SuperPATH (Superior Portal Assisted Total Hip) — a minimally invasive 'micro-posterior' approach (Chow, Penenberg, Murphy 2011) that works through a superior capsular window while preserving the short external rotators and the posterior capsule
- SuperPATH preserves the external rotators (piriformis, obturator internus, gemelli, quadratus femoris) and the posterior capsule through a superior capsular window — the fundamental difference from the conventional posterior (Moore/Southern) approach, which divides them and then repairs them.
- The deep working interval is between gluteus minimus (retracted anteriorly) and the piriformis tendon (retracted posteriorly). No muscle or tendon is released — if you release the rotators it becomes a standard posterior approach.
- Dislocation runs 0.5 to 1 percent (about 0.8 percent in the 479-hip Gofton series), the lowest of any approach, because the posterior stabilisers are preserved — so NO hip precautions are needed.
- The trade-off is limited visualisation. Acetabular reaming, cup positioning and femoral preparation are done through the 3×4 cm window by tactile feedback and imaging, so femoral fracture (1 to 3 percent) and cup malposition (2 to 5 percent) are the dominant technical risks, especially early in the learning curve.
- The learning curve is 50 to 100 cases. The first 20 to 30 cases should be ideal patients (primary OA, normal anatomy, BMI less than 30) with a low threshold (5 to 10 percent) to convert to a conventional posterior approach.
- Recovery is rapid — immediate full weight bearing, no precautions, discharge on day 1 is common, driving at 2 to 4 weeks — but the functional advantage over the standard posterior approach resolves by one year.
When & Why
Indication. Symptomatic hip arthritis in a well-selected patient who wants rapid recovery and meets the anatomical criteria for a tissue-sparing approach. The ideal candidate has primary osteoarthritis with normal proximal-femur anatomy and a spherical head, a BMI less than 35, good bone quality and a small-to-medium femoral head. It also suits avascular necrosis with minimal head collapse (Ficat I to III), an elderly femoral-neck fracture with normal proximal-femur anatomy, and closely staged bilateral THR (2 to 4 weeks apart) where tissue preservation matters.
Primary OA with normal anatomy and a spherical head, BMI less than 35, good bone quality, a small-to-medium femoral head, and a patient who wants rapid recovery. Also suits AVN with minimal collapse, an elderly femoral-neck fracture with normal anatomy, and closely staged bilateral THR.
Mild acetabular dysplasia (Crowe I to II) with normal femoral anatomy, a fused but non-deformed ankylosed hip, inflammatory arthritis with preserved bone, or a hip previously arthroscoped for FAI once the anatomy is near-normal.
Severe proximal-femur deformity, a femoral head greater than 54 to 55 mm (cannot extract through the window), severe acetabular deformity (protrusio, Crowe III to IV), severe obesity (BMI greater than 40), active infection, or surgeon inexperience.
The one principle that defines the approach. SuperPATH (Superior Portal Assisted Total Hip) is one end of a continuum of posterior approaches — from micro (external-rotator-sparing, this technique) through mini (rotator-sacrificing) to the standard posterior. It is extensile: if exposure, anatomy or a complication demands it, you can extend the superior window and release the rotators to become a conventional posterior approach at any point. That extensility is the safety net of the technique. Consent specifically for the learning curve and a higher early technical-complication rate (femoral fracture, cup malposition, conversion to conventional in 1 to 5 percent), for dislocation being low but not zero, for possible leg-length discrepancy, and for the real possibility of conversion to a standard posterior approach if the anatomy will not cooperate. Setup. Lateral decubitus with the pelvis secured perpendicular to the table (CRITICAL — pelvic tilt is the main source of cup malposition when you cannot verify directly); a beanbag or dedicated positioner; pad bony prominences. Drape the C-arm into the field (strongly recommended, especially during the learning curve). Standard arthroplasty antibiotics and skin prep. Re-confirm templated cup size, stem size, offset and neck length before draping — intra-operative correction is hard through a small window.
SuperPATH rewards ideal anatomy and punishes complex anatomy. Deformity, severe obesity, a very large head, complex revision and surgeon inexperience are all reasons to choose a conventional posterior approach regardless of a patient's preference for a 'minimally invasive' scar. Safety over incision length, always.
The Operation
The goal: replace the hip through a 6 to 10 cm posterolateral incision by developing the gluteus-minimus-to-piriformis interval, creating a 3×4 cm superior capsular window, cutting the femoral neck in situ, preparing and implanting both components through that window, and leaving the external rotators and posterior capsule intact — so that nothing needs repairing and the hip is inherently stable. The exposure is laid out as the opening steps below (and is extensile to the posterior (Moore/Southern) approach to the hip if needed).
Operative sequence
- Lateral decubitus, affected hip superior; secure the pelvis perpendicular to the table (anterior support at pubis/ASIS, posterior at sacrum). Pelvic perpendicularity is CRITICAL for cup positioning, because you cannot verify it directly through a small window.
- Confirm pelvic position with the C-arm if available (AP view: symmetric obturator foramina, equal iliac-wing height). Pad the fibular head, malleolus and contralateral greater trochanter.
