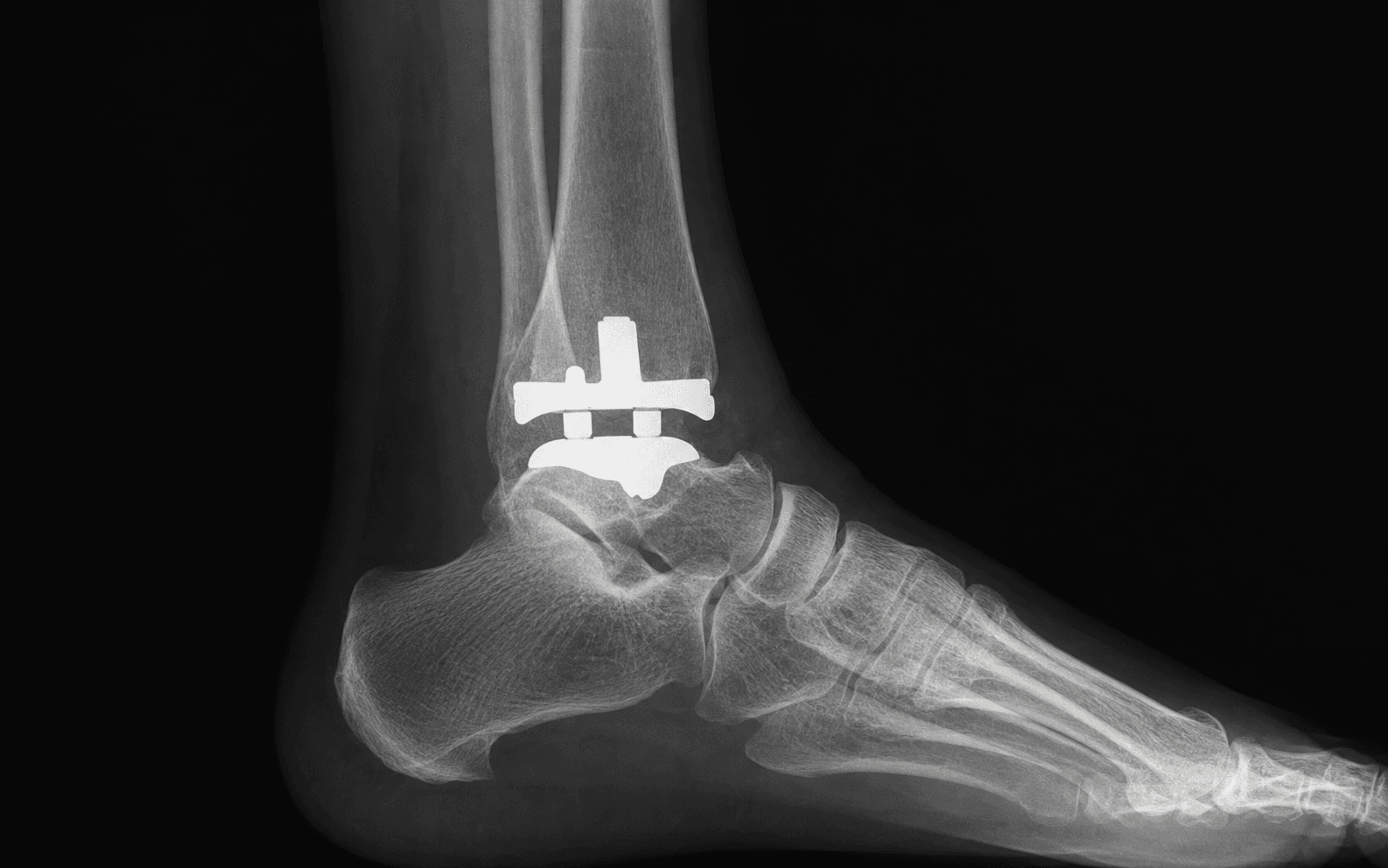
Motion-preserving arthroplasty for end-stage ankle arthritis via the anterior approach
- Motion preservation is the primary advantage over arthrodesis — it preserves 20-30 degrees of sagittal motion and protects the ipsilateral hindfoot and knee joints from accelerated degeneration.
- The anterior approach runs between tibialis anterior and extensor hallucis longus and protects the deep peroneal nerve and anterior tibial vessels — the interval is developed lateral to tibialis anterior to keep the neurovascular bundle safe.
- Three-component mobile-bearing designs allow greater sagittal and coronal motion than fixed-bearing implants but require precise coronal and sagittal alignment to avoid edge loading and early polyethylene wear.
