Splits the anterior third of gluteus medius and minimus in line with their fibres, anterior to the superior gluteal nerve · advanced
- Splits the ANTERIOR third of gluteus medius in line with its fibres, staying anterior to the superior gluteal nerve - which enters the muscle 4 to 5 cm proximal to the greater trochanter in the posterior two-thirds. This is NOT a true internervous plane; it splits a single nerve territory.
- The most inherently stable of the hip approaches, with the lowest dislocation rate (0.5 to 1 percent), because the intact abductors act as a dynamic restraint.
- Main disadvantage: abductor dysfunction in 20 to 30 percent from splitting and detaching gluteus medius and minimus. The quality of the abductor repair is the single biggest determinant of outcome.
- Excellent exposure of BOTH the acetabulum and the femur - better than anterior for both, and better than posterior for acetabular visualization.
- Highest heterotopic ossification rate of all approaches (15 to 40 percent) from extensive soft-tissue stripping; routine prophylaxis is warranted.
When & Why
Indication. Symptomatic end-stage hip arthritis that has failed conservative management, where the surgeon wants excellent exposure of BOTH the acetabulum and the femur through a single, inherently stable approach. The commonest underlying diagnoses are: - Primary osteoarthritis (Kellgren-Lawrence Grade 3-4) after at least six months of failed non-operative care (NSAIDs, physiotherapy, weight loss, injections).
- Displaced femoral neck fracture in the elderly (typically greater than 65-70 years) needing a hemiarthroplasty or THA - the lateral approach exposes the femur well.
- Avascular necrosis (Ficat/Arlet Stage 3-4) from steroids, alcohol, sickle cell or idiopathic causes.
- Developmental dysplasia (Crowe I-III) - the lateral approach gives comprehensive access to a dysplastic acetabulum and femur.
- Inflammatory arthritis (rheumatoid, psoriatic, ankylosing spondylitis) with severe joint destruction, where synovectomy may also be needed.
- Post-traumatic osteoarthritis after an acetabular fracture or femoral neck malunion. Relative contraindications. Active infection (absolute, until eradicated), poor lateral soft tissues from previous burns, radiation or scarring, severe osteoporosis (greater trochanter fracture and poor repair healing), young high-demand patients (prefer an abductor-sparing approach), morbid obesity (difficult positioning and higher wound tension - consider anterior), severe coagulopathy, and uncorrected medical comorbidity. Where the lateral approach fits today. The Hardinge approach was the workhorse of the 1970s-1990s and remains the most inherently stable approach, but it is now the third choice (less than 10 percent of THAs) behind posterior and anterior because of its abductor dysfunction rate. Choose it when you genuinely need both-sided exposure and when stability is paramount.
You need excellent exposure of BOTH acetabulum and femur (complex primary, DDH), stability is paramount, and the surgeon is experienced with the technique.
Standard primary THA (the commonest approach worldwide, 60-70 percent), extensile revision exposure, abductor preservation, or femoral access for revision.
Young active patients wanting rapid recovery, the lowest abductor dysfunction risk, or a supine rapid-discharge protocol.
Consent specifically for abductor dysfunction (20-30 percent, the dominant complication) with Trendelenburg gait and lateral hip pain or weakness, the rare but devastating superior gluteal nerve injury, heterotopic ossification, leg-length discrepancy, dislocation (lower than other approaches), infection, periprosthetic fracture, and the usual anaesthetic and DVT risks. Setup. Lateral decubitus with the affected hip superior. The pelvis must be PERPENDICULAR to the table - confirm with C-arm or an alignment device, because pelvic rotation is the commonest cause of cup malposition. Pad the axilla (brachial plexus), the peroneal nerve at the fibular head, and the dependent limb at the malleoli. Secure the pelvis with anterior and posterior supports and a beanbag or wide straps.
