Alternative to Fusion | Maintains Segmental Motion | Reduces Adjacent Segment Disease
- Strict patient selection - single/2-level disease, no facet arthrosis, no instability
- Contraindications - OPLL, ankylosing spondylitis, severe osteoporosis, facet arthropathy
- Equivalent outcomes to ACDF for radiculopathy/myelopathy at 5-10 years
- Adjacent segment protection - theoretical benefit, reduced radiographic ASD
- Preserves motion - maintains approximately 8-10° segmental flexion-extension
- “CDA vs ACDF: Non-inferior outcomes, may reduce ASD
- “Best indication: Young patient, single level, soft disc, no facet disease
- “Avoid: OPLL, severe spondylosis, instability, osteoporosis
- “Most are semi-constrained metal-on-polyethylene designs
Contraindications are exam favorites: OPLL (risk of progression), facet arthropathy (will fail), instability (needs fusion), severe osteoporosis (subsidence), active infection, and prior surgery at same level.
Primary theoretical advantage over ACDF. ASD occurs at 2.9% per year with ACDF vs approximately 1% with CDA in some studies. However, whether this translates to clinical benefit remains debated.
Know the major devices: Prestige LP (metal-on-metal), ProDisc-C (metal-on-poly), Mobi-C (approved for 2-level), Bryan (first FDA approved). Each has specific characteristics.
Multiple IDE trials show CDA is non-inferior to ACDF at 5-10 years. May have lower reoperation rates for ASD. No difference in clinical outcomes (NDI, arm/neck pain).
- Favors CDA
- Under 45 years
- Favors ACDF
- Over 60 years
- Reasoning
- Motion preservation benefits young; older patients less benefit from preserved motion
- Favors CDA
- Single level
- Favors ACDF
- 3+ levels
- Reasoning
- CDA approved for 1-2 levels; multilevel fusion may be more reliable
- Favors CDA
- Normal facets
- Favors ACDF
- Facet arthropathy
- Reasoning
- CDA requires healthy facets for motion; arthropathy causes continued pain
- Favors CDA
- Stable segment
- Favors ACDF
- Any instability
- Reasoning
- Instability is absolute contraindication to CDA
- Favors CDA
- Normal BMD
- Favors ACDF
- Osteoporosis
- Reasoning
- CDA relies on bone-implant interface; osteoporosis causes subsidence
- Favors CDA
- Absent
- Favors ACDF
- Present
- Reasoning
- OPLL progresses; motion may worsen; fusion preferred
- Favors CDA
- Soft disc herniation
- Favors ACDF
- Severe osteophytes
- Reasoning
- CDA better with soft disc; extensive bony disease may need fusion
Overview
Cervical disc arthroplasty (CDA) is a motion-preserving surgical option for treatment of symptomatic cervical degenerative disc disease causing radiculopathy or myelopathy. The procedure involves removal of the pathological disc and replacement with an artificial prosthesis that maintains segmental motion.
Historical Development
The concept emerged from successful total hip and knee arthroplasty. The first cervical disc replacement was performed in 1966 by Fernström using a stainless steel ball bearing. Modern designs began with the Bryan disc (approved 2009), followed by ProDisc-C, Prestige LP, and Mobi-C.
Epidemiology and Usage
CDA represents approximately 5-10% of anterior cervical procedures internationally. Usage is increasing but remains limited by strict indications and device cost. Most common level is C5-6 followed by C6-7.
The primary theoretical advantage of CDA over ACDF is preservation of segmental motion to reduce stress on adjacent levels and potentially decrease adjacent segment disease. However, clinical superiority has not been definitively proven.
Pathophysiology and Mechanisms
Relevant Cervical Anatomy
Understanding the motion segment is essential for CDA:
Motion Segment Components:
- Intervertebral disc (nucleus and annulus)
- Facet joints (zygapophyseal joints)
- Uncovertebral joints (joints of Luschka)
- Ligaments (ALL, PLL, ligamentum flavum)
Normal Cervical Motion:
- Total cervical ROM: 45-55° flexion, 55-70° extension
- C5-6 and C6-7 contribute most motion (15-20° each)
- Coupled rotation/lateral bending
Biomechanics of CDA
Load Sharing:
- Healthy disc: 80% axial load through disc, 20% through facets
- After CDA: Similar load distribution if properly positioned
- Facet overload occurs with posterior device placement
Center of Rotation (COR):
- Normal COR is within the disc space, slightly posterior
- CDA devices attempt to replicate normal COR
- Anterior COR placement causes excessive facet loading
Adjacent Segment Biomechanics
Fusion Effects:
- Increased stress at adjacent levels
- Hypermobility compensation
- Accelerated degeneration over time
CDA Theoretical Benefits:
- Maintains near-normal motion
- Reduces stress concentration
- May slow ASD progression
CDA requires healthy facet joints to function properly. Facet arthropathy is a contraindication because the prosthesis cannot restore facet function, and motion preservation with diseased facets causes ongoing pain.