- Re-confirm templated cup and stem size, offset and neck length before draping — intra-operative troubleshooting is difficult through a limited exposure.
- Posterolateral incision, 6 to 10 cm long, centred 2 to 3 cm POSTERIOR to the greater-trochanter apex (more posterior than the 1 cm of a conventional posterior incision, to reach the superior capsule). Do not compromise safety for a small scar — use 10 to 12 cm in a larger or muscular patient.
- Deepen to and split the fascia lata/ITB and the gluteal fascia longitudinally over the posterior aspect of the greater trochanter, matching the skin incision.
- Identify the oblique fibre direction of gluteus maximus and split it BLUNTLY in the line of its fibres (finger or scissors, centred over the posterior GT, minimal bleeding if along the fibres). This is a muscle-splitting (not internervous) step that only provides superficial access.
- The defining deep interval is the next step, not this split. Protect the inferior gluteal neurovascular bundle by staying in the fibre line and avoiding cautery deep to the muscle.
- Clear the trochanteric bursa and fat. Identify the short external rotators from superior to inferior: piriformis (most superior, to the superior-posterior GT), obturator internus with the superior and inferior gemelli (common tendon to the medial GT), and quadratus femoris (ischial tuberosity to the intertrochanteric crest).
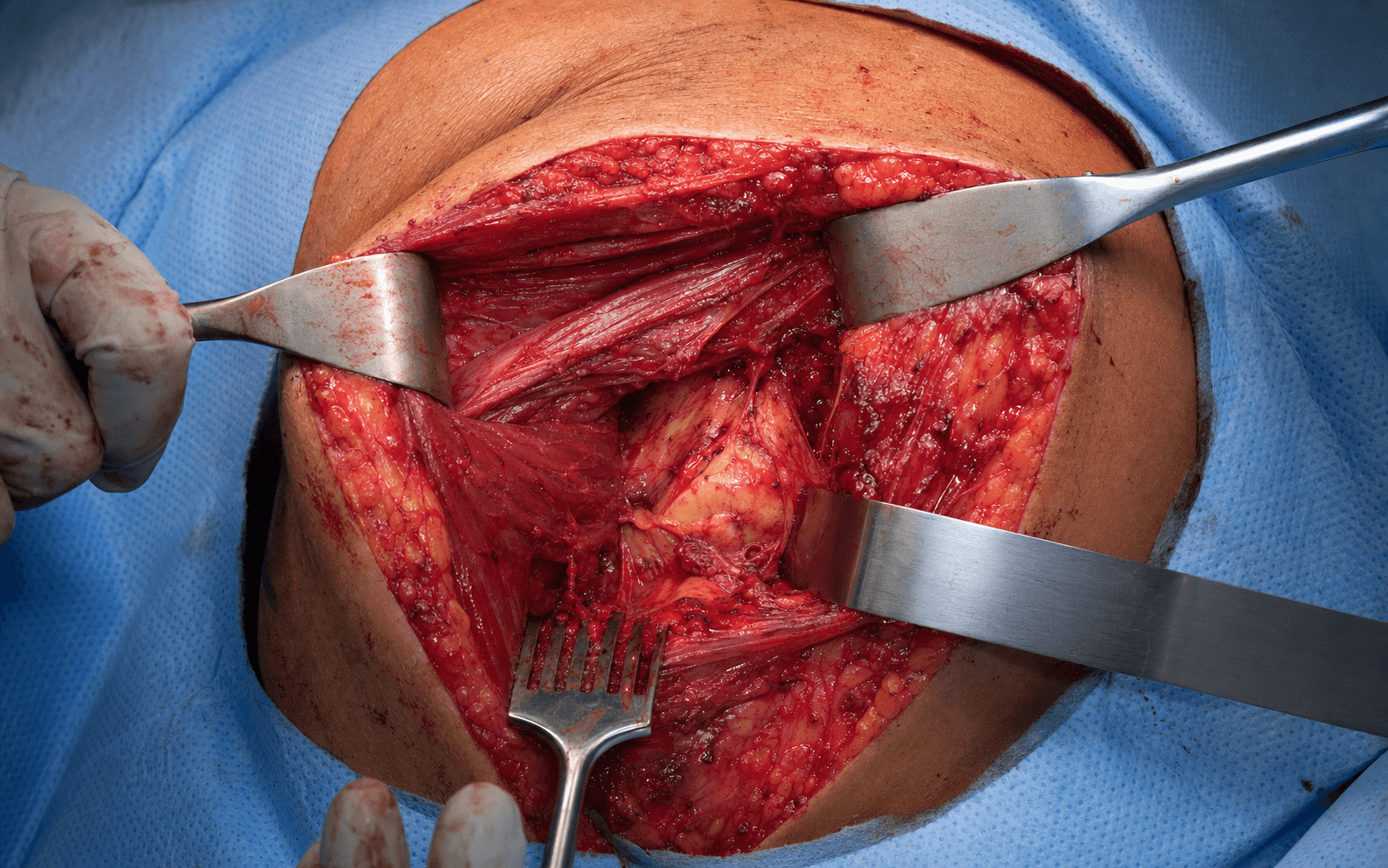
- HALLMARK: do NOT release them. Develop the interval between gluteus minimus (retracted anteriorly, together with gluteus medius) and the piriformis tendon (retracted posteriorly) using blunt or curved self-retaining retractors. This exposes the superior capsule over the saddle of the femoral neck WITHOUT dividing any muscle or tendon.