The Operation
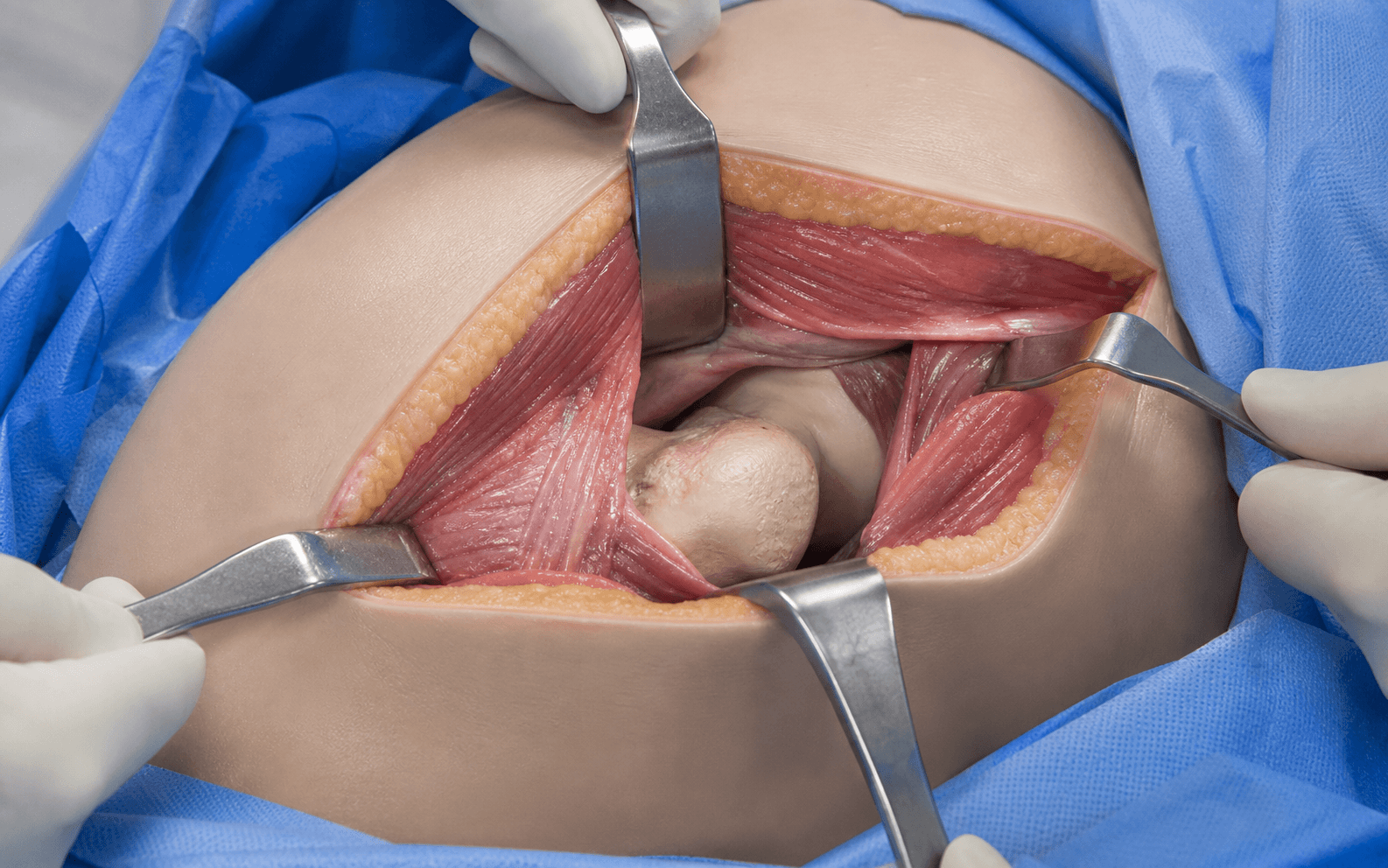
The goal: split the anterior third of gluteus medius and minimus in line with their fibres, reflect the anterior abductor-capsule sleeve off the greater trochanter, dislocate the hip, replace the acetabulum and femur, and then perform a meticulous transosseous abductor repair - the step that determines the outcome. The exposure is laid out in full as the first steps below.
Operative sequence
- Lateral decubitus, affected hip superior, pelvis perpendicular to the table (confirm with imaging).
- Palpate and mark the iliac crest (superior extent), the ASIS (anterior reference), the greater trochanter (the most prominent lateral landmark and the centre of the incision) and the femoral shaft axis (guides the distal extension).
- A longitudinal incision centred on the greater trochanter, along the femoral shaft axis.
- Length 15-20 cm total - 5-7 cm proximal to the greater trochanter and 10-12 cm distal.
- In lateral decubitus the incision is essentially vertical over the lateral hip.
- Deepen through subcutaneous fat with cautery, securing haemostasis.