- Wound complications occur in up to 15 percent of cases — meticulous soft-tissue handling, avoidance of excessive retraction, and layered closure over the anterior ankle are mandatory.
- “Indications favour lower-demand patients with well-aligned ankles and preserved talar bone stock — severe coronal deformity greater than 15-20 degrees, avascular necrosis of the talus, and peripheral neuropathy are relative contraindications.
- “The anterior approach places the deep peroneal nerve and anterior tibial artery immediately deep to the extensor retinaculum — identify and protect them before capsulotomy.
- “Coronal alignment must restore the mechanical axis to neutral or slight valgus — varus malalignment greater than 5 degrees accelerates polyethylene wear and increases the risk of malleolar fracture.
- “Registry data show 10-year survivorship of 70-85 percent for modern implants — revision is most commonly performed for aseptic loosening, subsidence, or infection.
When & Why
Indication. Symptomatic end-stage tibiotalar arthritis — most often post-traumatic — that has failed non-operative care, in a patient who is a good candidate for motion preservation. Typical primary indications: - End-stage primary or post-traumatic tibiotalar osteoarthritis with preserved motion and low-to-moderate physical demand
- Adjacent-joint arthritis (subtalar or talonavicular) where an arthrodesis would accelerate degeneration of those joints
- Patients who prioritise motion preservation over fusion for functional activities such as stair climbing or walking on uneven ground Contraindications. Absolute:
- Active or recent deep infection
- Avascular necrosis of the talus with collapse
- Severe fixed coronal deformity greater than 15-20 degrees not correctable by osteotomy
- Peripheral neuropathy (Charcot neuroarthropathy)
- Insufficient bone stock for component support Relative:
- High physical demand (manual labour, high-impact sports)
- Obesity (BMI greater than 35)
- Poor soft-tissue envelope or prior anterior incisions with compromised vascularity
- Young age (less than 50 years) with long life expectancy The one decision that matters: TAR or arthrodesis? Both relieve pain; they differ in what they trade. TAR buys motion and protects adjacent joints at the cost of a higher wound/infection burden and a finite implant lifespan; arthrodesis is more forgiving of demand and deformity but sacrifices the tibiotalar joint and accelerates adjacent-joint degeneration.
- Total Ankle Replacement
- 20-30 degrees sagittal motion retained
- Ankle Arthrodesis
- Complete loss of tibiotalar motion
- Total Ankle Replacement
- Reduces stress on subtalar and midfoot
- Ankle Arthrodesis
- Accelerates subtalar and midfoot degeneration
- Total Ankle Replacement
- 85-92 percent (registry data)
- Ankle Arthrodesis
- 90-95 percent (solid fusion)
- Total Ankle Replacement
- Higher (5-15 percent wound, 1-3 percent deep)
- Ankle Arthrodesis
- Lower (2-5 percent wound)
- Total Ankle Replacement
- Component exchange or fusion conversion
- Ankle Arthrodesis
- Revision fusion or TAR conversion
- Total Ankle Replacement
- Low-to-moderate activity
- Ankle Arthrodesis
- High-demand labour acceptable
Consent specifically for anterior wound problems (the most common complication, up to 15 percent), the small risk of deep infection and a two-stage revision if it occurs, intraoperative malleolar fracture, the possibility of talar component subsidence and revision surgery, and the long-term reality of a 15-25 percent revision rate at 10 years. Counsel that high-impact sport is discouraged and that the implant is not designed to last a lifetime. Setup. Supine with a bump under the ipsilateral hip to internally rotate the limb, the foot at the end of the table to allow full dorsiflexion and plantarflexion, and a thigh tourniquet inflated to 300 mmHg after exsanguination. Spinal or general anaesthesia with a regional block for postoperative analgesia; antibiotic prophylaxis (cefazolin, or vancomycin if MRSA risk) within 60 minutes of incision. Equipment: radiolucent table, large C-arm, ankle arthroplasty instrumentation, narrow-bladed oscillating saw, laminar spreaders, a Hintermann distractor and fluoroscopy.
The Operation
The goal: expose the ankle through the anterior approach while protecting the deep peroneal nerve and anterior tibial artery, debride the gutters completely, make balanced tibial and talar cuts that restore a neutral mechanical axis, implant a well-sized prosthesis, and close the anterior soft-tissue envelope without tension. The exposure and gutter work are laid out as the first steps below — they are the heart of the operation (and are covered in depth on the anterior approach to the ankle page).