Device Classification
By Bearing Surface
Prestige LP (Medtronic):
- Titanium ceramic composite
- Ball-and-trough design
- Unconstrained articulation
- No polyethylene wear concerns
Advantages: Durable, low wear Concerns: Metal ion release, MRI artifact
The Prestige LP is a common choice given its long track record and IDE trial data showing non-inferiority to ACDF at 7 years.
By Constraint
Unconstrained:
- Bryan, Prestige
- Full freedom of motion
- Relies on soft tissues for stability
Semi-constrained:
- ProDisc-C, Mobi-C, PCM
- Ball-and-socket with controlled motion
- Some intrinsic stability
By Fixation
Keel Fixation: ProDisc-C - immediate stability, more bone removal Press-fit/Porous: Bryan, Prestige - bone ingrowth, less bone removal Screw Augmented: Some designs allow supplemental fixation
Classification Systems
McAfee Classification of Heterotopic Ossification
- Description
- No HO present
- Clinical Significance
- Normal outcome
- Incidence
- 30-40%
- Description
- HO present but not affecting ROM
- Clinical Significance
- Asymptomatic, no treatment needed
- Incidence
- 25-35%
- Description
- HO affecting ROM but not bridging
- Clinical Significance
- May limit motion, usually asymptomatic
- Incidence
- 15-25%
- Description
- Complete bridging HO
- Clinical Significance
- Spontaneous fusion, no motion
- Incidence
- 5-10%
- Description
- Complete fusion with ankylosis
- Clinical Significance
- No motion, may still be functional
- Incidence
- Less than 5%
HO formation is graded on postoperative imaging to assess motion preservation.
Clinical Assessment
Patient Selection - The Most Critical Step
- Age 25-55 years
- Single or 2-level disease (C3-C7)
- Radiculopathy or mild myelopathy
- Primarily soft disc herniation
- Normal facet joints on imaging
- No significant kyphosis
- Good bone quality
- No prior surgery at level
- Age over 60
- Facet arthropathy
- Significant instability
- OPLL or DISH
- Severe osteoporosis
- Severe kyphosis (more than 15°)
- Inflammatory arthritis
- Significant osteophyte formation
Physical Examination
Standard cervical spine examination with focus on:
- Neurological deficit (motor, sensory, reflexes)
- Spurling test for radiculopathy
- Myelopathy signs (Hoffmann, hyperreflexia, gait)
- Range of motion assessment
- Axial neck pain evaluation
Differential Diagnosis
Before offering CDA, confirm that symptoms arise from a compressible, motion-suitable cervical disc lesion and exclude mimics that would change management:
- Distinguishing Features
- Dermatomal arm pain, positive Spurling, MRI soft disc, healthy facets
- Key Investigation
- MRI
- Implication for CDA
- Ideal CDA candidate
- Distinguishing Features
- Older patient, uncovertebral osteophytes, multilevel change
- Key Investigation
- CT + MRI
- Implication for CDA
- Often favours ACDF if facet/bony disease
- Distinguishing Features
- Ossified PLL on CT, often multilevel myelopathy
- Key Investigation
- CT
- Implication for CDA
- Contraindication - progresses, fusion preferred
- Distinguishing Features
- Translation more than 3.5mm or angulation more than 11 degrees on dynamic films
- Key Investigation
- Flexion-extension X-ray
- Implication for CDA
- Absolute contraindication to CDA
- Distinguishing Features
- Non-dermatomal, distal Tinel/Phalen, normal neck exam
- Key Investigation
- Nerve conduction studies
- Implication for CDA
- Not a spinal lesion - CDA inappropriate
- Distinguishing Features
- Diffuse limb signs, Horner, weight loss, apical mass
- Key Investigation
- MRI brachial plexus / chest imaging
- Implication for CDA
- Excludes degenerative diagnosis
- Distinguishing Features
- Joint-pattern pain, no neurological deficit
- Key Investigation
- Examination + targeted imaging
- Implication for CDA
- Reassess indication for any cervical surgery
Contraindications
Absolute:
- Active infection
- Osteoporosis (T-score below -2.5)
- Metabolic bone disease
- Metal allergy (device-specific)
- Prior surgery at operative level
- Significant instability (translation more than 3mm)
- Ankylosing spondylitis
- OPLL
Relative:
- Facet arthropathy
- Moderate kyphosis
- More than 2 levels involved
- Age over 60
- Significant osteophyte formation
- Workers compensation claims
The most common exam question regarding CDA involves identifying contraindications. Remember OPLL, instability, facet arthropathy, and osteoporosis as the key contraindications that favor ACDF instead.
