Smith-Robinson Approach | Disc Excision | Interbody Fusion | Plate Fixation
- Smith-Robinson approach is standard anterior cervical exposure
- Longus colli dissection protects vertebral artery and sympathetic chain
- Recurrent laryngeal nerve is at risk on right side (loops around subclavian)
- Dysphagia is commonest complication (transient in most)
- Anterior plate increases fusion rate especially in multilevel
- “Left-sided approach preferred to avoid RLN (loops around aorta - longer protected course)
- “Esophagus lies behind trachea - retract together medially
- “Vertebral artery lies in transverse foramen from C6 upward
- “Superior laryngeal nerve at risk with retraction above C3
Left-sided approach preferred as recurrent laryngeal nerve has longer protected course around aortic arch. On the right side, RLN loops around subclavian artery and is more variable and vulnerable. Some surgeons prefer right for better angle to right-sided pathology.
The longus colli muscles must be dissected to expose disc space and protect vertebral artery laterally. Carotid sheath (carotid, IJV, vagus) retracted laterally. Esophagus and trachea retracted medially.
Dysphagia is the most common complication (50% transient, 2-5% persistent). Minimize with: deflating endotracheal cuff during retraction, limiting retraction pressure, shorter surgical time, and avoiding high retractor blade placement.
Anterior plate increases fusion rates especially in multilevel surgery. Cage height should restore disc height and lordosis but avoid over-distraction. Bone graft options include autograft, allograft, or cage with bone substitute.
- Details
- Radiculopathy, myelopathy, disc herniation
- Clinical Relevance
- Failed conservative treatment or progressive neuro deficit
- Details
- C5-6 (60%), C6-7 (30%)
- Clinical Relevance
- Correlates with degenerative disease pattern
- Details
- Left preferred (RLN protection)
- Clinical Relevance
- Right may be used for right-sided pathology
- Details
- 95% single level, 85% two level
- Clinical Relevance
- Plate increases rate in multilevel
- Details
- 2.5-4% per year
- Clinical Relevance
- Similar to lumbar spine
- Details
- Dysphagia (most common), hoarseness, hematoma
- Clinical Relevance
- Most transient, rare but serious permanent
ACDFACDF - Indications
Hook:ACDF is indicated for Arm pain, Cord compression, Disc herniation, and Failed conservative care
SMITHSMITH - Approach Layers
Hook:SMITH-Robinson approach layers from superficial to deep
LEFTLEFT Side Approach
Hook:LEFT side preferred for recurrent laryngeal nerve protection
Overview and Epidemiology
Anterior cervical discectomy and fusion (ACDF) is one of the most commonly performed spinal procedures. First described by Robinson and Smith in 1955, it revolutionized cervical spine surgery by providing anterior access for neural decompression.
- 1955: Smith and Robinson describe anterior approach with iliac crest graft
- 1958: Cloward describes cylindrical dowel graft technique
- 1970s-80s: Introduction of anterior cervical plating
- 1990s-2000s: Development of cage technology
- 2000s-present: Total disc replacement as alternative
- Cervical radiculopathy: Failed conservative treatment (6-12 weeks)
- Cervical myelopathy: Any progressive or significant myelopathy
- Disc herniation: Symptomatic soft or hard disc
- Cervical instability: Traumatic or degenerative
- Tumor/infection: Anterior column pathology
For cervical radiculopathy without myelopathy, 6-12 weeks of conservative treatment is recommended before surgery. Myelopathy with progressive symptoms or significant cord compromise should proceed to surgery without delay.
Pathophysiology and Mechanisms
- Skin and platysma muscle
- Superficial cervical fascia
- Sternocleidomastoid muscle (lateral landmark)
- Carotid sheath (lateral): Contains carotid artery, internal jugular vein, vagus nerve
- Trachea and esophagus (medial): Retracted together
- Pretracheal fascia: Dissected to reach spine
- Longus colli muscles: Cover anterior vertebral bodies
The vertebral artery enters the transverse foramen at C6 (variable, can be C5-C7). During lateral dissection and foraminotomy, stay medial to the uncovertebral joint to avoid vertebral artery injury.