Operative sequence
- Supine with a bump under the ipsilateral hip to internally rotate the limb; foot at the end of the table so the ankle moves through full dorsiflexion and plantarflexion; thigh tourniquet to 300 mmHg after exsanguination.
- Palpate and mark the tibialis anterior and extensor hallucis longus (EHL) tendons, the ankle joint line, and the navicular tuberosity.
- Plan the incision centred over the ankle joint, slightly lateral to the midline, running from 6-8 cm proximal to the joint line to the navicular tuberosity distally.
- The internervous interval lies between tibialis anterior (medial) and EHL (lateral); develop it lateral to tibialis anterior so the neurovascular bundle stays protected within the lateral flap.
- Incise the skin and the extensor retinaculum in line with the skin incision.
- Identify the deep peroneal nerve and anterior tibial artery — they lie immediately deep to the superior extensor retinaculum in the interval between tibialis anterior and EHL.
- Develop the interval lateral to the tibialis anterior tendon and control the bundle with a vessel loop, protected throughout the case.
- This is the step that decides whether the case is safe: identify the bundle under direct vision before any capsular work.
- Raise full-thickness flaps and perform a full-thickness capsulotomy; elevate the capsule medially and laterally as full-thickness flaps (avoid undermining — the anterior ankle skin is unforgiving).
- Expose the tibial plafond (trapezoidal — wider anteriorly than posteriorly) and the talar dome (biconcave with a central ridge).
- Assess the medial and lateral gutters and the ligaments: in severe varus the deltoid may be contracted and need release, and in valgus the lateral ligaments (anterior talofibular and calcaneofibular) may be attenuated.
- Remove all anterior, medial and lateral osteophytes with osteotomes and rongeurs.
- Debride the medial and lateral gutters completely — and the often-narrowed fibular gutter — so the components can sit in correct rotation without impingement.
- Verify clearance with a Freer elevator before moving to bony resection; residual osteophyte forces component malrotation and early polyethylene wear.
- Set the extramedullary tibial alignment guide parallel to the tibial crest; coronal alignment 0-2 degrees valgus; posterior slope 3-5 degrees for mobile-bearing designs.
- Protect the medial and lateral malleoli with retractors.
- Make the tibial cut with a narrow oscillating saw, ensuring the blade exits safely without fracturing a malleolus; confirm the cut surface is perpendicular to the mechanical axis.
- Reference the talar resection guide from the tibial cut.
- Perform the talar dome resection, protecting the posterior neurovascular structures; resect osteophytes from the talar neck and posterior aspect.
- Prepare the medial and lateral talar gutters to accept the component flanges; verify the talar cut is parallel to the tibial cut in the coronal plane.
- Insert trial tibial and talar components.
- Assess coronal and sagittal stability; perform any ligament releases or additional bone resection needed to achieve balanced gaps.
- Verify full dorsiflexion and plantarflexion without impingement; use fluoroscopy to confirm a neutral mechanical axis and appropriate component sizing.
- Remove the trials and irrigate the bone surfaces.
- For cemented components, apply cement to the tibial and talar surfaces and impact the final components; for press-fit designs, impact the components directly.
- Ensure no cement extrudes into the gutters or posterior capsule; confirm final alignment and stability with fluoroscopy.
- Close the capsule with absorbable suture and approximate the retinaculum.
- Close the subcutaneous layer and skin without tension (interrupted nylon or absorbable); consider a drain and a negative-pressure dressing in high-risk patients.
- Apply a sterile dressing and a posterior splint or boot with the ankle in neutral.
The neurovascular bundle lies immediately deep to the extensor retinaculum between tibialis anterior and EHL. Identify it under direct vision and control it with a vessel loop before capsulotomy; develop the interval lateral to tibialis anterior so the bundle remains in the protected lateral flap. Blind or overly medial dissection can transect the deep peroneal nerve or the anterior tibial artery.
Intraoperative malleolar fracture occurs in 5-10 percent of cases and is associated with poor outcomes. Use narrow oscillating saw blades, protect both malleoli with retractors as the blade exits, and consider prophylactic K-wire stabilisation in osteopenic bone. Over-resection when removing large anterior osteophytes can also compromise tibial support.
Spend the first 15-20 minutes on thorough medial and lateral gutter debridement. Residual osteophyte in either gutter forces component malrotation and causes edge loading. Use a narrow osteotome and pituitary rongeur under direct vision, then verify clearance with a Freer elevator before proceeding to bone resection.