Investigations
Essential Imaging
Standard Series:
- AP, lateral, oblique views
- Flexion-extension lateral (dynamic)
Assessment Points:
- Disc height at affected level
- Alignment (lordosis vs kyphosis)
- Osteophyte formation
- Facet joint appearance
- Dynamic instability (translation, angulation)
- Adjacent level disease
Instability Criteria (contraindication to CDA):
- Translation more than 3.5mm
- Angulation more than 11° compared to adjacent levels
Dynamic imaging is essential for assessing stability and identifying contraindications to motion preservation.
Additional Studies
DEXA Scan: Assess bone mineral density - T-score below -2.5 is contraindication
EMG/NCS: Confirm radiculopathy, exclude peripheral neuropathy
Diagnostic Injections:
- Selective nerve root blocks for radiculopathy
- Facet injections if uncertain pain source
- Discography (controversial, rarely used)

Management Algorithm
Conservative Management First
All patients should fail adequate conservative treatment (typically 6-12 weeks):
- Activity modification
- NSAIDs, muscle relaxants
- Physical therapy
- Epidural steroid injections
Adequate conservative trial is mandatory before considering surgical intervention.
Surgical Technique
Standard Smith-Robinson Approach
Key Steps (identical to ACDF):
- Left-sided approach preferred (recurrent laryngeal nerve)
- Transverse skin incision at operative level
- Platysma divided in line with fibers
- Medial to carotid sheath, lateral to trachea/esophagus
- Longus colli retracted laterally
- Confirm level with fluoroscopy
Standard anterior cervical approach provides excellent visualization for disc arthroplasty.
Complications
Intraoperative Complications
Identical to ACDF:
- Recurrent laryngeal nerve injury (2-5%)
- Dysphagia (transient: 30-50%, persistent: 2-5%)
- Esophageal injury (rare but serious)
- Vascular injury (vertebral artery, carotid)
- Horner syndrome (sympathetic chain)
Prevention relies on meticulous technique and left-sided approach when possible to protect the RLN.
Postoperative Complications
Early:
- Hematoma (rare but serious)
- Infection (less than 1%)
- Neurological worsening (rare)
- Dysphagia (common, usually transient)
Late/Device-Specific:
- Incidence
- 2-5%
- Risk Factors
- Osteoporosis, endplate violation
- Management
- May require revision to fusion
- Incidence
- 15-70% radiographic
- Risk Factors
- Unclear, possibly surgical trauma
- Management
- Most asymptomatic; severe may limit motion
- Incidence
- Less than 1%
- Risk Factors
- Poor bone quality, malposition
- Management
- Revision surgery
- Incidence
- Rare clinically
- Risk Factors
- Metal-on-metal designs
- Management
- Usually not problematic
- Incidence
- 5-15%
- Risk Factors
- HO, natural progression
- Management
- May not require intervention
Heterotopic Ossification (HO)
McAfee Classification:
- Grade 0: No HO
- Grade I: HO present, not affecting motion
- Grade II: HO affecting motion but not completely bridging
- Grade III: Complete bridging (spontaneous fusion)
- Grade IV: Complete fusion with no motion
HO is radiographically common but clinically significant HO is relatively rare. Most patients maintain satisfactory motion despite some HO formation.
