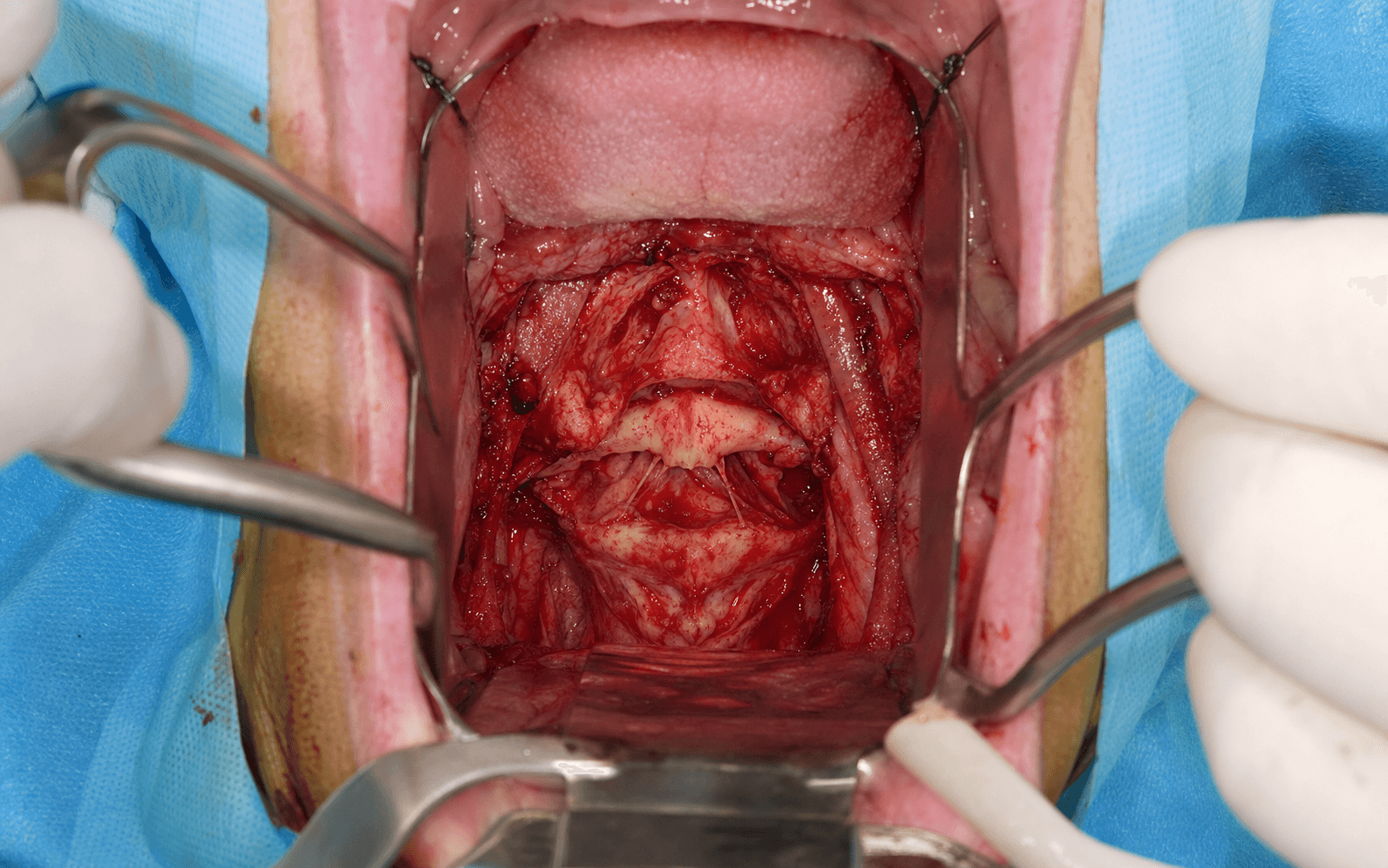
Midline Transpharyngeal | Soft Palate Split | Anterior Arch C1 & Odontoid Exposure
- Midline transpharyngeal exposure through a mouth-gag retractor with a midline split of the posterior pharyngeal wall.
- A soft palate split extends superior access to the lower clivus and the C1 anterior arch, but adds velopharyngeal incompetence risk.
- The vertebral arteries lie approximately 2 cm lateral to the midline — stay strictly midline, within 1 cm on either side.
- Always requires posterior stabilisation after odontoid resection or C1–C2 decompression (Harms–Goel or Magerl).