Always perform a trial reduction and cycle the ankle through a full range of motion under fluoroscopy. Address any residual gutter impingement or edge loading before cementing or impacting the final components. Patient-specific and computer-navigated guides have substantially reduced alignment outliers.
Restore the mechanical axis to neutral or slight valgus. Residual varus greater than 5 degrees (or valgus greater than 10 degrees) accelerates asymmetric polyethylene wear and instability — verify on final fluoroscopy before leaving the theatre.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | 0-2 weeks | Posterior splint or boot, ankle neutral | Non-weight-bearing or heel-touch weight-bearing; elevation and ice; sutures out at 14-21 days | | 2 | 3-6 weeks | Walking boot, progressive weight-bearing | Active and active-assisted range of motion; oedema control and scar massage; proprioception from week 4 | | 3 | 7-12 weeks | Wean to supportive shoe | Full weight-bearing; formal physiotherapy for gait, strengthening and balance; low-impact activity at 8-10 weeks | | 4 | 3-6 months | — | Progressive strengthening and proprioception; return to work (sedentary 6-8 weeks, manual 12-16 weeks); low-impact sport at 4-6 months, high-impact discouraged | Most patients return to sedentary work by 6-8 weeks and manual work by 12-16 weeks; low-impact sport is permitted from 4-6 months and high-impact activity is discouraged. Complications
- Incidence
- 5-15 percent
- Recognition
- Erythema, drainage, exposed tendon or implant at 2-4 weeks
- Prevention and management
- Prevention: full-thickness flaps, layered closure without tension, negative-pressure dressing in high-risk patients. Management: local wound care, negative-pressure therapy, plastic surgery consultation for flap coverage if deep exposure
- Incidence
- 1-3 percent
- Recognition
- Persistent pain, swelling, sinus tract, elevated CRP/ESR, positive aspiration culture
- Prevention and management
- Prevention: antibiotic prophylaxis, meticulous haemostasis. Management: two-stage revision with antibiotic spacer and IV antibiotics for 6 weeks
- Incidence
- 5-10 percent
- Recognition
- Recognised on fluoroscopy or immediate postoperative radiograph
- Prevention and management
- Prevention: protect malleoli with retractors, narrow saw blades, prophylactic K-wires in osteopenic bone. Management: internal fixation with screws or tension-band wiring
- Incidence
- 3-8 percent at 5 years
- Recognition
- Progressive loss of height on serial radiographs, component migration
- Prevention and management
- Prevention: assess bone stock on preoperative CT, avoid over-resection. Management: revision to larger component, bone graft, or conversion to arthrodesis
- Incidence
- 5-15 percent at 10 years
- Recognition
- Progressive radiolucent lines, component migration, pain on weight-bearing
- Prevention and management
- Prevention: precise alignment, cement technique, patient selection. Management: revision TAR or arthrodesis
- Incidence
- 2-5 percent
- Recognition
- Pain after minor trauma, new fracture line on radiograph around keel or pegs
- Prevention and management
- Prevention: avoid stress risers, protect bone during implantation. Management: ORIF if displaced; non-operative if stable
- Incidence
- 5-10 percent at 10 years
- Recognition
- Cystic lucencies on radiographs, particle disease on histology
- Prevention and management
- Prevention: optimal alignment to minimise edge loading. Management: liner exchange, bone grafting of cysts, or revision
Viva & Exam Focus
ALIGNALIGN — preoperative planning and alignment goals
ANTERIORANTERIOR — approach and intraoperative safeguards
Critical danger structures and exam traps. Six structures and pitfalls account for most preventable failures and dominate the operative viva.
Lies immediately deep to the extensor retinaculum in the interval between tibialis anterior and EHL. Aggressive medial retraction or blind dissection can transect the deep peroneal nerve or anterior tibial artery. Identify the bundle under direct vision and protect it with a vessel loop before capsulotomy.
The medial malleolus is at risk during tibial resection if the saw blade exits medially; the lateral malleolus is vulnerable during fibular gutter preparation. Intraoperative malleolar fracture occurs in 5-10 percent of cases. Use narrow oscillating saw blades, protect the malleoli with retractors, and consider prophylactic K-wire stabilisation in osteopenic bone.
The talar component relies on subchondral bone stock — patients with prior trauma, avascular necrosis, or large cysts have reduced support. Subsidence greater than 3 mm leads to component migration, edge loading, and early failure. Preoperative CT assesses talar bone quality; bone graft or custom implants may be required in deficient cases.