- Identify the thick white fascia lata / iliotibial band over the lateral thigh and incise it longitudinally in line with its fibres directly over the greater trochanter.
- Excise the trochanteric bursa to expose the lateral surface of the gluteus medius muscle belly.
- Identify the anterior third of the gluteus medius belly and the tensor fascia lata just anterior to it (TFL is your anterior landmark - do not split into it).
- Split the medius in line with its fibres, starting at the trochanteric apex and extending proximally no more than 5 cm - the superior gluteal nerve enters the muscle 4-5 cm from the greater trochanter in the posterior two-thirds.
- Carry the split through full thickness to expose gluteus minimus beneath, and split minimus similarly, to expose the joint capsule.
- Elevate the anterior third to half of gluteus medius and minimus from the greater trochanter as a continuous muscle-capsule sleeve, reflecting it anteriorly and superiorly.
- Preserve the posterior portion of medius on the trochanter - this is the tissue you will repair back to.
- An alternative is a thin bone-wafer osteotomy (2-3 mm) carrying the tendons, for anatomic bone-to-bone repair - but it risks greater trochanter fracture if too much bone is taken.
- Incise the exposed anterior and superior capsule in a T- or H-pattern and tag the flaps; the capsule may be excised or preserved for repair (less critical than in the posterior approach).
- Dislocate by flexing, adducting and externally rotating the hip, placing a bone hook around the femoral neck, and delivering the head anteriorly.
- Mark the neck cut about 1 cm above the lesser trochanter (adjust for offset and anatomy).
- Cut with an oscillating saw perpendicular to the anatomic neck axis (not the shaft axis), protect the posterior wall with a retractor, and remove the head.
- Send the head for culture, histology and size measurement (head outer diameter minus 8-10 mm estimates the cup size).
- Place three retractors around the rim: anterior over the ilium (stay on bone, never intrapelvic), superior over the superior rim, and inferior over the transverse acetabular ligament (mind the sciatic nerve).
- Excise the labrum circumferentially and clear the pulvinar to see the walls.
- Identify the transverse acetabular ligament (TAL) - it marks the true floor and, when matched, sets native anteversion (about 20 degrees).
- Begin 2-4 mm smaller than the templated size and ream at 40 degrees inclination and 20 degrees anteversion (Lewinnek safe zone), using the TAL as a version guide.
- Ream concentrically to subchondral bone, looking for the bleeding-dot sign of healthy bone, increasing sizes until good rim fit.
- Make the final reamer 1-2 mm smaller than the cup for press-fit. Avoid excessive medial reaming (protrusio, floor weakness).
- Select a cup 1-2 mm larger than the final reamer and impact it at 40 degrees inclination and 20 degrees anteversion until it sits flush and does not toggle.
- Add screws only if needed (poor bone, large cup greater than 60 mm, inadequate press-fit, dysplasia, revision). Use the Wasielewski quadrant system: the anterosuperior quadrant (external iliac vessels) and anteroinferior quadrant (obturator vessels/nerve) are avoided, the posteroinferior quadrant risks the sciatic nerve, and the posterosuperior quadrant has the deepest, safest bone.
- Bring the femur into the wound in extension, adduction and external rotation; retract the abductors superiorly and release a little vastus lateralis if needed.
- Open the canal with a box chisel at the anteromedial calcar to achieve neutral alignment.
- Broach from 2-3 sizes below the template, in 10-15 degrees anteversion, until cortical chatter signals endosteal contact; the final broach defines the stem size.
- Stability (the key strength of this approach): test extension plus external rotation (anterior) and flexion plus adduction plus internal rotation (posterior) - the lateral approach should be rock-solid.
- Leg length: equal or up to 5 mm lengthening; measure from fixed landmarks.
- Offset: adequate soft-tissue tension without over-tightening.
- Range of motion: flexion 110-120 degrees, extension 20-30, abduction 45, adduction 30, rotation 45 each - checking for impingement. Adjust head, neck or stem choice as needed.
- Seat the final liner into a clean, dry cup taper until the snap of Morse-taper engagement; confirm full seating.
- Clean and dry the femoral canal, then impact the final stem (typically 1-2 mm proud of the final broach).
- Clean and dry both the stem trunnion and head bore, then impact the head with firm blows (5-6 for a 12 mm taper, 6-8 for larger heads) - inadequate seating drives trunnionosis and taper corrosion.
