful red eye, photophobia
- Ophthalmology emergency - can cause vision loss
- Aortitis and aortic root dilatation
- Aortic regurgitation (1-10%)
- Conduction defects
- Apical pulmonary fibrosis (rare)
- Restrictive lung disease from chest wall fusion
Physical Examination
- Loss of lumbar lordosis
- Increased thoracic kyphosis
- Fixed cervical flexion (chin-on-chest deformity in severe cases)
- Question mark posture (global kyphosis)
- Schober test: Mark L5 and 10cm above. On forward flexion, less than 5cm increase is abnormal
- Modified Schober: Mark 5cm below and 10cm above PSIS
- Chest expansion: Less than 2.5cm at nipple line is abnormal
- Occiput-to-wall distance: Should be zero - increased indicates cervical kyphosis
- Tragus-to-wall distance: Alternative cervical mobility measure
Investigations
Laboratory Studies
- ESR and CRP elevated in 50-70%
- Normal inflammatory markers do not exclude AS
- Useful for monitoring disease activity
- Positive in 90-95% of AS patients
- Not diagnostic alone - supports clinical diagnosis
- Useful in early disease when imaging inconclusive
- Negative (seronegative spondyloarthropathy)
- Helps distinguish from RA
Imaging
Plain Radiographs:
Sacroiliac joints:
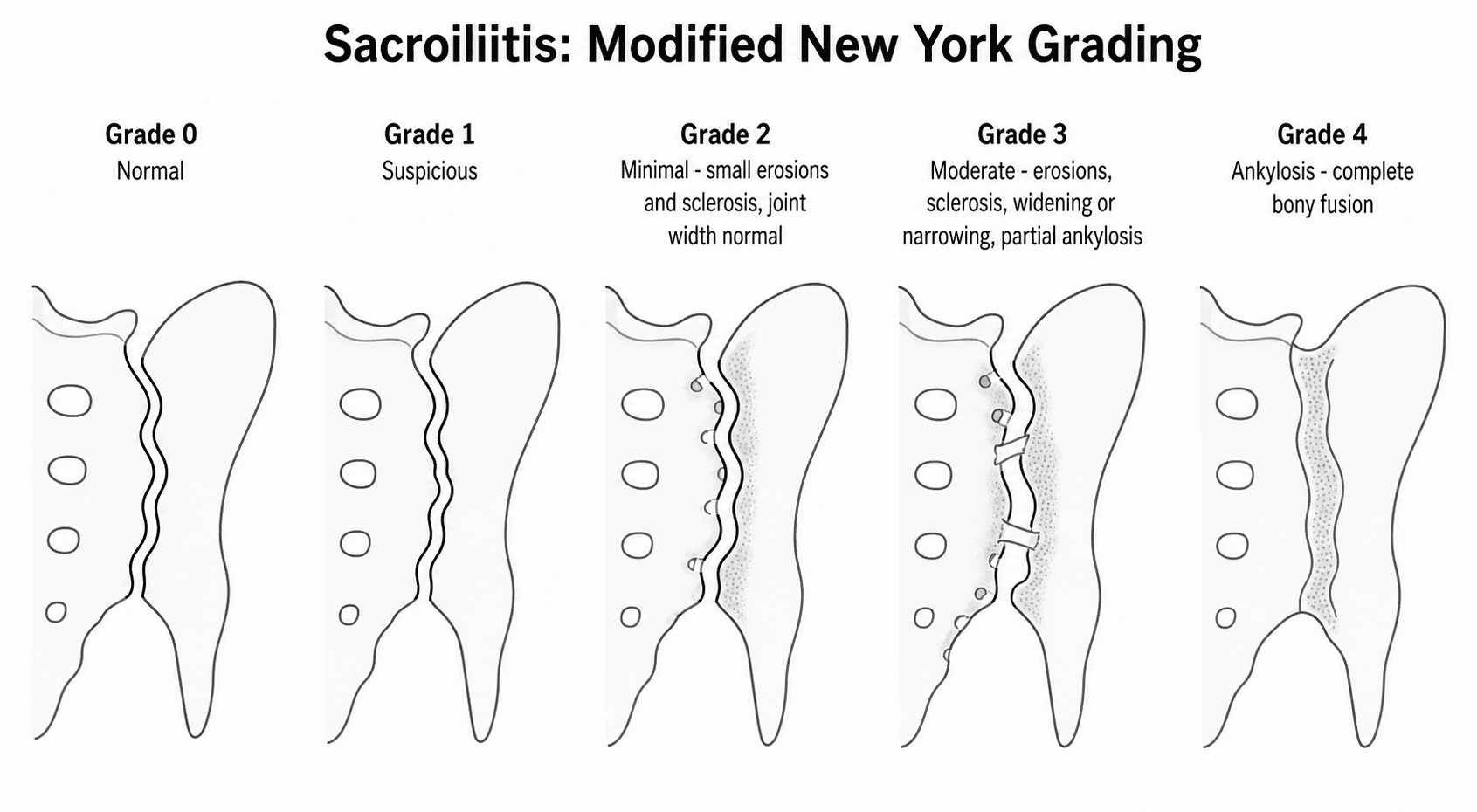
- Bilateral symmetric sacroiliitis
- Grading 0-4 (modified New York criteria)
- Erosions, sclerosis, joint space widening/narrowing, fusion
Spine:
- Squaring of vertebral bodies
- Syndesmophytes (marginal, vertical)
- Bamboo spine (complete fusion)
- Romanus lesion (shiny corner sign)
- Anderson lesion (discovertebral destruction)
- Bone marrow edema at SI joints - active sacroiliitis
- Can detect inflammation before radiographic changes
- STIR/T2 fat-sat sequences best for edema
- Enables diagnosis 5-10 years earlier than X-ray
- Best for fracture detection in AS spine
- Superior to X-ray for visualizing fractures through fused segments
- Image entire spine when fracture suspected
Definite AS requires: Radiographic sacroiliitis (bilateral grade 2-4 OR unilateral grade 3-4) PLUS at least one clinical criterion (inflammatory back pain, limited lumbar motion, reduced chest expansion). These criteria miss early disease - ASAS criteria incorporate MRI.
Differential Diagnosis
The two highest-yield distinctions are AS versus DISH (both ankylose the spine and both fracture as long bones) and inflammatory versus mechanical/degenerative back pain.
- Ankylosing Spondylitis
- Onset under 40
- DISH (Forestier)
- Over 50
- Degenerative / Mechanical
- Any, usually older
- Ankylosing Spondylitis
- Bilateral fusion (defining)
- DISH (Forestier)