Postoperative Care
Immediate Postoperative Period
Day of Surgery:
- Mobilize out of bed same day
- Clear liquid diet, advance as tolerated
- Monitor for hematoma (airway compromise)
- Neurological checks every 2 hours
- Ice for swelling, voice rest
Day 1-2:
- Discharge home if stable (outpatient or overnight stay typical)
- No collar required in most cases
- Swallowing exercises for dysphagia
- Wound care instructions
Early Recovery (Weeks 1-6)
Activity Guidelines:
- ROM exercises begin immediately (unlike fusion)
- Light activities as tolerated
- Walking encouraged
- Avoid heavy lifting (more than 5 kg) for 2 weeks
- No driving until off narcotics and comfortable looking over shoulder
Wound Care:
- Keep incision clean and dry
- Steri-strips fall off naturally (7-14 days)
- Sutures/staples removed at 10-14 days
- No submerging wound for 2 weeks
Return to Activities
- Timeline
- 1-2 weeks
- Conditions
- As tolerated
- Timeline
- 2-4 weeks
- Conditions
- No heavy lifting
- Timeline
- 1-2 weeks
- Conditions
- Off narcotics, full neck ROM
- Timeline
- 6-12 weeks
- Conditions
- Full strength, no symptoms
- Timeline
- 3 months minimum
- Conditions
- Surgeon clearance required
- Timeline
- 3-6 months
- Conditions
- Based on clinical and radiographic progress
Follow-up Schedule
Standard Protocol:
- 2 weeks: Wound check, early progress
- 6 weeks: Clinical and radiographic assessment
- 3 months: ROM assessment, return to full activity clearance
- 6 months: Routine follow-up
- 12 months: Final outcome assessment
- Annually thereafter: As needed or per protocol
Radiographic Follow-up:
- Flexion-extension views to confirm motion preservation
- Assess device position and HO development
- Compare to baseline
Unlike ACDF which requires fusion healing (3-6 months immobilization focus), CDA allows immediate ROM exercises. This is a key advantage for early return to function and the primary reason no collar is needed.
Outcomes and Prognosis
Clinical Outcomes
IDE Trial Results (5-7 year follow-up):
Multiple prospective randomized trials have demonstrated:
- CDA is non-inferior to ACDF for neurological success
- Similar improvements in NDI, VAS arm, VAS neck
- Possibly lower reoperation rates with CDA
- Patient satisfaction equivalent
Range of Motion Preservation
Average ROM at Operated Level:
- Preoperative: 8-12°
- Postoperative: 7-10° (most motion preserved)
- Adjacent levels: No significant hypermobility
Adjacent Segment Disease
Radiographic ASD at 5-10 years:
- ACDF: 35-40%
- CDA: 20-25%
Symptomatic ASD (requiring surgery):
- ACDF: 2.9% per year
- CDA: 1-2% per year (possibly lower)
The reduction in adjacent segment disease is the primary theoretical advantage of CDA over ACDF. However, while radiographic ASD is clearly reduced, whether this translates to meaningful clinical benefit remains debated.
Long-Term Device Survivorship
At 10 years:
- Overall device survival: greater than 90%
- Revision to fusion: 5-10%
- Spontaneous fusion (HO): 5-15%
Guidelines, Registries & Global Practice
Global Epidemiology
Cervical degenerative disc disease causing radiculopathy or myelopathy is the indication for both ACDF and CDA. ACDF remains the most common anterior cervical procedure worldwide; CDA is a growing minority of anterior cervical operations, used selectively in younger patients with single- or two-level soft-disc disease and healthy facets. The strongest comparative evidence base is the suite of US FDA investigational device exemption (IDE) randomised trials, which underpin device approvals and guideline positions globally (Gornet et al. 2019, PMID 31226684; Radcliff et al. 2017, PMID 29372135).