A neutral mechanical axis and 3-5 degrees posterior tibial slope are required for mobile-bearing implants. Varus greater than 5 degrees or valgus greater than 10 degrees causes asymmetric polyethylene wear and instability. Use extramedullary or computer-assisted alignment guides and verify with intraoperative fluoroscopy before final implantation.
The anterior ankle incision is under tension with ankle motion and is vulnerable in patients with prior surgery, diabetes, or peripheral vascular disease. Superficial wound breakdown occurs in 5-15 percent; deep infection follows in up to 3 percent. Use full-thickness flaps, avoid undermining, close in layers without tension, and consider plastic surgery consultation for high-risk patients.
Stress risers occur at the tibial keel or talar pegs; polyethylene wear particles cause osteolysis around the components. Periprosthetic fracture risk is 2-5 percent at 5 years. Osteolysis presents with cystic lucencies on radiographs. Serial surveillance radiographs every 1-2 years detect early bone loss before catastrophic failure.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old woman with post-traumatic ankle arthritis presents with severe pain and stiffness. Standing radiographs show end-stage tibiotalar osteoarthritis with neutral coronal alignment, 5 degrees posterior tibial slope, and preserved talar bone stock. She is a retired office worker who walks daily for exercise. Discuss your surgical recommendation and the key technical steps for total ankle replacement.”
“You are planning total ankle replacement on a 58-year-old man with primary ankle osteoarthritis. Standing radiographs demonstrate 12 degrees of varus deformity with medial gutter narrowing and deltoid ligament contracture. How do you decide between corrective osteotomy, TAR, and arthrodesis?”
“A 65-year-old woman is 18 months after total ankle replacement with a mobile-bearing implant. She presents with new-onset activity-related pain and swelling. Standing radiographs show a 4 mm lucent line around the tibial component and cystic changes in the talus. What is your diagnostic work-up and management plan?”
Indications and contraindications
- Primary indication: end-stage tibiotalar OA with preserved motion, neutral alignment, low-to-moderate demand
- Motion preservation protects adjacent subtalar and midfoot joints from accelerated arthritis
- Absolute contraindications: active infection, talar AVN with collapse, fixed deformity greater than 15-20 degrees, neuropathy
- Relative contraindications: high demand, obesity, prior anterior incisions, age less than 50 years
Surgical anatomy — anterior approach
- Interval: between tibialis anterior (medial) and EHL (lateral) — develop lateral to tibialis anterior
- Deep peroneal nerve and anterior tibial artery lie immediately deep to the extensor retinaculum
- Protect the neurovascular bundle with a vessel loop before capsulotomy
- Medial and lateral gutters contain osteophytes that must be fully debrided to prevent impingement
- Tibial plafond is trapezoidal (wider anteriorly); talar dome is biconcave with central ridge
Alignment goals
- Coronal: 0-2 degrees valgus (neutral mechanical axis)
- Sagittal: 3-5 degrees posterior tibial slope for mobile-bearing designs
- Residual varus greater than 5 degrees or valgus greater than 10 degrees accelerates polyethylene wear
- Talar component subsidence risk increases with poor bone stock or over-resection
- Fluoroscopic verification of alignment before final implantation is mandatory
Implant designs
- Mobile-bearing (three-component): greater motion, requires precise alignment, risk of insert dislocation
- Fixed-bearing: more constrained, tolerates mild malalignment, less physiologic motion
- Choice depends on alignment, ligament integrity, and bone stock
- Registry 10-year survivorship 70-85 percent for modern implants
Complications
- Wound complications: 5-15 percent; risk factors include diabetes, prior surgery, prolonged operative time
- Deep infection: 1-3 percent; two-stage revision required for established infection
- Intraoperative malleolar fracture: 5-10 percent; protect with retractors and consider prophylactic fixation
- Talar subsidence: 3-8 percent; prevented by adequate bone stock and precise alignment
- Aseptic loosening and osteolysis: 5-15 percent at 10 years; most common long-term failure mode
Post-operative rehabilitation
- Weeks 0-2: protected weight-bearing in boot, early active ROM once wound stable
- Weeks 3-6: progressive loading, oedema control, scar massage, proprioception
- Weeks 7-12: wean to shoe, formal physiotherapy, return to low-impact activities
- Months 3-6: strengthening, gait training, return to work (sedentary 6-8 weeks, manual 12-16 weeks)
- High-impact sports discouraged; low-impact activities permitted at 4-6 months
Registry evidence and outcomes
- 5-year survivorship 85-92 percent; 10-year survivorship 70-85 percent (modern implants)
- Revision most commonly for aseptic loosening, subsidence, or infection
- TAR reduces adjacent-joint arthritis compared with arthrodesis but has higher wound and infection risk
- Patient selection and alignment accuracy are the strongest predictors of long-term success
Background & Evidence
Implant designs — the practical classification. Modern prostheses split into mobile-bearing (three-component) and fixed-bearing families. The choice rests on alignment, ligament integrity and bone stock.