- Spared (may have bridging only)
- Degenerative / Mechanical
- Degenerative, not fused
- Ankylosing Spondylitis
- Thin marginal syndesmophytes
- DISH (Forestier)
- Flowing 'candle-wax' osteophytes, right-sided thoracic
- Degenerative / Mechanical
- Marginal osteophytes
- Ankylosing Spondylitis
- Disc preserved early
- DISH (Forestier)
- Disc height preserved
- Degenerative / Mechanical
- Disc/facet degeneration
- Ankylosing Spondylitis
- 90-95% positive
- DISH (Forestier)
- Not associated
- Degenerative / Mechanical
- Not associated
- Ankylosing Spondylitis
- Often raised
- DISH (Forestier)
- Normal
- Degenerative / Mechanical
- Normal
- Ankylosing Spondylitis
- Inflammatory (better with movement)
- DISH (Forestier)
- Stiffness, often mild
- Degenerative / Mechanical
- Mechanical (worse with movement)
Both AS and DISH create a rigid, long-lever spine that fractures through all columns after trivial trauma and is easily missed on plain films. The orthopaedic management principle (CT whole spine, assume unstable, long-segment fixation) is the same - so do not let the AS-versus-DISH label delay imaging or stabilisation.
Management
Medical Management
- Continuous NSAIDs more effective than on-demand
- Indomethacin, naproxen, etoricoxib all effective
- May slow radiographic progression (controversial)
- Continue if effective and tolerated
- Indicated when NSAIDs fail (2 agents over 4 weeks)
- Adalimumab, etanercept, infliximab, golimumab, certolizumab
- Highly effective for symptoms and inflammation
- Most funders require high disease activity (ASDAS/BASDAI) plus failure of 2 NSAIDs
- Secukinumab, ixekizumab
- Alternative to TNF inhibitors
- Particularly useful if TNF failure
- Sulfasalazine: May help peripheral arthritis, limited axial benefit
- Methotrexate: Not effective for axial disease
- Corticosteroids: Local injections useful; avoid long-term systemic
- Maintain posture and mobility
- Regular stretching and strengthening
- Hydrotherapy beneficial
- Lifelong commitment required
This section covers the medical management approach.
Surgical Management
Indications for Spinal Surgery
- Spinal fractures: Most common surgical indication
- Kyphosis correction: For fixed forward gaze, inability to see horizon
- Spinal stenosis: Rare, cauda equina syndrome
- Pseudoarthrosis: Anderson lesion causing instability
Spinal Fracture Management in AS
The ankylosed spine functions as a long bone. Fractures extend through all three columns. Even minor trauma can cause fractures. Neurological injury occurs in 50-70% of cases. Treat all fractures as unstable until proven otherwise.