Side-by-Side Guidance & Regulatory Position
- Position on CDA
- Single-level devices approved (Prestige, ProDisc-C, Bryan, Secure-C, PCM); Mobi-C and others approved for 1- and 2-level use
- Evidence Basis
- Level I IDE RCTs vs ACDF
- Position on CDA
- Cervical disc replacement may be used with normal arrangements for consent, audit and governance; evidence on efficacy and safety adequate for selected patients
- Evidence Basis
- Systematic review of RCTs
- Position on CDA
- CDA endorsed as an evidence-based alternative to ACDF in appropriately selected 1-2 level disease without instability, facet arthrosis or OPLL
- Evidence Basis
- Level I trial evidence; non-inferiority to ACDF
- Position on CDA
- Used selectively in younger single/two-level patients; ACDF remains the default for multilevel, deformity or instability
- Evidence Basis
- RCT evidence + Cochrane review (PMID 23656959)
- Position on CDA
- Accepted motion-preserving option; uptake varies by reimbursement and device access
- Evidence Basis
- RCT and registry/cohort data
Registry & Long-Term Evidence
There is no single dedicated international cervical-arthroplasty registry equivalent to the arthroplasty joint registries; long-term comparative evidence comes chiefly from the FDA IDE trials and pooled analyses. Pooled long-term RCT data (Zhang et al. 2020, PMID 32312321) show CDA roughly halves the odds of adjacent segment disease (OR 0.51) and reoperation (OR 0.41) versus ACDF, while the Cochrane review (Boselie et al. 2013, PMID 23656959) confirms clinical equivalence at 1-2 years with statistically favourable but not clinically decisive differences.
Practice Variation & Medicolegal Points
Uptake of CDA varies widely between health systems, driven less by clinical equipoise than by device cost, reimbursement and surgeon training. Documentation of selection criteria (single/two-level disease, stable segment, healthy facets, absence of OPLL and osteoporosis) and a clear consent discussion - that CDA is an alternative to the established ACDF, that data beyond 10 years remain limited, and that conversion to fusion may be required - is essential for medicolegal protection.
Special Considerations
Two-Level CDA
Only Mobi-C FDA-approved for 2 levels
Considerations:
- Patient selection even more critical
- Both levels must meet criteria
- Outcomes generally equivalent to single-level
- Cost implications
Failed CDA - Revision Options
Indications for Revision:
- Persistent pain with confirmed source
- Device failure (subsidence, migration)
- Progressive neurological deficit
- Severe HO limiting motion
Revision Options:
- Revision CDA (rare, technically demanding)
- Conversion to ACDF (most common)