- Roughen the greater trochanter to a bleeding bed and drill 3-5 holes (2.0-2.5 mm) from the lateral cortex, exiting anterolateral or superolateral, spaced 10-15 mm apart.
- Pass heavy non-absorbable sutures (Ethibond #5 or FiberWire #2) through the medius and minimus tendon and then the bone tunnels, with the hip in neutral or slight abduction.
- Use multiple interrupted sutures, reduce any bone wafer anatomically, and test the repair - it must be solid without gapping or pulling through.
- Copious irrigation, then layered closure: any residual medius split, fascia lata/IT band (the strong layer), subcutaneous and skin.
- Drain optional (modern practice often omits it).
- Mobilise day 0, weight-bearing as tolerated with good bone and repair (toe-down if poor), abduction precautions for 6 weeks (no active abduction), DVT prophylaxis for 35 days, and heterotopic ossification prophylaxis (indomethacin 75 mg daily for 6 weeks) given the high HO rate of this approach.
The superior gluteal nerve (L4-L5-S1) exits the pelvis above piriformis and enters gluteus medius 4-5 cm proximal to the greater trochanter, running in the POSTERIOR two-thirds of the muscle. Split only the ANTERIOR third of the medius, use TFL as your anterior landmark, and limit the proximal split to 5 cm. Injury causes complete abductor paralysis with a severe, usually permanent Trendelenburg gait.
Examiners want you to say it plainly: the direct lateral approach is NOT an internervous plane - it splits the anterior third of gluteus medius (a single superior gluteal nerve territory) in line with its fibres specifically to stay anterior to the nerve branches in the posterior two-thirds, and the proximal split is capped at 5 cm because the nerve enters the muscle at 4-5 cm.
The lowest dislocation rate of any approach (0.5-1 percent) is now matched by a posterior approach with capsular repair (1-2 percent) and the anterior approach (0.5-2 percent), both of which spare the abductors. The 20-30 percent abductor dysfunction rate is the reason use has fallen below 10 percent.
Aftercare & Complications
Rehabilitation | Phase | Timing | Weight-bearing / motion | Focus | |-------|--------|--------------------------|-------| | 1 | 0-2 weeks | Mobilise day 0; WBAT with good repair (TDWB if poor); walker or crutches | Abduction precautions - NO active abduction; free flexion | | 2 | 2-6 weeks | Protected weight-bearing; passive ROM | Strengthen flexors, extensors and adductors - NOT abductors yet | | 3 | 6-12 weeks | WBAT; begin active abduction at 6 weeks | Gait normalisation, abductor strengthening, stairs | | 4 | 3-6 months | Full activity | Return to low-impact sport; impact sport by 6 months if recovered | Abduction precautions for 6 weeks are unique to this approach and protect the repair. Most patients return to desk work by 6 weeks; impact sport is delayed to 6 months. Around 85-90 percent are satisfied, though function is limited by the abductor dysfunction rate. Heterotopic ossification prophylaxis (indomethacin 75 mg daily for 6 weeks, or a single 7-8 Gy dose within 72 hours if NSAIDs are contraindicated) is routine given the highest-in-class HO rate. Complications
- Recognition
- Trendelenburg gait, lateral hip pain and weakness, positive Trendelenburg test
- Prevention
- Meticulous transosseous repair; protect 6-12 weeks; optimise bone health
- Management
- Physiotherapy with compensation strategies, cane in the opposite hand; revision repair or tendon transfer if severe
- Recognition
- Complete abductor weakness immediately postoperatively, severe Trendelenburg gait
- Prevention
- Split anterior third only; limit proximal split to 5 cm; use TFL as a landmark
- Management
- Usually permanent; physiotherapy for compensation, abductor reconstruction or tendon transfer if severe
- Recognition
- Progressive stiffness weeks to months postoperatively; ectopic bone on radiograph (Brooker I-IV)
- Prevention
- Indomethacin 75 mg daily for 6 weeks, or single-dose radiation 7-8 Gy within 72 hours
- Management
- Most asymptomatic - observe; excise mature Brooker III-IV ankylosis with postoperative prophylaxis
- Recognition
- Sudden severe pain, short malrotated leg; radiograph confirms
- Prevention
- Correct component position (40 degrees inclination, 20 degrees anteversion); restore offset
- Management
- Closed reduction under sedation; investigate cause; revision if recurrent (rare here)
- Recognition
- Visible fracture line or instability during detachment or drilling; postoperative radiograph
- Prevention
- Thin bone wafer only; careful 2.0-2.5 mm drilling; gentle impaction
- Management
- Cable or cerclage wiring or tension band; protected weight-bearing and delayed active abduction
- Recognition