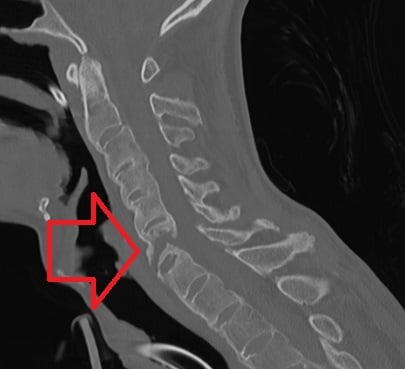
- Assume unstable - all 3 columns involved
- Image entire spine - non-contiguous fractures in 5-10%
- CT is essential - X-rays miss 30% of fractures
- MRI for cord assessment - if neurological deficit
- Immobilize in position of deformity - do not attempt correction
- Early stabilization reduces complications
- Long posterior instrumentation (3+ levels above and below)
- Consider anterior support if significant kyphosis
- Cement augmentation for osteoporotic bone
- Reserved for non-displaced, stable fractures without neurological deficit
- Halo vest or Minerva cast problematic due to rigid spine
- Higher complication rates than surgical treatment
- Mortality 5-15% (higher than general population)
- Neurological injury in up to 70%
- High rate of epidural hematoma
- Delayed union and pseudoarthrosis risk
This section covers fracture management in AS.
Andersson Lesion (Discovertebral Lesion and Spinal Pseudarthrosis)
The imaging section lists the "Anderson lesion (discovertebral destruction)" and the surgical indications list "pseudoarthrosis: Anderson lesion causing instability" — but this important entity is never developed. An Andersson lesion is a localised, lucent, destructive lesion of the discovertebral junction in the ankylosed spine. Clinically it presents as NEW, focal pain in an otherwise stiff or fused back, and it has two recognised forms.
- Inflammatory type
- Active spondylodiscitis-like inflammation of the discovertebral junction
- Mechanical (pseudarthrosis) type
- A stress fracture or established non-union through the rigid fused column with continued micromotion
- Inflammatory type
- Earlier, active inflammatory disease
- Mechanical (pseudarthrosis) type
- Later, in the established bamboo spine
- Inflammatory type
- Erosive discovertebral lesion with marrow oedema on MRI
- Mechanical (pseudarthrosis) type
- Lucent lesion with sclerotic margins and a transdiscal/transvertebral cleft; mobility may be seen on dynamic or flexion-extension films
- Inflammatory type
- Medical control of inflammation
- Mechanical (pseudarthrosis) type
- Surgical stabilisation if there is instability or progressive kyphosis — treat it like a fracture non-union
The critical safety point: an Andersson lesion can closely mimic INFECTIVE spondylodiscitis (and occasionally malignancy) on imaging. If infection cannot be confidently excluded, biopsy before attributing the lesion to AS. The mechanical (pseudarthrosis) type is the surgically relevant one — it is effectively a non-union through the ankylosed spine, so when it causes instability or progressive deformity it is stabilised with long-segment fixation in the same way as an acute AS fracture.
FUSEDSpinal Fracture Principles in AS
Hook:FUSED spines fracture like long bones - through everything!
Complications
Disease Complications
- Spinal fractures: High risk with minor trauma
- Cauda equina syndrome: Late complication from arachnoiditis
- Atlanto-axial subluxation: Rare but serious
- Restrictive lung disease: Costovertebral fusion
- Aortic regurgitation: From aortitis
- Uveitis complications: Vision loss if untreated
- Amyloidosis: Rare, late complication
Surgical Complications
- Neurological injury: High risk with fractures, osteotomy
- Epidural hematoma: Common with AS fractures
- Pseudoarthrosis: Difficult healing, especially at osteotomy sites
- Implant failure: Osteoporotic bone, long lever arms
- Dural tear: Ossified dura may be encountered
- Heterotopic ossification: After hip surgery
Disease Activity and Outcome Measures
Biologic eligibility and treat-to-target monitoring throughout this topic are expressed in indices (BASDAI, ASDAS, mSASSS) that the management and guideline sections quote but never define. Knowing what each measures — activity, function, mobility or structural damage — is high-yield.