- The preserved piriformis, short rotators and intact posterior capsule shield the sciatic nerve (1 to 2 cm posterior) throughout. If you release the rotators, it is no longer SuperPATH.
- With minimus anterior and piriformis posterior, the superior capsule over the femoral-neck saddle is in view. Create a roughly 3×4 cm window: superior border = anterior acetabular rim, inferior = superior femoral neck, anterior = anterior capsular reflection, posterior = capsular thickening (do NOT extend into it).
- Smaller than 3×3 cm forces the technique and raises the complication rate; larger than 5×5 cm surrenders the preservation advantage. The posterior and inferior capsule stay INTACT — they are the primary posterior stabilisers.
- Cut the neck in situ through the window — SuperPATH never dislocates first. Use a curved oscillating blade or sequential angled passes, working circumferentially (anterior then lateral then posterior), protecting the acetabulum, posterior capsule and rotators with retractors.
- The 360 degree cut MUST be complete before any extraction. An incomplete cut plus forced head removal is the classic cause of proximal femoral fracture; confirm completeness by gently rotating the head, and consider fluoroscopy.
- Examiner nuance: in the canonical Chow description the femur is channelled and broached FIRST with the head and neck intact (the intact head acts as a handle and stabilises the proximal femur), then the neck is cut at the broach-neck level and the head removed, then acetabular work follows. The numbering here reflects a common acetabulum-first variant; either way, complete the osteotomy before extraction.
- Thread a corkscrew into the head (ream a starter hole if needed, engage subchondral bone) and deliver it through the window by rotation, flexion/extension and gentle leverage — not force. The head typically rotates out antero-superiorly.
- Heads greater than 50 mm get progressively harder; heads greater than 54 to 55 mm may be impossible to extract without enlarging the window (a relative or absolute contraindication). Always send the head for culture and histology. Head outer diameter plus 8 to 10 mm approximates the cup size.
- Place specialised curved retractors: an anterior Hohmann under the anterior rim (protects the femoral neurovascular bundle), a posterior retractor over the posterior wall (placed carefully — you cannot see the wall directly), and an inferior retractor beneath the transverse acetabular ligament (TAL).
- Excise the labrum circumferentially (anterior under vision, posterior by feel) and clear the pulvinar centrally. Palpate the TAL — it is the most reliable version landmark (parallel to the TAL is about 20 degrees anteversion). Only the anterior third-to-half of the acetabulum is seen directly; the posterior half is prepared by feel and fluoroscopy.
- Ream with curved handles through the window, starting 2 to 4 mm undersized and advancing 1 to 2 mm at a time. Feel the resistance change from cartilage (soft) to subchondral bone (hard) to cancellous bone (softer), and look for bleeding bone when the reamer is removed.
- Target 40 degrees inclination and 20 degrees anteversion (Lewinnek safe zone 30 to 50 degrees inclination, 10 to 30 degrees anteversion). Use the mechanical alignment guide for inclination and the TAL for version; confirm with fluoroscopy (AP inclination, cross-table lateral version).
- Avoid over-reaming (poor fixation, rim notching) and excessive medial reaming (protrusio). Excessive POSTERIOR reaming is the highest fracture risk — when in doubt, under-ream.
- Insert a cup 1 to 2 mm larger than the final reamer for press-fit (2 mm oversize in osteoporotic bone, line-to-line or 1 mm oversize in hard sclerotic bone), using a curved impactor with alignment guides, oriented to 40 by 20 degrees via guide plus TAL plus fluoroscopy.
- Impact with progressive mallet blows, listening for a rising pitch and feeling for seating; assess stability by levering the cup (it should be rock-solid). Most SuperPATH surgeons avoid screws (placement is difficult); if used, stay in the posterosuperior safe zone.
- Verify the final position fluoroscopically (AP: inclination, concentric seating, no fracture; lateral: anteversion). Cup malposition (2 to 5 percent) and posterior-wall fracture (1 to 3 percent) are the common acetabular errors — both born of limited visualisation.
- Flex and externally rotate the hip to deliver the proximal femur anteriorly through the same window (rotators still intact and retracted). Open the canal with a curved box chisel at the osteotomy site, removing anterior-medial calcar bone to a central entry — avoid varus entry, anterior cortex perforation, or lateral/GT entry.
- Broach with curved broaches (standard broaches hit the preserved rotators), starting undersized and advancing by feel: cortical chatter and firm mallet resistance signal endosteal contact; check depth against templating and rotational stability. Fluoroscopy (AP alignment, lateral depth and version) helps.
- You work entirely by tactile feedback and cannot see the canal. Conservative broaching is safer — a smaller stable stem beats an aggressive one with a fracture (1 to 3 percent).
- Assemble trial stem, head/neck and liner through the window. The hip should reduce with an audible clunk; a difficult reduction suggests malposition, impingement or interposed soft tissue.