- Infection risk is high due to the contaminated pharyngeal field — meticulous layered closure is essential.
When & Why
What it exposes. The transoral route provides the most direct midline anterior corridor to the lower clivus, the anterior arch of C1, the odontoid process, and the C2 vertebral body. No other anterior cervical approach reaches this level without extensive dissection or a mandibular swing. Why this approach is chosen. It is the classic and gold-standard anterior approach for pathology at the craniocervical junction that cannot be reduced posteriorly and requires direct ventral decompression — particularly irreducible basilar invagination, rheumatoid pannus, and selected tumours. Primary indications: - Irreducible anterior compression at the craniocervical junction (basilar invagination, rheumatoid pannus, tumours)
- Odontoid resection for basilar invagination with ventral cervicomedullary compression
- Selected C1–C2 tumours requiring anterior column access (chordoma, metastasis)
- Chronic irreducible atlantoaxial subluxation with anterior cord compression
- Selected infectious pathology (tuberculous abscess, osteomyelitis) needing anterior debridement Contraindications: - Patient unable to tolerate prone or sitting position for posterior stabilisation
- Severe trismus or limited mouth opening preventing retractor placement
- Active oral or pharyngeal infection
- Previous high-dose radiotherapy to the pharynx with poor tissue quality
- Isolated posterior pathology better addressed by posterior approaches alone Alternative approaches. When the anterior compression is reducible with traction or positioning, posterior C1–C2 fusion alone suffices and the transoral route is avoided. Purely clival pathology above the palate is reached endoscopically endonasally, and selected lateral mass pathology by a lateral extrapharyngeal route; complex tumours may need combined staged anterior–posterior procedures. Approach variants. Exposure is tailored to how rostral or how wide the access must be.
- Indication
- C1–C2 odontoid pathology
- Technique
- Midline pharyngeal split only
- Risk profile
- Moderate (infection 2–5 percent)
- Indication
- Basilar invagination, clival tumours, high odontoid
- Technique
- Midline palate division for rostral access
- Risk profile
- Higher (velopharyngeal incompetence 10–15 percent)
- Indication
- Large tumours, limited mouth opening
- Technique
- Mandibular swing osteotomy
- Risk profile
- High morbidity, rarely performed
- Indication
- Minimally invasive access
- Technique
- Endoscope through mouth with standard retractor
- Risk profile
- Reduced soft tissue trauma, steep learning curve
Position & landmarks. Supine on a radiolucent table with the head in a Mayfield clamp or horseshoe and slightly extended (about 15–20 degrees) to open the oral corridor; the surgeon stands at the head of the table. The mouth is opened maximally with a Dingman or Crowe-Davis gag and the tongue depressed with a blade. The anterior tubercle of C1 is the central reference point, palpable through the posterior pharyngeal wall; the odontoid is the midline prominence above it and the C2 body the inferior extension. The planned incision is a midline vertical cut in the posterior pharyngeal wall from the C1 tubercle to the C2–C3 disc (4–6 cm), staying strictly within 1 cm of the midline. A lateral fluoroscopy C-arm or O-arm and microscope or loupes are made available for the deep dissection.
The Exposure
Work down through the pharyngeal layers strictly in the midline, splitting the superior constrictor along its raphe and elevating longus colli subperiosteally to reach the anterior arch of C1, then deliver and resect the odontoid while protecting the dura. There is no classical internervous plane — safety comes from absolute midline discipline between the two vertebral arteries.
Exposure sequence
- Perform nasotracheal intubation or tracheostomy to keep the oral field clear; position the patient supine with the head extended about 15–20 degrees.
- Insert the mouth-gag retractor (Dingman or Crowe-Davis) to open the oral cavity maximally and depress the tongue with a blade.
- Visualise the soft palate and posterior pharyngeal wall; infiltrate the posterior pharyngeal wall with 1 percent lignocaine and 1:100000 adrenaline for haemostasis.
- Confirm levels with lateral fluoroscopy; have the microscope or loupes ready for the deep dissection.
- If superior exposure to the lower clivus or a high-riding odontoid is needed, split the soft palate in the midline from the uvula to the hard palate junction.
- Retract the uvula laterally or divide it; tag the palate edges with sutures for later identification during closure.
- The nasopharynx is now accessible for rostral work.
- Make a vertical midline incision in the posterior pharyngeal wall from the C1 anterior tubercle to the C2–C3 disc (4–6 cm), carried through mucosa, submucosa and the superior constrictor muscle along the midline raphe.