- Crack or loss of stability during broaching or impaction; postoperative radiograph
- Prevention
- Templating to avoid varus; careful broaching; recognise osteoporosis
- Management
- Vancouver B1 stable stem - plate or cables; B2 loose stem - revision long stem; B3 poor bone - allograft or megaprosthesis
- Recognition
- Foot drop, posterior leg and plantar numbness immediately postoperatively
- Prevention
- Keep hip flexed; gentle retraction; careful inferior retractor; limit leg lengthening
- Management
- Remove tension (leg length, cement); baseline electrophysiology at 3 weeks; AFO; explore if no recovery by 3 months
- Recognition
- Wound erythema, drainage, warmth; raised CRP or ESR within 2 weeks
- Prevention
- Cefazolin within 60 minutes; glucose control; haemostasis; layered closure
- Management
- Early with stable implant - washout and modular exchange, retain components, IV antibiotics; late or loose - two-stage revision
- Recognition
- Pain years postoperatively, squeaking, ALVAL, raised metal ions, pseudotumor on MRI
- Prevention
- Firm head impaction; clean and dry both tapers; avoid ceramic-on-titanium pairings
- Management
- Revision with head and usually stem exchange; debride ALVAL tissue; send tissue for metal analysis
Viva & Exam Focus
LATERALLATERAL - key features of the approach
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Why has the lateral approach fallen out of favour compared to the anterior and posterior approaches?”
“How do you protect the superior gluteal nerve during the lateral approach, and what are the consequences of injury?”
“Describe your technique for repairing the abductors in the lateral approach and the factors that affect healing of the repair.”
Current role
- Was the commonest approach (1970s-1990s), now third choice (less than 10 percent) after posterior and anterior
- Lowest dislocation rate (0.5-1 percent) - abductors give active stability
- Declining because of abductor dysfunction (20-30 percent) and high HO rate (15-40 percent)
Key anatomy
- NOT a true internervous plane - splits the anterior third of gluteus medius (superior gluteal nerve territory) in line with fibres
- Superior gluteal nerve enters medius 4-5 cm from the greater trochanter in the posterior two-thirds - cap the proximal split at 5 cm
- Splits medius and minimus, reflecting the anterior portion off the greater trochanter as a muscle-capsule sleeve
Critical steps
- Lateral decubitus with a perpendicular pelvis (rotation causes cup malposition)
- Longitudinal incision centred on the greater trochanter, 15-20 cm
- Split the anterior third (TFL as anterior landmark), reflect the anterior abductor sleeve, T-capsulotomy, dislocate
- Excellent exposure of BOTH acetabulum and femur
Component positioning
- Ream to the bleeding-dot sign; cup at 40 degrees inclination and 20 degrees anteversion (Lewinnek), final reamer 1-2 mm smaller than cup
- TAL sets native anteversion; screws if needed go in the posterosuperior Wasielewski quadrant
- Broach to cortical chatter; clean and dry both tapers; firm head impaction (5-6 hits for a 12 mm taper)
Abductor repair - the determinant
- Roughen the greater trochanter to a bleeding bed; 3-5 drill holes (2.0-2.5 mm)
- Heavy non-absorbable sutures (Ethibond #5 or FiberWire #2), hip in neutral or slight abduction
- Test the repair is solid; protect for 6 weeks (no active abduction)
Complications
- Abductor dysfunction 20-30 percent (highest of any approach) - Trendelenburg gait
- Superior gluteal nerve injury 2-5 percent - usually permanent abductor paralysis
- Heterotopic ossification 15-40 percent - prophylax with NSAIDs or radiation
- Greater trochanter fracture 2-5 percent; dislocation only 0.5-1 percent
Approach comparison
- Dislocation: lateral 0.5-1 percent (lowest) vs posterior 2-5 (1-2 with repair) vs anterior 0.5-2
- Abductor dysfunction: lateral 20-30 percent (highest) vs posterior 1-5 vs anterior 1-3
- Nerve at risk: superior gluteal (lateral), sciatic (posterior), LFCN/femoral (anterior)
Background & Evidence
Epidemiology and current role. Total hip arthroplasty is one of the most performed and most cost-effective elective operations in orthopaedics. The direct lateral (Hardinge) approach was the commonest approach worldwide through the 1970s-1990s; it now accounts for less than 10 percent of primary THAs in most countries, behind the posterior approach (60-70 percent) and the anterior approach (20-30 percent and growing). Relevant gluteal anatomy. - Gluteus medius - origin the outer ilium between the anterior and posterior gluteal lines; insertion the lateral and superoposterior greater trochanter; superior gluteal nerve (L4, L5, S1); primary hip abductor (anterior fibres medially rotate and flex). The approach splits its anterior third.