- What it measures
- Patient-reported disease ACTIVITY — six items (fatigue, spinal pain, peripheral pain/swelling, enthesitis, plus morning-stiffness severity and duration), scored 0 to 10
- Key point
- A score of at least 4 conventionally defines active disease and is the classic biologic-eligibility threshold; entirely subjective, with no objective inflammation captured
- What it measures
- Disease activity COMBINING patient-reported items with an acute-phase reactant (CRP preferred)
- Key point
- Validated states: inactive under 1.3, low 1.3 to 2.1, high 2.1 to 3.5, very high over 3.5; preferred for treat-to-target because it adds objective CRP
- What it measures
- Patient-reported FUNCTION — ten items on daily activities, scored 0 to 10
- Key point
- Tracks disability and complements the activity scores; does not measure inflammation
- What it measures
- Clinician-measured spinal MOBILITY (tragus-to-wall, cervical rotation, lumbar flexion/Schober, lumbar side-flexion, intermalleolar distance)
- Key point
- Objective measure of mobility loss and accumulating structural restriction
- What it measures
- Radiographic STRUCTURAL damage and progression — cervical and lumbar vertebral corners on the lateral radiograph
- Key point
- The standard endpoint for radiographic progression (for example the MEASURE 1 result of an mSASSS change under 2 in most patients)
BASDAI is purely patient-reported, and a value of at least 4 is the traditional threshold for starting a biologic. ASDAS adds CRP, giving an objective composite with validated activity states, which is why modern treat-to-target guidance increasingly favours it. Do not confuse disease ACTIVITY (BASDAI, ASDAS) with FUNCTION (BASFI), MOBILITY (BASMI) or radiographic STRUCTURAL damage (mSASSS) — an examiner may ask which index you would use to justify escalating therapy versus tracking long-term fusion.
Guidelines, Registries & Global Practice
Global Epidemiology
- Pooled global prevalence of AS is approximately 0.2-0.5%, with the strongest determinant being background HLA-B27 frequency. AS is rare where HLA-B27 is rare (e.g. parts of sub-Saharan Africa, Japan has low prevalence) and more common where HLA-B27 is high (e.g. some Northern European and Indigenous Arctic/First Nations populations).
- Historic male predominance (2-3:1) is now recognised as partly artefact - women are diagnosed later and more often have non-radiographic axial SpA.
- Mean diagnostic delay remains 5-10 years globally, driven by attribution to mechanical back pain.
Side-by-Side Guidelines
- Diagnosis emphasis
- ASAS criteria - MRI sacroiliitis for nr-axSpA
- Biologic trigger
- High activity (ASDAS at least 2.1 or BASDAI at least 4) after 2 NSAIDs
- Distinctive point
- Treat-to-target; bDMARD and tsDMARD (JAKi) both endorsed
- Diagnosis emphasis
- Imaging + clinical, MRI for early disease
- Biologic trigger
- TNFi preferred first-line biologic
- Distinctive point
- Strong recommendation for continuous NSAIDs and PT
- Diagnosis emphasis
- Specialist referral for inflammatory back pain
- Biologic trigger
- TNFi or secukinumab if BASDAI at least 4 and spinal pain after 2 NSAIDs
- Distinctive point
- Defined response criteria for continuation funding
- Diagnosis emphasis
- CT whole spine for any suspected fracture
- Biologic trigger
- n/a
- Distinctive point
- Ankylosed-spine fracture = long-bone-type unstable injury
Registry & Practice Variation
- Arthroplasty registries (NJR, AOANJRR, SHAR, NZJR) consistently show AS patients undergoing THA at a younger age than primary OA, with good implant survival but higher heterotopic ossification.
- High-resource settings: early MRI, rapid access to biologics (TNFi, IL-17i, JAK inhibitors), and treat-to-target monitoring with ASDAS.
- Limited-resource settings: diagnosis often at the bamboo-spine/fixed-deformity stage; NSAIDs and physiotherapy remain the mainstay where biologics are unaffordable, so fracture prevention, fall counselling and arthroplasty/osteotomy services carry greater burden.
- Across all settings, rheumatology-orthopaedic co-management is essential because spinal fractures and hip involvement are the principal orthopaedic endpoints of the disease.
Controversies & Areas of Uncertainty
- Do NSAIDs slow radiographic progression? Earlier data suggested continuous NSAIDs retard syndesmophyte formation, but the ENRADAS trial did not confirm a structural benefit of continuous over on-demand dosing. Continuous use is justified for symptom control, not proven disease modification.
- Do biologics prevent ankylosis? Anti-TNF and IL-17 agents control inflammation but the link to halting new bone formation is unresolved (the "TNF paradox"). Some long-term cohort and IL-17 data suggest reduced progression, but no agent reliably stops fusion.