- Assessment is LIMITED: measure leg length externally (ASIS to medial malleolus on both sides, or fluoroscopic comparison of the lesser trochanters), gauge soft-tissue tension by feel, and test stability with only gentle ROM — you cannot run a full conventional arc. Meticulous pre-operative templating carries the load here.
- Clean the cup taper and impact the liner until a LOUD snap (the lock engages) — you cannot see the lock directly, so some surgeons confirm seating with fluoroscopy. Clean and dry the canal; impact the final stem with a curved inserter to the templated depth (typically 10 to 15 degrees anteversion), seating it 1 to 2 mm proud of the final broach.
- Clean the stem taper (trunnion) and the head bore completely; impact the head straight with firm blows (a 28 to 36 mm head needs about 6 to 8 blows) until the final blow rings high-pitched. Confirm the final position with AP and lateral fluoroscopy.
- Reduce the hip (should be easy, with an audible clunk). Stability is inherent — the preserved posterior capsule (ischiofemoral ligament) plus the intact rotators give dual posterior restraints, so dislocation runs 0.5 to 1 percent despite only gentle intra-operative testing and NO post-operative precautions.
- Irrigate. The superior window is left open or loosely approximated; the rotators need NO repair (nothing was released, saving 15 to 20 minutes versus a conventional posterior repair). Close the fascia lata and skin in layers; drains are usually omitted because dead space is minimal.
The single step that defines SuperPATH is developing the gluteus-minimus-to-piriformis interval without releasing the short external rotators. Retract gluteus medius and minimus anteriorly and the piriformis tendon posteriorly with blunt, curved retractors. If you find yourself releasing the rotators off the greater trochanter, you have converted to a standard posterior approach — the stability and recovery advantages are gone. The preserved rotators and intact posterior capsule are also what shield the sciatic nerve, so retract the piriformis gently and avoid any dissection posterior to the capsule.
SuperPATH trades direct visualisation for soft-tissue preservation, so you must use every aid to accuracy: the transverse acetabular ligament for version (parallel is about 20 degrees anteversion), mechanical alignment guides on the reamer and impactor for 40-degree inclination, real-time fluoroscopy (AP for inclination, cross-table lateral for version and the posterior wall), and navigation or robotics where available. Cup malposition and posterior-wall fracture both stem from limited acetabular visualisation — technology is how you close that gap.
- Location
- Exits the sciatic notch below piriformis, 1 to 2 cm posterior to the capsule
- How it is protected
- More protected than in the standard posterior approach — preserved rotators and intact capsule form a barrier; retract piriformis gently, avoid posterior dissection
- Injury risk
- Less than 0.5 percent (lower than conventional 0.5 to 2 percent)
- Location
- Exits the greater sciatic notch above piriformis, 4 to 5 cm proximal to the GT, between medius and minimus
- How it is protected
- Limit proximal dissection to less than 5 cm above the GT; avoid deep superior retractor placement; split maximus only in its fibre line
- Injury risk
- Less than 1 percent
- Location
- Exits below piriformis with the sciatic nerve, supplies gluteus maximus
- How it is protected
- Blunt splitting of maximus strictly in the fibre line; avoid cautery deep to the muscle; minimal retraction
- Injury risk
- Less than 0.5 percent
- Location
- Posterior rim and wall — CANNOT be seen directly through the superior window
- How it is protected
- Conservative reaming by feel; fluoroscopy during reaming (lateral view shows the wall); gentle posterior retractor placement; controlled cup impaction
- Injury risk
- 1 to 3 percent fracture (higher than conventional, due to limited visualisation)
- Location
- Greater trochanter adjacent to the window; proximal shaft during broaching
- How it is protected
- Gentle head extraction avoiding GT leverage; conservative broaching by tactile feedback; curved instruments kept coaxial; fluoroscopy to confirm broach position
- Injury risk
- 1 to 3 percent (higher than conventional less than 1 percent)
Aftercare & Complications
Rapid-recovery rehabilitation | Phase | Timing | Mobilisation and precautions | Imaging and milestones | |-------|--------|------------------------------|------------------------| | 1 | Day 0 | Full weight bearing as tolerated, NO hip precautions, walker or crutches; multimodal pain control | — | | 2 | Day 1 | Discharge home is common (outpatient or 23-hour protocols); continue PT | — | | 3 | Week 2 | Wound check; staple or suture removal if used | — | | 4 | Week 6 | Progressive return to activity | AP pelvis and lateral hip X-ray: component position, occult fracture, heterotopic ossification | | 5 | Month 2 to 4 | Driving from about 2 to 4 weeks; desk job 3 to 4 weeks, manual 6 to 8 weeks; low-impact sport sooner, high-impact by 3 to 4 months | Clinical review | DVT prophylaxis. LMWH (enoxaparin 40 mg daily) or a DOAC (rivaroxaban, apixaban) for 35 days plus mechanical prophylaxis (TED stockings, intermittent pneumatic compression) and early mobilisation — the same protocol as conventional THR, with the SuperPATH advantage of walking on day 0. Heterotopic ossification runs 5 to 15 percent (LOWER than the 10 to 25 percent of a conventional posterior approach, because there is less soft-tissue trauma). In high-risk patients (ankylosing spondylitis, DISH, previous HO, hypertrophic OA), give prophylaxis — indomethacin 25 mg three times daily for 6 weeks, or a single 7 to 8 Gy radiation dose within 72 hours. Complications
- Recognition
- Intra-op: abnormal resistance or sound during broaching, fluoroscopic crack. Post-op: pain, X-ray fracture line at GT or shaft
- Prevention
- Conservative broaching by tactile feedback; curved instruments coaxial to the canal; fluoroscopy; complete neck osteotomy before extraction; low threshold to convert
- Management