-
Recurrent laryngeal nerve (RLN):
- Left: Loops around aortic arch (longer protected course)
- Right: Loops around subclavian artery (shorter, more vulnerable)
- Supplies all intrinsic laryngeal muscles except cricothyroid
- Injury causes hoarseness, aspiration
-
Superior laryngeal nerve (SLN):
- External branch at risk with retraction above C3
- Supplies cricothyroid muscle
- Injury affects voice quality/projection
-
Sympathetic chain:
- Lies lateral on longus colli
- Injury causes Horner syndrome
- Anterior longitudinal ligament (superficial)
- Annulus fibrosus
- Nucleus pulposus
- Posterior longitudinal ligament
- Uncovertebral joints (Joints of Luschka) - lateral margin
Classification Systems
When to perform ACDF
- Key Features
- Dermatomal arm pain, motor/sensory deficit
- Timing
- After 6-12 weeks failed conservative
- Key Features
- Long tract signs, gait disturbance, hand dysfunction
- Timing
- Urgent - avoid delay
- Key Features
- Acute or subacute, may be single level
- Timing
- Failed conservative or significant deficit
- Key Features
- Hard disc, osteophytes, foraminal stenosis
- Timing
- Failed conservative treatment
- Key Features
- Flexion-distraction, facet dislocation
- Timing
- Urgent
Myelopathy with progression or significant cord compression should not be delayed for conservative treatment.
Clinical Assessment
History:
- Neck pain (axial)
- Arm pain (radicular - dermatomal distribution)
- Numbness/tingling (dermatomal)
- Weakness (myotomal)
- Hand clumsiness (myelopathy)
- Gait disturbance (myelopathy)
- Bladder/bowel symptoms (severe myelopathy)
- Duration and progression
- Response to conservative treatment
Examination:
- Motor
- Deltoid, biceps
- Sensory
- Lateral arm
- Reflex
- Biceps
- Motor
- Wrist extensors, biceps
- Sensory
- Lateral forearm, thumb
- Reflex
- Brachioradialis
- Motor
- Triceps, wrist flexors
- Sensory
- Middle finger
- Reflex
- Triceps
- Motor
- Finger flexors, intrinsics
- Sensory
- Medial forearm, ring/little finger
- Reflex
- None reliable
- Motor
- Intrinsics
- Sensory
- Medial arm
- Reflex
- None reliable
Myelopathy signs:
- Upper motor neuron signs (hyperreflexia, clonus, Babinski)
- Lhermitte sign (electric shock with neck flexion)
- Hoffmann sign (thumb/index flexion with middle finger flick)
- Gait disturbance (broad-based, spastic)
- Hand dysfunction (grip and release test)
- Inverted radial reflex
The C5-6 disc compresses the C6 nerve root (exiting above the disc). Similarly, C6-7 disc affects C7 root. The nerve root exits above the pedicle of the same numbered vertebra (unlike lumbar spine where root exits below).
Differential diagnosis - what mimics cervical radiculopathy/myelopathy:
- Distinguishing Features
- Dermatomal arm pain, myotomal weakness, reflex loss
- Key Discriminator
- Spurling test positive; MRI root compression matches level
- Distinguishing Features
- Night pain, thumb/index/middle numbness, thenar wasting
- Key Discriminator
- Tinel/Phalen positive; NCS shows median neuropathy at wrist
- Distinguishing Features
- Ring/little finger numbness, intrinsic wasting
- Key Discriminator
- Sensory loss spares forearm (vs C8/T1); NCS localises to elbow
- Distinguishing Features
- Positional arm symptoms, vascular or lower-trunk pattern
- Key Discriminator
- Provocative manoeuvres; vascular studies; often normal MRI
- Distinguishing Features
- Severe shoulder pain then patchy weakness, often post-viral
- Key Discriminator
- Multifocal/non-dermatomal; MRI spine normal
- Distinguishing Features
- Pain with shoulder movement, no distal neurology
- Key Discriminator
- Reproduced by shoulder, not neck, examination
- Distinguishing Features
- Bilateral UMN signs, cranial nerve or cerebellar signs
- Key Discriminator
- Brain MRI; cord signal absent or beyond cervical level
- Distinguishing Features
- Mixed UMN and LMN signs, fasciculations, no sensory loss
- Key Discriminator
- No sensory level; EMG diffuse denervation
The most dangerous trap is operating on imaging that does not match the clinical picture. Painless progressive weakness with fasciculations and no sensory loss suggests motor neurone disease - decompression will not help and the diagnosis may be missed. Always confirm clinico-radiological correlation before committing to ACDF.