- Develop the submucosal plane only 5–10 mm laterally; coagulate small pharyngeal vessels with bipolar.
- Open the prevertebral fascia sharply to expose the longus colli muscles and the anterior longitudinal ligament.
- Elevate the longus colli subperiosteally off the anterior arch of C1 and the C2 body with a Cobb elevator, working from the midline outward.
- Use the anterior tubercle of C1 as the central landmark; identify the anterior arch of C1, palpate the odontoid apex superiorly, and expose the C2 body inferiorly.
- Keep all dissection strictly within 1 cm of the midline — the vertebral arteries are protected by staying medial to their course in the C1 groove.
- Remove the anterior arch of C1 with rongeurs or a high-speed burr where it overlies the odontoid, to deliver the odontoid into view.
- Divide the apical and alar ligaments; drill the odontoid from apex to base with a high-speed burr under direct vision.
- Divide the transverse ligament if still intact; remove any pannus or tumour; protect the dura throughout with Penfield dissectors.
- Achieve haemostasis with bone wax and bipolar coagulation.
- If the dura is breached or thinned, place a dural patch (fascia lata or synthetic) over the defect.
- Insert a lumbar drain if a CSF leak is present or anticipated, to divert CSF away from the contaminated pharyngeal closure.
The vertebral artery lies approximately 2 cm lateral to the midline in the C1 groove; injury causes posterior circulation stroke, Wallenberg syndrome, or death. The safe working corridor is less than 1 cm on either side of the midline, using the anterior tubercle of C1 as the central landmark. Any lateral deviation risks direct injury. If brisk arterial bleeding is encountered, apply direct pressure with a patty — do not clamp or ligate in the deep field — and obtain urgent endovascular consultation.
The vertebral artery lies approximately 2 cm lateral to the midline at C1–C2; the safe working corridor is less than 1 cm on either side. The anterior tubercle of C1 is the central landmark, and lateral deviation is the most common cause of inadvertent injury.
Dangers & Extensions
Structures at risk, by layer.
- Structure at risk
- Pharyngeal vessels
- Protection
- Stay midline, bipolar coagulation, adrenaline infiltration
- Structure at risk
- Superior constrictor; glossopharyngeal nerve (lateral in pharyngeal wall)
- Protection
- Split in the midline raphe, limit lateral retraction to avoid neuropraxia
- Structure at risk
- Longus colli, anterior longitudinal ligament
- Protection
- Subperiosteal elevation, protect the medial branches
- Structure at risk
- Vertebral artery (approximately 2 cm lateral in the C1 groove)
- Protection
- Never exceed 1 cm lateral to midline; use the anterior tubercle landmark
- Structure at risk
- Spinal cord, dura, anterior spinal artery
- Protection
- Protect with Penfield dissectors during drilling; careful magnified technique
Vertebral artery injury management. If brisk arterial bleeding is encountered lateral to the midline: apply immediate tamponade with bone wax or a muscle patty; do not attempt primary repair in the transoral field; obtain urgent endovascular consultation for possible stenting or sacrifice; and monitor the posterior circulation in ICU. Prevention is absolute midline discipline, with preoperative CTA to map a dominant or anomalous vertebral artery and intraoperative navigation or fluoroscopy to confirm position. Specific complications and their incidence.
- Incidence
- 2–8 percent
- Prevention and management
- Prophylactic antibiotics, watertight two-layer closure; culture-directed IV antibiotics, lumbar drain if CSF leak
- Incidence
- 10–15 percent
- Prevention and management
- Meticulous three-layer palate closure; speech therapy, palatal lengthening or flap if persistent
- Incidence
- 5–10 percent
- Prevention and management
- Dural repair, lumbar drain; 5–7 days drainage, re-exploration if persistent
- Incidence
- 20–40 percent (transient)
- Prevention and management
- Early swallow assessment, nasogastric feeding, speech therapy
- Incidence
- Common
- Prevention and management
- Maintain intubation or tracheostomy 48–72 hours, steroids for oedema
- Incidence
- Less than 1 percent
- Prevention and management
- Absolute midline discipline, preoperative CTA; endovascular management
Infection rates after transoral surgery range from 2–8 percent despite prophylactic antibiotics. The pharyngeal closure must be watertight, and a CSF leak dramatically increases the meningitis risk. Early recognition with lumbar drainage and culture-directed antibiotics is essential.