- Vancouver classification: AG (GT avulsion) cables or screws if displaced; AL undisplaced protected weight bearing; AL displaced or B1 ORIF plate or cables; B2 or B3 revision long stem bypassing the fracture by 2 cortical diameters
- Recognition
- Intra-op: alignment guides or fluoroscopy outside the safe zone. Post-op: steep (greater than 50 degrees) or flat (less than 30 degrees) cup on X-ray, excessive anteversion or retroversion on the cross-table lateral
- Prevention
- TAL for version (parallel is 20 degrees); mechanical guides for inclination; real-time fluoroscopy; navigation or robotics; adequate 3×4 cm window; 50-plus cases before independent practice
- Management
- Asymptomatic and within the Lewinnek safe zone: observe. Outside the safe zone or symptomatic (impingement, instability, edge loading): revise the cup within 6 to 8 weeks, before bone ingrowth
- Recognition
- Intra-op: resistance change or crepitus during reaming or impaction, fragment retrieval, fluoroscopic disruption. Post-op: X-ray or CT wall fragment
- Prevention
- Concentric reaming by feel; conservative posterior reaming (err on under-reaming); fluoroscopy during reaming; controlled impaction; gentle posterior retractor placement
- Management
- Small crack with a stable cup: screws in the posterosuperior safe zone. Displaced or unstable: ORIF (lag screws, buttress or spring plate), often after extending to a conventional posterior exposure. Greater than 30 percent wall loss: consider a cage or augment construct
- Recognition
- Patient reports the hip giving way; leg shortened and rotated (posterior: IR; anterior: ER); X-ray shows the head out of the cup
- Prevention
- Preserved posterior capsule and rotators (dual restraints); appropriate head size (36 to 40 mm, dual mobility if high risk); cup in the Lewinnek safe zone; adequate soft-tissue tension
- Management
- Closed reduction under sedation (Allis maneuver); post-reduction X-ray then CT to find the cause. First episode: reduce, brace 6 weeks. Recurrent (2 or more) or irreducible: revise (cup position, larger head or dual-mobility liner, restore tension)
- Recognition
- Intra-op: crepitus or abnormal movement during head extraction or broaching. Post-op: lateral hip pain, Trendelenburg gait if displaced
- Prevention
- Do not lever the head against the GT; gentle broaching; adequate window so the head is not squeezed past the GT; recognise the vulnerable osteoporotic GT
- Management
- Undisplaced (less than 1 cm, abductors intact): protected weight bearing and abduction brace. Displaced or abductor dysfunction: ORIF with tension band or cables and plate. Persistent nonunion with abductor failure: trochanteric advancement
- Recognition
- Post-op foot drop (common peroneal division most often), posterior thigh or leg numbness; EMG confirms and localises
- Prevention
- Lower risk than the standard posterior approach (preserved rotators and capsule shield the nerve); avoid over-retracting the piriformis; avoid lengthening more than 2 cm; avoid posterior haematoma
- Management
- AFO for foot drop, PT or OT, serial EMG at 6, 12 and 24 weeks; most stretch injuries recover partly by 6 months. No recovery by 3 to 6 months: neurology referral, consider exploration or grafting
- Recognition
- Intra-operative decision: inadequate exposure, unexpected anatomy, or a complication needing better visualisation
- Prevention
- Appropriate patient selection; meticulous pre-operative planning; gain proficiency (50-plus cases) before complex cases; low threshold to convert
- Management
- Release the external rotators off the GT, extend the capsulotomy posteriorly and inferiorly to a full posterior exposure, complete the case, and plan a standard posterior repair; apply conventional posterior precautions post-op
- Recognition
- Intra-op: no audible snap on impaction. Post-op: early dislocation, squeaking, metallosis; liner proud on X-ray
- Prevention
- Clean the cup taper thoroughly; firm impaction until a loud snap; fluoroscopy can confirm seating (radiopaque markers)
- Management
- Intra-op: remove, re-clean and re-impact. Post-op early (less than 6 weeks): open liner exchange. Late with symptoms: open exchange, plus cup revision if the taper is damaged
- Recognition
- Patient reports asymmetry; block test and ASIS-to-malleolus measurement; compare lesser-trochanter heights on an AP pelvis
- Prevention
- Pre-operative templating; intra-operative external measurement of both legs at trial; fluoroscopic comparison of lesser trochanters (less accurate than conventional)
- Management
- Less than 10 mm: shoe lift if symptomatic. 10 to 20 mm: shoe lift and PT. Greater than 20 mm and symptomatic: consider revision (shorter neck or modular stem if too long; larger or high-offset stem if too short)
- Recognition
- Persistent wound drainage, fever, raised ESR or CRP, positive aspiration culture
- Prevention
- Pre-operative cefazolin, chlorhexidine or povidone-iodine prep, laminar flow, minimise operative time (longer during the learning curve)
- Management
- Early (less than 3 weeks) with stable implants: DAIR. Late or failed DAIR: two-stage revision (explant, cement spacer, 6 to 12 weeks IV antibiotics, re-implant)
- Recognition
- Leg swelling or pain (DVT), dyspnoea or chest pain (PE); raised D-dimer, Doppler US, CTPA
- Prevention
- LMWH or DOAC for 35 days, early mobilisation (walk on day 0), mechanical prophylaxis
- Management
- Therapeutic anticoagulation (LMWH or DOAC); IVC filter if recurrent despite anticoagulation
- Recognition
- Thigh pain (femoral), groin pain (acetabular), progressive radiolucent lines greater than 2 mm on serial X-rays
- Prevention
- Adequate cup press-fit (1 to 2 mm undersize reaming), appropriate stem fill, accurate positioning to avoid edge loading
- Management
- Asymptomatic with stable radiolucencies: observe. Symptomatic or progressive: revision
Viva & Exam Focus
PRESERVEDSuperPATH — the PRESERVED principle
WINDOWWorking through the WINDOW — technique principles
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old active patient with primary hip OA asks about SuperPATH versus the conventional posterior approach. How do you counsel them?”