Investigations
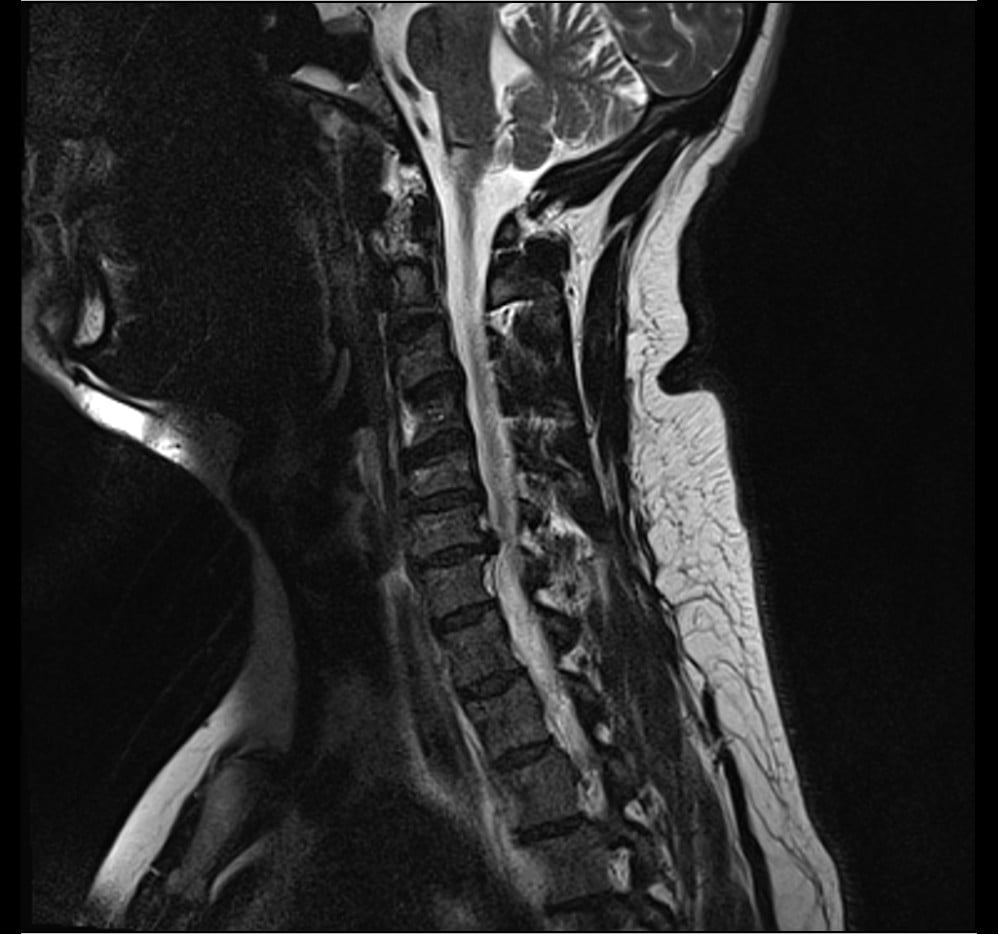
Gold standard imaging
- T1-weighted: Anatomy, bone marrow changes
- T2-weighted: Cord signal (myelomalacia), disc pathology
- Gradient echo (T2*): Metal artifact reduction, better disc visualization
- Disc herniation (soft disc)
- Osteophyte complex (hard disc)
- Cord compression
- Cord signal change (poor prognostic sign)
- Foraminal stenosis
MRI should correlate with clinical findings to confirm surgical level(s).


Management Algorithm
- 1Radiculopathy
Conservative treatment 6-12 weeks unless progressive deficit
50-70% improve with conservative care
- 2Myelopathy
Early surgical referral - avoid delay
Progression may be irreversible
- 3Failed Conservative
Confirm clinical-radiological correlation, plan surgery
ACDF for 1-3 levels, consider alternatives for more
- 4Surgical Options
ACDF vs disc replacement vs posterior approach
Based on pathology and patient factors
For radiculopathy without myelopathy
- NSAIDs
- Oral corticosteroids (short course for acute)
- Neuropathic pain agents (gabapentin, pregabalin)
- Muscle relaxants
- Cervical traction (controversial)
- Strengthening exercises
- Postural training
- Activity modification
- Cervical epidural steroid injection
- Selective nerve root blocks
- Transforaminal vs interlaminar approach
- 50-70% improve with conservative treatment
- Natural history of radiculopathy is generally favorable
Give adequate conservative trial unless progressive deficit or myelopathy.