- Posterior decompression/fusion
CDA Following Prior Fusion
Generally Contraindicated:
- Adjacent level CDA after ACDF controversial
- Some surgeons perform "hybrid" constructs
- Limited data on outcomes
- Risk of hypermobility at CDA level
Workers Compensation
Considerations:
- Higher failure rates reported
- May be relative contraindication
- Patient selection paramount
- Some surgeons avoid CDA in workers comp
Cost-Effectiveness
- Higher upfront device cost than ACDF
- Potential savings from reduced reoperations
- Cost-effectiveness studies show mixed results
- Value may emerge with longer follow-up
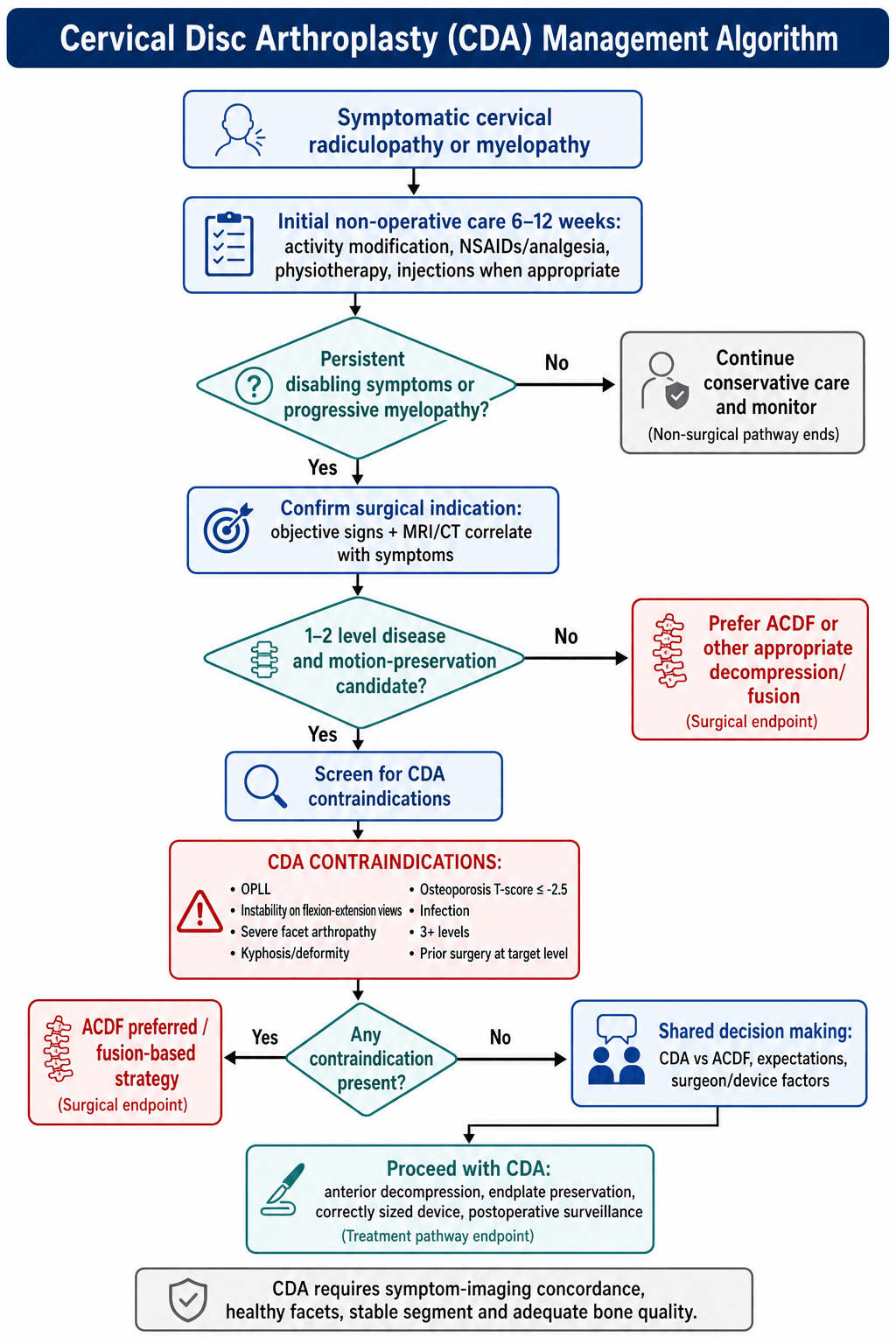
Clinical Algorithm
CDA Decision Pathway
Step 1: Confirm Indication
- Cervical radiculopathy or myelopathy
- Failed 6+ weeks conservative treatment
- Imaging correlates with symptoms
Step 2: Assess CDA Candidacy
- Age (ideal under 45, consider up to 60)
- Single or 2-level disease
- No facet arthropathy on CT
- No instability on dynamic radiographs
- No OPLL
- Adequate bone density (T-score above -2.5)
Step 3: Identify Contraindications
- Absolute: OPLL, instability, osteoporosis, infection
- Relative: Age over 60, facet disease, 3+ levels, kyphosis
Step 4: Shared Decision Making
- Present CDA vs ACDF options
- Discuss theoretical benefits and limitations
- Consider patient preferences and expectations
Step 5: Proceed with Appropriate Procedure
- CDA if all criteria met
- ACDF if any contraindication or patient preference
MCQ Practice Points
Q: What are the absolute contraindications to cervical disc arthroplasty?
A: The absolute contraindications include OPLL (ossification of posterior longitudinal ligament), segmental instability (translation more than 3.5mm or angulation more than 11°), severe osteoporosis (T-score below -2.5), active infection, and ankylosing spondylitis. Remember the mnemonic DISC: Deformity, Instability, Spondylosis (severe), Calcium loss.
Q: What is the primary theoretical advantage of CDA over ACDF?
A: The primary theoretical advantage is reduction in adjacent segment disease (ASD). By preserving motion at the operated level (8-10°), CDA reduces stress transfer to adjacent segments. Radiographic ASD is 20-25% with CDA vs 35-40% with ACDF at 10 years. However, whether this translates to meaningful clinical benefit remains debated.
Q: Which cervical disc arthroplasty device is FDA-approved for 2-level procedures?
A: Mobi-C is the only FDA-approved device for 2-level cervical disc arthroplasty. It has a mobile polyethylene bearing between cobalt-chrome endplates and demonstrated non-inferiority to ACDF in IDE trials. Other devices (Prestige LP, ProDisc-C, Bryan) are only approved for single-level use.