Extensile options. Extend rostrally by splitting the soft palate to reach the lower clivus; further rostral access needs endoscopic assistance or, rarely, a mandibulotomy (high morbidity, seldom performed in modern practice). Extend inferiorly to C3 by continuing the pharyngeal incision and elevating longus colli further, though the standard corridor is limited to C2–C3. Lateral extension is deliberately avoided — the corridor is kept within 1 cm of the midline to protect the vertebral arteries, and wider lateral exposure requires an alternative extrapharyngeal or endoscopic route. For complex pathology the transoral decompression is combined with posterior C1–C2 fusion (Harms–Goel) in the same sitting or within 48 hours. Closure. Approximate the longus colli with absorbable suture and close the prevertebral fascia if possible; close the superior constrictor and submucosa with interrupted absorbable sutures, then the pharyngeal mucosa with continuous or interrupted absorbable suture — watertight closure in two layers is essential. If the palate was split, close it in three layers: nasal mucosa, the muscular layer (levator and tensor veli palatini), and oral mucosa, reconstructing the uvula if divided. Remove the mouth gag, inspect the pharynx for bleeding, and place a nasogastric tube for feeding if prolonged intubation is anticipated. Post-operative care. Maintain the nasotracheal tube or tracheostomy for 48–72 hours with ICU monitoring of the airway, neurological status and CSF leak; document a cuff leak and give steroids before extubation. Keep the patient nil by mouth with nasogastric feeding until a videofluoroscopic swallow study or FEES is safe, and immobilise in a cervical collar or halo until the posterior fusion is performed. Follow up at 2 weeks (wound and pharyngeal inspection), 6 weeks (flexion-extension radiographs), 3 months (CT for resection and fusion), 6 months and 1 year.
Procedures Through This Approach
- Odontoid resection for basilar invagination or irreducible atlantoaxial subluxation.
- Anterior decompression of rheumatoid pannus or ventral tumour.
- Tumour biopsy or debulking (chordoma, metastasis).
- Drainage of a retropharyngeal or prevertebral abscess.
- Anterior C1–C2 discectomy (rare, usually combined with posterior). Always combined with posterior stabilisation. Any anterior decompression that removes the odontoid or disrupts the transverse ligament destabilises the C1–C2 complex — the transoral approach provides decompression but no stability. Posterior C1–C2 fusion — Harms–Goel technique (C1 lateral mass and C2 pedicle screws) or Magerl transarticular screws is mandatory, performed in the same sitting or within 48 hours; extend to an occipitocervical fusion if the occipital condyles are involved.
Viva & Exam Focus
TRANSORALTRANSORAL — key surgical principles
Hook:TRANSORAL approach — stay midline, protect the vertebral arteries, and always fuse posteriorly.
DANGERDANGER — layer-by-layer risk
Hook:DANGER structures increase with lateral or superior extension beyond the safe midline corridor.
Exam viva scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old with basilar invagination and progressive myelopathy has an odontoid tip 8 mm above Chamberlain's line with no reduction on traction. How would you manage this?”
“On day 3 after transoral odontoid resection, the patient develops fever, neck stiffness, and clear nasal discharge. What is your assessment and management?”
“During odontoid resection you encounter brisk arterial bleeding 1.5 cm lateral to the midline on the left. What is your immediate response and subsequent management?”
Position and landmarks
- Supine with the head extended 15–20 degrees
- Mouth-gag retractor (Dingman or Crowe-Davis)
- Nasotracheal intubation or tracheostomy
- Anterior tubercle of C1 is the central landmark
- Midline vertical pharyngeal incision from C1 to C2–C3
Internervous plane
- No classical internervous plane
- Midline raphe of the superior constrictor
- Strictly midline dissection between the vertebral arteries
- Safe corridor less than 1 cm lateral to the midline
- Longus colli elevated subperiosteally
Danger structures by layer
- Mucosal: pharyngeal vessels (bipolar)
- Muscular: superior constrictor (midline raphe split)
- Deep: longus colli, anterior longitudinal ligament
- Vascular: vertebral artery (approximately 2 cm lateral)
- Dural: spinal cord and dura (protect during drilling)
Soft palate split decision
- Required for lower clivus or high-odontoid exposure
- Adds 10–15 percent velopharyngeal incompetence risk
- Close in three layers: nasal mucosa, muscle, oral mucosa
- Speech therapy essential post-operatively
Procedures and stabilisation
- Odontoid resection for basilar invagination
- Anterior decompression of pannus or tumour
- Always combine with posterior C1–C2 fusion (Harms–Goel)
- Posterior fusion same sitting or within 48 hours
- Occipitocervical extension if occipital condyles involved
Complications and consent
- Vertebral artery injury (less than 1 percent but catastrophic)
- CSF leak (5–10 percent) — lumbar drain, dural repair
- Infection or meningitis (2–8 percent) — watertight closure
- Velopharyngeal incompetence (10–15 percent with palate split)
- Airway oedema — maintain intubation 48–72 hours
References
Guidelines, registries and global practice. The transoral approach is a specialised technique performed at major spine centres worldwide; the principles — CT and MRI planning, vertebral-artery mapping, and mandatory posterior stabilisation after anterior decompression — are near-universal across contemporary practice systems.