“During SuperPATH you fracture the posterior acetabular wall while reaming. How do you recognise and manage this intra-operatively?”
“You are planning to start performing SuperPATH. What preparation and learning-curve management would you put in place to minimise complications?”
Core principle
- SuperPATH = Superior Portal Assisted Total Hip — a tissue-sparing posterior approach
- Preservation (not release or repair): work the gluteus-minimus-to-piriformis interval (minimus anterior, piriformis posterior) leaving the external rotators and posterior or inferior capsule intact
- Superior capsule window 3×4 cm — the portal for every step (neck cut, head removal, acetabular and femoral prep)
- Advantage: dislocation 0.5 to 1 percent (lowest of any approach), no precautions, faster recovery (discharge day 1, driving 2 to 4 weeks)
- Disadvantage: learning curve 50 to 100 cases and limited visualisation (fracture 1 to 3 percent, malposition 2 to 5 percent early)
Who is and is not a candidate
- Ideal: primary OA, normal anatomy, BMI less than 35, small-to-medium head (less than 54 mm), good bone, wants rapid recovery
- Relative: AVN with minimal deformity, elderly femoral-neck fracture with normal anatomy, closely staged bilateral THR
- Not a candidate: severe femoral deformity, head greater than 54 mm, severe acetabular deformity (Crowe III to IV, protrusio), BMI greater than 40, active infection, surgeon inexperience
Critical steps
- Lateral decubitus, pelvis perpendicular (critical for cup positioning with limited verification)
- Incision 6 to 10 cm, 2 to 3 cm posterior to the GT
- Blunt gluteus-maximus split (superficial access only)
- Deep interval: minimus anterior, piriformis posterior — rotators preserved, not released
- Superior capsule window 3×4 cm; posterior or inferior capsule intact
- Neck osteotomy in situ — complete the 360 degree cut before extraction
- Acetabular reaming by tactile feedback to 40 by 20 degrees; fluoroscopy recommended
- Femoral prep is the most demanding step — curved instruments, work by feel, conservative broaching
- Closure needs NO repair (nothing released)
Danger zones
- Sciatic nerve: 1 to 2 cm posterior — more protected than conventional (preserved rotators and capsule barrier), injury less than 0.5 percent
- Superior gluteal nerve: 4 to 5 cm proximal to the GT — limit proximal dissection
- Posterior acetabular wall: cannot be visualised directly — fracture risk 1 to 3 percent; fluoroscopy essential
- Proximal femur (GT and shaft): adjacent to the window — fracture risk 1 to 3 percent
- Inferior gluteal neurovascular bundle: below piriformis — protect with blunt maximus splitting
Technical pearls
- External-rotator preservation is the hallmark — if released, it is a conventional posterior approach
- Fluoroscopy is highly recommended (especially during the learning curve): pelvic positioning, reaming, cup verification, fracture detection
- Window size is critical: too small (less than 3×3 cm) forces the technique, too large (greater than 5×5 cm) loses the preservation advantage
- Complete the neck osteotomy before extraction — an incomplete cut plus forced extraction fractures the femur
- Acetabular reaming by tactile feedback; TAL for version (parallel is 20 degrees anteversion)
- Conservative femoral broaching is safer than aggressive — a smaller stable stem beats a larger stem with a fracture
- Keep a low threshold to convert to conventional (5 to 10 percent of learning-curve cases)
Major complications
- Periprosthetic femur fracture 1 to 3 percent (versus conventional less than 1 percent) — Vancouver classification guides management
- Cup malposition 2 to 5 percent (versus conventional 1 to 2 percent) — prevented with TAL, fluoroscopy, navigation; revise if outside the safe zone or symptomatic
- Posterior-wall fracture 1 to 3 percent — small and stable: screws through the cup; large or unstable: ORIF; massive: cage
- Dislocation 0.5 to 1 percent — lowest of any approach; closed reduction then CT, revise if recurrent