Q: A patient develops McAfee Grade III heterotopic ossification after CDA. What does this mean clinically?
A: McAfee Grade III indicates complete bridging heterotopic ossification, meaning spontaneous fusion has occurred. Grade 0 = no HO, Grade I = HO present but not affecting ROM, Grade II = HO affecting ROM but not bridging, Grade III = complete bridging, Grade IV = complete fusion with ankylosis. Despite Grade III HO, many patients remain functional as the segment is effectively fused.
Q: During cervical disc arthroplasty, you violate the inferior endplate with the burr. What should you do?
A: If significant endplate violation occurs, convert to ACDF. CDA relies on intact endplates for device stability and load distribution. Endplate violation increases subsidence risk significantly. For minor focal breaches with most endplate intact, cautious CDA may proceed with close monitoring. Patient safety takes priority over motion preservation goals.
At a Glance
- Details
- Motion-preserving alternative to ACDF using artificial disc prosthesis
- Details
- 5-10% of anterior cervical procedures internationally
- Details
- 25-55 years (ideal candidates)
- Details
- Cervical radiculopathy or myelopathy, 1-2 level disease, failed conservative Rx
- Details
- OPLL, instability, facet arthropathy, osteoporosis (T-score less than -2.5)
- Details
- Smith-Robinson (same as ACDF), left-sided preferred
- Details
- Preserve endplates (critical for device stability)
- Details
- Non-inferior to ACDF at 5-10 years
- Details
- 8-10° flexion-extension at operated level
- Details
- Radiographic ASD 20-25% vs 35-40% with ACDF at 10 years
- Details
- Prestige LP (M-on-M), ProDisc-C (M-on-P), Mobi-C (2-level approved)
- Details
- 15-70% radiographic, most asymptomatic
DISCDISC - CDA Contraindications
Hook:DISC problems contraindicate disc replacement - severe DISC disease needs fusion
MOTIONMOTION - CDA Benefits
Hook:MOTION preservation is the goal of cervical disc arthroplasty
IDEALIDEAL - Perfect CDA Candidate
Hook:IDEAL patient has soft disc, healthy facets, young age
BRYANBRYAN - First FDA-Approved Device (2009)
Hook:BRYAN disc was the landmark first approval for CDA in the US
Summary
Key Takeaways
-
Patient Selection is Paramount: CDA requires strict adherence to indications and contraindications - facet arthropathy, instability, OPLL, and osteoporosis preclude CDA
-
Equivalent Clinical Outcomes: Multiple IDE trials demonstrate CDA is non-inferior to ACDF for neurological success and patient-reported outcomes at 5-10 years
-
Motion Preservation: CDA maintains 8-10° of motion at the operated level, potentially reducing stress on adjacent segments
-
ASD Reduction: Radiographic ASD is reduced with CDA compared to ACDF, though clinical significance of this finding remains debated
-
Complications Differ: While approach-related complications are identical to ACDF, CDA has unique issues including HO, subsidence, and device-specific failures
-
Know the Contraindications: Exam questions commonly test identification of contraindications - remember DISC (Deformity, Instability, Spondylosis, Calcium loss)
-
Technique Differs: Unlike ACDF, endplate preservation is critical for CDA - violation may require conversion to fusion
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old office worker presents with 4 months of left C6 radiculopathy (weak wrist extension, diminished biceps reflex, lateral forearm numbness). MRI shows left C5-6 disc herniation with foraminal stenosis. She has failed physiotherapy and two epidural injections.”
“You are counseling a 58-year-old patient about CDA versus ACDF for single-level C6-7 disease. He asks about the advantages and disadvantages of each.”
“A 35-year-old woman is 6 months post cervical disc arthroplasty for C5-6 radiculopathy. She returns with new right C7 radiculopathy. MRI shows C6-7 disc herniation.”
“During a cervical disc arthroplasty at C5-6, you violate the inferior endplate of C5 with the burr.”