- Position on craniocervical junction approaches
- CT and MRI mandatory for all craniocervical pathology; transoral for irreducible anterior compression; posterior stabilisation required after odontoid resection
- Position on craniocervical junction approaches
- Multidisciplinary assessment; endoscopic alternatives considered when appropriate; infection-prevention protocols emphasised
- Position on craniocervical junction approaches
- Centralisation to specialist centres; combined anterior–posterior expertise; consent must include velopharyngeal incompetence and CSF leak
Registry and population evidence. Basilar invagination and rheumatoid craniocervical pathology are rare, so most series are single-centre retrospective. Harms–Goel C1–C2 fusion after transoral decompression achieves greater than 95 percent fusion rates with low morbidity in experienced hands. Infection rates of 2–8 percent are reported across series, and CSF leak is the strongest predictor of meningitis. Global practice variation. In high-resource centres, endoscopic-assisted transoral and purely endoscopic endonasal approaches are increasingly used to reduce soft-tissue morbidity; in resource-limited settings, the open transoral approach with meticulous technique remains standard. Posterior stabilisation uses C1 lateral mass and C2 pedicle screws (Harms–Goel) or transarticular screws (Magerl) depending on local expertise and anatomy. Consent (globally applicable). Discuss vertebral artery injury (less than 1 percent but catastrophic), CSF leak (5–10 percent), infection and meningitis (2–8 percent), velopharyngeal incompetence (10–15 percent with palate split), airway compromise requiring prolonged intubation or tracheostomy, dysphagia, and the absolute requirement for posterior stabilisation.
For the Operative Surgery station you must describe the transoral approach systematically: positioning, mouth-gag retraction, midline pharyngeal incision, the soft-palate-split decision, the vertebral-artery distance (approximately 2 cm), the odontoid-resection technique, layered closure, and the mandatory posterior C1–C2 fusion — and know the specific complications of velopharyngeal incompetence and CSF-leak management.
Transoral-transpharyngeal approach to the anterior craniocervical junction. Ten-year experience with 72 patients.
- Ten-year experience with 72 patients demonstrating the safety and efficacy of the transoral approach for anterior craniocervical junction pathology with mandatory posterior stabilisation
Posterior C1-C2 fusion with polyaxial screw and rod fixation.
- Polyaxial screw and rod fixation provides rigid stabilisation for C1-C2 with fusion rates greater than 95% and low complications, ideal after transoral decompression
Evolution of transoral approaches, endoscopic endonasal approaches, and reduction strategies for treatment of craniovertebral junction pathology: a treatment algorithm update.
- Provides updated treatment algorithm integrating transoral and endoscopic approaches for craniovertebral junction pathology including basilar invagination
Odontoid upward migration in rheumatoid arthritis. An analysis of 45 patients with 'cranial settling'.
- Classic analysis of cranial settling in rheumatoid arthritis establishing the role of anterior decompression for irreducible basilar invagination
Transoral-transpharyngeal approach to the craniocervical junction.
- Soft palate division increases rostral exposure but carries 10–15 percent risk of velopharyngeal incompetence
- Three-layer closure technique reduces but does not eliminate palatal dysfunction
- Curved incision along the palate edge may reduce tension compared with straight midline split
- Most velopharyngeal incompetence resolves with speech therapy within 6–12 months
Transoral and transnasal odontoidectomy complications: A systematic review and meta-analysis.
- Vertebral artery lies approximately 2 cm lateral to midline at C1–C2 level
- Safe working corridor is less than 1 cm on either side of the midline
- Anterior tubercle of C1 is the critical central landmark
- Lateral deviation is the most common cause of inadvertent injury
Infection rate after transoral approach for the upper cervical spine.
- Infection rate after transoral odontoid resection was 4.2 percent in a large series
- Watertight two-layer pharyngeal closure and prophylactic antibiotics are essential
- CSF leak increased meningitis risk significantly
- Early lumbar drainage and culture-directed antibiotics improved outcomes in infected cases