Surgical Technique
Smith-Robinson anterior cervical approach
Positioning:
- Supine with neck in neutral or slight extension
- Head on gel ring or Mayfield
- Arms tucked at sides
- Fluoroscopy to confirm level
Approach Steps
Transverse skin crease incision (cosmetic) or longitudinal incision for multilevel. Left side preferred. Incise platysma in line with skin.
Identify medial border of sternocleidomastoid. Develop plane between carotid sheath laterally and trachea/esophagus medially. Blunt dissection to pretracheal fascia.
Divide pretracheal fascia. Identify anterior spine covered by longus colli. Confirm level with fluoroscopy using needle in disc.
Subperiosteal elevation of longus colli off anterior vertebral bodies. Elevate to expose uncovertebral joints (lateral limit of dissection). Place self-retaining retractor under longus colli.
The longus colli must be elevated carefully to protect the vertebral artery and sympathetic chain laterally.
Complications
Frequently encountered issues
- Incidence
- 30-50% transient, 2-5% persistent
- Prevention/Management
- Minimize retraction, deflate ETT cuff, shorter surgery
- Incidence
- 2-5% transient, 0.2-1% permanent
- Prevention/Management
- Left-sided approach, gentle retraction, protect nerve
- Incidence
- 1-2%
- Prevention/Management
- Meticulous hemostasis, consider drain
- Incidence
- 5% single level, 15% multilevel
- Prevention/Management
- Use plate, cage with bone graft, no smoking
- Incidence
- 2.5-4% per year
- Prevention/Management
- Minimize levels, consider disc replacement
Dysphagia is the most common complication but usually resolves within weeks.
DANGERDANGER - Complications
Hook:DANGER zones in ACDF - watch for these complications
Postoperative Care
First 24-48 hours
- Airway assessment (watch for hematoma)
- Neurological checks
- Pain management
- Dysphagia screening before oral intake
- Increasing neck swelling
- Stridor or respiratory distress
- New neurological deficit
- If airway compromise developing
- Open wound at bedside to decompress
- May need emergency intubation (can be very difficult)
- Return to OR for evacuation
First 48 hours critical for hematoma detection.
Outcomes and Prognosis
- Success Rate
- 85-95%
- Recovery Timeline
- Arm pain improves within days/weeks
- Factors Affecting Outcome
- Duration of symptoms, motor deficit
- Success Rate
- 70-80% stabilize/improve
- Recovery Timeline
- May take 6-12 months
- Factors Affecting Outcome
- Preop severity, cord signal change
- Success Rate
- 90-95%
- Recovery Timeline
- Rapid improvement typical
- Factors Affecting Outcome
- Soft disc better than hard disc
Prognostic factors:
- Better Prognosis
- Short (less than 6 months)
- Worse Prognosis
- Prolonged (greater than 2 years)
- Better Prognosis
- Soft disc
- Worse Prognosis
- Hard disc, severe spondylosis
- Better Prognosis
- Mild, recent onset
- Worse Prognosis
- Severe, long-standing, cord signal change
- Better Prognosis
- Single level
- Worse Prognosis
- Multiple levels
- Better Prognosis
- Non-smoker, no diabetes
- Worse Prognosis
- Smoker, diabetic, workers comp
ACDF has excellent outcomes for radiculopathy; myelopathy outcomes depend on severity and duration.
Guidelines, Registries & Global Practice
ACDF is one of the most frequently performed spine operations worldwide and is a core procedure across FRCS (Tr&Orth), FRACS, EBOT/FEBOT, ABOS, DNB/MS and SICOT curricula. Evidence and recommendations are drawn from international guidelines and registries to give a global picture rather than any single country's practice.
Global epidemiology
- Cervical radiculopathy has an annual incidence of roughly 80-100 per 100,000, peaking in the fifth and sixth decades; the great majority improve with non-operative care.
- Degenerative cervical myelopathy is the commonest cause of non-traumatic spinal cord dysfunction in adults worldwide, and its prevalence is rising with ageing populations.
- C5-6 and C6-7 are consistently the most commonly operated levels across all regions, mirroring the distribution of degenerative load.