- Mobile-bearing (three-component)
- Tibial tray, mobile polyethylene insert, talar component
- Fixed-bearing
- Tibial and talar components with a fixed polyethylene insert
- Mobile-bearing (three-component)
- Greater sagittal and coronal motion (up to 30-40 degrees total arc)
- Fixed-bearing
- More constrained; less physiologic motion
- Mobile-bearing (three-component)
- Precise alignment to avoid edge loading and insert dislocation
- Fixed-bearing
- Tolerates mild malalignment better than mobile-bearing
- Mobile-bearing (three-component)
- Higher insert dislocation risk
- Fixed-bearing
- Lower dislocation risk
- Mobile-bearing (three-component)
- Well-aligned ankle with good bone stock and competent ligaments
- Fixed-bearing
- Severe deformity or ligament insufficiency
- Mobile-bearing (three-component)
- STAR, Mobility, Salto Talaris, INBONE
- Fixed-bearing
- Various two-component designs
TAR versus arthrodesis — the evidence. Functional outcomes. Modern three-component mobile-bearing implants achieve 20-30 degrees of sagittal motion and improve AOFAS scores by 30-40 points at 5 years. Gait analysis shows more physiologic ankle kinematics and reduced compensatory knee and hip motion than arthrodesis. Patient-reported outcomes favour TAR for activities requiring ankle dorsiflexion; fusion patients report higher rates of adjacent-joint pain at 10 years. Survivorship and revision. Registry data (NJR, AJRR, AOANJRR) show 5-year survivorship of 85-92 percent and 10-year survivorship of 70-85 percent for contemporary implants. The 10-year revision rate is about 15-25 percent, most commonly for aseptic loosening, subsidence or infection. Arthrodesis has a lower re-operation rate for the index joint but higher rates of symptomatic adjacent-joint arthritis requiring later fusion. Wound and infection. Wound complications and infection are higher after TAR (5-15 percent wound issues, 1-3 percent deep infection) than after arthrodesis (2-5 percent wound). Arthrodesis non-union occurs in 5-10 percent and may require revision. Both procedures carry a risk of deep-vein thrombosis, though TAR patients mobilise earlier. Registry survivorship at a glance.
- Swedish Ankle Registry (Henricson 2011): 10-year survivorship 72 percent for early designs; modern implants exceed 80 percent
- UK National Joint Registry: 5-year revision rate approximately 8-12 percent for contemporary prostheses
- AOANJRR (Australia): 10-year revision rate 15-20 percent; mobile-bearing designs outperform fixed-bearing in some cohorts
- AJRR (United States): early data show 5-year survivorship greater than 85 percent with newer designs
References
Better implant survival with modern ankle prosthetic designs: 1,226 total ankle prostheses followed for up to 20 years in the Swedish Ankle Registry
- Registry analysis of 1,226 TARs with up to 20-year follow-up demonstrating improved survivorship with modern implant designs
- Contemporary implants showed significantly better 10-year survival than earlier generations in the Swedish Ankle Registry
- Aseptic loosening and infection remain the most common revision indications despite design improvements
The Agility Total Ankle Arthroplasty: A Concise Follow-up at a Minimum of 20 Years
- Minimum 20-year follow-up of the Agility TAR in a long-term cohort with documented survivorship and functional outcomes
- Implant demonstrated durability in selected patients beyond two decades
- Long-term complications included subsidence and polyethylene wear in some cases
Early Clinical Outcomes and Complications of Transfibular Total Ankle Arthroplasty: The Australian Experience
- Prospective series of transfibular TAR approach with early clinical and radiographic outcomes reported
- Complication profile included wound issues, malalignment, and early subsidence in the Australian cohort
- Patient-reported outcomes improved significantly but highlighted the learning curve for this approach
Survivorship of 4,748 Contemporary Total Ankle Replacements from the French Discharge Records Database
- Large database study of 4,748 TARs providing contemporary survivorship estimates from national records
- Overall revision rates and indications quantified at mid-term follow-up in a broad population
- Younger age and certain comorbidities associated with higher revision risk