- Conversion to conventional 1 to 5 percent (learning curve) — release rotators, extend the capsulotomy, complete as conventional with repair and precautions
Viva high-yield
- What is SuperPATH? A tissue-sparing posterior approach preserving the external rotators and posterior capsule through a superior window, giving enhanced stability (dislocation 0.5 to 1 percent) and rapid recovery, traded against a learning curve and limited visualisation
- How does it differ from conventional posterior? Rotators and posterior capsule are preserved (retracted, not released) versus released and repaired; superior window only versus complete posterior capsulotomy; lower dislocation and no precautions versus higher dislocation if repair fails
- Main complications? Femoral fracture 1 to 3 percent, cup malposition 2 to 5 percent, posterior-wall fracture 1 to 3 percent — all from limited visualisation — offset by very low dislocation; use fluoroscopy or navigation to compensate
- Who is not a candidate? Severe femoral deformity, head greater than 54 mm, severe acetabular deformity, BMI greater than 40, and surgeon inexperience
- How do you position the cup accurately with limited visualisation? Multi-modal — TAL for version, mechanical guides for inclination, real-time fluoroscopy, and navigation or robotics
Background & Evidence
Approach choice is surgeon-dependent, not country-specific. The major national societies (AAOS, BOA or BOAST, AO Foundation, EFORT) do not mandate a single THA approach; the posterior, direct anterior, anterolateral and tissue-sparing (SuperPATH) variants are all accepted, and the evidence shows the approach matters most for early recovery rather than for long-term survivorship. Registry context. The large arthroplasty registries (NJR for England and Wales, AOANJRR for Australia, AJRR for the US, SHAR for Sweden) track survivorship by fixation and bearing rather than by minimally invasive sub-technique. SuperPATH uses the same cementless cups and stems as the standard posterior approach, so the registry survivorship data for those implants apply; dedicated long-term SuperPATH-specific registry survivorship remains limited because it is a relatively newer, lower-volume technique. Key evidence points 1. Dislocation around 0.8 percent — in the largest cited multicentre series of 479 hips (Gofton 2014), with several series reporting no dislocations at all; attributed to the preserved posterior capsule and external rotators. 2. Periprosthetic femoral fracture is the dominant intra-operative risk — about 0.8 percent in the 479-hip series and 4 of 344 (about 1.2 percent) in the Flevas series; it is the complication most directly tied to limited-visualisation femoral preparation. 3. Faster early recovery, equivalent positioning — Level I and II evidence (the Xie RCT; the Ramadanov network meta-analysis) shows a shorter incision, less blood loss, a shorter stay and lower early pain, with cup abduction and anteversion equivalent to conventional and direct anterior approaches. 4. Early advantages are not sustained — Harris Hip Score and functional differences versus the standard posterior approach resolve by one year (Xie RCT). 5. Same implants, registry data transfer — SuperPATH uses the same cementless components as the standard posterior approach, so implant-specific registry survivorship applies; dedicated long-term SuperPATH survivorship data remain limited. Beyond elective OA. A randomised trial (Jia et al., Injury 2019) and a meta-regression of five RCTs (Ramadanov et al., Orthop Surg 2024) found SuperPATH hemiarthroplasty for neck-of-femur fracture gives smaller incisions, less blood loss and faster early function, with elderly patients (over 70) appearing to benefit most — supporting its use beyond elective OA. A contemporary single-surgeon series (Flevas et al., Life 2022) reported 344 cases with a mean stay of 1.3 days, no dislocations and no infections; complications were four intra-operative femoral fractures and two peroneal nerve palsies — reinforcing that the dominant intra-operative risk is the proximal femur, not instability.