Major guidelines, side by side
- Radiculopathy
- Trial of non-operative care first if no progressive deficit
- Myelopathy
- Operate for moderate-severe DCM; offer surgery or structured non-op for mild DCM
- Arthroplasty vs ACDF
- Both acceptable for 1-2 level disease without instability
- Radiculopathy
- Surgery superior for short-term relief of refractory radiculopathy
- Myelopathy
- Decompression recommended for symptomatic myelopathy
- Arthroplasty vs ACDF
- TDR non-inferior to ACDF for selected 1-2 level disease
- Radiculopathy
- Conservative care first; refer if red flags or persistent deficit
- Myelopathy
- Urgent referral for suspected myelopathy
- Arthroplasty vs ACDF
- Arthroplasty an option in appropriately selected patients
- Radiculopathy
- Emphasis on clinico-radiological correlation before surgery
- Myelopathy
- Early decompression to limit irreversible cord injury
- Arthroplasty vs ACDF
- Motion preservation favoured in young, single-level, no facet arthrosis
Registry and outcome evidence
- FDA IDE randomised trials (Mobi-C, Prestige, ProDisc-C, Bryan) underpin the global acceptance of cervical arthroplasty as non-inferior to ACDF for selected 1-2 level disease, with lower index-level reoperation in long-term follow-up.
- Spine registries and large administrative datasets (for example the Quality Outcomes Database in North America and national spine registries in Europe and Australasia) consistently report high patient-reported improvement and low major-complication rates after ACDF, supporting its status as a workhorse procedure.
High- vs limited-resource practice variation
- In well-resourced settings, PEEK/titanium cages, anterior plating, intra-operative fluoroscopy and (increasingly) arthroplasty are routine.
- In limited-resource settings, structural allograft or autograft (Smith-Robinson tricortical iliac crest) without a plate remains a valid, low-cost technique with good single-level fusion rates; intra-operative imaging and disc replacement may be unavailable.
- Across all settings the principles are identical: confirm clinico-radiological correlation, decompress adequately, restore disc height and alignment, and do not delay surgery for progressive myelopathy.
Controversies and Areas of Uncertainty
These are high-yield discussion points where an examiner probes judgement rather than recall - state both sides and where the evidence currently sits.
Long-term IDE data show TDR is non-inferior at one level and clinically superior at two levels with lower reoperation, yet ACDF remains the default in many systems on grounds of cost, surgeon familiarity and concerns about heterotopic ossification and long-term implant behaviour. The debate is about patient selection, not whether TDR works.
The left-versus-right RLN argument is anatomically logical but not consistently supported by clinical series. Defensible positions exist for both sides; the unwary candidate who states left is "always safer" can be pushed.
For mild degenerative cervical myelopathy (mJOA 15-17), AOSpine permits either surgery or structured non-operative care with close monitoring. The uncertainty is which mild patients will progress - cord signal change, large cord compression and clinical deterioration push toward surgery.
Anterior plating improves lordosis and multilevel stability but contributes to early dysphagia; zero-profile and stand-alone cages reduce early dysphagia with comparable fusion. The trade-off is alignment/stability versus swallowing morbidity.
Routine drainage after ACDF is not evidence-based for preventing airway-threatening haematoma (which is usually arterial and rapid); meticulous haemostasis and vigilant post-op monitoring matter more. Practice varies widely.
For multilevel myelopathy, anterior (ACDF/corpectomy), posterior (laminoplasty, laminectomy and fusion) and combined approaches all have advocates. Sagittal alignment (kyphosis favours anterior), number of levels, OPLL and bone quality drive the decision.
MCQ Practice Points
Q: Which side is preferred for the anterior cervical approach and why?
A: Left side is preferred. The recurrent laryngeal nerve (RLN) on the left loops around the aortic arch, giving it a longer and more protected course, while the right RLN loops around the subclavian artery, making it shorter and more vulnerable to injury during retraction.
Q: A C5-6 disc herniation will compress which nerve root?
A: C6 nerve root. In the cervical spine, the nerve root exits ABOVE the pedicle of the same-numbered vertebra, so the C5-6 disc affects the C6 root. This is opposite to the lumbar spine pattern.
Q: What is the recommended timing for surgical intervention in cervical myelopathy?
A: Early surgery is recommended - do not delay for conservative treatment. Evidence shows better outcomes when surgery is performed within 6 months of symptom onset. Myelopathy with progressive symptoms is urgent.
Q: What is the rate of dysphagia after ACDF?
A: 50% transient dysphagia (usually resolves within weeks), with 2-5% persistent dysphagia. Dysphagia is the most common complication of ACDF.
Q: What is the annual rate of adjacent segment disease after cervical fusion?
A: 2.5-4% per year. This is similar to lumbar spine fusion. Total disc replacement may reduce this rate but evidence is limited.