- Gluteus minimus - origin the outer ilium between the anterior and inferior gluteal lines; insertion the anterior greater trochanter and capsule; superior gluteal nerve; abducts and medially rotates and stabilises the head. Lies deep to medius and is split with it.
- Superior gluteal neurovascular bundle - L4-L5-S1, exits the greater sciatic foramen ABOVE piriformis, runs between medius and minimus, and enters medius 4-5 cm proximal to the greater trochanter in the posterior two-thirds. Injury causes complete abductor paralysis.
- Tensor fascia lata - anterior to medius; the anterior landmark of the split. The surgical plane - and how the other approaches differ. The direct lateral approach is NOT a true internervous plane: it splits the anterior third of gluteus medius (superior gluteal nerve territory) in line with its fibres, between the anterior and posterior portions of medius and minimus. By contrast, the posterior (Moore) approach uses a true internervous plane between the superior gluteal nerve (medius and minimus) and the inferior gluteal nerve (maximus) but carries a higher dislocation risk; the anterior (Smith-Petersen/DAA) uses a true internervous plane between the femoral nerve (sartorius) and the superior gluteal nerve (TFL), best preserving the abductors but with limited femoral exposure and lateral femoral cutaneous nerve risk; and the anterolateral (Watson-Jones) passes between TFL and medius - two muscles of the same nerve - so it shares the lateral approach's abductor risk.
- Lateral (Hardinge)
- 0.5-1% (lowest)
- Posterior
- 2-5% (1-2% with repair)
- Anterior (DAA)
- 0.5-2%
- Comment
- Lateral's key advantage
- Lateral (Hardinge)
- 20-30% (highest)
- Posterior
- 1-5%
- Anterior (DAA)
- 1-3%
- Comment
- Lateral's main disadvantage
- Lateral (Hardinge)
- 15-40% (highest)
- Posterior
- 3-10%
- Anterior (DAA)
- 5-15%
- Comment
- Extensive soft-tissue stripping
- Lateral (Hardinge)
- Superior gluteal (2-5%)
- Posterior
- Sciatic (1-2%)
- Anterior (DAA)
- LFCN/femoral (5-15%)
- Comment
- Different nerve in each
- Lateral (Hardinge)
- 1-2%
- Posterior
- 1-2%
- Anterior (DAA)
- 2-4%
- Comment
- DAA higher on the learning curve
- Lateral (Hardinge)
- less than 10% (declining)
- Posterior
- 60-70% (commonest)
- Anterior (DAA)
- 20-30% (growing)
- Comment
- Trend away from lateral
Greater trochanter and capsule. The greater trochanter receives medius (superolateral facet), minimus (anterior facet), piriformis (medial apex), the obturator internus and gemelli (medial), and obturator externus (trochanteric fossa); its blood supply is chiefly the medial femoral circumflex artery. Detachment or fracture therefore causes abductor failure, which is why the repair is critical. The hip capsule attaches from the acetabular rim to the femoral neck (intertrochanteric line anteriorly, above the neck posteriorly) and is reinforced by the iliofemoral (strongest), pubofemoral and ischiofemoral ligaments. Survivorship (registry evidence). Major arthroplasty registries (NJR England/Wales/NI/IoM, AOANJRR Australia, the Swedish register, the New Zealand registry) report broadly consistent revision rates for primary THA of about 1-1.5 percent at 1 year, 3-4 percent at 5 years, 5-6 percent at 10 years, and 7-9 percent at 15 years. Registry data show no clinically important difference in all-cause revision between lateral, posterior and anterior approaches; reasons for revision include aseptic loosening, dislocation and instability (lowest for lateral), infection, periprosthetic fracture, and abductor failure (more specific to lateral). Younger age, AVN, DDH and low surgeon or unit volume raise revision risk. Functional outcomes. Satisfaction is 85-90 percent (slightly lower than posterior or anterior, driven by abductor dysfunction). Oxford Hip Scores average 40-42 out of 48. Normal abductor strength returns in 60-70 percent; about 5-10 percent have an obvious Trendelenburg gait, and 1-2 percent severe abductor failure from nerve injury.