- SuperPATH (tissue-sparing)
- 6 to 10 cm, 2 to 3 cm posterior to the GT
- Conventional posterior (Moore/Southern)
- 15 to 20 cm, about 1 cm posterior to the GT
- SuperPATH (tissue-sparing)
- Preserved (retracted, not released)
- Conventional posterior (Moore/Southern)
- Released off the GT, then repaired at closure
- SuperPATH (tissue-sparing)
- Intact (superior window only)
- Conventional posterior (Moore/Southern)
- Opened (posterior capsulotomy), then repaired
- SuperPATH (tissue-sparing)
- None
- Conventional posterior (Moore/Southern)
- 6 to 12 weeks (no flexion past 90 degrees, no adduction, no internal rotation)
- SuperPATH (tissue-sparing)
- 0.5 to 1 percent (lowest of any approach)
- Conventional posterior (Moore/Southern)
- 1.5 to 2.5 percent (depends on repair quality)
- SuperPATH (tissue-sparing)
- 1 to 2 days, often outpatient
- Conventional posterior (Moore/Southern)
- 2 to 4 days
- SuperPATH (tissue-sparing)
- 2 to 4 weeks
- Conventional posterior (Moore/Southern)
- 6 to 12 weeks
- SuperPATH (tissue-sparing)
- 50 to 100 cases (steep)
- Conventional posterior (Moore/Southern)
- Mature technique, widely familiar
- SuperPATH (tissue-sparing)
- Limited visualisation — fracture 1 to 3 percent, malposition 2 to 5 percent early
- Conventional posterior (Moore/Southern)
- Higher dislocation if the rotator or capsule repair fails
- SuperPATH (tissue-sparing)
- Equalises to conventional by 1 year
- Conventional posterior (Moore/Southern)
- Decades of registry data
References
Modified micro-superior percutaneously-assisted total hip: early experiences and case reports (original SuperPATH description)
- First description of the SuperPATH approach as a hybrid of the percutaneously-assisted total hip (PATH) and supercapsular (SuperCap) techniques
- Defines a micro-posterior family on a continuum: micro (external-rotator-sparing, SuperPATH) to mini (external-rotator-sacrificing) to standard posterior — allowing extension if needed
- Core principle is preservation of the external rotators and capsule, working through a superior capsulotomy without dislocating the hip
SuperPath: The Direct Superior Portal-Assisted Total Hip Approach (definitive technique)
- Authoritative step-by-step technique: lateral decubitus with the leg in the home position, a 6 to 8 cm incision from the GT tip in line with the femur, and a blunt gluteus-maximus split
- Defines the deep interval — gluteus medius or minimus retracted anteriorly and the piriformis tendon retracted posteriorly — to reach the capsule without dissecting any muscle
- The femur is channelled and broached first with the head and neck intact, then the neck is osteotomised at the broach-neck level and the head removed; acetabular work is portal-based
- A multicentre series of nearly 500 SuperPATH THAs reported a 30-day all-cause readmission of 2.3 percent, transfusion 3.3 percent and a mean length of stay of 1.6 days with 91 percent discharged home
Supercapsular percutaneously-assisted total hip arthroplasty: radiographic outcomes and surgical technique
- Radiographic review of the first 100 SuperPATH cases (66 reported in detail)
- All components well-seated, leg length within 5 mm, mean cup abduction 40.13 degrees (SD 6.30 degrees)
SuperPATH versus conventional posterior approach for THA: a prospective randomised controlled trial
- 92 patients with unilateral primary hip OA randomised 1 to 1 to SuperPATH or conventional posterior approach
- No significant difference in operative time, blood loss, transfusion, complications, or radiographic cup abduction or anteversion and stem alignment
- SuperPATH had a shorter incision and length of stay, lower VAS pain at 1 week and at 1 and 3 months, and higher Harris Hip Score and Barthel Index at 1 and 3 months — differences resolved by 1 year
Thirty-day readmission rate and discharge status following THA using the SuperPATH technique
- Multicentre series of 479 primary SuperPATH THAs across three institutions
- Dislocation 0.8 percent, periprosthetic fracture 0.8 percent, DVT 0.2 percent, and no reported infections
- 30-day all-cause readmission 2.3 percent, transfusion 3.3 percent, mean length of stay 1.6 days, and 91.5 percent discharged directly home (versus 27.3 percent historically)
In-hospital costs for THA performed using the SuperPATH surgical technique
- Retrospective comparison of all SuperPATH THAs versus all other THAs in a large US hospital system (2013 to 2015)
- Overall in-hospital cost reduction of 15.0 percent with the tissue-sparing technique (operating-room costs down 17.3 percent, PT or OT down 26.8 percent, pharmacy down 25.3 percent)
- Length of stay 1.2 versus 2.6 days, transfusion 1.9 percent versus 15.8 percent, and 30-day readmission 0.4 percent versus 2.9 percent favouring SuperPATH
Short-term outcomes of DAA versus SuperPATH in THA: systematic review and network meta-analysis of RCTs
- 16 RCTs and 1,392 patients pooled (3 Level-I and 13 Level-II trials)
- Versus conventional approaches, SuperPATH reduced operative time, incision length, intra-operative blood loss and early (day-1) VAS pain
- No difference between SuperPATH and the direct anterior approach in acetabular cup positioning angles or functional outcome
Hip hemiarthroplasty for senile femoral neck fractures: minimally invasive SuperPath approach versus traditional posterior approach
- 100-patient RCT in neck-of-femur fracture comparing SuperPATH hemiarthroplasty with the traditional posterior approach
- SuperPATH gave a smaller incision, less bleeding and earlier weight-bearing
- Outcomes equalised by 3 months and at 2 years
Patient-related predictors for the functional outcome of SuperPATH hemiarthroplasty versus conventional-approach hemiarthroplasty: a systematic review and meta-regression of RCTs
- Meta-regression of 5 RCTs, 404 patients, examining predictors of functional outcome after SuperPATH hemiarthroplasty
- Elderly patients (over 70) benefited most from the SuperPATH hemiarthroplasty approach
The supercapsular percutaneously assisted total hip (SuperPATH) approach revisited: technique improvements after the perioperative experience of 344 cases
- Single-surgeon series of 344 SuperPATH cases with technique refinements
- Mean length of stay 1.3 days, no dislocations and no infections
- Complications were 4 intra-operative femoral fractures and 2 peroneal nerve palsies