- TNFi versus IL-17i first-line: Both are effective; IL-17 inhibitors are avoided in inflammatory bowel disease (may worsen it), while TNFi covers concomitant IBD and uveitis better - choice is comorbidity-driven rather than efficacy-driven.
- nr-axSpA as a disease entity: Whether non-radiographic axial SpA is early AS or a partly separate entity (with more women and a lower progression rate) remains debated, affecting how aggressively to treat.
- Spinopelvic targets for THA: With a stiff fused spine, optimal acetabular orientation is contested; "safe zone" cup targets derived from mobile-spine patients may not apply, and functional/spinopelvic planning is increasingly recommended.
- Osteotomy choice: Pedicle subtraction osteotomy gives more correction per level than Smith-Petersen but with higher neurovascular risk; the optimal trade-off and use of multilevel SPO remain individualised.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old man with known ankylosing spondylitis presents after a ground-level fall. He has neck pain and bilateral arm numbness. X-rays are reported as normal.”
“A 28-year-old man presents with 18 months of low back pain. He reports morning stiffness lasting over an hour that improves with exercise. His pain wakes him at night. Examination shows reduced lumbar flexion.”
“A 60-year-old man with longstanding AS has progressive difficulty seeing ahead when walking. He cannot see the horizon and has trouble eating. He has a fixed chin-on-chest deformity.”
“A 45-year-old man with AS has bilateral hip pain limiting walking to 100 metres. X-rays show severe bilateral hip arthritis. He has 30 degrees of fixed thoracolumbar kyphosis.”
Diagnosis
- HLA-B27 positive in 90-95% (not diagnostic alone)
- Bilateral symmetric sacroiliitis on imaging
- MRI detects early sacroiliitis (bone marrow edema)
- Modified New York criteria: sacroiliitis + clinical features
Inflammatory Back Pain
- Age less than 40, insidious onset
- Morning stiffness greater than 30 minutes
- Improves with exercise, worse with rest
- Night pain - wakes in second half of night
Spinal Fractures
- ALL fractures are UNSTABLE (3 columns)
- CT entire spine - X-rays miss 30%
- Immobilize in position of deformity
- Surgical stabilization preferred
Physical Examination
- Schober test: less than 5cm increase abnormal
- Chest expansion: less than 2.5cm abnormal
- Occiput-to-wall: increased with kyphosis
- Question mark posture in advanced disease
Treatment Ladder
- NSAIDs first-line (continuous more effective)
- Physiotherapy essential - lifelong
- TNF inhibitors if NSAID failure
- IL-17 inhibitors alternative biologic
Surgical Considerations
- Airway: fibreoptic intubation often needed
- Positioning: avoid forced positions
- THA: high HO risk - prophylaxis essential
- Osteotomy: C7-T1 for cervical kyphosis
Evidence Base
MEASURE 1 - Secukinumab (IL-17A inhibition) in AS
- ASAS20/40 at week 208 was 79.7%/60.8% (150 mg dose)
- No radiographic progression (mSASSS change under 2) in 79% of patients
- Consistent safety profile - low serious infection and Candida rates
Spinal Fractures in Ankylosing Spinal Disorders (AS/DISH)
- Neurological deficit on admission in 67.2% of AS patients
- Overall complication rate 51.1% in AS; 3-month mortality 17.7%
- Most fractures cervical and from low-energy impact, with frequent delayed diagnosis
Cementless THA for Bony Ankylosis in AS
- Harris Hip Score improved from 49.5 to 82.6; reankylosis rate 0%
- Heterotopic ossification in 12 patients; anterior dislocation in 4.3%
- Survivorship 98.8% at 5 years and 85.8% at 8.5 years (revision endpoint)
ASAS Classification Criteria for Axial SpA
- Active sacroiliitis on MRI strongly associated with axial SpA (OR 45)
- Imaging-arm candidate criteria: sensitivity 97.1%, specificity 94.7%
- Knowledge of MRI changed classification in 21.1% of patients
Defining Active Sacroiliitis on MRI (ASAS/OMERACT)
- Bone marrow oedema/osteitis is the essential lesion for active sacroiliitis
- STIR/T2 fat-saturated sequences best demonstrate inflammation
- Structural lesions alone (sclerosis, erosion, fat) are insufficient for the active definition
ATLAS - Adalimumab (anti-TNF) in AS
- ASAS20 at week 12: 58.2% adalimumab vs 20.6% placebo (p under 0.001)
- ASAS40 and partial remission (22.1% vs 5.6%) significantly higher
- No significant excess of infections versus placebo over 24 weeks