Q: What is the immediate management of suspected postoperative hematoma with airway compromise?
A: Open the wound at the bedside to evacuate hematoma and relieve pressure on the airway. This should be done before or while attempting intubation, as intubation may be extremely difficult due to swelling.
Exam Cheat Sheet
Key Numbers
- C5-6 most common level (55-65%)
- Fusion rate: 95% single, 85% multilevel
- Dysphagia: 50% transient, 2-5% persistent
- Adjacent segment disease: 2.5-4%/year
Approach Anatomy
- Left side preferred (RLN protection)
- Carotid sheath retracted laterally
- Trachea/esophagus retracted medially
- Longus colli protects vertebral artery
Nerve Root Levels
- C5-6 disc = C6 root compression
- C6-7 disc = C7 root compression
- Root exits ABOVE pedicle of same number
- Different from lumbar spine pattern
Complications
- Dysphagia (most common)
- Hematoma (airway emergency)
- RLN injury (hoarseness)
- Pseudarthrosis (especially multilevel)
Exam Traps
- Not knowing left vs right approach rationale
- Wrong nerve root level correlation
- Delaying surgery for myelopathy
- Not recognizing hematoma emergency
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old man presents with 8 weeks of right arm pain radiating to the thumb with numbness. He has weakness of wrist extension. MRI shows a C5-6 disc herniation compressing the C6 nerve root.”
“A 62-year-old woman presents with difficulty writing and buttoning clothes, unsteady gait, and electric shocks down her spine when she flexes her neck. Examination shows hyperreflexia and Hoffmann sign bilaterally. MRI shows multilevel stenosis C4-C7 with cord compression and T2 signal change in the cord at C5-6.”
“You are called to see a patient 6 hours after ACDF who is developing stridor and has increasing neck swelling. The patient is becoming increasingly distressed.”
“A fit 38-year-old non-smoker has single-level C5-6 soft-disc radiculopathy that has failed three months of conservative care. He asks whether he should have a fusion or a disc replacement. How do you counsel him and decide?”
Evidence Base
Surgery vs Physiotherapy vs Collar for Radiculopathy (Persson RCT)
- Surgery gave faster relief of pain, sensory loss and weakness at 4 months
- All three arms converged by 1-year follow-up
- Conservative care has a generally favourable natural history
- Reserve surgery for failed conservative care or progressive deficit
Cervical Disc Arthroplasty vs ACDF - 7-Year IDE Trial (Mobi-C)
- Single-level TDR non-inferior; two-level TDR superior at 7 years
- Lower index-level and adjacent-level reoperation with TDR
- Motion preserved with TDR
- TDR contraindicated in significant facet arthrosis, kyphosis or instability
Zero-Profile Spacer vs Cage-Plate - Dysphagia (Meta-analysis)
- Anterior plates contribute to early dysphagia
- Zero-profile/low-profile devices lower early dysphagia rates
- No difference in fusion, function or late dysphagia
- Plate still favoured where lordosis correction or maximal multilevel stability is needed
Surgery for Cervical Spondylotic Myelopathy (AOSpine North America)
- Surgery improves function and quality of life at all severity grades
- Benefit seen even in moderate and severe myelopathy
- Complication rate ~19%, comparable to historical series
- Do not delay - myelopathy is progressive and recovery is duration-dependent
Adjacent-Segment Disease After Anterior Cervical Arthrodesis (Hilibrand)
- Adjacent-segment disease ~2.9% per year, ~25% at 10 years
- Highest risk at C5-6 and C6-7
- Single-level fusion carried higher adjacent-level risk than multilevel
- Two-thirds of affected patients ultimately required further surgery
Incidence and Natural History of Dysphagia After Anterior Cervical Surgery (Bazaz)
- Dysphagia is common early (~50% at 1 month) but largely resolves
- Persistent moderate/severe dysphagia uncommon (~5% at 6 months)
- Female sex and multilevel surgery increase risk
- Most dysphagia is self-limiting and managed expectantly
The classic teaching of a left-sided approach to protect the recurrent laryngeal nerve rests on the more constant, longer left RLN course around the aortic arch (the right RLN loops around the subclavian and may run non-recurrently in roughly 1 in 200). However, large series and meta-analyses have not consistently shown a difference in symptomatic RLN palsy between left and right approaches, so surgeon familiarity and the side of pathology are legitimate determinants. Quote the anatomical rationale in the viva, but acknowledge the evidence is not definitive.