References
The direct lateral approach to the hip
- Original description of the transgluteal approach: the gluteus medius and minimus are split in line with their fibres and the anterior portion is reflected off the greater trochanter in continuity with the vastus lateralis and anterior capsule as a single myofascial sleeve
- Avoids a formal trochanteric osteotomy and its associated non-union and wire-related complications, while preserving the posterior abductor insertion for repair
- Key technical caveat: the split must stay anterior and not be carried more than a few centimetres proximal to the trochanter to avoid the superior gluteal nerve branches
The safe distance for the superior gluteal nerve in direct lateral approach to the hip and its relation with the femoral length: a cadaver study
- In 15 cadaveric hips, the in-line split through gluteus medius lay within the anterior third of the muscle in every specimen, confirming the anatomical rationale of the anterior-third split
- Mean distance from the prominent lateral trochanter to the most inferior branch of the superior gluteal nerve was 44 mm, but in 3 of 15 hips it was under 30 mm
- The safe distance did not correlate with femoral length or body height, so a fixed proximal limit cannot be guaranteed safe in every patient
Surgical approach, abductor function, and total hip arthroplasty dislocation
- Pooled analysis of 13,203 primary THAs: dislocation rate 0.55% for the direct lateral approach versus 3.23% for posterior (3.95% without and 2.03% with posterior soft-tissue repair) and 2.18% for anterolateral
- Across 8 studies of 2,455 hips, postoperative limp occurred in 4 to 20% after the lateral approach versus 0 to 16% after the posterior approach
- Posterior capsular and short-rotator repair roughly halves the posterior dislocation rate, narrowing but not eliminating the lateral approach stability advantage
Posterior versus lateral surgical approach for total hip arthroplasty in adults with osteoarthritis
- Cochrane review of 4 prospective comparative studies (241 participants): no statistically significant difference in dislocation (1.3% lateral versus 4.2% posterior; RR 0.35, 95% CI 0.04 to 3.22)
- Total nerve injury was significantly higher with the direct lateral approach (2 of 43, 2% versus 10 of 49, 20%; RR 0.16 favouring posterior), though no single nerve reached significance
- Hip internal rotation in extension was greater after the posterior approach; overall evidence quality was judged insufficient for a firm recommendation
Abductor function after total hip replacement. An electromyographic and clinical review
- EMG and clinical review of 79 hips (direct lateral, modified direct lateral with trochanteric sliver, and posterior): a positive Trendelenburg test was far more common after the direct lateral approach (8 of 29) than after the other approaches (1 each)
- Frank denervation was uncommon (5 of 28 abductor-weak hips), implying most abductor dysfunction is mechanical (detachment or repair failure) rather than superior gluteal nerve injury
- Radiographic union of the trochanteric sliver in the modified group was associated with significantly better abductor function than malunion or non-union
Further reading 1. Palan J, Beard DJ, Murray DW, Andrew JG, Nolan J. Which approach for total hip arthroplasty: anterolateral or posterior? Clin Orthop Relat Res. 2009;467(2):473-477. 2. Sheth D, Cafri G, Inacio MC, Paxton EW, Namba RS. Anterior and anterolateral approaches for THA are associated with lower dislocation risk without higher revision risk. Clin Orthop Relat Res. 2015;473(11):3401-3408. 3. Berend KR, Lombardi AV Jr, Mallory TH, et al. The long-term outcome of 755 consecutive constrained acetabular components in total hip arthroplasty. J Arthroplasty. 2005;20(7 Suppl 3):93-102. 4. Hardinge K, Cleary J. The direct lateral approach to the hip. Oper Orthop Traumatol. 2013;25(4):341-347. 5. Amlie E, Høvik Ø, Reikerås O. Dislocation after total hip arthroplasty with 28 and 32-mm femoral head. J Orthop Traumatol. 2010;11(2):111-115. 6. National and international arthroplasty registries (NJR England/Wales/NI/IoM, AOANJRR Australia, Swedish Arthroplasty Register, New Zealand Joint Registry). Annual Reports.