Indications
- Cervical radiculopathy or myelopathy
- Failed 6+ weeks conservative treatment
- 1-2 level disease (C3-C7)
- Imaging correlates with symptoms
Contraindications (DISC)
- Deformity - kyphosis more than 15°
- Instability - translation more than 3.5mm
- Spondylosis - facet arthropathy, OPLL
- Calcium loss - osteoporosis T-score below -2.5
Device Types
- Metal-on-metal: Prestige LP (Ti alloy)
- Metal-on-poly: ProDisc-C, Mobi-C
- Hybrid: Bryan (polymer nucleus)
- Mobi-C only FDA-approved for 2-level
Outcomes vs ACDF
- Clinical outcomes: Non-inferior at 5-10 years
- Motion preserved: 8-10° at operated level
- Radiographic ASD: Reduced (20-25% vs 35-40%)
- Reoperation: May be lower with CDA
Surgical Pearls
- Smith-Robinson approach (left side preferred)
- Preserve endplates (unlike ACDF)
- Center device in coronal and sagittal planes
- Fluoroscopy mandatory for positioning
Complications
- Approach-related: Same as ACDF (dysphagia, RLN)
- HO: 15-70% radiographic, usually asymptomatic
- Subsidence: 2-5% (avoid if osteoporosis)
- Spontaneous fusion: 5-15%
Evidence-Based Practice
Prestige LP 2-Level CDA vs ACDF - 10-Year IDE Trial (Gornet et al., 2019)
- Prospective randomised IDE trial: 209 two-level CDA vs 188 ACDF; 10-year follow-up over 84%
- Overall success at 10 years: 80.4% CDA vs 62.2% ACDF (statistically superior)
- Neurological success: 92.6% vs 86.1%; NDI success 88.4% vs 76.5%
- Index-level secondary surgery 4.7% vs 17.6%; adjacent-level 9.0% vs 17.9%
- Segmental motion maintained; severe (grade III/IV) HO 39.0% at 10 years
Mobi-C 2-Level CDA vs ACDF - 5-Year IDE Trial (Radcliff et al., 2016)
- Mobi-C is the only device FDA-approved for 2-level cervical arthroplasty
- Prospective randomised IDE trial: 225 two-level CDA vs 105 ACDF; 60-month follow-up over 86%
- Greater improvement in NDI and SF-12 PCS and higher satisfaction with CDA
- Reoperation 4% CDA vs 16% ACDF (statistically lower with CDA)
- No significant difference in adverse-event rates between groups
Cochrane Review - Arthroplasty vs Fusion, Single-Level Disease (Boselie et al., 2013)
- Cochrane systematic review of 9 RCTs (2400 participants), 5 at low risk of bias
- Results consistently favoured arthroplasty, often statistically significant
- For NO primary outcome was the difference clinically relevant
- Overall quality of evidence rated low to moderate at 1-2 years
- Long-term adjacent-segment benefit not yet confirmed at time of review
Bryan Disc vs ACDF - 4-Year IDE Trial (Sasso et al., 2011)
- Prospective randomised IDE trial: 242 Bryan CDA vs 221 single-level ACDF
- 48-month overall success 85.1% CDA vs 72.5% ACDF (p = 0.004)
- Greater NDI, neck-pain and arm-pain improvement with CDA (each p less than 0.03)
- Mean prosthesis range of motion 8.08 degrees at 24 months, 8.48 degrees at 48 months
- Similar total and serious adverse-event rates between groups
Long-Term Meta-Analysis - ASD & Reoperation, CDA vs ACDF (Zhang et al., 2020)
- Meta-analysis of 13 RCTs with mean 83.1-month (more than 60-month) follow-up
- Adjacent segment disease lower with CDA: OR 0.51 (95% CI 0.35-0.76, p = 0.001)
- Reoperation lower with CDA: OR 0.41 (95% CI 0.25-0.69, p = 0.001)
- Better clinical-score success with CDA: OR 1.54 (95% CI 1.15-2.08)
- Greater preserved range of motion with CDA (mean difference 1.77 degrees)
Mobi-C 1- & 2-Level CDA vs ACDF - 7-Year IDE Trial (Radcliff et al., 2017)
- 599 patients (1- and 2-level); 7-year follow-up overall 80.2%
- Two-level overall success 60.8% CDA vs 34.2% ACDF (p less than 0.0001) - CDA superior
- Single-level overall success 55.2% CDA vs 50% ACDF (non-inferior)
- Lower adjacent-level reoperation single-level (3.7% vs 13.6%) and 2-level (4.4% vs 11.3%)
- Index-level reoperation at 2 levels 4.4% CDA vs 16.2% ACDF (p = 0.001)